Ageing in forensic psychiatric secure settings:
The voice of older patients
Claudio Di Lorito, Tom Dening, and Birgit Vӧllm
Division of Psychiatry and Applied Psychology, School of Medicine University of Nottingham
Corresponding author: Claudio Di Lorito Room A10, Institute of Mental Health University of Nottingham
Triumph Road
Nottingham NG7 2TU
Email: [email protected]
Abstract
Older patients account for around 20% of the population in secure forensic psychiatric services in the UK. However, little qualitative research has investigated the experience of ageing in secure settings. This study aimed to gather the individual views of a sample of patients over 50 years old in the UK at different levels of security. Fifteen participants were selected and underwent one-on-one qualitative interviews. The interviews were analysed through thematic analysis, which generated seven themes: Self-agency, activities, social life, practical matters, recovery, physical health and service improvement. Study findings
highlighted the complexity of ageing in secure settings. Despite the positive feedback
reported in aspects such as physical health care, education opportunities, staff and support of religious practices, participants experienced added barriers to recovery, caused by social isolation/withdrawal and activities/treatment that did not respond to their complex age-related needs, generating poor motivation to engage. Our findings call for the
development/implementation of programmes tailored to the unique needs of older patients. This process requires an active involvement of the primary stakeholders and further patient-centred research.
Keywords: Older patients, forensic psychiatry, old age psychiatry, secure services, qualitative research
EM). The views expressed in this article are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Introduction
Secure forensic mental health services in England and Wales offer specialist/intensive treatment to mentally ill individuals who, given their psychiatric symptoms, may pose a risk of harm to themselves or others.
In the last decade, the number of older patients in UK secure forensic psychiatric settings has increased. In 1995, Wong et al. reported that 8% of the total patients’ population in
Broadmoor Hospital, a high secure hospital in the UK, was over 50 years old. In 2018, the over 50s constitute 21% of the patients in Rampton Hospital, another high secure service (Di Lorito, Dening, & Vӧllm, 2018).
Demographic trends (e.g. longer life-expectancy), more frequent prosecution of historic offences, particularly sexual offences and changes in the legal system (e.g. increased number of lifetime sentences) have caused an accumulation of long-stay and newly admitted older patients in forensic psychiatric care (RECOOP, 2015; Yorston, 2015; Moll, 2013; Frazer, 2003).
The few existing studies on older patients found that they experience complex care needs and long-term institutionalisation which may potentially hinder their recovery (Lightbody, Gow, & Gibb, 2010; Yorston & Taylor, 2009; Shah, 2006; Tomar, Treasden, & Shah, 2005; Curtice, Parker, Wismayer, & Tomison, 2003; Coid, Fazel & Khatan, 2002; Paradis, Broner, Maher, & O’Rourke, 2000). However, this evidence is almost entirely based on staff reports and clinical data, which neglects the views of the patients. We therefore deemed it timely to undertake this patient-centred research.
2014), which places strong emphasis on human agency (Ward, Mann & Gannon, 2007), thus implying an imperative for patient-based research.
Our study aimed to answer the following questions: (i). What is the experience of older patients in forensic psychiatric services? (ii). Are these services meeting their needs? (iii). What can be done to enhance their experience and recovery opportunities?
Methods
This study was part of a larger project on older patients in three forensic psychiatric settings (high, medium and low secure), within Nottinghamshire Healthcare NHS Foundation Trust. The project comprised a quantitative element (Di Lorito, Dening, & Vӧllm, 2018) and a qualitative study around patients’ experience (presented here).
Participants
Inclusion criteria:
1. aged 50 years old or above, in line with current conventions in old age forensic research (Cooney and Braggins, 2010; Baldwin and Leete, 2012; Moll, 2013).
2. been resident in the service for at least one year, to have experience of secure settings. 3. able to give full consent, determined by the researcher.
4. no reasons for not participating identified by the clinical team.
Data collection
Study participants were interviewed individually using a semi-structured interview schedule, but new topics that emerged during the session were also explored to ensure that all relevant information was captured. The interview schedule comprised 25 questions including: (i) Likert-type opening prompts to stimulate participants’ reflection and administered orally through an easy-read response sheet; (ii) open-ended questions for further in-depth investigation. It was informed by results from the following pre-study groundwork undertaken by the research team:
(i) Systematic reviews and empirical studies around older forensic populations (Di Lorito, Dening, & Völlm, 2018; Di Lorito, Vӧllm, & Dening, 2018; Di Lorito, Völlm, & Dening, 2017; Di Lorito, Castelletti, Tripi, Gandellini, Dening, & Völlm, 2017).
(ii) Review of the NICE guidelines on mental wellbeing and independence in older people (NICE, 2015).
(iii) The primary needs that forensic services should address to promote patients’ recovery, as indicated in the Good Lives Model for offender rehabilitation
(https://www.goodlivesmodel.com/information).
(iv) One Patient and Public Involvement (PPI) exercise carried out with three patients in Rampton Hospital. Through this exercise, we gathered feedback around the interview questions, and edited the schedule to make it more relevant to the patients.
Data analysis
The interviews were transcribed, transferred onto NVivo software Version 11 (QSR International Pty Ltd., 2012) and analysed through thematic analysis, a method for
identifying, analysing and reporting themes within data (Braun & Clarke, 2006). We adopted a semi-deductive approach to thematic analysis, and set some initial themes based on our preliminary groundwork. We examined the transcripts and assessed the fitness of these themes.
Where data did not fit into the existing themes, we would generate a tentative new theme. All themes were expanded, restricted, or merged through a back-and-forth process, until a final code book (Table 1) was agreed upon by the whole research team. Relevant data were then extracted and categorised into the final themes.
Ethical approval and data protection
Ethics approval (REC reference: 16/EM/0505) was obtained by the Health Research Authority (HRA) and permission to run the study by Nottinghamshire Healthcare NHS Foundation Trust Research & Development (R&D). We abided by the Declaration of
Helsinki (World Medical Association, 2013), Good Clinical Practice (GCP), the Department of Health Research Governance Framework for Health and Social Care (Department of Health, 2005) and the Data Protection Act 1998. To safeguard the patients’ anonymity, we did not label any quotation included in this paper (e.g. gender, age of participant).
Results
The initial list of themes (based on our preliminary groundwork) included: Social life, recovery, self-agency, activities and service improvement. The new themes, which emerged from the participants’ interviews were: Practical matters and physical health. We derived seven final themes, each of which included several sub-themes (Table 1). These are discussed below.
Self-agency
The theme of self-agency explored how much in control patients felt in shaping their own present and future. Most patients felt they were in control of some specific practical aspects of daily living:
‘I have control on the little things. I bought myself a couple of dresses, and put on some make
up, just things to put me up a bit’
Others felt that they had decision-making power to shape their own treatment:
‘The OT staff come on the ward and say, ‘We would like you to go on this group’. I think
about it and make a choice’
Participants also acknowledged that relinquishing a degree of control was to be expected within secure units:
‘We have to realise that we are in a secure unit and there are parts of our lives we can’t
change’
However, several patients, perceived that control was totally in the hands of members of staff:
‘I haven’t been in control of my own life since I’ve been locked away. I’ve had people telling
More often, the temporary loss of decision power constituted a ‘necessary evil’ to pursue life goals:
‘This to me is a means to an end and I’ve got to get through this to be where I want’
The notion of control over one’s destiny was linked to envisioning a life outside the
institution. Patients had frequent thoughts about future plans, which often focused on family: ‘I think a lot about the future, because most of my family are aging. And because I’m the
oldest man in the family, I need to look after them’
Future plans also reflected a wish to help others:
‘I would really like to become a drug counsellor. I think my journey put me in a better
position to understand what drug users are going through’
Participants frequently expressed concerns when discussing the future. Some issues related to readjusting to contemporary living:
‘Being out will be so strange after so long. The smallest things like crossing the road is going
to be a massive step’
Others had concerns around employment:
‘I think people wouldn’t employ an older person with mental health issues. I can end up
relying on benefits, rather than having an active job’
Relapse was also a tangible risk, in the absence of round-the-clock care from the clinical team:
‘Because I’ve done it before, my main concern is: Am I going to fall in the wrong again?’
These feelings were prominent among those who risked being moved back to prison, by virtue of their section or because they had a life sentence:
‘If I do all the work, they put a referral to medium security. But once I’ve done all the work in an RSU and I am out, they can lock me back in prison’
Activities
This theme focussed around participants’ feedback around educational/recreational activities and on their suitability for older patients. Participants felt confident that educational activities prepared them to live independently in the community:
‘I find IT classes helpful for when I will be outside. It’s all done through the internet now’
Patients who regularly attended the local library were also satisfied:
‘We got a ward library here, so every Friday we can put our names on the board and go to
the library’
When the hospital resources could not fulfil their educational needs, patients had alternative development opportunities:
‘I’ve done distance learning through Leicester College on equality and diversity and I’m now
nutrition and health’
Leisure activities could also be relaxing and soothing:
‘My artwork, it’s a chill out for me. It takes me to another place’
Physical activities also provided a social role within the community:
‘I got gardening projects starting up. I got plenty to do. I give advice on how to go about in
In addition, such activities promoted outdoor life and contact with nature:
‘When I do horticulture, I really feel I’m all one with nature. It is one of the best things I have
here’
In relation to the age-friendliness of activities, some patients stated that the activity programme was suitable for any age group:
‘It’s targeted to all ages. Take the garden for example, anybody can do something there’
Patients with mobility issues, however, complained about the inaccessibility of activities: ‘I use a wheelchair or a frame to move and most of the activities are not accessible’
Those patients having stayed in services for a long time reported a loss of enthusiasm in a ‘repetitive’ programme of activities:
‘Because I’ve been here an unprecedented amount of time, I’ve done most of the groups and
have lost all my enthusiasm’
Not engaging in activities had a negative impact on social inclusion:
‘In this place you need to occupy your mind and it’s not very helpful if you’re sitting there
alone with a book on your lap’
For this reason, the few activities specifically for the over 50s received positive feedback: ‘I attend the Sage1 group once a month. We go to the OT room and we pick an old film to
watch. It’s so comfortable and relaxing!’
Therefore, most interviewees advocated for a wider implementation of age-relevant initiatives:
‘I’d be happier to see more people together in my age group in social functions or in the
1 The Sage group is a monthly social event in Arnold Lodge. It is dedicated to older patients from across all
wards, who gather to watch a film.
Social life
This theme explored how the participants felt they related with members of staff, peers, and external visitors (e.g. family). Interviewees reported that members of staff exhibited genuine commitment to their emotional wellbeing:
‘You always have somebody to talk to. They are very caring.’
They were able to respond to their individual needs:
‘Some of the patients haven’t got the confidence to ask for support, but they recognise that
and they sit down with them’
Thus, patients often regarded their clinical team almost as extended family and treasured their support:
‘I have applied to get leave and the staff have supported that. It’s important to know that my
clinical team are all behind me’
The patients recognised that attachment was mutual:
‘They have a vested interested to get to know you, cos they also spend most of their life here’
However, some patients felt that the younger members of staff could be insensitive to age-related issues:
‘Some of them do not understand that people over 50 might have different problems and treat
everybody the same’
‘They may have issues with their own mental health. And I could have issues too’
Age difference could also impact on good rapport between patients:
‘A lot of the times the younger lads don’t want you around. And I struggle to have a
conversation with them, because most of their things revolves around computers’
Friendships could end when patients are moved across wards of discharged:
‘People from the other ward, I spent time with them every day for three years. They knew
when I was sad and I knew when I had to cheer them up. So now I am trying to adjust to new
people here’
Some patients, especially those on more settled wards, reported being on good terms with their peers:
‘I think it’s because this is a recovery ward, everybody relates well’
Participants often reported no contact with family:
‘I have not been in contact with my daughter for three years’
Barriers to familial relationships included the practicalities of visits:
‘My mom is very old and she’s had an operation, so she cannot come very often’
Because of the risk for social isolation, befriending schemes were in place:
‘A volunteer visitor visits me every month to talk about things that happen outside’
Interviewees wished further implementation of such initiatives:
‘I think there should be more opportunities of visits from the outside, so people just don’t sit
there alone’
Practical matters
Participants were asked to reflect on the practical aspects of their daily routines, which might impact on their experience in secure care. Food reviews were overall positive, but several patients reported unmet age-related needs:
‘I would appreciate some more food that I can chew. An alternative would be good’
These included feeling uncomfortable to dine in boisterous environments:
‘I rarely go to the dining room to eat, because of the noise. You get a lot of chairs scraping
on the floor, lots of shouting between patients’
Access to the telephone was another area where the older patients reported age-related unmet needs:
‘I can’t stand for a long time to be able to use the phone. And sometimes, it can get pretty late
before I can make a call, so I just miss out’
The hospital shopping arrangements were found to be age-friendly:
‘They give me a shopping sheet, I write down what I want and the porter brings it over in
boxes’
Concerns were reported around the availability of funds. For this reason, all the participants described saving strategies:
‘I try and save each day some pounds in the safe, in the bank and in the room. Today I spent
about £5 and managed to save £15 for the next week and that is how I meet my budget’
There appeared to be some welcome flexibilitywithin the policy that it is allowed to accommodate the needs of partnered patients:
‘I have just got married and when my husband visits me, the staff let us hold hands. I really
appreciate it’
In relation to sexual expression, the patients generally agreed that intimacy on the ward would be inappropriate and could pose a threat to successful rehabilitation:
‘I would view it as inappropriate in a small community, and I think you’ve got to concentrate
on your treatment’
Others reported no sexual needs:
‘I have no worries in that sense. You see, I’m older, so these things don’t matter to me’
Autoeroticism, however, was still relevant for some, who complained that regulations had become stricter over time:
‘We used to receive magazines back then and they helped a lot. We also had a programme
called ‘Sexcetera’ about sexual expression, but they have cancelled it so there’s nothing these
days’
Recovery
This theme explores participants’ views on recovery and on the different elements that impact on it, including spirituality and treatment. One patient provided an eloquent image of
recovery, framed within the metaphor of life as a river:
‘Life’s like a river. The stream is when you set out for the journey. You are confident, nothing
stopping it. Then there’s the waterfall. Suddenly the water has no control of where it’s going,
splashing. That’s when recovery begins, when you wake to the fact. You reflect on what
caused the fall. Each rock represents an issue that caused the fall and as you sort the rocks
out, you let go of the pain from them. That’s when you’ve recovered’
Several elements contributed to success in recovery in the view of participants. Personal commitment was key:
‘You’re not forced to come here. You need to want to come here and you will eventually get
better’
Another relevant factor was support from the community:
‘We have group meetings here, so I can come here and say what’s on my mind and everybody
tries to help me to get around that’
Patients believed that recovery was also linked with quality of life. Although most patients spoke well of certain aspects of treatment, such as the staff and activities, they overall did not think of themselves as having great quality of life:
‘It’s not life, it’s more of an existence. You just get on with your routine, day in and day out’
It was further affected by long stay:
‘When you talk about someone being locked up for this amount of time, it’s utterly
horrendous’
Systemic aspects of secure settings such as restrictiveness, also caused poor quality of life: ‘Limitations of what you can do here have a great impact on quality of life. I’ve always been
an outdoor person and now I’m stuck in here’
‘Being in the church, makes you feel contended and relaxed. No punishing there’
Spirituality also gave the patients hope for the future: ‘It gives me a feeling that I will get free one day’
Religious practices promoted a sense of community:
‘You sit with the staff, other patients and the padre…you’re all equal in the eyes of God’
Pastoral care was considered akin to talking therapy:
‘The chaplain came today. I told him the full story of the psychotic incident and he gave me
support’
Given the benefits for the patients, the services were very supportive of any spiritual practice: ‘I don’t go to church cos it’s quite a walk, but I have on ward communion. We also get an
Imam, who comes here and a prayer room’
Treatment was another core element of recovery. Very positive feedback was reported around treatment groups:
‘We have groups on alcohol, violence, drugs, and relationships. There’s always a group for
each person’s needs’
Participants offered new insight into personal issues:
‘You get a different perspective form the staff and from the other peers’
However, the benefits of treatment did not end with group sessions:
‘I have weekly sessions with my doctor and I can get support from the staff in the evening
In a small number of cases, the interviewees stated that there was little emphasis in secure settings to prepare older patients to move along the care pathway:
‘A lot of therapy groups are constructed for younger people. I’m here as an older person, and
I have my issues and strengths, which are as important as those of a younger patient’
Physical health
All the participants experienced physical health conditions. They generally held positive views on how their physical health needs were met:
‘We’ve got a good health care system and if the staff notice anything, they immediately get
you sorted’
They frequently noted that their health needs were met better than in the community: ‘If I have pain in my back, they’d give me ibuprofen. When I was outside, there were times
when I did not have ibuprofen in the medicine box in my flat’
Extra consultations were always available, if needed:
‘They do health checking every month. But they come to see you more often if you have got
any complaints, injuries or worries’
Information on physical health care was also found to be adequate:
‘When I was first diagnosed with diabetes, they immediately gave me information’
Physical activity was a key element to wellbeing, as it boosted self-confidence, helped promoted a sense of purpose and helped obtain visible physical improvements:
‘My kids are saying ‘Dad, I’ve never seen you so well’. It shows me that I’m achieving
Gym sessions were especially popular among the older patients:
‘All of us over 50 go to the gym. One chap is over 70 and he does all the exercises’
Small fitness suites were also provided on the wards, an initiative which was very well received:
‘We have a private gym here on the ward, so, if you feel edgy, you can just go and relax’
The patients, however, reported that much remained to be improved, to ensure equal opportunities to all patients to get active:
‘We only get 45 minutes for the gym. And with the time it takes me to get there, I’m looking at
35 minutes’
The gym equipment was reported to be only suitable for younger patients:
‘The weights in the gym are too heavy. The over 50s can’t lift 30, 40 or 50 kilos’
Service improvement
We asked participants to report on any possible improvements in the service to enhance their experience. They reported on dedicated units/wards for ageing patients and understaffing issues. It was felt that dedicated units for the over 50s could be beneficial in some respects. They would reduce social isolation:
‘People of the same age stick together and you can be a little cut off if you don’t relate with
the younger people’
They would solve some irreconcilable intergenerational differences:
‘I might want to watch something on TV that a very young person wouldn’t want to watch’
‘I’d feel a little safer from the young and assaultive guys’
Dedicated wards for the over 50 would be more settled:
‘I imagine it’d be a lot quieter. And I can see better conversation, rather than shouting all
over the place’
The patients identified barriers to developing these services:
‘There’s problems with staffing and the prospect of a dedicated ward would be dismissed
straightaway’
Other interviewees manifested opposite views toward units for the over 50s:
‘I think wards need to be like a community, and in a community, you get people of all ages’
Several interviewees contended mixed environments are more settled:
‘When you get younger people coming through, if you have older people around, some of
their calm radiates’
They continued that older patients could benefit from mixing with the younger ones:
‘The young people can teach us about technology. It’s a fast world and you need to be up to
date’
Another area in need of improvement was staff-to-patient ratio. Some patients reported that at times wards were run on fewer than three staff. Understaffing could impact on the
atmosphere on the ward:
‘When the staff do long days, they can get quite edgy, and when you ask for things, they
sometimes respond with a nasty follow up’
‘People who are high dependent and need attention all the time get it. But the guys who are
self-dependent tend to be a little bit forgotten’
Given the staff shortages, movement of personnel across units and wards was frequent. This was cause for further disruption of patients’ routine:
‘Each ward is different, even the small things, like the boxes where they keep the keys. There
should be some sort of uniformity, so members of staff would just need to learn the routine of
the patients’
Discussion
This paper presents findings from a qualitative investigation of a sample of older patients living in secure forensic psychiatric units, providing novel insight into the experience of ageing in secure care.
In line with existing literature on old age forensic psychiatry (Yorston & Taylor, 2009), our findings highlighted good elements of care, such as physical healthcare provision and
educational/cultural opportunities. In addition to the benefits of spirituality documented in the prison literature (Reed, 1980; Bishop et al., 2014; Allen et al., 2013; Allen et al., 2008), our participants also provided positive feedback around support for their spiritual needs.
Our results also highlighted several challenges experienced by the older patients. As found in prison studies (Crawley & Sparks, 2006; Loeb et al., 2007), participants expressed concerns about the future and their attachment toward forensic units (Yorston & Taylor, 2009; Doron, 2007; Aday, 1994; Aday & Webster, 1979), which affected treatment compliance. Long-stay caused dependency from staff, decreased self-confidence to live independently and
activities, which was not found to be age-relevant and accessible for those with limited mobility. Accessibility issues have been consistently reported in the forensic literature (Joyce & Maschi, 2016; Yorston & Taylor, 2009), showing how little has been done to improve the situation over time.
Regarding the risk of social isolation, in line with previous research (Yorston & Taylor, 2009), we found that the participants encountered great barriers to building good
relationships with their own peers. Although mental health issues were recognised as a mediating factor, poor peer relationships were also the result of intergenerational issues, most patients in mixed-age wards being of younger age. Contrary to previous findings on long-stay patients of all ages (Völlm et al., 2017) and in line with research in old age forensic
psychiatry (Yorston & Taylor, 2009; Crawley, 2005), our participants reported limited contact with their families, a trend which might be related to ageing.
Given the added risk of social isolation, participants frequently discussed potential solutions. In contrast with previous evidence (Yorston & Taylor, 2009), when asked to comment on possible units for the over 50s, several patients supported mixed-age wards, contending that the benefits of living in a diverse community outnumbered intergenerational issues.
Consensus was instead found on the necessity to develop cross-ward social opportunities for older patients, there being just one intiative for over 50s, in the medium secure setting.
This study is characterised by some limitations. Sample size and composition might have affected the generalisability of findings. The only two women and participant of Black ethnicity were from medium security, thus neglecting representation of these populations from other services. In addition, our findings might over represent the views of the more compliant patients, who were more likely to be involved. In addition, the views of patients who lacked capacity to consent were not included.
In relation to data collection,our primarily deductive approach may have imposed themes upon the patients. However, we were aware of this possibility and allowed for new themes to be added, if necessary. Regarding data analysis, qualitative means of investigation require a degree of data interpretation which may alter/filter patients’ reports. To mitigate this risk, we kept our text input at a minimum in the results section, to safeguard the integrity of patients’ narratives.
In terms of research implications, we were only able to involve three services in our study. Although purposively sampled, our participants might not be representative of the wider population of ageing patients in secure services across the UK and in other countries. We therefore advocate that further research with nationally representative samples be undertaken.
independence in ageing people (NICE, 2015) and the Care Act 2015. A timely response is therefore needed.
It remains uncertain whether dedicated units for older patients are practically feasible,
financially sustainable and therapeutically effective. However, good practice can be promoted through (further) development of age-relevant approaches. Some examples reported in the literature include Cognitive Stimulation Therapy (CST), reminiscence, speech and language therapy, modifications to environments (e.g. shower chairs, handrails), flexible regimes (e.g. dedicated hours for phone calls) and personalised discharge packages (Natarajan & Mulvana, 2017).
These strategies need to be tailored to older patients’ needs, and so optimal allocation of funding and investment of resources is vital. We have shown that older patients do have views about their treatment and needs and, therefore, systems need to be in place to ensure their active input into how services are organised. Because older patients constitute a
References
Aday, R. H. (1994). Aging in prison: a case‐study on new elderly offenders. International Journal of Offender Therapy and Comparative Criminology, 38, 79–91.
Aday, R., & Webster, E. (1979). Aging in prison: the development of a preliminary model. Offender Rehabilitation, 3, 271–282.
Allen, R. S., Phillips, L. L., Roff, L. L., Cavanaugh, R., & Day, L. (2008).
Religiousness/spirituality and mental health among ageing male inmates. Gerontologist, 48, 692–697.
Allen, R. S., Harris, G. M., Crowther, M. R., et al. (2013). Does religiousness and spirituality moderate the relations between physical and mental health among aging prisoners?
International Journal of Geriatric Psychiatry, 28, 710–717. https://doi.org/10.1002/gps.3874. Baldwin, J., & Leete, J. (2012). Behind bars: the challenges of an ageing population.
Australian Journal of Dementia care, 2, 16-19.
Bishop, A. J., Randall, G., Merten, M. J. (2014). Consideration of forgiveness to enhance the health status of older male prisoners confronting spiritual, social, or emotional
vulnerability. Journal of Applied Gerontology, 33, 998–1017. https://doi.org/10.1177/ 0733464812456632.
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77-101.
Coid, J., Fazel, S., & Kahtan, N. (2002). Elderly patients admitted to secure forensic psychiatry services. The Journal of Forensic Psychiatry, 13, 416-427. DOI:
10.1080/09585180210154470
Cooney, F., & Braggins, J. (2010). Doing Time. Good practice with older people in prison - the views of prison staff. Prison Reform Trust, London.
Crawley E. (2005). Institutional thoughtlessness in prisons and its impacts on the dayto‐ day prison lives of elderly men. Journal of Contemporary Criminal Justice 21, 350–363. https://doi.org/10.1177/1043986205282018.
Crawley, E., & Sparks, R. (2006). Is there life after imprisonment? How elderly men talk about imprisonment and release. Criminology and Criminal Justice 6, 63–82.
https://doi.org/10.1177/1748895806060667.
Curtice, M., Parker, J., Wismayer, F.S., & Tomison, A. (2003). The elderly offender: an 11-year survey of referrals to a regional forensic psychiatric service. The Journal of Forensic Psychiatry & Psychology, 14, 253-265. DOI: 10.1080/1478994031000077989
Di Lorito, C., Dening, T., & Völlm, B. (2018). The characteristics and needs of older forensic psychiatric patients: A UK cross-sectional study. Submitted for publication.
Di Lorito, C., Völlm, B., & Dening, T. (2017). The individual experience of ageing prisoners: systematic review and meta‐synthesis through a Good Lives Model framework. International Journal of Geriatric Psychiatry. doi: 10.1002/gps.4762. [Epub ahead of print]
Di Lorito, C., Castelletti, L., Tripi, G., Gandellini, M. G., Dening, T., & Völlm, B. (2017). The Individual Experience of Aging Patients and the Current Service Provision in the Context of Italian Forensic Psychiatry: A Case Study. Journal of forensic nursing, 13, 118-125.
Doron, I. (2007). Heaven or hell? Aging behind bars in Israel. International Journal of Aging, 9, 145–159. https://doi.org/10.2190/HA.9.2.e.
Drennan, D., Wooldridge, J., Aiyegbusi, A., Alred, D., Ayres, J., Barker, R., Carr, S., Euson, S., Lomas, H., Moore, E., Stanton, D. & Shepherd, G (2014). Implementing Recovery through Organisational Change Briefing Paper 10. London: Centre for Mental Health and Mental Health Network. Accessed 10.06.2016 at:
http://www.imroc.org/wp- content/uploads/ImROC-briefing-10-Making-Recovery-a-Reality-in-Forensic-Settings-final-for-web.pdf
Frazer, L. (2003). Ageing inside. school for policy studies working paper series paper number 1. University of Bristol, Bristol. Retrieved from:
http://www.clinks.org/sites/default/files/basic/filesdownloads/Older%20Prisoners%20LF%20 Report%20sps01_lf.pdf
Joyce, J., & Maschi, T. (2016). ‘In here, time stands still’. The rights, needs and experiences of older people in prison. Irish Penal Reform Trust: Dublin, Ireland.
Lightbody, E., Gow, R.L., & Gibb, R. (2010). A survey of older adult patients in special secure psychiatric care in Scotland from 1998 to 2007. The Journal of Forensic Psychiatry & Psychology, 21, 966-974. DOI: 10.1080/14789949.2010.504858
Loeb, S. J., Steffensmeier, D., & Myco, P. M. (2007). In their own words: older male prisoners’ health beliefs and concerns for the future. Geriatric Nursing, 28, 319–329. https://doi.org/10.1016/j.gerinurse.2007.02.001.
Moll, A. (2013). Losing track of time: dementia and the ageing prison population. Mental Health Foundation, London. Accessed RECOOP, 2015.10.17 at:
http://www.mentalhealth.org.uk/content/assets/PDF/publications/losing-track-of-time-2013.pdf?view=Standard
Natarajan, M., & Mulvana, S. (2017). New horizons: forensic mental health services for older people. British Journal of Psychiatry Advances, 23, 44-53.
National Institute for Health and Care Excellence 2015. Mental wellbeing and independence in older people. NICE guideline (NG32). London: National Institute for Health and Care Excellence.
Paradis, C., Broner, N., Maher, L.M., & O’Rourke, T. (2000). Mentally Ill Elderly Jail Detainees. Journal of Offender Rehabilitation, 31, 77-86. DOI: 10.1300/J076v31n01_05 Reed, M. B. (1980). Aging in a total institution: the case of older prisoners (Doctoral Dissertation). Available at: https://www.ncjrs.gov/pdffiles1/Digitization/
65232NCJRS.pdf [Accessed 10 Dec 2016]
Resettlement and Care for Older ex-Offenders and Prisoners (RECOOP). (2015). Retrieved from http://www.recoop.org.uk/pages/resources/
Shah, A. (2006). An Audit of a Specialist Old Age Psychiatry Liaison Service to a Medium and a High Secure Forensic Psychiatry Unit. Medicine, Science, and the Law, 46, 99-104. The Centre for Mental Health (2015). Secure mental health services. Retrieved October 27, 2017, from:
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/198033/Nation al_Service_Framework_for_Older_People.pdf
Tiwana, R., McDonald, S., & Völlm, B. (2016). Policies on sexual expression in forensic psychiatric settings in different European countries. International journal of mental health systems, 10, 5.
Tomar, R., Treasaden, I. H., & Shah, A. K. (2005). Is there a case for a specialist forensic psychiatry service for the elderly? International Journal of Geriatric Psychiatry, 20, 51-56. DOI: 10.1002/gps.1247
Ward, T., Mann, R. E., & Gannon, T. A. (2007). The Good Lives Model of offender rehabilitation: Clinical implications. Aggression and Violent Behavior, 12, 87−107.
Wong, M.T.H., Fenwick, P.B.C., Lumsden, J., Fenton, G.W., Maisey, M.N., Lewis, P. et al. (1995). Elderly offenders in a maximum security mental hospital. Aggressive Behaviour, 21, 321-324.
Yorston, G.A. (2015). Managing aggression and violence in older people. London: The Royal College of Psychiatrists.
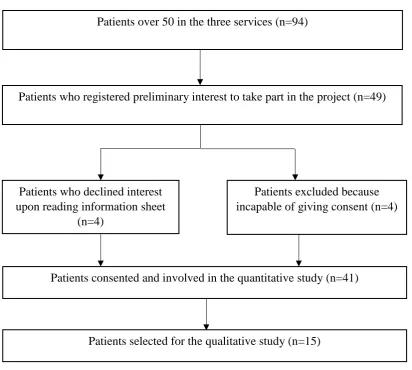
Figure 1. Selection of participants
Patients over 50 in the three services (n=94)
Patients who registered preliminary interest to take part in the project (n=49)
Patients who declined interest upon reading information sheet
(n=4)
Patients excluded because incapable of giving consent (n=4)
Patients consented and involved in the quantitative study(n=41)
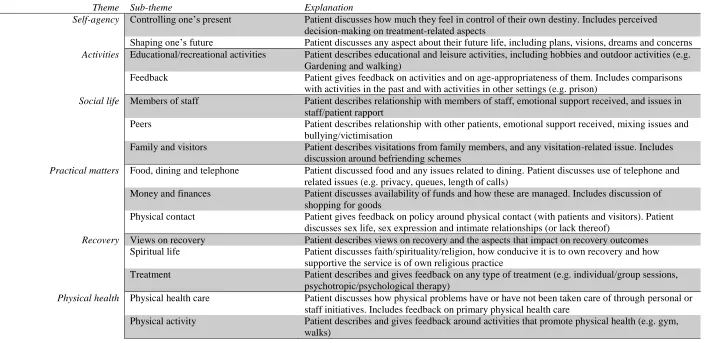
Table 1. Code book
Theme Sub-theme Explanation
Self-agency Controlling one’s present Patient discusses how much they feel in control of their own destiny. Includes perceived
decision-making on treatment-related aspects
Shaping one’s future Patient discusses any aspect about their future life, including plans, visions, dreams and concerns
Activities Educational/recreational activities Patient describes educational and leisure activities, including hobbies and outdoor activities (e.g.
Gardening and walking)
Feedback Patient gives feedback on activities and on age-appropriateness of them. Includes comparisons
with activities in the past and with activities in other settings (e.g. prison)
Social life Members of staff Patient describes relationship with members of staff, emotional support received, and issues in
staff/patient rapport
Peers Patient describes relationship with other patients, emotional support received, mixing issues and
bullying/victimisation
Family and visitors Patient describes visitations from family members, and any visitation-related issue. Includes
discussion around befriending schemes
Practical matters Food, dining and telephone Patient discussed food and any issues related to dining. Patient discusses use of telephone and
related issues (e.g. privacy, queues, length of calls)
Money and finances Patient discusses availability of funds and how these are managed. Includes discussion of
shopping for goods
Physical contact Patient gives feedback on policy around physical contact (with patients and visitors). Patient
discusses sex life, sex expression and intimate relationships (or lack thereof)
Recovery Views on recovery Patient describes views on recovery and the aspects that impact on recovery outcomes
Spiritual life Patient discusses faith/spirituality/religion, how conducive it is to own recovery and how
supportive the service is of own religious practice
Treatment Patient describes and gives feedback on any type of treatment (e.g. individual/group sessions,
psychotropic/psychological therapy)
Physical health Physical health care Patient discusses how physical problems have or have not been taken care of through personal or
staff initiatives. Includes feedback on primary physical health care
Physical activity Patient describes and gives feedback around activities that promote physical health (e.g. gym,