EFFECT OF PHOTO-POLYMERIZATION DELAY ON THE BOND STRENGTH AND MICROHARDNESS OF DUAL-POLYMERIZING RESIN CEMENT
Basheer Alsayed
A thesis submitted to the Faculty of The University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the Department of Comprehensive Oral Sciences of the Adams School of Dentistry at the Division of Operative
Dentistry and Biomaterials
Chapel Hill 2020
ABSTRACT
Basheer Alsayed: Effect of photo-polymerization delay on the bond strength and microhardness of dual-polymerizing resin cement.
(Under the direction of Taiseer Sulaiman)
Objective: To examine the effect of photo-polymerization delay on dentin shear-bond strength and Vickers microhardness of two different dual-polymerizing resin cements.
Materials and Methods: Shear bond strength (SBS) of two dual-polymerizing; adhesive (RelyX Ultimate, 3M) and self-adhesive (RelyX Unicem 2, 3M) resin cements were evaluated. Dentin specimens (n=80) were prepared for SBS test according to ISO standard 29022:2013. Teeth were randomly allocated into 8 groups based on the type of dual-polymerizing resin cement, and the photo-polymerization delay times (0-2-5-10 minutes). Vickers microhardness test (HV) was performed following (ASTM E384-17)with a total of 32 specimens were prepared on the basis of type of cement and photo-polymerization time intervals using a 1mm thickness mold. Each specimen was tested immediately and after 24h of storage. The statistical analysis
Results: For the SBS outcome, the interaction between resin cement and polymerization time was highly significant (p < 0.0001), suggesting that the effect of photo-polymerization time is different between the two resin cement types. The variable for resin cement type was also statistically significant (p<0.0001). When adhesive cement was used, the dentin SBS values were higher than self-adhesive cement groups.
For the immediate and after 24h storage Vickers microhardness outcome, the interaction between resin cement and photo-polymerization time was not statistically significant. The variable for resin cement type is statistically significant (p<0.0001).
ACKNOWLEDGEMENTS
First of all, I would like to thank and praise God for giving me the power and strength to achieve my dreams. Also, I would like to thank the Saudi Arabian Cultural Mission for giving me this opportunity, support and funding to reach my goals.
I would like to express my profound gratitude to my mentor Dr. Taiseer Sulaiman, and my thesis committee members, Drs. Wendy Clark and Ryan Cook for their great guidance and help throughout this project. I would also like to thank Mr. Brandon Rogers for the help and support he genuinely offered in the laboratory. Dr. Ceib Phillips and Miss. Poojah deserve many thanks for their help with the statistical analysis of my data.
I would like to offer my exceptional gratitude to Drs. Gustavo Oliveira, Lee Boushell, Harald H. Heymann, Al Wilder, Patricia Miguez, Mauro Nunes, John Sturdevant, Ricardo Walter, Sumitha Ahmed, Jean-pierre Albouy and Terence Donovan. It has been an honor and a privilege to be part of the UNC Operative Dentistry Family. Many thanks also to the staff of the Division of Operative Dentistry, Mrs. Melissa Bennett, Mrs. Barbara Walton, Mrs. Kimberly Stoen and Miss. Carmen Ramsey and Mr. Jose Negron for all your devotion and commitment.
Exceptional thanks to my parents, Mrs. Ina’am Basinan and Mr. Fareed Alsayed for their being extremely supportive and for the love, care, prayers and sacrifice they have been giving me. I would not be who I am without you two, so blessed to have the greatest parents of all time. I love so much you two.
TABLE OF CONTENTS
LIST OF TABLES………...………x
LIST OF FIGURES………xi
LIST OF ABREVIATIONS AND SYMBOLS………xii
CHAPTER 1: REVIEW OF THE LITERATURE………..1
1. Introduction………..1
2. Literature Review……….4
2.1. Composition of Teeth Substrates………..4
2.1.1. Dental Enamel………..4
2.1.2. Dental Dentin………...4
2.2. Adhesion to Teeth Structure………..5
2.3. History and Classifications of Dental Cements………6
2.4. Dental Resin Cements………...7
2.5. In vitro evaluation of bond performance………8
2.5.1. Bond strength Test (Shear test) ………...…9
2.5.2.1. Relationship I………10
2.5.2.2. Relationship II………...11
2.5.2.3. Relationship III……….…11
2.5.2.4 Relationship IV………..…12
2.6. Evaluation of polymerization efficiency (Hardness Test) ………...12
REFERENCES………...17
CHAPTER 2: MANUSCRIPT………..22
1. Introduction .………....22
2. Materials and Methods………..………24
2.1. Materials.………..24
2.2. Shear Bond Strength Test ………25
2.2.1. Preparation of Teeth Samples………..25
2.2.2. Preconditioning………...26
2.2.3. Insertion into a bonding clamp and cement placement………27
2.2.4. Notched-edge shear test………...27
2.3. Vickers Micro-hardness Test……….…29
3.2. Vickers Micro-hardness Test………..33
4. Discussion………..36
5. Conclusions………39
LIST OF TABLES
LIST OF FIGURES
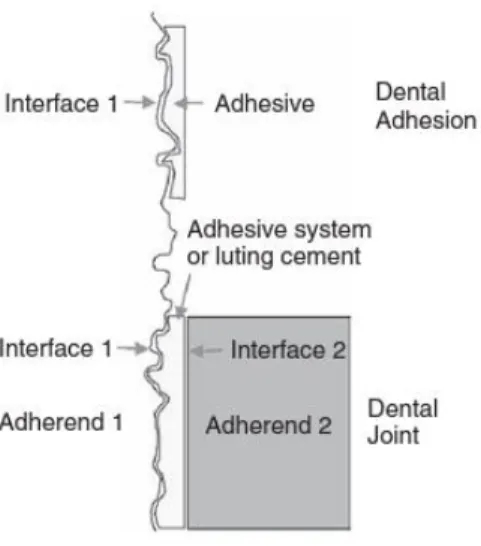
Figure 1.1: Definitions of The Terminology Associated with Adhesive Systems………..5
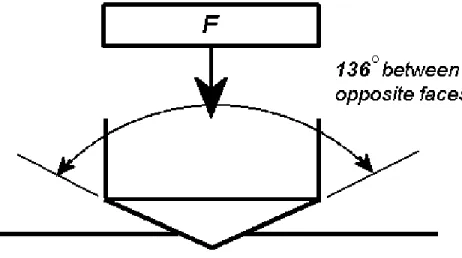
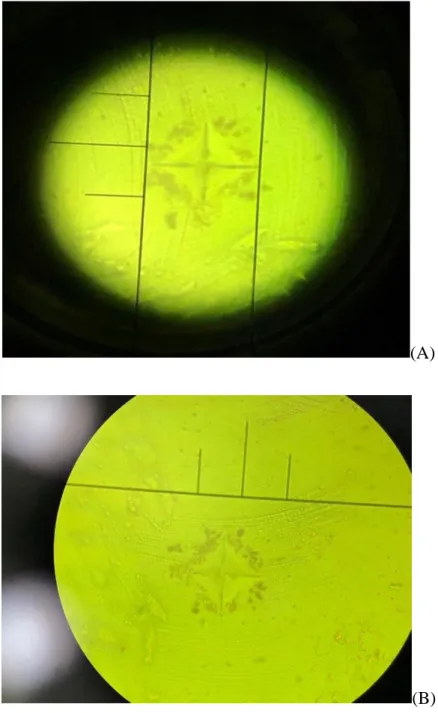
Figure 1.2: Schematic Illustration of Force Applied to the Surface by Micro-hardness Indenter.14 Figure 1.3: Illustrations of Indentations Left on the Surface Under the Microscope………15
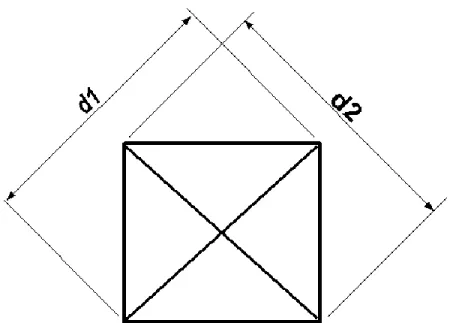
Figure 1.4: Schematic Illustration of the Area of Sloping surface of the Indentation…………...15
Figure 2.1: Bonding Clamp and Bonding Mold Inserts……….27
Figure 2.2: Schematic Illustration of Edge-notched Shear-bond Fixture………..28
Figure 2.3: Specimen Placed on Shear-bond Fixture……….28
Figure 2.4: FM-800 Vickers Micro-hardness tester………...30
Figure 2.5: Mean of Self-adhesive Cement Shear Bond strength per Group………32
Figure 2.6: Mean of Adhesive Cement Shear Bond Strength of per Group………..32
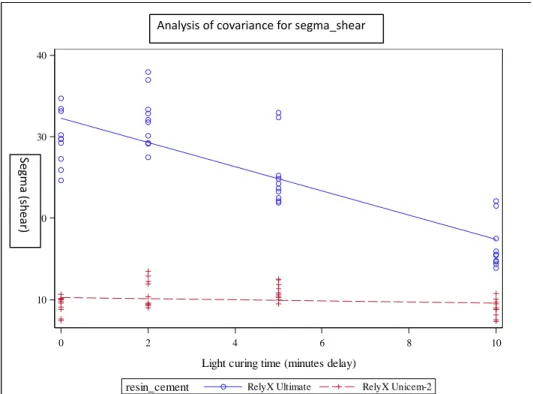
Figure 2.7: Analysis of Covariance for SBS groups………..33
Figure 2.8: Mean of Vickers Micro-hardness Test per Group………...35
LIST OF ABREVIATIONS AND SYMBOLS AB Acid-base cements
ADA American Dental Association Bis-GMA Bisphenol A glycidyl methacrylate C Cementum
cm2 Centimeter(s)
DC Degree of Conversion
D Dentin
DEJ Dentino-enamel Junction
E Enamel
FDP Fixed Dental Prostheses
FEPA Federation of European Producers of Abrasive
GPa Gigapascal HV Vickers Hardness
ISO International Standard Organization
Kgf Kilogram-force mw Megawatt
mm2 Square Millimeter(s) min Minute(s)
MPa MegaPascal N Newton
PFM Porcelain Fused to Metal
RXUl RelyX Ultimate Automix RXUn RelyX Unicem 2 Automix
RMGI Resin Modified Glass Ionomer SUA Scotchbond Universal Adhesive
SBS Shear Bond Strength SD Standard Deviation VHN Vickers Hardness Number
10-MDP 10-methacryloyloxydecyl dihydrogen phosphate 3D Three Dimensional
CHAPTER 1: REVIEW OF THE LITERATURE 1. Introduction
There is no day that passes by in everyday clinical practice that does not involve using or bonding indirect restorations either crowns, veneers, FDPs etc.
The luting cements used in these procedures, that we have available today, are various. Resin cements are divided according to the polymerization methods into three types: self-polymerization, photo-polymerization and dual-polymerization. The use of self-polymerization (also termed auto-polymerizing) cements is not limited by restoration thickness. These cements set (polymerize) uniformly even at the bottom of deep cavities. However, they have shorter working time compared to other cement types. Light-polymerization cements provide control of the time necessary to place/position the restoration, but their use is limited by the access of curing light and the thickness of the restoration. These cements should not be used if the restoration thickness is more than 3 mm, or with opaque restorations.1,2,3
Dual-polymerizing cements combine favorable characteristic of self and light-polymerization.4 These cements undergo polymerization to relatively high degree of conversion
scattering phenomena through thick or opaque restorations because these phenomena and/or conditions limit degree of conversion levels.4,5 They are capable to be polymerized in areas where
the photo polymerizing alone is not possible or limited. For example: Bonding opaque restorations like Zirconia restorations, and or metallic or porcelain fused to metal (PFM) restorations.
Dual-polymerizing resin cements have 2 components: chemical (self) and photo-polymerizing components. The chemical photo-polymerizing component alone is weak, and not enough to reach the maximum physical and mechanical properties. It has been proven that when photo-polymerization step was omitted, some dual-polymerizing resin cements showed inferior hardness (which is an indirect way to measure the degree of conversion).6,7,8,9
On the other hand, there are the photo-polymerizing components which make us always question. If we immediately polymerize, are we going to limit the potential of chemical- polymerizing components to reach to their maximum strength?
It has been shown that some dual-polymerizing cements suffer from self-polymerization inhibition when they immediately photo activated.10
It has been suggested that the early vitrification (polymer network formation) induced by photo activation could interfere with the self- polymerization. Thus, compromising the overall degree of conversion of dual-polymerizing resin cements. 11
There are two different forms of dual-polymerizing resin cements: one is adhesive and the other one is self-adhesive. With adhesive dual-polymerizing resin cements, a separate adhesive agent is required to condition the substrate.
the tooth surface and thus self-adhesion will be provided without a separate conditioner or adhesive application. Self-adhesive dual-polymerizing resin cements require a specific environment for them to work, that is mostly the tooth structure, and the presence of inorganic components like hydroxyapatites. 12,13
A study done by Baena et al., showed that the presence of these acidic functional monomers will cause a significant delayed initial polymerization rate which can deactivate free radicals and compromise the polymerization reaction.12
Although dual-polymerizing resin cements are ideal to use in many restorative procedures, one of the major deficiencies with this material is the lack of understanding for use among most of the clinicians. We need to understand how we can maximize what this cement has to offer for us as bond strength and good mechanical properties. If we understand that, we are going to prolong our Tx and our results. If we do not know how to use the material properly, whatever we have as treatment planned will fail.
Therefore, the main aim from this study was to look at the effect of delaying the photo-polymerization process on the dentin bond strength and the micro-hardness of different dual-polymerizing resin cements for clinically relevant delay times of 2, 5 and 10 minutes as compared with immediate photo-polymerization.
2. Literature Review
Dental enamel is formed by 94-95% inorganic substances, 4-5% organic and 1-4% water. Its main component is enamel rods or what is called enamel prisms. These rods extent from the amelodentinal junction to the external surface of enamel. During the adhesion process, the application of acidic materials acts on the enamel rods and creates 3 different etching patterns. Pattern 1 is found at the core level of the rods. Pattern 2 is found at the periphery of the rods while pattern 3 is a combination of previous patterns. The adhesion in dental enamel using 30-37% phosphoric acid is very reliable because with the presence of high percentage of inorganic substances, the acid results in formation of calcium phosphate and loss of adamantine structures.14
2.1.2. Dental Dentin
Dental detin is porous, wet tissue composed of hydroxyapatite in a collagen protein matrix. It is formed by 50-70% inorganic substances, 20-30% organic substances and 10-20% water. The adhesion in the dental dentin is more complex because of the complexity in its composition. Many factors can affect the adhesion process like: dentinal tubules number and diameter, water content, permeability and physiologic changes. The dental tubules are larger in diameter and greater in density when they are close to the dental pulp compared to dentino-enamal junction (DEJ). Dental caries, sclerosis or aging cause reduction in dentin permeability.14
That is why, mainly, the adhesion in dental dentin is achieved by hybridization and integration process.15
2.2. Adhesion to Teeth Structure
within the same material. That may involve a primary force which is covalent or ionic or a strong secondary force which is hydrogen bonding.
In dentistry, the composition of the substrate, which is either enamel (E), dentin (D) or cementum (C), varies among human teeth. That variation beside the presence of contaminants and water can affect the adhesion process; and, sometimes, make the chemical bonding between the tooth structure and the materials very difficult to achieve.16,17
Figure 1.1: Definitions of The Terminology Associated with Adhesive Systems (Adhesive, Adherends or Substrates and Interfaces). Figure is taken from Craig’s Restorative Dental Materials book.16
2.3. History and Classifications of Dental Cements
Materials that are formed by polymerization of macromolecules, are classified as acid-base cements (AB). Typically, in those materials, the matrix is the most soluble and the weakest component.18 All current cements except for dental resin cements and compomers fall into the AB
category.19
In dental literature, there are many articles and authors discussed classifications of dental cements. Three well-known names in dental materials have used different classification methods. The first author, Ronald L. Sakaguchi, in his book, Restorative Dental Material, classified dental cements according to chief ingredients following the traditional method of classifying cements mentioned above. He divided cements into zinc phosphate, zinc silico-phosphate, zinc oxide-eugenol, zinc polyacrylate, glass-ionomer, and resin.20
The second author, O’Brien, in his book, Dental Materials and their Selection, classified dental cements by matrix bond type into phosphate, phenolate, polycarboxylate, resin, and resin-modified glass-ionomer.21
Lastly, Donovan, in a classic review article classified cements simply based on knowledge and experience of use into conventional and contemporary. The conventional dental cements are zinc phosphate, polycarboxylate, glass- ionomer, while the contemporary dental cements are resin-modified glass-ionomers, and resin.22
2.4. Dental Resin Cements
is successful, the cementation will allow greater fracture resistance, promote stronger bond and inhibit propagation of possible fissures.23, 24, 25
According to polymerization methods, dental resin cements are divided into: self-polymerization (or auto-polymerizing), photo-self-polymerization and dual-self-polymerization.
The self-polymerization cements can be used in cases where the photo-polymerization is not possible such as under opaque and thick restorations or even deep cavities. However, due to their limited working time, most clinicians prefer to use light-polymerization or dual-polymerization cements.1,2,3
Most available resin-based dual-polymerizing cements contain a polymeric matrix of methacrylate monomers, silanated filler particles and photo-initiator components. During polymerization, viscous resin-based materials are transformed to a rigid state by free radical polymerization of variously sized methacrylate monomers. The polymerization reaction involves the conversion of the C=C double bonds, in the monomer methacrylate molecules, to single (primary) C-C covalent bonds resulting in the formation of a polymer chain.26, 27
Due to incomplete reaction of all available C=C bonds, methacrylate restorative materials contain significant amounts of unreacted monomer (~35 %).28 In addition, the formation of the
Before a few years ago, most adhesive systems available were applied in a 3-step or 2-step procedure. Recently, self-adhesive resin cement was developed with a single application step.30
The self-adhesive dual-polymerizing resin cements have added functional acidic monomers. The presence of these monomers beside the dual-polymerizing setting mechanism and the fillers make the self-adhesive resin cements capable of neutralizing the initial low pH of the cement. During setting reaction of the self-adhesive resin cements, the added acidic functional monomers need to be neutralized to prevent compromising polymerization, increased sorption/expansion and lowering overall properties.31
2.5. In vitro evaluation of bond performance
Bond strength tests have been performed a lot in dentistry, in part because they are relatively easy (meaning low technique sensitivity), fast to perform, and not equipment intensive.
Bond strength test methods are: macro-shear test, macro-tensile test, tensile, micro-shear test and push-out test. There are hundreds of studies published on different bond strength tests. They are useful to compare the relative bond strength between 2 or more materials.32
A meta-analysis and systematic review, that was published in 2001, evaluated the influencing factors on bond strength. They defined factors, in a descending order according to statistically-significant importance, as following: dentin depth, crosshead speed, specimen storage time and tooth storage maximum time, bonding area, tooth storage temperature, specimen storage temperature and material stiffness.33
found that thermocycling or artificial aging has an influence on the bond strength. It decreases the bond strength values – both, for micro-tensile and macro-shear tests. They also added that the long-term storage in water can decrease the bond strength significantly if specimens were tested with micro-tensile method but not with the macro-shear test.34
2.5.1. Bond strength Test (Shear test)
In the macro-shear test, a cylindrical shape specimen is built on and bonded to the substrate (enamel or dentin). Then, the specimen is positioned in a universal testing machine and either single-edged chisel, a flat-end rod or a wire loop is used to dislodge the cylinder from the substrate. The typical values with dentin macro-shear bond strength are 10 to 50 MPa. It is very important to note that shear test refers to the loading mode and what actually causes the debonding or interfacial failure in shear test is a tensile stress.35
The major differences between the macro and micro-shear bond strength test are: first, with micro-shear, the cylinder bonded specimen is built using silicone tubes of 0.5 mm in height and 0.7 mm in diameter. The typical bond strength values are about 20 MPa.35
Due to all of these major shortcomings, the micro-shear bond strength test has not been adopted nowadays very well. According to a review done by De Munck, only 7% of bond strength studies, that were published before 2009, have used this method.38,39
2.5.2. Relationship between laboratory and clinical bonding effectiveness
Regarding the correlation between a material’s bond-strength test values and the clinical retention rate of that material, it has been shown by this systematic review and meta-analysis done by Siegward et al., that there is no correlation found between the bond strength results and the retention of cervical restorations.40
On the other hand, in a study done by Van Meerbeek et al.41, a question was asked by the
authors: “can we predict clinical effectiveness in the laboratory?”. It was difficult to answer that question directly, however, the authors pointed out certain associations between laboratory and clinical data on the bonding effectiveness as following:
2.5.2.1. Relationship I
A good correlation coefficient of 0.81 was found between those reported annual failure rates and the shear bond strength data from the “Battle-of-the-Bonds” by Degrange et al.43,44
2.5.2.2. Relationship II
A study by Heintze et al. looked at the correlation between margin analysis data, that was performed in 2 research centers, and artificial clinical index.45
The artificial clinical index consisted of retention loss and marginal integrity (weighted). The results showed weak correlation. The in vitro studies that measured marginal adaptation, had only moderate quality value in term of its ability in prediction the clinical performance of
adhesives used in cervical lesions. The analysis showed great variability in clinical results, however, there was no correlation found between the in vitro methods employed at both research centers.
2.5.2.3. Relationship III
In a more recent study by Heintze et al., authors performed a correlation analysis between the same clinical index mentioned above (in relationship II) and micro-tensile bond strength data. They found, again, no significant correlation between the micro-tensile bond strength data and the clinical index. Also, they could not find any correlation with the clinical retention rate and the marginal integrity. The only significant correlation was between micro-tensile bond strength data when measured after 6-month storage in water, and the marginal discoloration of class V restorations.46
In a review article done by Van Meerbeek et al.47, authors searched for a potential
relationship between bond-strength laboratory data, that was obtained from recently performed reviews 48,49,and clinical retention rates of adhesives in class V lesions collected in the systematic
review.50
In their search, all bond-strength database was used. The data was filtered to include only bond-strength test results that were measured after the specimens had been subjected to some kind of in vitro aging procedure. The class V restoration-retention rates at 2 and 5 years were used. The preliminary results showed no significant correlation between both parameters for the 2-year and the 5-year clinical data. However, there was a strong correlation found between the aged bond-strength data and the 5-year clinical data. They concluded that, from the longer-term (5-years) clinical data, a significant association between in vitro bond strength and the clinical data becomes clear for the complete data set and, also, when all non-aged bond-strength data were excluded.47
2.6. Evaluation of polymerization efficiency (Hardness Test)
Polymerization efficiency (or degree of conversion) in dental resin cements can be assessed by direct and/or indirect methods. Direct methods are complex, expensive and sometimes they are time consuming to use compared to the indirect methods. Polymerization efficiency is measured directly by laser Raman method or infra-red spectroscopy. On the other hand, indirect methods are commonly employed by researchers. Indirect methods include: visual inspection, scraping and surface hardness. It has been proven that surface micro-hardness test acts as an indicator of the degree of conversion and it is correlated well with the infra-red spectroscopy.51 It provides, also, a
There are various methods to measure the hardness of a material. These methods differ by the variation in indenter’s type or indentation dimensions/area and related indentation shape or by the type of the material being tested (hard or soft).
Hardness test can be done by one the following methods: Brinell, Vickers, Rockwell, Knoop, Barcol, Shore A, Nano-hardness.The Vickers hardness test method, which is used in this study, consists of indenting the tested material with a diamond indenter that produces a square indentation. The indentation is in the form of a right pyramid with a square base and an angle of 136 degrees between opposite faces.53
According to the Vickers hardness-test standards (ASTM E384-17) 54, the specimens are
subjected to a full load determined by the type of the material and is normally applied for 10 to 15 seconds (Figure 1.2).
surface of the indentation is calculated (Figure 1.4). The Vickers hardness is obtained by dividing the kgf load by the square mm area of indentation.
(A)
(B)
Figure 1.4: Schematic Illustration of the Area of Sloping surface of the Indentation.
There are many advantages of using the Vickers hardness test. One, just one type of indenter is used for all types of metals and surface treatments. Two, readings are extremely accurate. Third, this method can test the precise hardness of materials under varying loads. The most disadvantage of Vickers machine is that it is a floor standing unit which is more expensive than the Brinell or Rockwell machines.
REFERENCES
1. Platt JA. Resin cements: into the 21st century. Compend Contin Educ Dent 1999. December;20(12):1173–6.
2. Tarle Z, Knezevic A, Demoli N, Meniga A, Sutaloa J, Unterbrink G et al. Comparison of composite curing parameters: effects of light source and curing mode on conversion, temperature rise and polymerization shrinkage. Oper Dent 2006. Mar-Apr;31(2):219–26. 10.2341/05-15.
3. Turp V, Ongul D, Gultekin P, Bultan O, Karataslı B, Pak Tunc E. Polymerization efficiency
of two dual-polymerization cements through dental ceramics. J Istanb Univ Fac Dent. 2015;49(1):10-18. Published 2015 Jan 31. doi:10.17096/jiufd.25575.
4. Faria-E-Silva AL, Pfeifer CS. Delayed photo-activation and addition of thio-urethane: Impact on polymerization kinetics and stress of dual-polymerizationd resin cements. J Dent. 2017;65:101-109.
5. Ilie N, Stawarczyk B. Quantification of the amount of blue light passing through monolithic zirconia with respect to thickness and polymerization conditions. J Prosthet Dent. 2015;113:114–121.
6. Meng X, Yoshida K, Atsuta M. Influence of ceramic thickness on mechanical properties and polymer structure of dual-cured resin luting agents. Dent Mater 2008;24(5):594–9.
7. Chang HS, Kim JW. Early hardness and shear bond strength of dual-polymerizing resin cement light polymerizationd through resin overlays with different dentin layer thicknesses. Oper Dent. 2013.
8. el-Badrawy WA, & el-Mowafy OM (1995) Chemical versus dual curing of resin inlay cements Journal of Prosthetic Dentistry 73(6)515-524.
9. Hasegawa EA, Boyer DB, & Chan DC (1991) Hardening of dual-polymerizationd cements under composite resin inlays Journal of Prosthetic Dentistry 66(2) 187-192.
10. Manso AP, Silva NR, Bonfante EA, Pegoraro TA, Dias RA, Carvalho RM. Cements and adhesives for all-ceramic restorations. Dental Clinics. 2011 Apr 1;55(2):311-32.
11. Goracci C, Cury AH, Cantoro A, Papacchini F, Tay FR, & Ferrari M. Microtensile bond strength and interfacial properties of self-etching and self-adhesive resin cements used to lute composite onlays under different seating forces Journal of Adhesive Dentistry 2006; 8(5) 327-335.
13. Pedreira, Ana Paula Ribeiro do Vale, D'Alpino, Paulo Henrique Perlatti, Pereira, Patrícia Nóbrega Rodrigues, Chaves, Sasha Braun, Wang, Linda, Hilgert, Leandro, & Garcia, Fernanda Cristina Pimentel. Effects of the application techniques of self-adhesive resin cements on the interfacial integrity and bond strength of fiber posts to dentin. Journal of Applied Oral Science, 2016:24(5), 437-446.
14. Abad-Coronel C, Naranjo B, Valdiviezo P. Adhesive Systems Used in Indirect Restorations Cementation: Review of the Literature. Dent J (Basel). 2019 Jul 1;7(3).
15. Migliau, G. Classification review of dental adhesive systems: From the IV generation to the universal type. Ann. Stomatol. 2017, 8, 1.
16. Craig, Robert G., John M. Powers, and Ronald L. Sakaguchi. Craig's Restorative Dental Materials. St. Louis, Mo: Mosby Elsevier, 2012; 273-274.
17. Ritter, A. V., Boushell., L. A., & Walter, R. Sturdevant's art and science of operative dentistry. St. Louis, Mo: Elsevier/Mosby, 2017.
18. Hill EE. Dental cements for definitive luting: a review and practical clinical considerations. Dental Clinics of North America. 2007; 51: 643-658.
19. Wilson AD, Nicholson JW. Acid-base cements, their biomedical and industrial applications. New York: Cambridge University Press; 1993. p. 1–383.
20. Craig, Robert G. Craig's Restorative Dental Materials. St. Louis, Mo: Mosby Elsevier, 1989; 189-225.
21. O’Brien W. Dental materials and their selection. 3rd edition. Chicago: Quintessence; 2002.
p. 133–55.
22. Donovan TE, Cho GC. Contemporary evaluation of dental cements. Compend Contin Educ Dent 1999;20(3):197–219.
23. Passia, N.; Lehmann, F.; Freitag-Wolf, S.; Kern, M. Tensile bond strength of different universal adhesive systems to lithium disilicate ceramic. J. Am. Dent. Assoc. 2015; 146, 729–734.
24. Passos, S.P.; Kimpara, E.T.; Bottino, M.A.; Júnior, S.; Coelho, G.; Rizkalla, A.S. Bond Strength of Different Resin Cement and Ceramic Shades Bonded to Dentin. J. Adhes. Dent. 2013, 15, 461–466.
26. Ferracane, J.L. and E.H. Greener, The effect of resin formulation on the degree of conversion and mechanical properties of dental restorative resins. J Biomed Mater Res, 1986; 20(1): p. 121-31.
27. Van Ende, A., et al., Does a low-shrinking composite induce less stress at the adhesive interface? Dent Mater, 2010. 26(3): p. 215-22.
28. Yap AU, Seneviratne C. Influence of light energy density on effectiveness of composite polymerization. Oper Dent. 2001; 26: 460-466.
29. Aguiar FH, Lazzari CR, Lima DA, Ambrosano GM, Lovadino JR. Effect of light curing tip distance and resin shade on microhardness of a hybrid resin composite. Braz Oral Res. 2005; 19: 302-306.
30. Silva RA, Coutinho M, Cardozo PI, Silva LA, Zorzatto JR. Conventional dual-cure versus self-adhesive resin cements in dentin bond integrity. J Appl Oral Sci. 2011;19(4):355–362.
31. Ferracane, Jack & Stansbury, Jeffrey & Burke, F. Self‐adhesive resin cements–chemistry, properties and clinical considerations. Journal of oral rehabilitation. 2010; 38. 295-314.
32. Ritter, A. V., Boushell., L. A., & Walter, R. Sturdevant's art and science of operative dentistry. St. Louis, Mo: Elsevier/Mosby, 2017.
33. Leloup G, D’Hoore W, Bouter D, Degrange M, Vreven J. Meta-analytical review of factors
involved in dentin adherence. J Dent Res 2001; 80:1605–14.
34. De Munck J, Mine A, Poitevin A, Van Ende A, Cardoso MV, Van Landuyt KL, et al. Meta-analytical review of parameters involved in dentin bonding. J Dent Res 2012; 91:351–7.
35. Craig, Robert G., John M. Powers, and Ronald L. Sakaguchi. Craig's Restorative Dental Materials. St. Louis, Mo: Mosby Elsevier, 2006.
36. Shimada Y, Yamaguchi S, Tagami J. Micro-shear bond strength of dual-cured resin cement to glass ceramics. Dent Mater 2002;18:380–8.
37. Shimada Y, Senawongse P, Harnirattisai C, Burrow MF, Nakaoki Y, Tagami J. Bond strength of two adhesive systems to primary and permanent enamel. Oper Dent 2002; 27:403–9.
38. De Munck J, Peumans M, Poitevin A, Mine A, Van Ende A, Van Meerbeek B. Literature review on factors affecting the bond strength to enamel/dentin. Unpublished observations.
40. Heintze SD, Rousson V, & Mahn E. Bond strength tests of dental adhesive systems and their correlation with the clinical results—A meta-analysis Dental Materials 2015; 31(4) 423-434.
41. Van Meerbeek B, Peumans M, Poitevin A, Mine A, Van Ende A, Neves A. Relationship between bond-strength tests and clinical outcomes. Dent Mater 2010;26: el 00–21.
42. Peumans M, Kanumilli P, De Munck J, Van Landuyt K, Lambrechts P, Van Meerbeek B. Clinical effectiveness of contemporary adhesives: a systematic review of current clinical trials. Dent Mater 2005;21: 864–81.
43. Degrange M, Hitmi L, Bouter D, Gonthier S, Basset F, BIijaoui J. Efficiency of new enamel– dentin bonding systems: assessment by general practitioners. In: Wilson NHF, Roulet JF, Fuzzi M, editors. Advances in operative dentistry. Quintessence Publishing; 2001. p. 173– 84.
44. Degrange M, Lapostolle B. L’expérience des batailles des adhésifs. L’Information Dentaire
2007;89:112–8.
45. Heintze SD, Blunck U, Göhring TN, Rousson V. Marginal adaptation in vitro and clinical outcome of Class V restorations. Dent Mater 2009;25:605–20.
46. Heintze SD, Chaiyasri T, Armstrong SR, Rousson V. Correlation of micro-tensile bond strength data and clinical outcome of Class V restorations. Ivoclar-Vidavent, Chulalongkorn University Bangkok, The University of Iowa, University of Lausanne, Unpublished data.
47. Van Meerbeek B, Peumans M, Poitevin A, Mine A, Van Ende A, Neves A, et al. Relationship between bond-strength tests and clinical outcomes. Dent Mater 2010;26:e100– 21.
48. De Munck J, Mine A, Poitevin A, Van Ende A, Van Meerbeek G. Testing bond strength. A review of the literature. In: Academy of Dental Materials 2009 Abstract.
49. Peumans M, Kanumilli P, De Munck J, Van Landuyt K, Lambrechts P, Van Meerbeek B. Clinical effectiveness of contemporary adhesives: a systematic review of current clinical trials. Dent Mater 2005;21:864–81.
50. Peumans M, De Munck J, Mine A, Van Meerbeek B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. Dent Mater 2014;30:1089-1103.
51. F. H. B. Aguiar, A. Braceiro, D. A. N. L. Lima, G. M. B. Ambrosano, and J. R. Lovadino, “Effect of light curing modes and light curing time on the microhardness of a hybrid composite resin,” Journal of Contemporary Dental Practice, vol. 8, no. 6, pp18, 2007.
53. Craig, Robert G., John M. Powers, and Ronald L. Sakaguchi. Craig's Restorative Dental Materials. St. Louis, Mo: Mosby Elsevier, 2011; p75-78.
CHAPTER 2: MANUSCRIPT
1. Introduction:
Today, resin-based cements are widely used in restorative dentistry especially for cementation of indirect restorations.1 Resin cements are desirable because of their high bond strength to etchable ceramic indirect restorations, low solubility, superior mechanical properties and good esthetics. In addition, strong adhesion (mechanical and/or chemical, depending on the resin) to the intaglio surface of the restoration has resulted in long-term fracture and fatigue resistance in the oral environment.2,3
The development of dual-polymerized resin cements was to achieve optimal polymerization, even when photo polymerization is blocked or attenuated by the indirect restorations. Some studies have evaluated the properties of dual-polymerized cements with and without photo-polymerization. The results showed that most dual-polymerized cements demonstrate inferior hardness (an indirect assessment of degree of conversion with dependence on other properties such as filler load) when photo-polymerization process is omitted.4,5,6,7
Meng et al.,8 reported poor microhardness of dual-polymerized resin cements when they
Adhesive and self-adhesive dual-polymerized resin cements are utilized more frequently nowadays among clinicians because of their simplicity in application. The main difference between the two types of cements the fact that self-adhesive resin cements have added functional acidic monomers that offer a reasonable degree of adhesion to dentin.9 Baena et al.,10concluded
that the presence of acidic functional monomers in self-adhesive resin cements can deactivate free radicals and compromise the curing reaction. Thus, compromising the overall degree of monomers conversion of self-adhesive cements. This is an important issue when considering the use of this material versus conventional adhesive resin cement.
Not all dual-polymerized resin cements polymerize adequately in every clinical situation. Some of the dual-polymerized cements can suffer from self-polymerization inhibition if immediately photo polymerized.11 It was recommended based on theories that
photo-polymerization should be delayed as much as possible (5-10 minutes after mixing), in order to allow self-polymerization process to start.11
Unfortunately, to the authors knowledge, no published studies have evaluated the effect of delaying photo-polymerization process on bond strength and micro-hardness of the two dual-polymerized resin cements (self-adhesive versus adhesive). Two studies have evaluated the effect of delaying photo-polymerization but have only presented different measurements of the mechanical properties and/or polymerization stress.12,13 Two other studies14,15 have examined
whether delayed photo exposure has an effect on orthodontic bond strength using resin modified glass ionomer (RMGI) cements. The applicability of these studies to the current research question is limited because of the following: 1) The resin component of RMGI materials is very low, being in the range of 18-32 % 16, 2) the substrate tested was either bovine (not human) dentin and 3)
significant difference among time interval groups. It is important to note that photo-polymerization delay of more than 10 minutes is clinically impractical.
Therefore, the aim of this study is to examine the effect of delaying the photo-polymerization process on the dentin shear bond strength and the Vickers microhardness of two different dual-polymerize resin cements for clinically relevant delay times of 2, 5 and 10 minutes as compared with immediate photo-polymerization.
The null hypotheses were that:
1. Delaying photo-polymerization processes yield no significant effect on the shear bond strength of the tested dual polymerizing resin cements.
2. There is no significant effect of delaying photo-polymerization processes on the microhardness of the tested dual-polymerizing resin cements.
2. Materials and Methods
2.1. Materials:
The following materials were used in this study (Table 2.1):
1. Self-adhesive resin cement, RelyX Unicem 2 Automix (RXUn), (3M ESPE, St. Paul, MN, U.S.A).
2. Adhesive resin cement, RelyX Ultimate Automix (RXUl), (3M ESPE, St. Paul, MN, U.S.A).
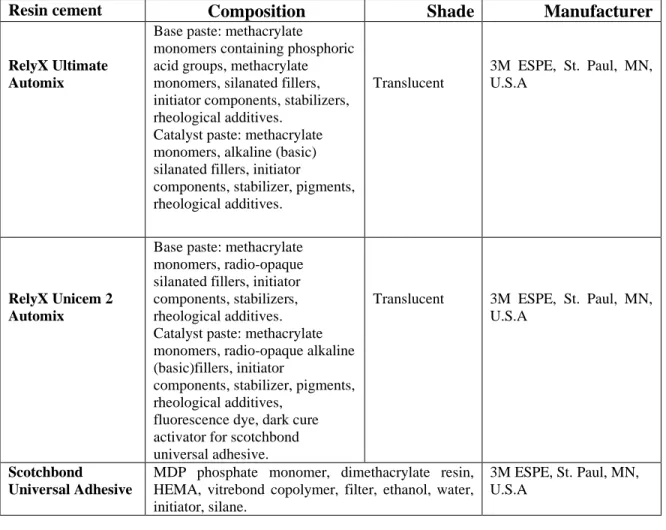
Table 2.1. Materials Used in the Present Study.
Resin cement Composition Shade Manufacturer
RelyX Ultimate Automix
Base paste: methacrylate
monomers containing phosphoric acid groups, methacrylate monomers, silanated fillers, initiator components, stabilizers, rheological additives.
Catalyst paste: methacrylate monomers, alkaline (basic) silanated fillers, initiator
components, stabilizer, pigments, rheological additives.
Translucent
3M ESPE, St. Paul, MN, U.S.A
RelyX Unicem 2 Automix
Base paste: methacrylate monomers, radio-opaque silanated fillers, initiator components, stabilizers, rheological additives. Catalyst paste: methacrylate monomers, radio-opaque alkaline (basic)fillers, initiator
components, stabilizer, pigments, rheological additives,
fluorescence dye, dark cure activator for scotchbond universal adhesive.
Translucent 3M ESPE, St. Paul, MN,
U.S.A
Scotchbond Universal Adhesive
MDP phosphate monomer, dimethacrylate resin, HEMA, vitrebond copolymer, filter, ethanol, water, initiator, silane.
3M ESPE, St. Paul, MN, U.S.A
2.2. Shear-bond Strength Test
The adhesion notched-edge shear bond strength test method was used following (ISO 29022:2013).17
2.2.1. Preparation of Teeth Samples
the absence of enamel and or pulp tissue using a stereomicroscope (3D Medical system) with 40x magnification. A standardized smear layer was then immediately produced by wet sanding with medium grit FEPA P320 silicon carbide paper (46.2 +/- 1.5). Teeth were hydrated throughout the entire experimental process by continuously immersing them in a phosphate buffered salt solution.
The teeth were randomly allocated into 8 experimental groups (n= 10/group) on the basis of type of cements and photo-polymerization time intervals as following:
• Group 1: RXUn + immediate polymerization. • Group 2: RXUn + 2min delay.
• Group 3: RXUn + 5min delay. • Group 4: RXUn + 10min delay.
• Group 5: RXUl + immediate polymerization. • Group 6: RXUl + 2min delay.
• Group 7: RXUl + 5min delay. • Group 8: RXUl + 10min delay. 2.2.2. Preconditioning:
calibrated and confirmed using the MARC Light Collector (BlueLight Analytics, Halifax, Canada) before each use. The specimens were carefully examined after complete polymerization; specimens with voids were excluded from testing.
2.2.3. Insertion into a Bonding Clamp and Cement Placement:
Specimens were inserted into a bonding clamp (Ultradent Products, Utah, USA) containing a white plastics button mold with a hole dimeter of (2,38 +/- 0.03) mm (Figure 2.1). Cement application was carefully applied according to manufacturer’s instructions. The cement was injected, through the plastic hole, to the bonding surface making a cemented cylinder and photo-polymerized according delayed time intervals described above. Specimens with voids or any defects were excluded, and a new specimen was fabricated instead. A small flat end packing instrument was used to remove the bonded sample avoiding “tug back” on the cement. Specimens were stored in water at (37+/- 2) °C for 24h prior to debonding. Specimens were tested immediately after removing from water.
Figure 2.1: Bonding Clamp and Bonding Mold Inserts (From ultradent.com).
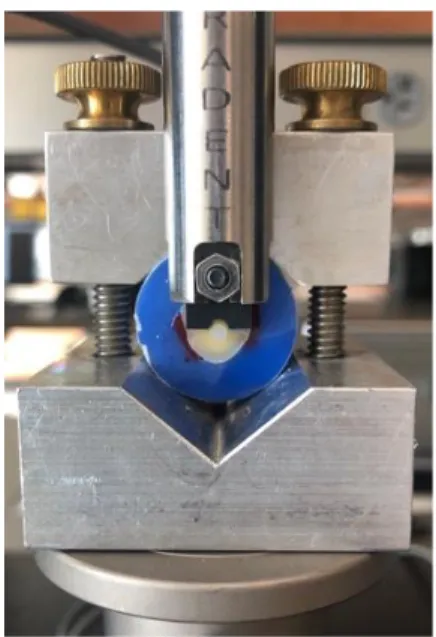
2.2.4. Notched-edge Shear Test
Figure 2.2: Schematic Illustration of Edge-notched Shear-bond Fixture. (from ISO standard 29022). (1) Tooth, (2) Cured potting material, (3) Cured cement button, (4) Cured adhesive
(when adhesive cement was used), (5) Notched-edge shear blade, (6) Test base clamp.
Figure 2.3: Specimen Placed on Shear-bond Fixture.
S= shear stress, expressed in MPa.
F= the maximum force recorded, expressed in N.
Ab= bonding area measured by measuring the diameter of the cement button as near to the bonding surface, expressed in mm2.
The statistical analysis was performed using linear regression to fit a model with explanatory variables for resin cement (categorical), polymerization time (continuous), and their interactions.
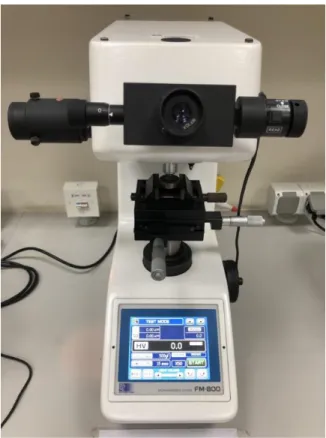
2.3. Vickers Micro-hardness Test
A total of 32 specimens were prepared on the basis of type of cements and photo-polymerization time intervals using a 1mm thick mold. A transparent polyester strip and a glass slide were placed over the cement. Pressure was applied to the glass slide with 100 grams weight for 5 seconds to extrude the excess material. Each specimen was photo-polymerized. The unit was placed 1mm away from the specimen (the thickness of the glass slide) for standardization among specimens.
Vickers microhardness test (HV) was performed following (ASTM E384-17)18
Figure 2.4: FM-800 Vickers Micro-hardness tester.
Each specimen was subjected to a load of 100 grams with a 10 seconds dwell time and 90o angle to the specimen’s surface. The load and the penetration depth of the indenter was continuously measured while loading-unloading the force. For each resin cement specimen, three indentations were performed in 3 different points separated by approximately 0.5mm. The mean value of these testing points was recorded. Specimens were storedin a dark incubator with 37oC and another reading was recorded after 24 hours of their preparation. Vickers Hardness Number (VHN) for each specimen was measured and recorded by the machine’s software using this formula:
A= The depth-sensing instrument.
The measurements were expressed in VHN and the mean and standard deviation for each group were calculated.The statistical analysis was performed using linear regression to fit a model with explanatory variables for resin cement (categorical), polymerization time (continuous), and their interactions. The outcomes of interest are microhardness immediately and after 24 hours of storage. If the interaction was not statistically significant, it was removed from the model. The linear model was refitted using resin cement and curing time only, and we assessed the effect of resin cement and curing time on the outcome separately.
3. Results
3.1. Shear Bond Test
Mean and Standard deviation (SD) values of SBS for each group are provided (Table 2.2). The interaction between resin cement and polymerization time was highly significant (p < 0.0001) suggesting that the effect of photo-polymerization time is different between the two resin cement types (Figure 2.5, Figure 2.6).
Table 2.2. Mean and SD of SBS per Group.
Group
Self-adhesive Cement Adhesive Cement
Immediate (G1) 2min (G2) 5min (G3) 10min (G4) Immediate (G5) 2min (G6) 5min (G7) 10min (G8)
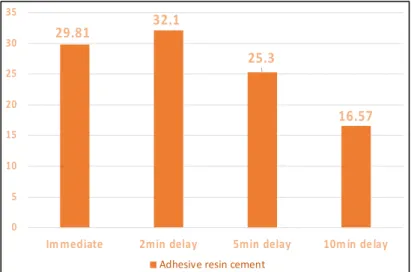
Mean 9.33 10.76 10.99 8.96 29.81 32.10 25.30 16.57
SD 1.02 1.59 1.02 1.09 3.29 3.37 4.04 2.93
Figure 2.5: Mean of Self-adhesive Cement Shear Bond strength per Group.
29.81 32.1 25.3 16.57 0 5 10 15 20 25 30 35
Im mediate 2min delay 5min delay 10m in de lay
Adhesive resin cement
9.33 10.76 10.99 8.96 0 2 4 6 8 10 12
Immediate 2min delay 5min delay 10min delay
Figure 2.7: Analysis of Covariance for SBS groups. 3.2. Vickers Micro-hardness Test
For the immediate outcome, mean and standard deviation values of Vickers microhardness for each group are summarized (Table 2.3), (Figure 2.8). The interaction between resin cement and polymerization time is not significant (p = 0.4414). After refitting the model, photo-polymerization time does not appear to have an effect on microhardness (p = 0.1707). The variable for resin cement type is statistically significant (p<0.0001). The intercepts of the regression lines between photo-polymerization time and immediate microhardness were different for the two types of resin cement, but their slopes did not appear to differ (Figure 2.9).
For the 24-hour storage outcome, mean and standard deviation values of Vickers microhardness for each group are summarized (Table 2.4). The interaction between resin cement and polymerization time is not significant (p = 0.4550). After re-fitting the model, photo-polymerization time does not appear to have an effect on microhardness (p = 0.1808). The variable
Analysis of covariance for segma_shear
0 2 4 6 8 10
Light curing time (minutes delay)
10 20 30 40 si g m a ( sh e e r) RelyX Unicem-2 RelyX Ultimate resin_cement
Analysis of Covariance for sigma_sheer
for resin cement type is statistically significant (p<0.0001). The intercepts of the regression lines between photo-polymerization time and 24 hours microhardness were different for the two types of resin cement, but their slopes did not appear to differ (Figure 2.10).
Table 2.3. Mean and Standard Deviation of Immediate Micro-hardness test per Group
Group Mean SD
SARC
Immediate (G1)
31.73 2.26
2min (G2)
35.78 4.10
5min (G3)
33.39 1.90
10min (G4)
30.02 2.02
ARC
Immediate (G5)
37.60 2.41
2min (G6)
43.16 1.77
5min (G7)
41.58 0.71
10min (G8)
38.49 0.99
Table 2.4. Mean and Standard Deviation of Micro-hardness test After 24h Storage per Group
Group Mean SD
SARC
Immediate (G9)
42.04 4.40
2min (G10)
45.43 3.86
5min (G11)
43.13 3.71
10min (G12)
40.00 4.85
ARC
Immediate (G13)
49.63 3.65
2min (G14)
52.78 2.75
5min (G15)
51.13 1.62
10min (G16)
Figure 2.8: Mean of Vickers Micro-hardness Test per Group.
Figure 2.9: Analysis of Covariance of Immediate Vickers Micro-hardness Outcome. 31.73 35.78 33.39 30.02 37.6 43.16 41.58 38.49 42.04 45.43 43.13 40 49.63 52.78 51.13 49.62 0 10 20 30 40 50 60
Immediate 2 min delay 5 min delay 10min delay
M e an o f m ic ro -h ar d n es s u n it Photo-polymerization time Micro-hardness (MHN)
SARC (immediate) ARC (immediate) SARC (stored) ARC (istored)
0 2 4 6 8 10
Light curing time (minutes delay)
30 35 40 45 Im m ed ia te T es tin g: M ea n U ni ts o f M ic ro ha rd ne ss Unicem Ultimate Material
Figure 2.10: Analysis of Covariance of Vickers Micro-hardness Outcome After 24h storage. 4. Discussion
The effect of delaying photo-polymerization on the dentin SBS and the microhardness of two different types of dual-polymerizing resin cements (adhesive and self-adhesive) was tested in this study. The first null hypothesis was rejected since delaying photo-polymerization processes yielded a statistically significant effect on the dentin shear bond strength of the tested dual-polymerizing resin cements. The second null hypothesis was accepted because although there was a difference in Vickers micro-hardness mean numbers, the difference was not significant.
In this study, the tested materials in all experimental groups had adequate SBS values that ranged from 8.9 MPa to 32.10 MPa. However, a significant finding of this study was the lower bonding ability of the self-adhesive cements (RXUn) in comparing to adhesive cements (RXUl). These results are in an agreement with the findings of many articles in dental literature.19,20,21De
Munck et al.,19assessed the bonding performance of the self-adhesive cement and evaluated the
interaction of the materials used with dentin by SEM.
0 2 4 6 8 10
Light curing time (minutes delay)
35 40 45 50 55 A ft e r 2 4 h w a te r st o ra g e : M e a n U n it s o f M ic ro h a rd n e ss Unicem Ultimate Material
Analysis of Covariance for WaterStorage_Mean
They found that the RelyX Unicem (self-adhesive) cement only interacted superficially with dentin and enamel and the micro-tensile bond strength was significantly lower compared to the tested adhesive cements.19
The most relevant aspects of self-adhesive resin cements and their potential impact on the clinical performance were addressed by Manso et al.20 They confirmed that self-adhesive resin
cements have lower mechanical properties than conventional resin cement. In addition, they are more prone to water sorption which can lead to significant hygroscopic expansion.20 It was
proven that uncured resin or slow self-polymerization can lead to further water sorption.11
Regarding the clinical performance, RelyX Unicem is by far the most investigated self-adhesive product, however, most of the clinical studies available are short-term and not conclusive.20
The SBS results of our study showed a statistically significant interaction between the polymerization time and resin cements. With self-adhesive resin cement, the SBS values were significantly higher when photo-polymerization time was performed between 2 and 5 minutes. When adhesive resin cement (RXUl) was used, the SBS was significantly higher when photo-polymerization was performed within the first two minutes.
Delaying photo-polymerization process to 10 minutes after cement application decreased the dentin SBS significantly with both types of cements. Holderregger et al., showed similar results in their multicenter study where RelyX Unicem exhibited the lowest shear-bond strength to human dentin of all the cements tested when it was left undisturbed for 10 minutes to set and tested in the self-polymerization mode.22 However, to the author’s knowledge, no article has evaluated the
This limitation is due to: 1) the rapid increase in viscosity after setting (acid-base) reaction, and 2) the increase in pH level and buffering components of the dentin smear layer as a result of a neutralization effect and water release during setting. 23,24 The water release at the dentin-cement
interface continues to happen during the polymerization process of the dual-polymerizing self-adhesive cement until all the acidic monomers are saturated25. This phenomenon can alter the bond
durability and hydrolytic stability which have been relevant concerns with the use of adhesive and self-adhesive systems.25
Exposing dual-polymerizing resin cements to different temperature can affect the rate of the degree of conversion and hardness.26Also, it has been proven that all three types of dental resin
cements (chemical-, photo-, and dual-polymerized), appear to be polymerized within the first 24 hours after mixing or after photo-activation without further significant changes in the degree of conversion or microhardness.27,28 Therefore, in this study, we modified on the Vickers
microhardness standards by testing the specimens immediately at room temperature (23°C) and after 24h storage at (37°C) to simulate higher intra-oral temperature.
The Vickers microhardness outcomes of the immediate and after 24h storage testing in this study were comparable. Two minutes delay of photo-polymerization showed the highest Vickers mean numbers followed by 5 minutes delay among all tested groups. Although the interaction between resin cement and polymerization time was not statistically significant, its important to note that there was a difference in their means. Delaying photo-polymerization process to 10 minutes after cement application decreased the Vickers micro-hardness units with both types of cements.
Self-adhesive resin cement yielded statistically significant (p<0.0001) inferior micro-hardness compared to adhesive resin cement. This finding was similar to what was found by Ilie et al., when they concluded that the influence of light on the polymerization process was material dependent. 29
One of the major limitations of this in-vitro study is that it cannot be directly compared to in-vivo conditions. The resin cement was applied and photo-polymerized without the presence of any overlaying restorative material, artificial aging or mechanical fatiguing. The intent of this study was to evaluate the direct effect of delaying photo-polymerization process, disregarding others factors that could potentially affect the interpretation of the results, such as artificial aging or mechanical fatiguing. However, it would be good to see if any of the mentioned factors has an effect on the results of delaying photo-polymerization process. Also, only 2 types of dual-polymerizing resin cements were used in this study. Different brands of dual-dual-polymerizing resin offer various chemical formulations that may result in different properties. Therefore, further research and controlled clinical trials should be conducted before any clinical recommendations can be given.
5. Conclusions
Within the limitations of this in-vitro study, the following conclusions were drawn:
REFERENCES
1. Krämer N, Lohbauer U, Frankenberger R. Adhesive luting of indirect restorations. Am J Dent 2000; 13:60D–76D.
2. Rosenstiel SF, Land MF, Crispin BJ. Dental luting agents: A review of the current literature. J Prosthet Dent 1998; 80(3):280–301.
3. Thompson JY, Stoner BR, Piascik JR, Smith R. Adhesion/cementation to zirconia and other non-silicate ceramics: where are we now? Dent Mater 2011; 27(1):71–82.
4. Chang HS, Kim JW. Early hardness and shear bond strength of dual-polymerizing resin cement light polymerizationd through resin overlays with different dentin layer thicknesses. Oper Dent. 2013.
5. El-Badrawy WA, & El-Mowafy OM (1995) Chemical versus dual curing of resin inlay cements Journal of Prosthetic Dentistry 73(6)515-524.
6. Hasegawa EA, Boyer DB, & Chan DC. Hardening of dual-polymerizationd cements under composite resin inlays Journal of Prosthetic Dentistry 1991; 66(2) 187-192.
7. Goracci C, Cury AH, Cantoro A, Papacchini F, Tay FR, & Ferrari M. Microtensile bond strength and interfacial properties of self-etching and self-adhesive resin cements used to lute composite onlays under different seating forces Journal of Adhesive Dentistry 2006; 8(5) 327-335.
8. Meng X, Yoshida K, & Atsuta M. Influence of ceramic thickness on mechanical properties and polymer structure of dual-cured resin luting agents Dental Materials 2008; 24(5) 594-599.
9. Ferracane JL, Stansbury JW, Burke FJ. Self‐adhesive resin cements–chemistry, properties and clinical considerations. Journal of oral rehabilitation. 2011;38(4):295-314.
10. Baena E, Fuentes MV, Garrido MA, et al. Influence of post-cure time on the micro- hardness of self-adhesive resin cements inside the root canal. Oper Dent 2012; 37(5):548– 56.
11. Manso AP, Silva NR, Bonfante EA, Pegoraro TA, Dias RA, Carvalho RM. Cements and adhesives for all-ceramic restorations. Dental Clinics. 2011; 55(2):311-32.
13. André L. Faria-e-Silva1, Evandro Piva2, Giana S. Lima3, Letícia C. Boaro4, Roberto R. Braga5, Luis R. M. Martins6: Effect of immediate and delayed light activation on the mechanical properties and degree of conversion in dual-cured resin cements. Journal of Oral Science, Vol. 54, No. 3, 261-266, 2012.
14. Komori A, Ishikawa H. The effect of delayed light exposure on bond strength: Light-polymerizationd resin-reinforced glass ionomer cement vs light-Light-polymerizationd resin. Am J Orthod Dentofacial Orthop 1999; 116:139-45.
15. Ando F, Komori A, Kojima I. Tensile bond strength of light-polymerizationd resin-reinforced glass ionomer cement with delayed light exposure. Odontology 2001; 89:45-8.
16. Ikeda, K., et al., Resin content in cement liquids of resin-modified glass ionomers. Dent Mater J, 1999. 18(3): p. 248-58.
17. ISO International Organization for Standardization. ISO 29022:2013. Dentistry-Adhesion -Notched-edge shear bond strength test; 2013-06. Available at: https://www.iso.org/standard/45285.html.
18. ASTM E384 – 17. Standard Test Method for Micro-indentation Hardness of Materials. Book of Standards Volume: 03.01. Available at: https://www.astm.org/Standards/E384.htm.
19. De Munck J, Vargas M, Van Landuyt K, Hikita K, Lambrechts P and Van Meerbeek B: Bonding of an auto-adhesive luting material to enamel and dentin. Dental Materials 2004; 20: 963 – 971.
20. Manso AP, Carvalho RM. Dental Cements for Luting and Bonding Restorations: Self-Adhesive Resin Cements. Dental Clinics. 2017; 61(4):821-34.
21. Hill EE. Dental cements for definitive luting: a review and practical clinical considerations. Dental Clinics. 2007;51(3):643-58.
22. Holderregger C, Sailer I, Schuhmacher C, Schlapfer R, Hammerle C and Fischer J: Shear bond strength of resin cements to human dentin. Dental Materials 2008; 24: 944 – 950. 23. Goracci C, Tavares AU, Fabianelli A, Monticelli F, Raffaelli O, Cardoso PC, Tay F, et al.
The adhesion between ber posts and root canal walls: comparison between microtensile and push-out bond strength measurements. eur J Oral Sci. 2004; 112(4):353-61.
25. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, Van Meerbeek B. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res; 2006; 84:118-132.
26. Oliveira M, Cesar PF, Giannini M, Rueggeberg FA, Rodrigues J, Arrais CA. Effect of temperature on the degree of conversion and working time of dual-cured resin cements exposed to different curing conditions. Oper Dent; 2012; 37:370-9.
27. Rueggeberg FA, Caughman WF. The influence of light exposure on polymerization of dual-cure resin cements. Oper Dent. 1993;18(2):48-55.
28. Yan YL, Kim YK, Kim KH, Kwon TY. Changes in degree of conversion and microhardness of dental resin cements. Oper Dent. 2010;35(2):203-10.