Supporting the Development of
Professional Identity in the
Millennial Learner
Michael A. Barone, MD, MPH,a,bChad Vercio, MD,c,dThanakorn Jirasevijinda, MDe
As teachers, we train learners to be knowledgeable and competent in the practice of medicine. No less important is the way teachers impact the development of learners’professional identity. Social scientists in the 1950s noted medical education’s charge“to shape the novice into the effective practitioner of medicine, to give [them] the best available knowledge and skills, and to provide [the novice] with a professional identity so that [they] come to think, act, and feel like a physician.”1Many have stressed the importance of curricula focused on learners’ personal and professional development.2An awareness of professional identity development helps teachers understand some of the workplace differences noted between generations, particularly with millennial learners.
Continuing the Council on Medical Student Education in Pediatrics series on great clinical teachers, our article focuses on supporting professional identity formation (PIF) in millennial learners.
Professional identity formation (ie, the socialization and
professionalization of a physician) develops in stages over time.3PIF consists of ordering and reordering personal and professional
priorities as one progresses from student to effective practitioner.3–5 This process has been linked to one’s personal identity
development.6Characteristics of 3 important stages of physician PIF include the following5:
Early: foundational education (premedical students and early medical students)
•follow social roles and rules
•appreciate others’viewpoints, yet self-views predominate;
Middle: training and/or supervised practice (later medical students and residents)
•view medical practice through multiple perspectives
•subordinate self-interests more effectively
•feel a sense of belonging but not yet“professional”
•may still have trouble reconciling competing expectations;
Later: practicing professional (practicing physicians)
•understand differing values and perspectives
•own and embody expectations of the profession
•begin to internalize the external values of the profession
•reconcile challenges between personal and professional expectations more effectively.
An identity as a physician is the foundation for professional behaviors. For example, a major pillar of professionalism is
a commitment to maintaining trust by subordinating self-interest and
aNational Board of Medical Examiners, Philadelphia, Pennsylvania; bSchool of Medicine, Johns Hopkins University, Baltimore, Maryland; cSchool of Medicine, Loma Linda University, Loma Linda, California; dRiverside University Health System, Moreno Valley, California; and eWeill Cornell Medical College, Cornell University, New York, New York
Drs Barone, Vercio, and Jirasevijinda conceptualized and drafted the initial manuscript and reviewed and revised the manuscript; and all authors approved thefinal manuscript as submitted and agree to be accountable for all aspects of the work.
DOI:https://doi.org/10.1542/peds.2018-3988 Accepted for publication Dec 17, 2018
Address correspondence to Michael A. Barone, MD, MPH, National Board of Medical Examiners, 3750 Market St, Philadelphia, PA 19104. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
managing professional responsibilities.5,7Through acknowledgment, questioning, and role modeling, clinical teachers can support a learner’s professional identity development, ensuring smooth transitions. Understanding personal identity formation and PIF is central to teaching, mentoring, and remediating learners.
Concern exists about the millennial generation’s preparedness to meet the expectations of the profession. Millennials (born 1981–2000) are said to have been reared in a“ child-focused”world with high parental involvement and relationships shaped by media.8In medicine, millennials have been characterized as having less commitment to and ownership of patients, a work life shaped more by personal demands, and a sense of greater importance to an organization despite a relative lack of experience. These factors could lead to conflicts with teachers about expectations and commitment.9,10Nonetheless, millennials bring many strengths to medicine, such as collaborative learning, acceptance of diversity, and a strong sense of social
consciousness.11In Table 1, we summarize millennials’
characteristics that potentially impact PIF in positive and negative ways.
Generational differences between teachers and learners may create conflicts. We propose the I-CA2R2E (individual connection, create, acknowledge and adjust, reflect and role model, and exchange) framework (Table 1) to provide strategies to maximize learners’PIF. The
framework addresses the 3 pillars of Self-Determination Theory, which are autonomy, competence, and
relatedness.12The 3 brief cases that follow illustrate how I-CA2R2E can help guide clinical teachers.
CASE 1: THE PERFORMANCE-FOCUSED LEARNER
A clerkship student meets with her preceptor to discuss dissatisfaction with feedback she received,
concerned that the preceptor pointed out areas for improvement.
Potential Issues
The learner, in her early stage of PIF, may view clinical work in a self-focused manner and perceive feedback as judgment and not an opportunity for growth.11
Proposed Solutions Using the I-CA2R2E Framework
I - Make individual connection and explore the learner’s experience with previous feedback.
C - Create a safe space to discuss how the feedback impacts the learner’s view of herself and her role (ie, as test taker versus lifelong learner).
A - Acknowledge grading pressures in medical school and the learner’s concerns that grades are“all that matters”for residency selection.
A - Adjust your own views on feed-back and recognize how genera-tional differences play a role in how feedback is received.
R - Reflect: encourage reflection on key influences in the learner’s identity development (mentors, patients, other experiences).
R - Role model by sharing how feed-back has benefitted you (for ex-ample, how listening to the observations and perspectives of others provided opportunities for personal and professional growth).
E - Exchange: arrange for follow-up with the learner to check in on challenges and successes.
CASE 2: THE SELF-INTERESTED LEARNER WITH MISPLACED PRIORITIES
A subintern visiting from another institution is upset because of his attending’s raising concerns about his level of commitment. The subintern’s
assignment on his patient’s
adjustment to a serious diagnosis was submitted late. When asked, the subintern explains he“prefers taking care of his patients” and that written assignments“matter less”than clinical care.
Potential Issues
The learner may not fully be able to subordinate self-interests and have trouble reconciling competing priorities.
Proposed Solutions Using the I-CA2R2E Framework
I - Make a connection by exploring personal background and career goals.
C - Create a safe space to explore how this learner prioritizes competing commitments.
A - Acknowledge that competing demands can be difficult to manage.
A - Adjust your own potential biases about this learner being“ dis-engaged”or“uninterested.”
R - Reflect: encourage the learner’s reflection on his ordering of priorities.
R - Role model by sharing how you have grappled with managing competing priorities.
E - Exchange: provide rationale for assignments and offer to assist and exchange ideas about the how this subintern can order future priorities.
CASE 3: THE LEARNER WITH A LIMITED VIEWPOINT
A senior resident objects to the residency program’s decision to limit intern shifts to 16 hours. He
complains program leadership is “getting soft”and publicly challenges other residents for having supported the program’s decision.
Potential Issues
The learner may have a limited ability to consider multiple perspectives.
The senior resident’s emotional approach to sharing his perspective is not productive.
Proposed Solutions Using the I-CA2R2E Framework
I - Recognize this resident’s individual perspective as he approaches un-supervised practice.
C - Create an opportunity for the resident to articulate rationale, not simply emotional reactions.
A - Acknowledge that the resident is entitled to his point of view, yet the decision-making process (program leadership and other resident input) should be respected. Encourage the resident to focus on outcomes and not only resident work hours.
A - Adjust your personal biases and understand that generational
differences impact expectations of learners.
R - Reflect and role model: probe the resident’s view on how his action manifested as role modeling for others (ie, hours in the hospital versus a focus on quality, safety, and relationships with patients). Reflect on a time when your own first impressions were modified over time.
E - Exchange: set a time for follow-up and ask for ideas about how future group decisions can be
collaborative.
CONCLUSIONS
Although it may seem a distant memory to great clinical teachers, the early stages of a medical learner’s PIF
can be disconcerting andfilled with conflict, self-doubt, and an inadequate sense of belonging to the profession. Millennial learners may particularly need guidance through challenges to make critical decisions (ordering and reordering priorities) that ultimately lead to the embodiment of
professional behaviors (ie, thinking, acting, and feeling like a physician). Supervisors who approach teachable moments with open-mindedness, a willingness to challenge
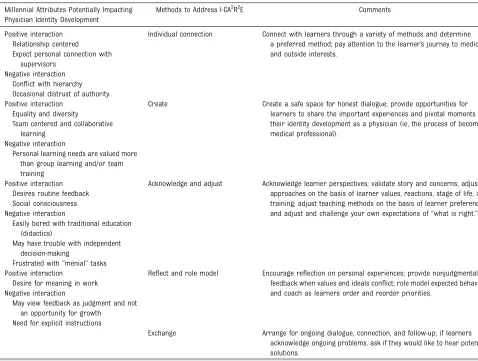
expectations, and tools to stimulate exploration and self-reflection (I-CA2R2E) will be able to promote learners’development of a strong foundational identity in medicine. When learners experience the investment of a clinical teacher in their professional journey, everyone benefits, including patients, who TABLE 1Millennial Attributes That May Positively and Negatively Interact With PIF and the I-CA2R2E Framework
Millennial Attributes Potentially Impacting Physician Identity Development
Methods to Address I-CA2R2E Comments
Positive interaction Individual connection Connect with learners through a variety of methods and determine a preferred method; pay attention to the learner’s journey to medicine and outside interests.
Relationship centered Expect personal connection with
supervisors Negative interaction
Conflict with hierarchy Occasional distrust of authority
Positive interaction Create Create a safe space for honest dialogue; provide opportunities for learners to share the important experiences and pivotal moments in their identity development as a physician (ie, the process of becoming medical professional).
Equality and diversity
Team centered and collaborative learning
Negative interaction
Personal learning needs are valued more than group learning and/or team training
Positive interaction Acknowledge and adjust Acknowledge learner perspectives; validate story and concerns; adjust approaches on the basis of learner values, reactions, stage of life, and training; adjust teaching methods on the basis of learner preferences; and adjust and challenge your own expectations of“what is right.” Desires routine feedback
Social consciousness Negative interaction
Easily bored with traditional education (didactics)
May have trouble with independent decision-making
Frustrated with“menial”tasks
Positive interaction Reflect and role model Encourage reflection on personal experiences; provide nonjudgmental feedback when values and ideals conflict; role model expected behavior; and coach as learners order and reorder priorities.
Desire for meaning in work Negative interaction
May view feedback as judgment and not an opportunity for growth
Need for explicit instructions
ultimately receive care from physicians who truly embody the expectations of the medical profession above their own needs.
ACKNOWLEDGMENT
We thank Dr Nicholas Potisek for his thoughtful contributions in
conceptualizing this article.
ABBREVIATIONS
I-CA2R2E: individual connection, create, acknowledge and adjust, reflect and role model, and exchange PIF: professional identity
formation
REFERENCES
1. Merton RK, Reader GG, Kendall PL, eds.
The Student-Physician: Introductory Studies in the Sociology of Medical
Education. Cambridge, MA: Published
for the Commonwealth Fund by Harvard University Press; 1957
2. Inui TS.A Flag in the Wind: Educating
for Professionalism in Medicine.
Washington, DC: Association of American Medical Colleges; 2003
3. Johnston S. See one, do one, teach one: developing professionalism across the generations.Clin Orthop Relat Res. 2006;449(449):186–192
4. Cruess SR, Cruess RL. Teaching professionalism - why, what and how.
Facts Views Vis ObGyn. 2012;4(4):
259–265
5. Cruess RL, Cruess SR, Boudreau JD, Snell L, Steinert Y. A schematic representation of the professional identity formation and socialization of medical students and residents: a guide for medical educators.Acad Med. 2015; 90(6):718–725
6. Kegan R.The Evolving Self: Problem and
Process in Human Development.
Cambridge, MA: Harvard University Press; 1982
7. American Board of Internal Medicine Foundation. The physician charter.
Available at: http://abimfoundation.org/ what-we-do/physician-charter. Accessed November 1, 2018
8. Clark University. About the Clark University poll. Clark University poll. Available at: http://www2.clarku.edu/ clark-poll-emerging-adults/. Accessed November 1, 2018
9. Eckleberry-Hunt J, Tucciarone J. The challenges and opportunities of teaching“generation y”.J Grad Med Educ. 2011;3(4):458–461
10. Shaw H.Sticking Points: How to Get 4 Generations Working Together in the 12
Places They Come Apart. Carol Stream,
IL: Tyndale House Publishers; 2013
11. Lancaster LC, Stillman D, Mackay H.
When Generations Collide: Who They Are, Why They Clash, How to Solve the
Generational Puzzle at Work. New York,
NY: Collins Business; 2005
12. Kusurkar R, ten Cate O. AM last page: education is notfilling a bucket, but lighting afire: self-determination theory and motivation in medical students.
Acad Med. 2013;88(6):904
DOI: 10.1542/peds.2018-3988 originally published online February 5, 2019;
2019;143;
Pediatrics
Michael A. Barone, Chad Vercio and Thanakorn Jirasevijinda
Supporting the Development of Professional Identity in the Millennial Learner
Services
Updated Information &
http://pediatrics.aappublications.org/content/143/3/e20183988
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/143/3/e20183988#BIBL
This article cites 5 articles, 0 of which you can access for free at:
Subspecialty Collections
ub
http://www.aappublications.org/cgi/collection/career_development_s
Career Development
b
http://www.aappublications.org/cgi/collection/medical_education_su
Medical Education following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2018-3988 originally published online February 5, 2019;
2019;143;
Pediatrics
Michael A. Barone, Chad Vercio and Thanakorn Jirasevijinda
Supporting the Development of Professional Identity in the Millennial Learner
http://pediatrics.aappublications.org/content/143/3/e20183988
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2019 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news