SLEEP DISORDERED BREATHING RISK IN SURGICAL AND EARLY CLASS II CORRECTION ORTHODONTIC POPULATIONS
Ross E. Aronson
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the School of Dentistry
(Orthodontics).
Chapel Hill 2019
ABSTRACT
Ross E. Aronson: Sleep Disordered Breathing Risk in Surgical and Early Class II Correction Orthodontic Populations
(Under the direction of Ceib Phillips, Tate Jackson, and Tung Nguyen)
ACKNOWLEDGEMENTS
Thank you to the members of my thesis committee, Dr. Ceib Phillips, Dr. Tate Jackson, and Dr. Tung Nguyen, for your considerable support, expertise and, insightful direction with the completion of this project and my orthodontic education.
Thank you to Dr. Tanisha Livingston for your incredible work and drive in all doings of this project. Thank you to dental students; Hannah Bodnar and Stephanie Companioni for your invaluable contribution to the completion of these projects through data collection.
Thank you to my classmates who were generous with their time and to the patients who presented to clinic and contributed their energy during a most uncertain and challenging
appointment. Special thank you to my wife, Jacqueline, for her unwavering drive for better. You are an inspiration.
TABLE OF CONTENTS
LIST OF TABLES……… vii
LIST OF FIGURES………..viii
LIST OF ABREVIATIONS………...…ix
INTRODUCTION………...………...1
1. ULTRA LONG TERM RECALL OF A PIVITOL CLASS II TRIAL………...3
1.1 INTRODUCTION………...………...3
1.2 MATERIAL AND METHODS.. …………..……….……….…6
1.3 RESULTS………....8
1.4 DISCUSSION………12
1.5 CONCLUSION…….……….………17
1.6 TABLES AND FIGURES……….18
2. ASSOCIATION BETWEEN DENTAL CHARACTERISTICS AND SLEEP DISORDERED BREATHING IN PATIENTS WITH A DENTOFACIAL DISHARMONY……...…….……...26
2.1INTRODUCTION….……….26
2.2 MATERIALS AND METHODS………...31
2.3 RESULTS….………...33
2.4 DISCUSSION………...
.
...……...………… ……...……..…342.5 CONCLUSION………...…..………37
2.6 TABLES AND FIGURES………..………..………...39
LIST OFTABLES
Long Term Stability of Single vs Two Phase Class II Treatment
1.1: Patient Contact. ………...22
1.2: Changes in Cephalometric Values Through Treatment and to Recall…...23
1.3: Cephalometric Data from Initial Records to Recall…...24
1.4: Physical and Dental Exam Data…...25
Association Between Dental Characteristics and Sleep Disordered Breathing In Patients With A Dentofacial Disharmony 2.1: Median and 95% CI for PSQI and FOSQ Total and Subscale Scores…...39
2.2: PSQI Results by Gender, Race, and Skeletal Class…...40
2.3: FOSQ Results by Gender, Race, and Skeletal Class…...41
\LIST OF FIGURES
Long Term Stability of Single vs Two Phase Class II Treatment
1.1: Cephalometric Superimposition of Initial, Final, and Recall Records of Participant A….………...………18 1.1A: Composite Photographs of Participant A…..………...19 1.2: Cephalometric Superimposition of Initial, Final, and
LIST OF ABREVIATIONS
AHI Apnea Hypopnea Index
BQ Berlin Questionnaire
CPAP Continuous Positive Airway Pressure ESS Epworth Sleepiness Scale
FOSQ Functional Outcomes of Sleep Questionnaire IMPA Incisor to Mandibular Plane Angle
MPA Mandibular Plane Angle
Neck Neck Circumference
OB Overbite
OJ Overjet
1. INTRODUCTION
Sleep disordered breathing (SDB) is a term used to describe a group of syndromes, either individually occurring or concurrent. These include Obstructive sleep apnea (OSA), central sleep apnea, and hypoventilation. These events disturb the sleep and severe fragmentation of the sleep cycle leads to daytime sleepiness due to lack of restful sleep and is concomitant with daytime cognitive dysfunction. If SDB goes undiagnosed and untreated, it can develop into diseases including hypertension, congestive heart failure, neurologic disorders, and cardiopulmonary diseases. Orthodontics by means of both orthopedic and surgical correction has the capacity to improve, impede, or exacerbate SDB1–3. Because of the profound impact that orthodontic
intervention can have on nighttime airway patency and penetrance of SDB, it is essential to understand who in the orthodontic population is at risk, what dental and skeletal factors are associated with risk, and be aware of what treatments might affect SDB. Regardless of the etiology of SDB, the American Dental Association has recommended that dentists screen for signs and symptoms of SDB through history and clinical examination and for risk factors that may lead to airway issues and to refer patients for a medical evaluation when appropriate4.
Questionnaire based screenings with a limited physical exam have been shown to have high sensitivity and clinically acceptable specificity in helping the dentist make a referral to a physician5–8.
breathing and 2) asses the stability of treatment for a Class II skeletal malocclusion across participants treated with early two-phase treatment vs. single later-phase treatment; comparing those treated with a mandibular forward-positioning appliance, or maxillary restraint, or those only observed during their initial phase of treatment.
The specific aims of the second manuscript, Association Between Dental Characteristics and Sleep Disordered Breathing in Patients with a Dentofacial Disharmony , were to 1)
Investigate the association between physical, skeletal, and dental characteristics and sleep disordered breathing in patients with a dentofacial disharmony warranting a
1. ULTRA LONG TERM RECALL OF A PIVOTAL CLASS II TRIAL
1.1 INTRODUCTION
The contemporary practice of orthodontics includes an emphasis on evidence- based care, and the treatment of patients with a skeletal Class II malocclusion during the adolescent growth period is one area where high-level data is available. 9,10 Despite the fact that multiple
randomized clinical trials suggest the superior efficiency of single-phase growth modification treatment, early treatment with headgear or functional appliances continues to remain an area of ongoing research and concern, especially in light of new theories on the interaction of sleep-disordered breathing and craniofacial anatomy and growth 11,12.
At the University of North Carolina (UNC), a two-phased randomized trial was
conducted in which early treatment in growing Class II patients was compared to a consolidated single phase of treatment during the adolescent growth spurt. Final results of the trial showed that any advantage created during an early treatment phase was lost by the end of comprehensive fixed appliance treatment; there were no significant differences across any of the randomized groups in terms of quality of treatment outcome and no advantage to an additional early phase of treatment.
In non-growing adults, mandibular forward positioning appliances are becoming more
commonplace in the treatment of sleep apnea when CPAP cannot be tolerated 2,13. In a growing
child, there could be the potential for lasting impact, positive or otherwise, on airway function when a similar device is used, such as a bionator, in the treatment of a dental or skeletal malocclusion. 14,15 Craniofacial growth continues long after phase two treatment is typically
completed, 16,17 and the effects of growth modification on both anatomic and physiologic
outcomes long-term remain poorly-defined. Orthopedic treatment, whether during two-phase treatment or single-phase treatment, might have an effect on craniofacial morphology and
therefore an effect on sleep- disordered breathing later in life 11,18. Up to this point published data
are of low quality, unclear, and suggestive that either deleterious or even beneficial effects might be gained from orthopedic treatment of Class II patients 19,20.
Similarly, high-quality data are scant regarding any effect of early treatment in terms of the long-term stability of the dental or skeletal correction after two phases of treatment. (21)
Pavlow et al. 2008 found that Peer Assessment Rating (PAR) score at the start of the second phase of treatment had an effect on PAR score at recall 5 years later. That group found that participants with a lower PAR score at the start of Phase 2 were also likely to have a lower PAR score at follow-up21. Since participants who had a Phase 1 of treatment were also more likely to
have a lower PAR score at the start of Phase 2, one might speculate that early treatment led to a more stable result21. The authors were careful to point out, however, that the benefit of early
treatment to stability was not likely to be clinically significant. We lack the data to know if there is a difference in stability with very long-term recall of over 20 years.
phase or two phases of care exist. A secondary aim was to evaluate the prevalence of markers for sleep disordered breathing in these groups.
1.2 MATERIAL AND METHODS
After IRB approval was obtained (16-0958), the patient list from the original Class II trial conducted at the University of North Carolina starting in 1990s was obtained and reviewed 9. 139
total patients who completed both phases of the study are described in Table 1.1.
Information in the patient list included the treatment group (Early Treatment with Headgear, Early Treatment with a Functional Appliance, or Control), complete demographic information, and all of the original treatment-related measures recorded during the study. Names of parents/guardians, historic home addresses, as well as date of birth were used to identify patients and attempt to obtain current contact information.
call who was unable to provide the patient’s contact information, a follow-up call was made three weeks later as needed. For patients who declined to participate in this study, their reason for non-participation was recorded.
After written consent, recall exam included height in inches, weight in pounds, and neck circumference in centimeters. Body mass index (BMI) was calculated from the physical exam data using the NIH online calculator. The intra-oral examination mirrored the original study and consisted of evaluation of the incisors for signs of trauma, including craze lines, enamel
fractures, and restorations secondary to trauma reported by the patient. Molar and Canine Angle classification, overbite (OB), and overjet (OJ) to the nearest mm. Crossbites in the anterior and posterior, as well as Mallampati Score were recorded. A Trios digital scanner (3Shape,
Copenhagen, Denmark) was used to obtain digital study models and bite registration. Intra-oral and extra-oral photographs were obtained and included right profile, right profile smiling, frontal smiling, frontal rest, buccal right and left in centric occlusion, maxillary and mandibular
occlusal, intraoral frontal in occlusion and separated, as well as right and left overjet. Two questionnaires were completed on site, the Epworth Sleepiness Scale and the Berlin Questionnaire to asses’ prevalence of daytime sleepiness. A cephalometric radiograph was obtained with the patient in natural had position. Compensation for participation consisted of a $20 gift card and parking voucher.
of the displacement between the orbital and nasal floors came from the orbit moving superiorly. The mandible was superimposed on the anterior contour just below pogonion as well as the inferior alveolar nerve.
1.3 RESULTS
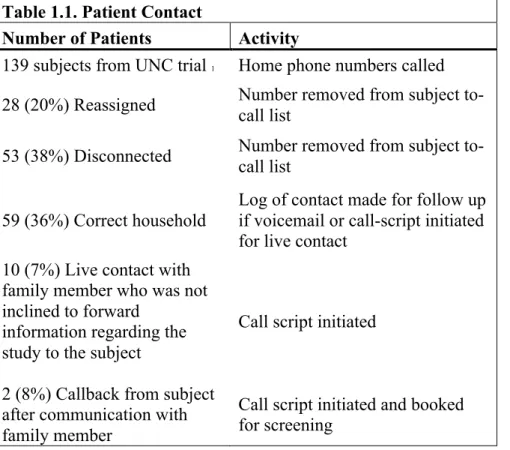
Patients who were treated more than twenty years ago were called using the IRB-approved procedure described above. All of these patients had historic contact information associated with LAN line telephones. 38% of the numbers were disconnected, and another 20% of the numbers had been reassigned to other individuals. 50 of the 139 phone numbers connected us to the correct families and we were able to speak with 12 family members, yielding a contact rate of 36% of the right households and a live contact rate of 8%. Of the 12 families we were able to contact, 10 of the individuals were reported to have moved out of convenient driving distance and that they were not able to participate. Two families had children who still lived in the area and the participants who reached were interested in participating (Table 1.2.).
Summary of Treatment and Long-Term Changes for Participant A
Figures 1.1, 1.1A, Tables 1.2, 1.3 and 1.4
Changes over phase I
After seven and a half months of observation her ANB had decreased by 1.1 degrees, her OJ decreased 6.8mm to 5.3mm and overbite slightly increased from 3.5 to 3.7mm. During this period there was maxillary and mandibular vertical and horizontal growth at all chin points as well as at gonion. Flattening of the occlusal plane occurred. The upper incisors retroclined and there was eruption of the upper molars and incisors. The lower incisors proclined and relative stability of the lower molar. Increase in nasal and pogonial projection, upper lip lengthening and forward movement also occurred. Lower lip and chin had significant forward movement and moderate vertical displacement. (Figure 1.1).
Dental findings at end of phase II
Participant A was then re-randomized for Phase II treatment, at the age of 12 years 1 month, in which both removable (described as a bionator) and fixed appliances were used. Phase II treatment lasted 21 months. At the end of Phase II, her ANB increased by 0.9 degrees to 5 degrees, and her OJ decreased to 2.9mm, her OB remained relatively stable and the upper incisors uprighted by 6.8 degrees. Her MPA remained stable through comprehensive treatment. Table 1.2 and Figure 1.2
Skeletal findings at recall
At long-term recall, the patient was 39.9 years of age. Superimposition (Figure 1.1) reveals long-term changes consistent with vertical skeletal growth, open-rotation of the
pogonial projection is more prominent due to lower lip flattening and the nasal-labial angle became more obtuse.
Dental findings at recall
The patient presented at long term recall with under 1mm of crowding in the upper and lower arch with no incisal trauma to note. Her OJ increased by 1.4mm to 4.3mm. Her upper incisors uprighted by 1 degree and her lower incisors proclined by 4 degrees and her mandibular plane angle rotated open by 2 degrees since completing comprehensive treatment.
Other findings at recall
She reported a history of TMD described as periauricular pain on mastication. She reported wearing a Maxillary full coverage splint at night to reduce damage from nighttime bruxism and TMD related discomfort, and she wears a mandibular Moore retainer.She currently sleeps with a TMD splint of full coverage design, and this increase in vertical dimension and potential posturing could be altering her sleep-time breathing.22 Her PSQI and Berlin scores
revealled no excessive daytime sleepiness and she did not self-report issues with sleep disordered breathing. She has a Malampatti score of II, her height is 5’9” and she weighs 182 lbs. Both her calculated BMI 26.9 (overweight) and neck circumference of 33.5cm put her at lower risk for SDB. An ESS score of 5 which indicates lower normal daytime sleepiness and Berlin
questionnaire score of low risk with no positive categories also point to low risk of SDB.
Subject B
Figures 1.2, 1.2B and 1.4, Table 1.2
Participant B was an 11.5-year-old Caucasian male at the start of the trial. He was randomly assigned to the functional appliance group for the initial phase of treatment, which lasted 14 months. During that treatment period his ANB had decreased by 1.8 degrees. There was an OJ reduction of 6.8mm to an edge-to-edge bite. The mandible and the maxilla grew vertically and anteriorly with a flattening of the palatal plane. The upper incisors had retroclined less than ½ of a degree and the maxillary molar stayed in the same location. The lower dentition had mesialized considerably and his IMPA increased from 100.7 degrees to 106.2.
Findings at end of phase II
Participant B was then re-randomized for Phase II treatment, in which fixed appliances with inter-arch elastics were used. Phase II treatment lasted 22 months. At the end of Phase II, his ANB decreased by 2.2 degrees to 1.3 degrees, and his OJ decreased to 2.6mm from 4.3mm and the upper incisors up righted by 5.2 degrees and the IMPA increased by 3 degrees during comprehensive treatment. The MPA decreased by 2 degrees to 28 degrees. The soft tissue profile straightened considerably at this time with a substantial increase in soft tissue pogonion in the AP dimension.
Skeletal and soft tissue findings at recall
At long-term recall, the patient was 38years and 11 months of age. Superimposition (Figure 3- SI) indicated long-term changes consistent with vertical skeletal growth and
pattern in aging; the nose increased in all dimensions, especially with anterior displacement. Upper and lower lip were more inferior and anterior with the rest of the facial structures and had relative flattening. AP pogonial projection increased significantly. Relative flattening of the profile occurred due to counter clockwise rotation about Nasion, which also moved anteriorly.
Dental findings at recall
At long term recall there was under 1mm of crowding in the upper and lower arch with incisal wear to the dentin on the upper and lower 3-3. Ellis class I trauma was present on the UR1, and U2s and the patient remained in a class I occlusion. His OJ decreased by less than 1mm. His upper incisors proclined by 7.5 degrees to SN but remained within the same
inclination within the maxilla. His lower incisors had very little movement, but the mandibular plane angle closed by 5 degrees since completing comprehensive treatment.
Other findings at recall
Other significant findings at recall included a Mallampati level III pharyngeal soft
tissue relationship. Patient B’s height was 5’8” and weight 285 lbs., giving a BMI index score of 43.3 BMI (obese) along with a Neck circumference 44.4mm. (Table 4). These are significant risk factors for SDB. His ESS score of 6 denotes a higher normal daytime sleepiness risk and a Berlin questionnaire result of high risk of SDB. Additionally, the patient reported using a Continuous Positive Airway Pressure (CPAP) machine nightly due to a diagnosis of OSA, the patient did not recall his pre-treatment Apnea-Hypopnea Index (AHI) and estimated it had been about 5 years since he had started using CPAP therapy. He reported compliance with the device, which was noted as over 4 hours per night 23. No retention appliance use was reported, and patient did not
little orthodontic relapse.
1.4 DISCUSSION
Patient contact difficulty
Of the 166 patients who began the second phase of the original class II trial, 137
completed the second phase of treatment. The timing in which our recall group was treated with regards to changes in technology played a part in our low recall percentage.During the early 1990s the primary contact for a family, other than mailing address, was through the home telephone number. It was not common to request email addresses, as that technology had just started becoming user friendly. Home telephone numbers were often not transferred as readily as they are today. Often, a home telephone number was disconnected and a new one provided when a family moved. This older practice created a challenge recalling these patients. Due to the generational positioning of the recall base the primary method of contact became obsolete since the time of the study.
Additionally, as with any recall-based study, when children move onward into adulthood it is not uncommon for families to move to a smaller home or change locations24,25. Today,
families may keep the same cell-phone or LAN line numbers, but during the late 90s this was not as common. 38% of the numbers contacted were disconnected and an additional 20% were repurposed, meaning 58% of all the families were unable to be reached by phone. Another difficulty was the geographic location of the subjects. Many of the families contacted informed us that over the last 20 or so years they had moved out of a convenient distance to visit the clinic. Despite the limited time commitment and prospect of compensation, the parents of the
their children who lived out of town. We can speculate that their family time is precious, and the parents are not eager to have it divided when the children finally do come to visit. If this study had regular recall intervals following the cessation of treatment, we would have been able to maintain contact with these subjects to a much better degree. Studies which aim to have long term recall may fair better in-patient retention if there are multiple visits in the retention window or otherwise a plan for continual contact until the office visit.
Skeletal Stability
The changes to participant A’s facial skeleton and soft tissues were, with one major exception, remarkably similar to what was observed by Beherent’s in 1984 in his Treatise on the Continuum of Growth in the Aging Craniofacial Skeleton26. The exception from the predicted
normal growth was that her mandibular plane angle did increase during the follow-up period, indicating a different growth pattern during this time than what we saw during treatment. Participant B’s skeletal changes also followed the pattern predicted by Behrents in 1984 26. In
both participants there was a maintenance of their corrected skeletal class II malocclusion into adulthood.
Dental Stability
Patient A’s Maxillary and Mandibular incisors slightly proclined as they often do
for females. Though we do not have final intra-oral films from her treatment, her current
occlusion and alignment are ideal. There is minimal relapse, and this might be due to her
continued use of nighttime retention with a maxillary occlusal splint and what was
retention protocol, which we can only assume is due to wear and lack of maintenance of
the retention appliances, as we would expect her occlusion to remain stable. Her lower
incisor crowding is to be expected and will most likely continue to worsen as she ages 27.
The position of participant B’s upper incisors uprighted during treatment as would
be expected with class II mechanics. Interestingly they returned to his pre-treatment
inclination during his retention period. We would expect the upper incisors to continue to
upright as well as the occlusal plane26. Though his occlusal plane did rotate as expected,
his incisor proclination is unusual along with his increase in NLA which should become
more acute with age26.
OSA and Functional Outcomes
Patient A’s phase one treatment consisted of growth observation and her later
orthodontic treatment involved the use of a Bionator removable functional appliance.
These appliances have been reported to improve mandibular projection when compared
to class II untreated controls, 28 but we cannot say if the use of this appliance mitigated
any potential sleep disordered breathing she would otherwise have had due to her skeletal
relationship. Interestingly, she currently sleeps with a TMD splint of full maxillary
coverage design, and this increase in vertical dimension and potential posturing could be
altering her sleep-time breathing 22Her questionnaire scores revealed no excessive
daytime sleepiness and she did not self- report issues with sleep-disordered breathing.
of comprehensive care. He has maintained a complete dentition, and he is in a class I
angle molar and canine classification and has appropriate incisor coupling and overbite
depth. On both the BQ and the ESS he measured for excessive daytime sleepiness, he is
also at high risk for SDB due to his elevated BMI, 43.3, and neck circumferences,
44.4cm. These findings correlate with the clinical manifestation of OSA as the participant
was diagnosed with obstructive sleep apnea and maintains a current treatment of CPAP
therapy. We cannot know for certain if his increased BMI is completely responsible for
his current SDB or if orthodontics had any role in his current state. Certain facial
characteristics are more prevalent in those with SDB, excessively long faces as well as
over closed patterns like subject B 15,29. In particular, a recent study of 252 persons, who
had undergone PSG, indicated that individuals with a class II pattern with a decreased
facial height had an increased AHI compared to other skeletal classes and facial heights
30.
Comorbidities
From this case study approach we are not able to extrapolate that early
treatment, or lack of, has any association with oropharyngeal airway or
temporomandibular joint comorbidities31. Common thinking would not suggest that the
subject who received early functional appliance treatment to posture the mandible
forward now should have OSA and that our growth modification control group
participant would have TMD issues. Obviously, these comorbidities are multifactorial,
design, we cannot establish any temporality.
Biases
Those who are willing to present for a study may be more organized and able to
take the time to present for a study32. Additionally, those willing to participate may be
more pleased with their current occlusion. Ultimately in this case study we did not
attempt to gather anything other than observational data in order to generate a hypothesis
for a larger scale study on stability and upper airway function. There is profound
difficulty in recalling patients of this generation and we have quite a small sample size as
a result. With a larger sample size, we could provide more than observations regarding
the effects of two-phase treatment on dental and skeletal stability and sleep disordered
breathing. It would be interesting to see if two phase treatment can provide a difference in
stability compared to a single phase of treatment and if the first, orthopedic, phase has
long term ramifications on the upper airway and ultimately SDB.
1.5 CONCLUSIONS
These are just two subjects out of a clinical trial where 139 subjects completed
both phases of treatment. Both subjects were randomized, and we were fortunate to be
able to recall a subject from both the control and early treatment group. Both of the
subjects had a comorbidity associated with the joint or airway while one had two phase
treatment and the other, a single comprehensive phase. We simply don’t have enough
two-phase treatment compared to single phase treatment on dental and skeletal stability
1.6 TABLES AND FIGURES
Figure 1.1.
Figure 1.2B Composite Photographs of Patient B Figure 1.2.
Table 1.1. Patient Contact
Number of Patients Activity
139 subjects from UNC trial 1 Home phone numbers called
28 (20%) Reassigned Number removed from subject to-call list
53 (38%) Disconnected Number removed from subject to-call list
59 (36%) Correct household
Log of contact made for follow up if voicemail or call-script initiated for live contact
10 (7%) Live contact with family member who was not inclined to forward
information regarding the study to the subject
Call script initiated
2 (8%) Callback from subject after communication with family member
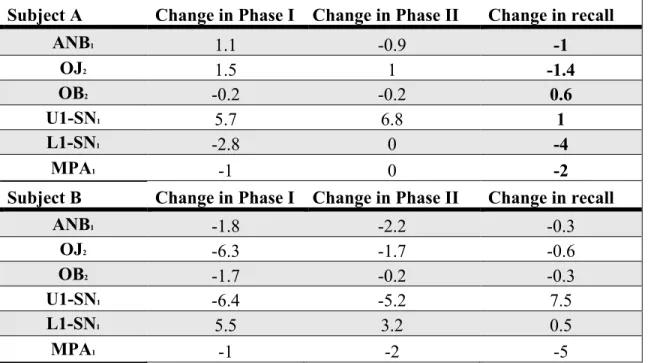
Table 1.2. Changes in Cephalometric Values Through Treatment and Through Recall
1. Degrees 2. Millimeters
Subject A Change in Phase I Change in Phase II Change in recall
ANB1 1.1 -0.9 -1
OJ2 1.5 1 -1.4
OB2 -0.2 -0.2 0.6
U1-SN1 5.7 6.8 1
L1-SN1 -2.8 0 -4
MPA1 -1 0 -2
Subject B Change in Phase I Change in Phase II Change in recall
ANB1 -1.8 -2.2 -0.3
OJ2 -6.3 -1.7 -0.6
OB2 -1.7 -0.2 -0.3
U1-SN1 -6.4 -5.2 7.5
L1-SN1 5.5 3.2 0.5
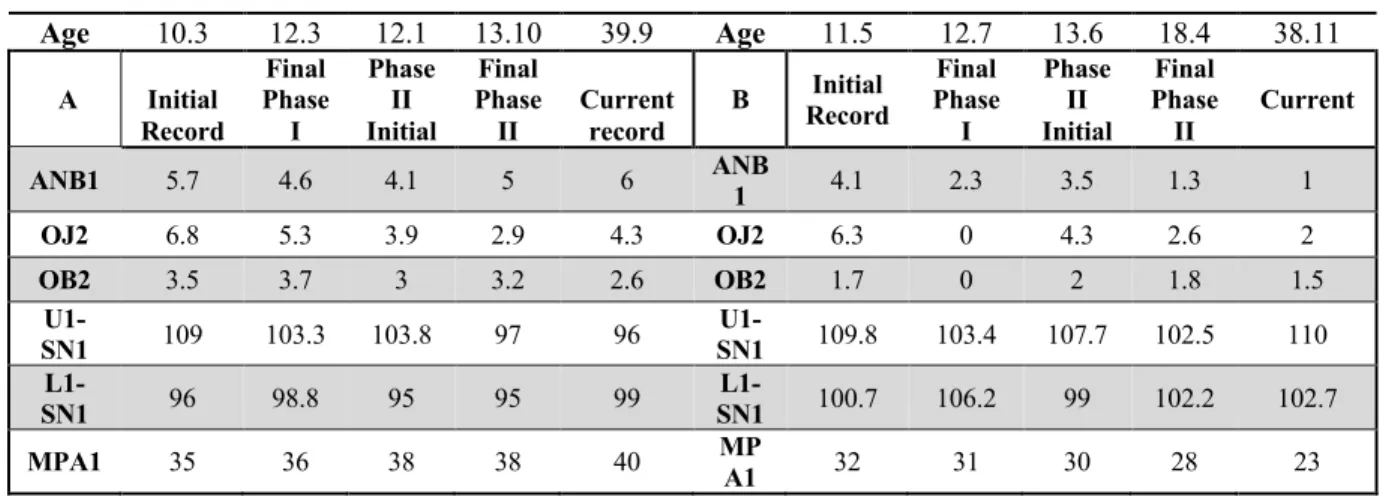
Table 1.3. Cephalometric Data from Initial Records to Recall
Age 10.3 12.3 12.1 13.10 39.9 Age 11.5 12.7 13.6 18.4 38.11
A Initial
Record Final Phase I Phase II Initial Final Phase II Current record
B Record Initial Phase Final I Phase II Initial Final Phase II Current
ANB1 5.7 4.6 4.1 5 6 ANB1 4.1 2.3 3.5 1.3 1
OJ2 6.8 5.3 3.9 2.9 4.3 OJ2 6.3 0 4.3 2.6 2
OB2 3.5 3.7 3 3.2 2.6 OB2 1.7 0 2 1.8 1.5
U1-SN1 109 103.3 103.8 97 96 SN1 U1- 109.8 103.4 107.7 102.5 110
L1-SN1 96 98.8 95 95 99 SN1 L1- 100.7 106.2 99 102.2 102.7
MPA1 35 36 38 38 40 MPA1 32 31 30 28 23
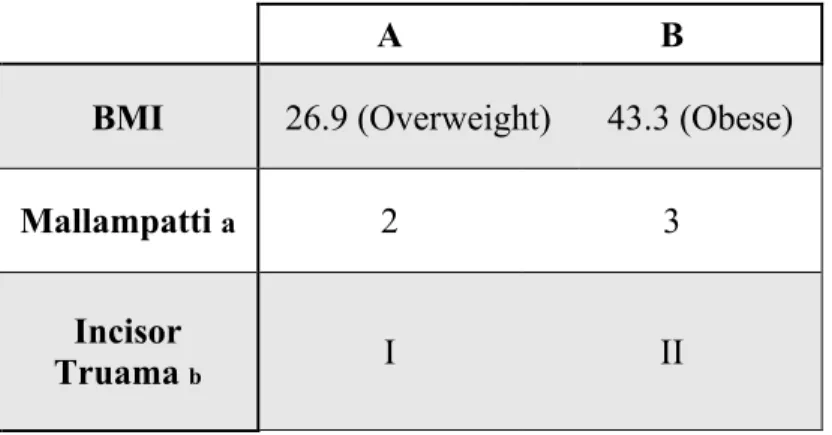
Table 1.4. Physical and Dental Exam Data
A B
BMI 26.9 (Overweight) 43.3 (Obese)
Mallampatti a 2 3
Incisor
Truama b I II
a) Mallampstti score 1-4 in upright position with oral cavity at eye level. Score of 1 indicates complete visualization of soft palate b) Ellis classification 0 through 7
2. ASSOCIATION BETWEEN DENTAL CHARACTERISTICS AND SLEEP DISORDERED BREATHING IN PATIENTS WITH A DENTOFACIAL DISHARMONY
2.1 INTRODUCTION
Background: Multiple publications have suggested an association between dental / craniofacial characteristics and sleep disordered breathing (SDB). There is little data on the prevalence of SDB and the dental and physical characteristics in association to SDB in an ortho-surgical population. The purpose of this study was to investigate the association between dental characteristics and sleep disordered breathing in patients with a dentofacial disharmony. Methods: 137 subjects between the ages of 12 and 60 who had a skeletal or dentofacial
disharmony severe enough to warrant a referral for orthognathic surgery workup were invited to participate. Subjects were identified among the list of patients in Dentofacial Deformities (DFD) and Craniofacial Clinics prior to surgery. The physical exam consisted of measurements of the subjects' weight, height, and neck circumference. BMI index measurements were then calculated for each subject. Intraoral measurements included dental classification, Overjet (OJ) and
Overbite (OB) measured in millimeters. The skeletal classification was determined from lateral cephalograms. Subjects were then asked to complete two self- administered validated
questionnaires the Functional Outcomes of Sleep Questionnaire (FOSQ) and the Pittsburg Sleep Quality Index (PSQI) to determine their perception of their sleep quality and effects of sleep on daily activities. Total scores and clinical screening criteria were calculated for each
Results: Of the 140 subjects, 59% were female and the average age was 18.4 (Sd = 67.2). 10% of the subjects were Class I, 30% Class II, and 59% Class III. The average overjet was 1.3mm (SD = 5.68) and overbite was 1.25 (SD = 3.74). Sixty-three percent self-reported having poor sleep quality and 36% reported poor daily functioning. There were no statistically significant relationships between, characteristics, overjet, , and skeletal class, and the total scores for FOSQ or PSQI or the clinical indicators of poor sleep quality or poor daily functioning. (P>0.05) There was a statistically significant difference in OB between those with good daily functioning and good sleep quality compared to those with poor daily function and poor sleep quality (P<0.05) Conclusion: A substantial proportion of the patients planned to undergo surgical correction of dentofacial deformities reported poor sleep quality prior to surgery. Clinicians should consider the impact of surgery on the airway, especially for patients who report sleep-disordered
breathing.
BACKGROUND
The prevalence of sleep disordered breathing in those presenting with a dentofacial disharmony severe enough to warrant an orthognathic surgery consult has not been well studied. Sleep disordered breathing (SDB) is a term used to describe a group of syndromes, either
individually occurring or concurrent. These include Obstructive Sleep Apnea (OSA), central sleep apnea, and hypoventilation33. The hypoventilation periods during sleep can consist of a
conditions over time if the SDB persists. 35If SDB goes undiagnosed and untreated, the
development of diseases including hypertension, congestive heart failure, neurologic disorders, and cardiopulmonary diseases may result. 36
The overall prevalence of SDB with daytime dysfunction, constituting obstructive sleep apnea syndrome, in the United States is estimated at approximately 5%37. About 4-5% of
children 12 and younger have SDB38 and10% of men and 3% of woman ages 30-49, and 17% of
males and 9% of woman ages 50 to 70 have moderate to severe (AHI >15) SDB39. Using
polysomnography (PSG) data from the Wisconsin sleep cohort study, Peppard et. al. estimated that about 26% of the population ages 30-70 experienced mild to severe SDB (AHI between 5 and 30 events per hour) with the prevalence varying depending on age and gender39,40.
Obesity, as marked by BMI, as well as an enlarged neck circumference are associated with the presence of OSA in certain populations41,8. Increased body weight is theorized to effect
night-time breathing through various mechanisms. The airway geometry is altered by visceral adipose deposits, airway collapsibility increases with excess weight, and additionally there may also be a disturbance in respiratory drive 43,44. There is a lack of boney support in the pharyngeal
airway, which makes it especially prone to both positive and negative pressures that can lead to collapse45,46,47. Neck circumference is an especially important clinical measure and is well
Previous research has indicated that an association exists between skeletal classification, and etiology of the malocclusion and the pharyngeal airway space 48 In a group of 120 adults, a
significantly greater SDB prevalence was observed in those adults with a convex facial profile and a skeletal class II malocclusion most likely due to mandibular retrognathia and subsequent posteriorly placed tongue that limits the airway space 29. A transversely constricted maxilla
which can occur in both class II and III malocclusions are frequently associated with a constricted oropharynx. Expanding the maxilla, whether surgically or non-surgically, and advancing the maxilla have been shown to decrease severity of SDB49,50 Cistulli et al. in 1998
found that surgical and non-surgically assisted rapid palatal expansion (RPE) decreased the average AHI in a group of 10 individuals by more than 50% from an average apnea-hypopnea index (AHI) of 19 to an average of 7. 15Pirelli et al. in 2004 showed that RPE performed on 31
children who had constricted maxillary skeletal bases and no confounding adenoid hypertrophy had an AHI decrease from 12.2 events on average to an AHI of < 1 after four months of
treatment, demonstrating that a constricted maxilla often occurs with OSA and can be a target of treatment49,51. In addition to increasing the width of the maxilla or advancing the
maxilla-mandibular complex, advancing the mandible surgically or orthopedically is an accepted treatment for OSA2,52–54. Advancing the mandible increases airway dimension and reduces
obstruction55. Conversely, it is also accepted that mandibular setback surgeries increase the
likelihood of a patient developing sleep disordered breathing 1,55
Regardless of the etiology of SDB, the patient’s quality of life and systemic health are impacted negatively by the presence of SDB. The American Dental Association has
examination and for risk factors that may lead to airway issues and to refer patients for a medical evaluation when appropriate.11 Questionnaire based screenings with a limited physical exam
have been shown to have high sensitivity and clinically acceptable specificity in helping the dentist make a referral to a physician6,7,56 Given that surgical correction of a severe skeletal
malocclusion or dentofacial disharmony has ramifications on the airway dimension, anatomical locations of respiratory structures and ultimate capacity to breath adequately during sleep3,35,57–59,
the purpose of this study was to assess the prevalence of SDB in patients presenting for an orthognathic surgery consult and to assess associations with clinical measurements.
2.2 MATERIALS AND METHODS Subjects:
This cross-sectional study was approved by the Institutional Review Board at the University of North Carolina at Chapel Hill (IRB 14-1132). Written consent/assent were obtained from all patients as well as the parent or guardian of all enrollees under the age of 18. Individuals between the ages of 12 and 60 years with a dentofacial disharmony who were referred by their orthodontist for an orthognathic surgery treatment consultation were eligible to participate. Individuals with facial trauma, previous facial surgery, repaired or unrepaired cleft lip and palate, prior diagnosis of obstructive sleep apnea or current use of a CPAP machine, and those with the inability to follow verbal and written English instructions were excluded.
Measurements:
measurements were used to record skeletal classification as either I,II, or III. Cephalometric values of ANB as well the differential of A and B points to Nasion-Perpendicular were used. ANB angle of <1 degree was noted as class III ; Class I was between 2-5 degrees, and Class II >5 degrees. The differential of B point to A point to Nasion Perpendicular lines were also measured (Class III > +3mm, Class I < +3 to >-3mm, Class II< -3mm). Skeletal classification was compared to the final surgical workup completed by an orthodontic resident and approved by an orthodontic faculty, any disagreements between examiner RA and the final surgical workup were to be brought to THJ. Angle Classification was recorded as angle class I, II, or III based on molar relationship. Overjet, and overbite were recorded clinically to the nearest millimeter.
Questionnaires:
Participants completed the Functional Outcomes of Sleep Questionnaire (FOSQ) and Pittsburgh Sleep Quality Index (PSQI) questionnaires. The FOSQ consists of thirty items related to a patient’s self-report of sleep quality and functional outcomes of sleep.33,60 These 30 items are
grouped into 5 subscales: Activity Level, Vigilance, General Productivity and Social Outcome. Each item is rated from “extreme difficulty (1)” to “no difficulty (4)” on a 4-point Likert scale. The score for each subscale was calculated as the average of the responses to the items belonging to that dimension; the five scores were subsequently added to produce a total score that ranges from 5-20 with greater scores indicating less effect of sleepiness on daily life.28 The total score
The PSQI consists of 19 self-related questions which assess seven components: Subjective Sleep Quality, Sleep Latency, Sleep Duration, Habitual Sleep Efficiency, Sleep Disturbances, use of Sleeping Medications, and Daytime Dysfunction. Additionally, there are 5 questions rated by the bed partner or roommate (parent) that are not included in the scoring of the PSQI. The scoring for the seven components are described by Buysee et al. in 1989 62.The
seven component scores were summed to yield a total PSQI score, which has a range of 0-21 with lower scores indicating better sleep quality. The total score was categorized as “good sleep quality” (Total < 5) or “poor sleep quality” (total >5)63
Statistical Analysis:
Descriptive statistics and 95% confidence intervals for the median subscale and total scores of the two questionnaires were calculated. Multivariate logistic regression models were fitted to calculate odds ratios (ORs) and 95% confidence intervals (CI) for poor sleep quality and poor daily functioning and was used to assess the relationship of the measurements to the
categorized total scores as indicators of sleep quality and day time sleepiness. Level of statistical significance was set at P<0.05.
2.3 RESULTS
of those with good daily function was 21.5 (IQR; 19.5,26) and was statistically different than those with poor daily function 23.85 (IQR; 20.925.7) (P=0.048). Median BMI was not
statistically different between good (21.79 IQR; 19.6, 26.4) and poor sleepers (2.24 IQR; 20.2, 26.2) (P=0.84). Table 2.1Of the total sample group 64% self-reported having poor sleep quality via PSQI score (95% CI; 55, 71) and 38% reported poor daily functioning via FOSQ score (95% CI; 29, 46).
Table 2.2 and Table 2.3. There were no statistically significant differences with respect to race, gender, or skeletal class between those with good sleep quality and those without or between those with good daily functioning and those without (P >0.21). And the average neck circumference, and age were not statistically significantly different between good and poor-quality sleepers or between good and poor daily functioning (P>0.18). However, overbite was significantly different between those with good daily functioning and those without (P = 0.048) and trended toward a significant difference between those with good sleep quality and those without (P =0.058).
However, OB did differentiate between the skeletal classes and was significantly higher in class II patients and lower in class III patients (P= <0.0001). Median OB was 2mm (IQR; 1,4) in Class I, 5mm (IQR; 1,6) in Class II, and 0mm (IQR; -2,2) in Class IIIs.
2.4 DISCUSSION
In this study, questionnaires and physical exam were used to screen those with a skeletal malocclusion which warranted a referral for an orthognathic surgery workup for increased risk of SDB. The questionnaires used are not surrogates for diagnosis of SDB, which should be obtained by a physician monitored or at-home PSG. However, the PSQI and FOSQ have been shown to have suitable specificity and sensitivity in screening for SDB and were chosen due to ease of use and clinical acceptability in risk assessment8,62,64. Hinz et al. in a community level sample of
9,284 persons, using the PSQI, found that 36% of the respondents reported poor sleep64
compared to 63% of our study sample: our sample had a 75% greater prevalence of SDB. This finding likely reflects the differences in the physical and dental characteristics between this sample’s participants and the general population. Factors generally linked to SRD include age, race, neck circumference, and obesity. This sample has a lower median age, 18.4 vs. 38 years, a lower BMI, 22.41 vs. 26.6, and is composed of more non-white ethnicities than the United States population in 201065. The prevalence of SDB increases with age and BMI33 but this was not so in
our sample. The US population is currently 12.6% African American and 15% non-white ethnicities, while African-Americans composed 26% of this sample and other non-white ethnicities composed 12% of our sample. There is a higher prevalence and increase severity of SDB in African-Americans66,67, and though there was no significant difference in the proportion
of African-Americans as poor functioners or poor quality sleepers47, a higher than normal
quality was higher than the population average. Difference in ventilatory response to hypoxia, and increased peripheral response to hypercapnia, and an increased apneic threshold are proposed mechanisms for the increased prevalence of SDB in African-Americans.67.
Obesity and sleep disordered breathing are correlated in the general population. In a review of the literature, Young et al. described that among 30-69 year old’s who represent the average age, sex, and BMI distributions of the United States in 2003, it is estimated that approximately 17% of adults have mild or worse SDB, and that 41% of those adults have SDB "attributable" to having a body mass index of over 25 (overweight). Additionally, they estimated that of the adults who have moderate or worse SDB that 58% of those persons have SDB
attributable to their excess weight68. There was a statistically significant difference in mean BMI
between good and poor daily functioners, 21.5 vs 23.85 respectively. These Index values are firmly within the same weight grouping, “normal weight” and the magnitude of the difference is relatively small and therefore it’s not clinically significant. However, the directionality of the result is confirmatory and similar to previous findings; an increase in BMI is associated with increased risk of SDB68,69.
Those presenting for a surgical workup at this clinic have craniofacial skeletal morphologies at the extreme of the spectrum, and it would not be surprising that they are at increased risk for SDB as severely deficient maxillae and mandibles could result in similarly deficient airways48,11,70. In the United States 13-15% of adults and youths are skeletally class II
and about 5% are Class III71. This is in stark contrast with our study population, in which 30%
severe skeletal deformity in the sample may well explain why variables such as gender, race, and neck circumference did not function as risk factors for SDB as they do in the general population
4,33,41,47.
Overbite was the only clinical variable associated with sleep quality and daily function: the odds of poor sleep quality and daily functioning increased as overbite depth decreased. This is in contrast to studies in the general population which found that short face height and deep overbite were associated with SDB30. Although skeletal class was not significant, Class III
patients in this study were more likely to have shallower overbites. It may be that in a class III population, deeper OB is a product of more counter-clockwise rotation of the mandible, which may be prognathic to begin with, and this combination of positions (forward with counter-clockwise rotation) is associated with increasing airway volume 72.
Further research is needed on the etiology of the skeletal classification (e.g. mandibular
prognathic vs. maxillary deficiency for a skeletal Class III) as skeletal deficiencies may be more associated with SDB than excess48,57. Because this study used two dimensional lateral
cephalograms, no information was available on the transverse dimension, and it has been shown that the width of the maxilla correlates to the width of the upper airway and SDB50–52.
Information on the vertical dimension and hyoid bone positioning in this sample was not collected and could provide further valuable insight. Though the use of questionnaires has significant clinical applicability and ease of use clinical practice, confirmatory PSG data was not obtained on these patients.
3.5 CONCLUSION
There was an increased prevalence of SDB in this patient population presenting for orthognathic surgery consultation. This population does not represent the general population in the proportion of racial makeup or skeletal classification and presents with different key
2.6 TABLES AND FIGURES
Table 2.1 Median and 95% CI for PSQI and FOSQ Total and Subscale Scores
PSQI Median Score Lower 95% CI Upper 95% CI
Global 5 5 6
Component 1 1 1 1
Component 2 1 1 1
Component 3 0 0 1
Component 4 0 0 0
Component 5 1 1 1
Component 6 0 0 0
Component 7 1 1 1
FOSQ
Total Score 18.6 18.3 19.8
Vigilance 3.6 3.6 3.8
Activity Level 3.6 3.5 3.7
Social Outcome 4 4 4
General
Table 2.2. PSQI Results by Gender, Race, and Skeletal Class
Poor Sleeper Good Sleeper
N % N % P Value
Gender F 49 56.32 F 38 43.68 0.99
Race
White 54 63 35 68.63 0.43
Black/Other 34 37 48 33
Skeletal
Class
1 11 12.5 2 3.92 0.24
2 26 29.55 15 29.41
3 51 57.95 34 66.67
Median IQR (P25,P75) Median IQR (P25,P75) P Value
Neck 1 33.6 32.0, 37.9 34 31.9, 38.0 0.83
Age 2 17 15, 20 16 14, 19 0.99
Overjet1 0 -2.5, 5.5 0 -2, 5 0.52
Overbite 1 1 -2.0, -3.0 2 0, 5 0.058
BMI 3 22.64 20.2, 26.2 21.79 19.6, 26.4 0.84
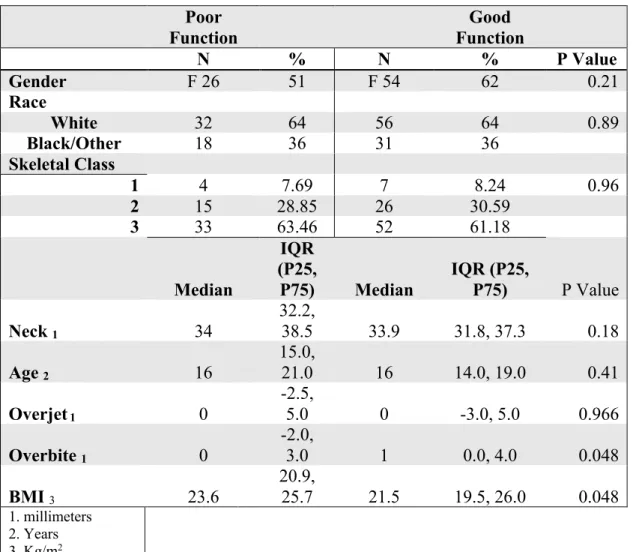
Table 2.3. FOSQ Results by Gender, Race, and Skeletal Class Poor Function Good Function
N % N % P Value
Gender F 26 51 F 54 62 0.21
Race
White 32 64 56 64 0.89
Black/Other 18 36 31 36
Skeletal Class
1 4 7.69 7 8.24 0.96
2 15 28.85 26 30.59
3 33 63.46 52 61.18
Median
IQR (P25,
P75) Median
IQR (P25,
P75) P Value
Neck 1 34
32.2,
38.5 33.9 31.8, 37.3 0.18
Age 2 16
15.0,
21.0 16 14.0, 19.0 0.41
Overjet1 0
-2.5,
5.0 0 -3.0, 5.0 0.966
Overbite 1 0
-2.0,
3.0 1 0.0, 4.0 0.048
BMI 3 23.6
20.9,
25.7 21.5 19.5, 26.0 0.048 1. millimeters
Table 2.4 Analysis of Effects of Sleep Quality and Daily Function
PSQI FOSQ
Type 3 Analysis of Effects
Effect DF
Wald Chi-Square
Pr > ChiSq Effect
DF
Wald Chi-Square
Pr > ChiSq
Neck 1 0.003 0.96 Neck 1 0.08 0.77
Age 1 0.56 0.45 Age 1 1.33 0.25
BMI 1 0.1 0.75 BMI 1 2.23 0.14
OK 1 0.65 0.42 OJ 1 0.34 0.56
OB 1 5.23 0.02 OB 1 4.11 0.04
Skel. Class 2 2.47 0.29 Skel.
Class 2 0.03 0.99
Overbite Good Sleep Quality
REFERENCES
1. Riley RW, Powell NB, Li KK, Troell RJ, Guilleminault C. Surgery and obstructive sleep apnea: Long-term clinical outcomes. Otolaryngol Neck Surg. 2000.
doi:10.1067/mhn.2000.102117
2. Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015. J Clin Sleep Med. 2015;11(7):773-827. doi:10.5664/jcsm.4858
3. Mattos CT, Vilani GNL, Sant’Anna EF, Ruellas ACO, Maia LC. Effects of orthognathic surgery on oropharyngeal airway: A meta-analysis. Int J Oral Maxillofac Surg. 2011. doi:10.1016/j.ijom.2011.06.020
4. Pang KP, Terris DJ. Screening for obstructive sleep apnea: an evidence-based analysis. AmJ Otolaryngol. 2006.
5. Buysse, DJ, Reynolds CF, Monk TH, Berman SR KD. Pittsburgh Sleep Quality Index ( PSQI ). Psychiatry Res. 1989. doi:10.1007/978-1-4419-9893-4
6. Chung F, Yegneswaran B, Liao P, et al. Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology. 2008;108(5):822-830.
doi:10.1097/ALN.0b013e31816d91b5
7. Nishiyama T, Mizuno T, Kojima M, et al. Criterion validity of the Pittsburgh Sleep Quality Index and Epworth Sleepiness Scale for the diagnosis of sleep disorders. Sleep Med. 2014;15(4):422-429. doi:10.1016/j.sleep.2013.12.015
8. Omachi TA. Measures of sleep in rheumatologic diseases: Epworth Sleepiness Scale (ESS), Functional Outcome of Sleep Questionnaire (FOSQ), Insomnia Severity Index (ISI), and Pittsburgh Sleep Quality Index (PSQI). Arthritis Care Res. 2011.
doi:10.1002/acr.20544
9. Tulloch JF, Phillips C, Koch G, Proffit WR. The effect of early intervention on skeletal pattern in Class II malocclusion: a randomized clinical trial. Am J Orthod Dentofacial
Orthop. 1997;111(4):391-400. doi:10.1016/S0889-5406(97)80021-2
10. Tulloch JFC, Proffit WR, Phillips C. Outcomes in a 2-phase randomized clinical trial of early class II treatment. Am J Orthod Dentofac Orthop. 2004;125(6):657-667.
doi:10.1016/j.ajodo.2004.02.008
11. Ikävalko T, Närhi M, Lakka T, et al. Lateral facial profile may reveal the risk for sleep disordered breathing in children-The PANIC-study. Acta Odontol Scand. 2015;73(7):550-555. doi:10.3109/00016357.2014.997795
treatment with headgear: a systematic review and meta-analysis. Eur J Orthod. 2017;39(2):176-187. doi:10.1093/ejo/cjw041
13. Medicine AOSATF of the AA of S. Clinical Guideline for the Evaluation, Management and Long-term Care of Obstructive Sleep Apnea in Adults. J Clin Sleep Med.
2009;5(3):263-276. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2699173/.
14. Julku J, Pirilä-Parkkinen K, Pirttiniemi P. Airway and hard tissue dimensions in children treated with early and later timed cervical headgear-a randomized controlled trial. Eur J Orthod. 2018;40(3):285-295. doi:10.1093/ejo/cjx088
15. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004.
16. Sarnäs K victor, Solow B. Early adult changes in the skeletal and soft-tissue profile. Eur J Orthod. 1980;2(1):1-12. doi:10.1093/ejo/2.1.1
17. Formby WA, Nanda RS, Currier GF. Longitudinal changes in the adult facial profile. Am
J Orthod Dentofac Orthop. 1994;105(5):464-476. doi:10.1016/S0889-5406(94)70007-9
18. Deng J, Gao X. A case-control study of craniofacial features of children with obstructed sleep apnea. Sleep Breath. 2012;16(4):1219-1227. doi:10.1007/s11325-011-0636-4 19. Godt A, Koos B, Hagen H, Göz G. Changes in upper airway width associated with Class
II treatments (headgear vs activator) and different growth patterns. Angle Orthod. 2011;81(3):440-446. doi:10.2319/090710-525.1
20. Hänggi MP, Teuscher UM, Roos M, Peltomäki TA. Long-term changes in pharyngeal airway dimensions following activator-headgear and fixed appliance treatment. Eur J Orthod. 2008;30(6):598-605. doi:10.1093/ejo/cjn055
21. Pavlow SS, McGorray SP, Taylor MG, Dolce C, King GJ, Wheeler TT. Effect of early treatment on stability of occlusion in patients with Class II malocclusion. Am J Orthod Dentofacial Orthop. 2008;133(2):235-244. doi:10.1016/j.ajodo.2006.02.038
22. Palotie T, Riekki S, Mäkitie A, Bachour A, Arte S, Bäck L. The Effect of mandible advancement splints in mild, moderate, and severe obstructive sleep apnea-the need for sleep registrations during follow up. Eur J Orthod. 2017. doi:10.1093/ejo/cjw068
23. Masa JF, Corral-Peñafiel J. Should use of 4 hours continuous positive airway pressure per night be considered acceptable compliance? Eur Respir J. 2014.
doi:10.1183/09031936.00121514
25. Lowenthal MF. Transition to the Empty Nest. Arch Gen Psychiatry. 1972. doi:10.1001/archpsyc.1972.01750190010003
26. Behrents RG. A TREATISE ON THE CONTINUUM OF GROWTH IN THE AGING
CRANIOFACIAL SKELETON. (VOLUMES I AND II) (ADULT). University of
MICHIGAN; 1984. https://books.google.com/books?id=Yo-XSwAACAAJ. 27. Little RM. Stability and relapse of mandibular anterior alignment: University of
Washington studies. Semin Orthod. 1999. doi:10.1016/S1073-8746(99)80010-3 28. Malta LA, Baccetti T, Franchi L, Faltin K, McNamara JA. Long-term dentoskeletal
effects and facial profile changes induced by bionator therapy. Angle Orthod. 2010;80(1):10-17. doi:10.2319/031609-156.1
29. Banabilh SM, Samsudin AR, Suzina AH, Dinsuhaimi S. Facial profile shape,
malocclusion and palatal morphology in Malay obstructive sleep apnea patients. Angle Orthod. 2010. doi:10.2319/011509-26.1
30. Capistrano A, Cordeiro A, Capelozza Filho L, et al. Facial morphology and obstructive sleep apnea. Dental Press J Orthod. 2015;20(6):60-67. doi:10.1590/2177-6709.20.6.060-067.oar
31. Schell C, Yin RK. Case study as a research method. ERS-RUPRI Conf Explor Rural
Entrep. 2006. doi:10.1177/15222302004003007
32. Coughlin SS. Recall bias in epidemiologic studies. J Clin Epidemiol. 1990. doi:10.1016/0895-4356(90)90060-3
33. Omachi TA, Claman DM, Blanc PD, Eisner MD. Obstructive sleep apnea: a risk factor for work disability. Sleep (Rochester). 2009.
34. Yaffe K, Laffan AM, Harrison SL, et al. Sleep-Disordered Breathing, Hypoxia, and Risk of Mild Cognitive Impairment and Dementia in Older Women. JAMA. 2011.
doi:10.1001/jama.2011.1115
35. Sánchez-de-la-Torre M, Campos-Rodriguez F, Barbé F, et al. Obstructive sleep apnoea and cardiovascular disease. Lancet Respir Med. 2013. doi:10.1016/S2213-2600(12)70051-6
36. Panossian L, Daley J. Sleep-disordered breathing. Continuum (Minneap Minn). 2013. doi:10.1212/01.CON.0000427211.98305.c6
37. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: A population health perspective. Am J Respir Crit Care Med. 2002.
doi:10.1164/rccm.2109080
Thorac Soc. 2008. doi:10.1513/pats.200708-135MG
39. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013. doi:10.1093/aje/kws342 40. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The Occurrence of
Sleep-Disordered Breathing among Middle-Aged Adults. N Engl J Med. 1993. doi:10.1056/NEJM199304293281704
41. Deegan PC, McNicholas WT. Predictive value of clinical features for the obstructive sleep apnoea syndrome. Eur Respir J . 1996;9(1):117-124. doi:10.1183/09031936.96.09010117 42. Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score
indicates a high probability of obstructive sleep apnoea. Br J Anaesth. 2012. doi:10.1093/bja/aes022
43. Strobel RJ, Rosen RC. Obesity and weight loss in obstructive sleep apnea: A critical review. Sleep. 1996. doi:10.1093/sleep/19.2.104
44. Barvaux VA, Aubert G, Rodenstein DO. Weight loss as a treatment for obstructive sleep apnoea. Sleep Med Rev. 2000. doi:10.1053/smrv.2000.0114
45. Malhotra A, White DP. Obstructive sleep apnoea. J Lancet. 2002. doi:10.1016/S0140-6736(02)09464-3
46. Ryan S. Obstructive Sleep Apnea. In: International Encyclopedia of Public Health. ; 2016. doi:10.1016/B978-0-12-803678-5.00311-8
47. AASM Task Force, A., 1999. Sleep – Related Breathing Disorders in Adults :
Recommendations for Syndrome Definition and Measurement Techniques in Clinical Research. SLEEP, 22(5) P 667–689., Almeida, F.R., 2005. Compliance titration and side effects of oral appliances in snoring and obstructive sleep apnea patients., Almeida, F.R. et al., 2009. Effect of a Titration Polysomnogram on Treatment Success with a Mandibular Repositioning Appliance. Journal of Clinical Sleep Medicine, 5(3) P 198–204., et al. Gender Differences in Sleep Apnea: The role of neck circumference. Chest. 2003. doi:10.1145/1041410.1041421
48. Muto T, Yamazaki A, Takeda S. A cephalometric evaluation of the pharyngeal airway space in patients with mandibular retrognathia and prognathia, and normal subjects. Int J Oral Maxillofac Surg. 2008. doi:10.1016/j.ijom.2007.06.020
49. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004. doi:10.1093/sleep/27.4.761
rapid maxillary expansion. Sleep. 1998.
51. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion (RME) for pediatric obstructive sleep apnea: A 12-year follow-up. Sleep Med. 2015.
doi:10.1016/j.sleep.2015.04.012
52. Foltán R, Hoffmannová J, Pavlíková G, et al. The influence of orthognathic surgery on ventilation during sleep. Int J Oral Maxillofac Surg. 2011. doi:10.1016/j.ijom.2010.10.006 53. Marklund M, Verbraecken J, Randerath W. Non-CPAP therapies in obstructive sleep
apnoea: Mandibular advancement device therapy. Eur Respir J. 2012. doi:10.1183/09031936.00144711
54. Boyd SB. Management of Obstructive Sleep Apnea by Maxillomandibular Advancement. Oral Maxillofac Surg Clin North Am. 2009. doi:10.1016/j.coms.2009.09.001
55. Li KK, Powell NB, Riley RW, Troell RJ, Guilleminault C. Long-term results of
maxillomandibular advancement surgery. Sleep Breath. 2000. doi:10.1007/s11325-000-0137-3
56. Thurtell MJ, Bruce BB, Rye DB, Newman NJ, Biousse V. The Berlin questionnaire screens for obstructive sleep apnea in idiopathic intracranial hypertension. J
Neuro-Ophthalmology. 2011;31(4):316-319. doi:10.1097/WNO.0b013e31821a4d54
57. Riley RW, Powell NB, Guilleminault C, Ware W. Obstructive sleep apnea syndrome following surgery for mandibular prognathism. J Oral Maxillofac Surg. 1987.
58. Turnbull NR, Battagel JM. The effects of orthognathic surgery on pharyngeal airway dimensions and quality of sleep. J Orthod. 2000. doi:10.1179/ortho.27.3.235
59. Eggensperger N, Smolka W, Iizuka T. Long-term changes of hyoid bone position and pharyngeal airway size following mandibular setback by sagittal split ramus osteotomy. J Cranio-Maxillofacial Surg. 2005. doi:10.1016/j.jcms.2004.10.004
60. Weaver TE, Laizner AM, Evans LK, et al. An instrument to measure functional status outcomes for disorders of excessive sleepiness. Sleep. 1997. doi:9415942
61. Billings ME, Rosen CL, Auckley D, et al. Psychometric Performance and Responsiveness of the Functional Outcomes of Sleep Questionnaire and Sleep Apnea Quality of Life Index in a Randomized Trial: The HomePAP Study. Sleep. 2014. doi:10.5665/sleep.4262
63. Zhong QY, Gelaye B, Sánchez SE, Williams MA. Psychometric Properties of the Pittsburgh Sleep Quality Index (PSQI) in a Cohort of Peruvian Pregnant Women. J Clin Sleep Med. 2015. doi:10.5664/jcsm.4936
64. Hinz A, Glaesmer H, Brähler E, et al. Sleep quality in the general population:
psychometric properties of the Pittsburgh Sleep Quality Index, derived from a German community sample of 9284 people. Sleep Med. 2017. doi:10.1016/j.sleep.2016.03.008 65. Bureau USC. American Fact Finder. In: American Fact Finder. ; 2013.
66. Ancoli-Israel S, Klauber MR, Stepnowsky C, Estline E, Chinn A, Fell R. Sleep-disordered breathing in African-American elderly. Am J Respir Crit Care Med. 1995.
doi:10.1164/ajrccm.152.6.8520760
67. Pranathiageswaran S, Badr MS, Severson R, Rowley JA. The influence of race on the severity of sleep disordered breathing. J Clin Sleep Med. 2013. doi:10.5664/jcsm.2572 68. Young T, Peppard PE, Taheri S. Excess weight and sleep-disordered breathing. J Appl
Physiol. 2005. doi:10.1152/japplphysiol.00587.2005
69. Skatrud J, Badr S, Palta M, Weber S, Dempsey J, Young T. The Occurrence of Sleep-Disordered Breathing among Middle-Aged Adults. N Engl J Med. 2002.
doi:10.1056/nejm199304293281704
70. Huynh NT, Morton PD, Rompré PH, Papadakis A, Remise C. Associations between sleep-disordered breathing symptoms and facial and dental morphometry, assessed with
screening examinations. Am J Orthod Dentofac Orthop. 2011. doi:10.1016/j.ajodo.2011.03.023
71. Proffit WR, Fields HW ML. Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthodon Orthognath Surg. 1998. doi:10.1186/s12903-017-0414-1
72. Jeong WS, Kim YC, Chung YS, Lee CY, Choi JW. Change in Posterior Pharyngeal Space after Counterclockwise Rotational Orthognathic Surgery for Class II Dentofacial
Deformity Diagnosed with Obstructive Sleep Apnea Based on Cephalometric Analysis. J