University of Miami
Scholarly Repository
Open Access Dissertations Electronic Theses and Dissertations
2014-07-29
The Effect of a Community-Based Exercise
Program on Inflammation, Metabolic Risk, and
Fitness Levels Among Persons Living with HIV/
AIDS
Stacy E. Cutrono
University of Miami, [email protected]
Follow this and additional works at:http://scholarlyrepository.miami.edu/oa_dissertations
This Open access is brought to you for free and open access by the Electronic Theses and Dissertations at Scholarly Repository. It has been accepted for inclusion in Open Access Dissertations by an authorized administrator of Scholarly Repository. For more information, please contact
Recommended Citation
Cutrono, Stacy E., "The Effect of a Community-Based Exercise Program on Inflammation, Metabolic Risk, and Fitness Levels Among Persons Living with HIV/AIDS" (2014).Open Access Dissertations.Paper 1263.
UNIVERSITY OF MIAMI
THE EFFECT OF A COMMUNITY-BASED EXERCISE PROGRAM ON INFLAMMATION, METABOLIC RISK, AND FITNESS LEVELS AMONG
PERSONS LIVING WITH HIV/AIDS
By
Stacy E. Cutrono A DISSERTATION Submitted to the Faculty of the University of Miami
in partial fulfillment of the requirements for the degree of Doctor of Philosophy
Coral Gables, Florida August 2014
©2014 Stacy E. Cutrono All Rights Reserved
UNIVERSITY OF MIAMI
A dissertation submitted in partial fulfillment of the requirements for the degree of
Doctor of Philosophy
THE EFFECT OF A COMMUNITY-BASED EXERCISE PROGRAM ON INFLAMMATION, METABOLIC RISK, AND FITNESS LEVELS AMONG
PERSONS LIVING WITH HIV/AIDS
Stacy E. Cutrono Approved:
________________ _________________
Kevin Jacobs, Ph.D. Arlette Perry, Ph.D.
Professor of Kinesiology and Professor of Kinesiology and
Sport Sciences Sport Sciences
________________ _________________
Joseph Signorile, Ph.D. M. Brian Blake, Ph.D.
Professor of Kinesiology and Dean of the Graduate School
Sport Sciences
________________
John Lewis, Ph.D.
Professor of Psychiatry and
CUTRONO, E. STACY (Ph.D., Exercise Physiology)
The Effect of a Community-Based (August 2014)
Exercise Program on Inflammation, Metabolic Risk, and Fitness Levels Among Persons Living with HIV/AIDS
Dissertation supervised by Professor Kevin Jacobs. No. of pages in text. (23)
The Human Immunodeficiency Virus (HIV) pandemic remains a top national health priority. Chronic inflammation may be a critical component in the disease course of HIV as C-reactive protein (CRP) is elevated and associated with increased mortality. This study examined the effect of three months of combined aerobic and resistance exercise training among a diverse cohort of HIV-infected men and women. The fixed effect of time for CRP was found to be non-significant (F[1,57.3]=1.7, p=0.19). There was a significant fixed effect for time for upper body (F[1,51.6]=18.1, p<0.05) and lower body strength (F[1,48.0]=15.7, p<0.05) and significant declines in diastolic blood pressure (p=0.002) and waist circumference (p=0.027). Though levels of CRP were not impacted after three months training, participants demonstrated a significant increase in muscular strength as well as beneficial changes in metabolic risk factors. Future studies should focus on determining the optimal exercise intervention length and mode to reduce inflammation.
Key Words: Human Immunodeficiency Virus, Aerobic Exercise, Resistance Training, C-reactive Protein, Inflammation, Metabolic Risk.
TABLE OF CONTENTS Page List of Figures ………... iv List of Tables ……….…… v List of Abbreviations ……….………...… vi Chapter 1 Introduction ………..……... 1 2 Methods ……….……….. 4 3 Results ……….……….... 9 4 Discussion ……….………..……….. 11 Figures ………..………...…. 16 Tables ………..………. 17 Bibliography ………...…. 20 iii
LIST OF FIGURES
Page Figure 1.
Changes in Levels of C-reactive Protein Across Exercise Compliance Groups …... 16
LIST OF TABLES
Page Table 1.
Demographic and Baseline Characteristics by Gender………..…... 17 Table 2.
Changes in Metabolic Risk Profile ………..………...… 18 Table 3.
Changes in Fitness Parameters………….………...… 19
LIST OF ABBREVIATIONS
1-RM: One repetition maximum
ACSM: American College of Sports Medicine AIDS: Acquired Immunodeficiency Syndrome ART: Antiretroviral treatment
BMI: Body Mass Index
CARET: Combined aerobic and resistance training CRP: C-reactive protein
DBP: Diastolic blood pressure FG: Fasting glucose
HIV: Human Immunodeficiency Virus HDL-C: High density lipoprotein cholesterol hsCRP: high sensitivity C-reactive protein LDL-C: Low density lipoprotein cholesterol MetS: Metabolic Syndrome
PLWH: Persons Living with HIV SES: Socioeconomic status
VO2max: Maximal oxygen consumption
Chapter 1 Introduction
Globally, the rate of new human immunodeficiency virus (HIV) infections has fallen by 33% since 2001 [1], but has held steady in the United States (U.S.) at an estimated 50,000 new cases per year [2]. As such, the HIV/Acquired Immune Deficiency Syndrome (AIDS) pandemic continues to affect millions worldwide and remains a top health priority in the U.S. Recent reports indicate that the state of Florida has one of the highest rates of newly reported HIV infections and newly reported AIDS cases in the country [3]. Furthermore, the burden of HIV/AIDS continues to disproportionately affect individuals of minority race/ethnicity, such as Blacks/African Americans and Hispanic/Latinos who represent 44% and 20% of new HIV infections, respectively, as well as individuals with lower socioeconomic status (SES) and reduced access to quality health care [2].
The use of combination antiretroviral therapy (ART) has significantly reduced the risk of mortality and morbidity in persons living with HIV (PLWH) since its introduction in the mid-1990s [4-7]. However, the extensive use of ART has given rise to serious and adverse side effects including hyperlipidemia, insulin resistance, and lipodystrophy thus increasing the risk for non-AIDS events such as cardiovascular disease and the development of metabolic syndrome (MetS) [8,9]. The pathogenic mechanism for metabolic changes secondary to combination ART have yet to be fully elucidated, however, current investigations indicate a greater risk of negative side effects are associated with use of drug combinations containing protease inhibitors or nucleoside reverse transcriptase inhibitors [10]. The risks associated with widespread and prolonged
2 use of ART may be managed through effective lifestyle interventions incorporating exercise and weight management.
Current research suggests that chronic inflammation may be a critical component in the course of disease states. The American Heart Association and the Centers for Disease Control and Prevention support the use of C-reactive protein (CRP), an acute, non-specific inflammatory biomarker, as an independent predictor of increased coronary risk and recommends using 3.0 mg/L as the minimum threshold for high risk classification [11]. In healthy young adults the median level of CRP is 0.8 mg/L [12]. However, among PLWH, CRP levels are elevated [9,13] with reported ranges of 1.94 to 4.80 mg/L [14-16] and are associated with opportunistic infections, progression to AIDS, and mortality. Individuals enrolled in Multicenter AIDS Cohort Study with CRP levels ≤ 1.2 mg/L were found to have a 47% reduction in time to AIDS progression compared to those with > 2.3 mg/L [17]. Individuals in the Strategies for Management of Anti-Retroviral Therapy trial with CRP levels ≥ 5 mg/L had 7.6 fold higher odds of developing an opportunistic infection than those with CRP ≤ 1.0 mg/L [18]. Thus, interventions that reduce CRP levels may improve the cardiovascular risk profiles and disease prognosis among PLWH.
The physiological and psychological benefits of regular exercise are numerous and well established. The available literature supports the therapeutic use of aerobic and resistance exercise for improving health and fitness outcomes among PLWH [19, 20]. For this reason, the American College of Sports Medicine (ACSM) recommends that PLWH engage in a regular exercise program consisting of aerobic exercise and resistance exercise on most days of the week [21]. A reduction in systemic inflammation may be
3 one of the mechanisms driving the protective effects of regular exercise for chronic disease risk [22], although recent research examining the effects of exercise interventions on circulating inflammatory biomarkers has produced inconsistent results. The third National Health and Nutrition Examination Survey found that 21% of sedentary individuals had elevated CRP levels compared to 13% of moderately active individuals [23]. Several other studies have reported significant declines in CRP levels after aerobic exercise interventions among older individuals [24], obese women [25] and breast cancer survivors [22]. Yet, a recent meta-analysis of randomized controlled trials reported a non-significant decrease in CRP levels among subjects in aerobic exercise interventions [26]. The pro-inflammatory changes secondary to treatment with ART are accepted as a necessary risk in an effort to reduce progression to AIDS and AIDS mortality, yet inflammatory changes measured by elevated CRP increase the risk of non-AIDS events, cardiovascular mortality, as well as progression to AIDS. Interventions with potential to manage treatment side effects and reduce inflammation are necessary among PLWH. The effect of exercise on CRP levels has not been well examined among PLWH, however, given the severity of treatment side effects its potential beneficial impact warrants further investigation.
The purpose of this study was to determine the effect of combined aerobic and resistance exercise training (CARET) on inflammation, metabolic risk profile, and aerobic and muscular fitness among PLWH after three months of training using data
Chapter 2 Methods
Study Design
The Healthy Living for Better Days was a 12-month, community exercise program conducted by research staff at the University of Miami to improve the health of low SES individuals with HIV residing in Miami-Dade. This study specifically analyzed baseline and 3-month data. Program outcome variables measured at baseline and three months included: 1) physical characteristics (body weight, body mass index, waist and hip circumferences, blood pressure), 2) non-lipid blood markers (high sensitivity CRP, fasting blood glucose, and insulin), 3) blood lipid profile (total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and total triglycerides), and 4) physical fitness variables (estimated VO2max and one repetition maximum for upper
and lower body strength).
Participants
Ninety male and female participants were enrolled in Healthy Living for Better Days through referrals from the Adult HIV clinic at the University of Miami/Jackson Health System and other local HIV clinics. Program eligibility criteria included: (1) confirmed HIV infection as established by external laboratory reports, (2) men or women ≥ 18 years of age, (3) currently receiving antiretroviral treatment, and (4) ability to attend weekly exercise sessions at the UHealth Fitness and Wellness Center. Program exclusion criteria included any medical condition or situation for which unsupervised exercise would be contraindicated. The Institutional Review Board of the University of Miami
5 approved Healthy Living for Better Days and all participants gave written informed consent.
Exercise Intervention
All exercise sessions for Healthy Living for Better Days were held at the UHealth Fitness and Wellness Center at the University of Miami Medical campus. Each participant was required to swipe an electronic badge to gain admittance to the wellness center allowing attendance to be recorded and tracked electronically. Participants were
encouraged to attend the supervised exercise sessions held four times a week, but were
also given open access to the wellness center. Study personnel directed each supervised session and were available to advise participants on their exercise intensity and progression. Each supervised exercise session was 40 to 60 minutes in length and consisted of at least 30 minutes of aerobic exercise completed on a treadmill, elliptical machine, or stationary bike and resistance exercises completed on stacked weight machines (bench press, shoulder press, biceps curl, triceps extension, leg extension, leg curls, leg press, squat, lateral raises, lat pull downs, back extension, and abdominal crunches). Aerobic exercise was performed at 60-80% of each individual’s age-predicted maximum heart rate (HRmax). The duration of exercise sessions progressed from 40 to 60
minutes over the first two weeks of the program. Two to four sets of eight to fifteen repetitions were performed for each upper and lower body exercise.
Measures
Physical Characteristics
Research staff used standard techniques to obtain anthropometric measurements. Weight and height were recorded to the nearest 0.1 kg and 0.1 cm, respectively, to
6
calculate body mass index (BMI). Waist circumference was measured in inches at the narrowest portion between the lowest rib and the iliac crest. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured by use of the automatic oscillometric device (Omron HEM-712CN2, Omron Healthcare, Inc., Bannockburn, Illinois).
Blood Sampling and Analyses
Blood samples were drawn from participants in the morning in a fasted condition and processed by the Diabetes Research Institute Clinical Laboratory. Chemistry and immunoassays were performed by automated analyzer (Roche Cobas-6000; Roche Diagnostics, Indianapolis, IN) utilizing the manufacturer’s reagents and following the manufacturer’s instructions. High sensitivity CRP (hsCRP) was quantified in serum by a high sensitivity latex-particle enhanced immunoturbidimetirc assay with a detection limit of 0.1 mg/L with an intra- and inter-assay coefficients of variation (CV) of 1.1 % and 2.2%, respectively. Fasting glucose (FG) was measured by the hexokinase method with intra- and inter-assay CVs of 1.9% and 2.7%, respectively. Total cholesterol and triglycerides were determined in serum or plasma by enzymatic, colorimetric assay with intra- and inter-assay CVs are 0.7% and 1.8%, respectively for total cholesterol and 0.9% and 2.3%, respectively for triglycerides. High density lipoprotein cholesterol (HDL-C) was measured using a third generation homogenous enzymatic colorimetric assay with intra- and inter-assay CVs of 0.6% and 1.9%, respectively. Low density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald equation.
7 Physical Fitness
Cardiorespiratory fitness was measured using a Rockport One-Mile Fitness Walking Test [21], which has been validated in healthy adults aged 30-69 years [27] and been used in other clinical populations [28]. The test was modified for use indoors with participants performing the one-mile walk on a treadmill rather than on an outdoor track. Participants were instructed to walk for one mile on the treadmill as quickly as possible and were allowed to modify speed at their discretion throughout the test. Heart rate was measured for ten seconds immediately upon completion by palpating the radial artery. Age, gender, body weight, and walk time were also recorded and used in a regression equation to predict maximal oxygen consumption (VO2max).
Muscular strength was measured using the ACSM protocol for one-repetition maximum (1-RM) testing [21]. Program participants completed a maximum of four trials of 10, 8, 6, and 3 repetitions with rest periods between 2 and 4 minutes between trials. The initial weight was selected within the subject’s perceived capacity (50-70% of capacity) and resistance was progressively increased until the participants reached their maximum. The final maximum weight lifted successfully one time for bench press and leg press was recorded as the 1-RM.
Metabolic syndrome was defined using ATPIII criteria [29]. Three or more criteria had to be met to be classified as having MetS: 1) high fasting serum triglycerides (≥150mg/dl), 2) abnormal waist circumference (>102 cm for men and >88 cm for women), 3) low HDL-C level (<40 mg/dl for men and <50 mg/dl for women), 4) high blood pressure (BP) (≥130/85 mm Hg), and 5) high FG level (≥110 mg/dl). Participants who self-reported being diagnosed with diabetes or who were receiving treatment for
8 diabetes were classified as having a high FG level. The same criteria were used for high BP.
Statistical analysis
Statistical analyses were performed with the Statistical Package for Social Sciences (SPSS) version 22 for Windows (IBM Inc., Chicago, IL, USA). Statistical analyses included descriptive statistics and frequencies for each variable. Linear Mixed Modeling (LMM) was used to assess the fixed effect of time on changes in the outcome variables (hsCRP, estimated VO2max, 1-RM bench press, and 1-RM leg press) from
baseline to 3-months follow up. The significance level of all analyses was α < 0.05. LMM with heterogeneous compound symmetry covariance allowed us to account for missing values, subject attrition, inter-correlated responses between time points, and non-constant variability. Paired t-tests were used to assess changes in metabolic risk factors (BP, BMI, FG, HDL-C, waist circumference and triglycerides) from baseline to 3-months follow up. Chi-square analysis was used to assess the change in MetS prevalence from baseline to 3-months follow up.
Given that the exercise program consisted of four sessions per week, participants were stratified into exercise compliance groups based on average exercise sessions attended as follows: (a) Non-compliant (average of <1x/week for 3 months), (b) Somewhat compliant (average 1-2x/week for 3 months), and (c) Compliant (≥ 2x/week for 3 months), where compliant individuals completed at least 50% of the prescribed exercise. Comparisons between groups from baseline to 3 months were analyzed using
Chapter 3 Results
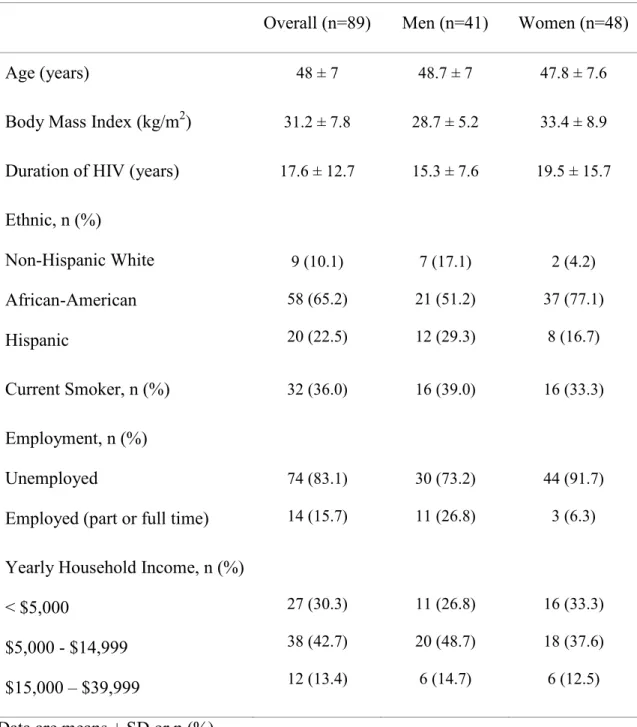
Demographic data are presented in Table 1. Ninety PLWH were enrolled in Healthy Living for Better Days. The majority of participants were women (53.9%), Black/African American (65.2%), and unemployed or disabled at the time of participation (83.1%). Nearly one-third of participants were classified as having MetS at baseline. Fifty-five percent of total participants were non-compliant (49/89), 20.2% were somewhat compliant (18/89), and 24.7% were compliant (22/89) with the prescribed exercise. After three months participation in Healthy Living for Better Days, nearly one-quarter (24.7%) of our participants were meeting physical activity recommendations defined as a combination of moderate- and vigorous-intensity aerobic exercise at least 75 minutes/week and resistance training twice per week.
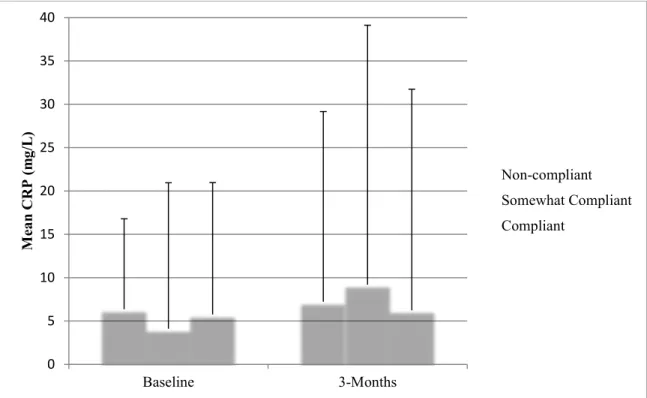
The fixed effect of time for hsCRP was found to be non-significant (F[1,57.3]=1.7, p=0.19) (Figure 1). Mean hsCRP at baseline was 5.75 ± 7.62 mg/L (median 2.30) and 7.54 ± 14.19 mg/L (median 2.95) at 3-months follow up. Comparing hsCRP across categories of exercise compliance groups (see Figure 1) revealed non-significant fixed effects for time (F[1,55.5]=2.4, p=0.13), exercise compliance (F[2,62.1]=0.06, p=0.94) and exercise compliance x time (F[2,55.5]=0.99, p=0.38). Comparing hsCRP levels by gender group revealed a significant fixed effect for gender (F[1,68.6]=4.08, p<0.05]), with women displaying an overall higher mean hsCRP (8.50 ± 12.69 mg/L) than men (4.46 ± 13.65 mg/L). The fixed effect for time (F[1,57.4]=1.75, p=0.19]) and gender x time was non-significant (F[1,57.4]=0.06, p=0.80]).
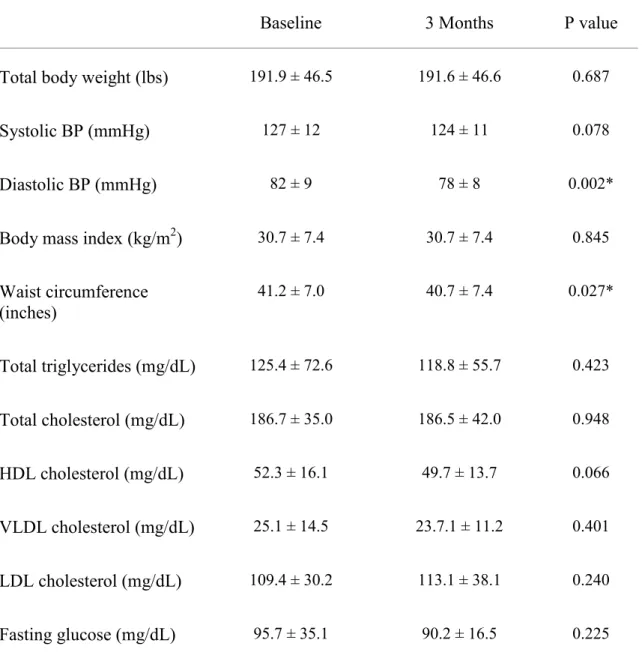
10 Changes in participant’s metabolic risk profile can be found in Table 2. Diastolic BP (p=0.002) and waist circumference (p=0.027) significantly decreased from baseline to three months. There were no significant changes from baseline to three months for body weight, SBP, BMI, triglycerides, total cholesterol, HDL-C, VLDL-C, LDL-C, or FG. There was a non-significant decline in individuals with MetS from baseline to three months (32% vs. 19%, Χ2(1, N
baseline=89, N3months=63)=3.43, p=0.06).
The fixed effect of time for changes in VO2max was found to be non-significant
(F[1,36.3]=3.5, p=0.07) (Table 3). For upper body 1-RM, a significant fixed effect was found for time (F[1,51.6]=18.1, p<0.05) and the parameter estimate between baseline and three months follow up was also significant (t[51.6]= -4.3, p<0.05). Likewise, for lower body 1-RM a significant fixed effect was found for time (F[1,48.0]=15.7, p<0.05) and the parameter estimate between baseline and three month follow up was also significant
Chapter 4 Discussion
A strength of the Health Living for Better Days program was its enrollment of a diverse sample of participants comprised mainly of minorities (>85%). Black/African Americans and Hispanic/Latinos continue to bear a disproportionate burden of new HIV cases despite only representing represent 13.1% and 16.9% of the general U.S. population, respectively [30]. For this reason our results may be more generalizable to the larger population of PLWH. A majority of participants were of low SES as evidenced by high rates of unemployment (83.1%) and low household income (73%), defined as earning less than $15,000 annually. Furthermore, over half of the sample was comprised of women, who according to the CDC accounted for one in four new HIV infections in 2010 [2].
Disappointingly, a majority of participants (55%) were not compliant with the prescribed exercise regime.Previous literature has documented barriers and challenges to appointment adherence or research participation among PLWH [31,32]. Though few studies have specifically assessed challenges to participating in exercise programs, there have been reports of moderate withdrawals (range 3% to 44%) and low compliance (range 24% to 82%) in other exercise interventions [19]. Macarthur et al. [33], reported transportation and difficulty exercising as challenges to completing exercise testing and training. Similarly, Neidig et al. [34], reported changes in employment, unreliable transportation, and family responsibilities as contributors to withdrawal from an aerobic exercise trial. Nevertheless, Healthy Living for Better Days was designed as a community-based exercise program in an effort to expand access to a variety of
12 participants. The program was well received by most participants (data not reported), however, the low compliance highlights the challenge of engaging this population in exercise programs.
Mean levels of hsCRP were elevated at baseline (5.75 ± 0.82 mg/L, Figure 1) and 40% of our participants had hsCRP values that would be classified as high coronary risk (>3 mg/L) under AHA and CDC guidelines [11]. Median levels of hsCRP at baseline and 3-months follow up were greater than values previously reported in the literature among PLWH (1.20-2.83 mg/L) [14,17]. Elevated CRP has been associated with metabolic risk factors such as obesity, hypertension, and dyslipidemia [35]. Among our participants BMI and waist circumference were elevated at baseline and additionally a few of our participants displayed very high CRP values perhaps reflective of the disease course of the HIV infection. Thus, it is possible that our cohort had more severe inflammation than the general population of PLWH. Women in our sample were found to have significantly higher hsCRP levels than men. This is consistent with data from the third National Health and Nutrition Examination Survey that found that the odds of having elevated CRP levels is two-fold higher among women than men [35].
Despite low compliance, participants showed a trend for an increase in VO2max of
2.2 mL/kg/min with three months of training (Table 3). Although this trend was not significant, our results were consistent with previously reported changes in VO2max (range
+2.6 mL/kg/min to +4.7 mL/kg/min) after three months of training among PLWH [8,36]. Exercise adherence did not appear to be a contributing factor as even the compliant cohort of subjects showed no significant improvement in hsCRP. In contrast to our three-month program consisting of CARET, Lindegaard et al. [37] found that hsCRP levels
13 declined in a small sample (n=18) of HIV-positive men who performed 35 minutes of endurance training 3x/week for 16 weeks (baseline hsCRP, 2.42 mg/L [1.01-5.80], 16-week hsCRP, 1.82 mg/L [0.76-4.36]; p < 0.0001). However, the effect of exercise on inflammatory biomarkers was not the primary variable studied by Lindegaard et al. [37]. Nonetheless, we cannot rule out the possibility that a longer intervention or higher sustained intensity of aerobic exercise is needed to impact systemic inflammation.
Participants significantly increased both upper and lower body strength after three months of CARET as has been shown in other studies that involved resistance training among PLWH [20,38,39]. The improvements in strength in our study, however, were not associated with a significant improvement in hsCRP levels from baseline to the 3-month follow up (Figure 1). Likewise, Lindegaard et al., [37] found that despite a 30% improvement in strength after 16 weeks of resistance training, there was no significant change in CRP levels (baseline CRP: 1.54 mg/L [1.0-2.37], 16-week CRP: 1.65 mg/L [1.07-2.54]; p = 0.44) among HIV-positive men. Similarly, among older adults assigned to 10-months of strength and flexibility training serum CRP levels were not improved compared to those in an aerobic exercise arm [24]. These results may indicate that aerobic exercise rather than resistance training may be the primary mode of exercise by which systemic inflammation is impacted.
It has been suggested that reduction in systemic inflammation may be the mechanism driving the protective effects of regular physical activity and exercise for chronic disease risk [22]. Yet, a meta-analysis by Kelley et al., [26] of randomized controlled trials among adult subjects reported a non-significant 3% decrease in CRP levels in aerobic exercise interventions ranging from eight weeks to six years. On the
14 other hand, CRP levels were reported to significantly decline in aerobic exercise trials among older adults [24] and postmenopausal obese women [25] after 10-months and 12-months of training, respectively. Thus, greater gains in aerobic fitness as measured by
VO2max may be necessary to affect hsCRP levels in PLWH. Future studies examining the
role of exercise interventions on systemic inflammation should incorporate randomization to an aerobic-only comparison arm.
The presence of one or more cardiovascular risk factors, specifically those which contribute to the classification of MetS, are associated with a pro-inflammatory state. Data from the third National Health and Nutrition Examination Survey indicated that the presence of at least one abnormal cardiovascular risk factor was associated with a three-fold higher prevalence of elevated CRP [35]. Among PLWH metabolic changes secondary to the extensive use of ART, such as insulin resistance, adiposity and poor lipid profiles, has contributed to an elevated cardiovascular risk profile [40-42]. In our cohort nearly one third of participants had MetS at baseline. After three months of CARET we observed a significant decrease in DBP and waist circumference. Though not significant, we observed a trend towards decreased SBP, total triglycerides, FG, and the number of individuals with MetS. We did not observe changes in total body weight or BMI. Several studies have reported a rapid progression to MetS after initiation of ART [43-46]. Given the deleterious impact of ART on metabolic risk factors and the rate of change reported in previous studies among PLWH, it appears that our program may have been effective in delaying a worsening of these side effects. A longer intervention, in combination with changes in total body weight, may be necessary to reduce metabolic
15 In conclusion, our study enrolled a diverse cohort of HIV-infected individuals receiving ART, who were of predominantly low SES. Overall mean levels of hsCRP were elevated in our cohort of HIV-infected individuals receiving ART. Though levels of hsCRP were not impacted after three months of CARET, participants demonstrated a significant increase in upper and lower body muscular strength as well as beneficial changes in waist circumference and diastolic blood pressure. Although low compliance to the prescribed exercise limits our ability to make definitive conclusions about the impact of exercise on systemic inflammation, it is possible that a longer intervention or greater intensity is necessary to induce improvements in aerobic fitness and metabolic profiles and thus impact systemic inflammation. Future studies should focus on effective ways of engaging and retaining HIV-infected minorities in structured exercise interventions and discerning the optimal dose and duration of exercise to reduce inflammation.
Figure 1. Changes in Levels of C-reactive Protein Across Exercise Compliance Groups
Data are means ± SD
Non-compliant, average of <1x/week for 3 months Somewhat Compliant, average 1-2x/week for 3 months Compliant, ≥ 2x/week for 3 months
hsCRP, high sensitivity C-reactive protein
0 5 10 15 20 25 30 35 40 Baseline 3-Months M ea n CRP (m g/ L) Non-compliant Somewhat Compliant Compliant 16
Table 1. Demographic and Baseline Characteristics by Gender
Overall (n=89) Men (n=41) Women (n=48)
Age (years) 48 ± 7 48.7 ± 7 47.8 ± 7.6
Body Mass Index (kg/m2) 31.2 ± 7.8 28.7 ± 5.2 33.4 ± 8.9
Duration of HIV (years) 17.6 ± 12.7 15.3 ± 7.6 19.5 ± 15.7
Ethnic, n (%) Non-Hispanic White African-American Hispanic 9 (10.1) 58 (65.2) 20 (22.5) 7 (17.1) 21 (51.2) 12 (29.3) 2 (4.2) 37 (77.1) 8 (16.7) Current Smoker, n (%) 32 (36.0) 16 (39.0) 16 (33.3) Employment, n (%) Unemployed
Employed (part or full time)
74 (83.1) 14 (15.7) 30 (73.2) 11 (26.8) 44 (91.7) 3 (6.3)
Yearly Household Income, n (%) < $5,000 $5,000 - $14,999 $15,000 – $39,999 27 (30.3) 38 (42.7) 12 (13.4) 11 (26.8) 20 (48.7) 6 (14.7) 16 (33.3) 18 (37.6) 6 (12.5)
Data are means ± SD or n (%)
18
Table 2. Changes in Metabolic Risk Profile
Baseline 3 Months P value
Total body weight (lbs) 191.9 ± 46.5 191.6 ± 46.6 0.687
Systolic BP (mmHg) 127 ± 12 124 ± 11 0.078
Diastolic BP (mmHg) 82 ± 9 78 ± 8 0.002*
Body mass index (kg/m2) 30.7 ± 7.4 30.7 ± 7.4 0.845
Waist circumference (inches) 41.2 ± 7.0 40.7 ± 7.4 0.027* Total triglycerides (mg/dL) 125.4 ± 72.6 118.8 ± 55.7 0.423 Total cholesterol (mg/dL) 186.7 ± 35.0 186.5 ± 42.0 0.948 HDL cholesterol (mg/dL) 52.3 ± 16.1 49.7 ± 13.7 0.066 VLDL cholesterol (mg/dL) 25.1 ± 14.5 23.7.1 ± 11.2 0.401 LDL cholesterol (mg/dL) 109.4 ± 30.2 113.1 ± 38.1 0.240 Fasting glucose (mg/dL) 95.7 ± 35.1 90.2 ± 16.5 0.225
Data are means ± SD
*Significant difference from baseline to three months (p<0.05, paired t-test) BP, blood pressure
VLDL, very low density lipoprotein LDL, low density lipoprotein HDL, high density lipoprotein
19
Table 3. Changes in Fitness Parameters
Baseline 3 Months Statistic
VO2max (mL/kg/min) 27.2 ± 8.9 29.4 ± 10.0 F[1,36.3]=3.5, p = 0.07 Upper Body 1-RM (lbs) 114 ± 51 125 ± 46 F[1,51.6]=18.1, *p < 0.05 Lower Body 1-RM (lbs) 225 ± 81 250 ± 96 F[1,48.0]=15.7, *p < 0.05 Data are means ± SD.
*Significant fixed effect on time (p<0.05)
VO2max, maximal volume of oxygen consumed
BIBLIOGRAPHY
(1) Joint United Nations Programme on HIV/AIDS. UNAIDS Report on the Global AIDS Epidemic. 2013.
(2) Centers for Disease Control and Prevention. HIV in the United States: At A Glance. Available at: http://www.cdc.gov/hiv/statistics/basics/ataglance.html#ref1. Accessed 11/15, 2013.
(3) Florida Health. Epidemiology of HIV Infection and Trends in Florida Reported Through 2012. 2013.
(4) Antiretroviral Therapy Cohort Collaboration. Causes of death in HIV-1-infected patients treated with antiretroviral therapy, 1996-2006: collaborative analysis of 13 HIV cohort studies. Clin Infect Dis . 2010;50(10):1387-1396.
(5) Darbyshire J. Therapeutic interventions in HIV infection - a critical view. Trop Med Int Health . 2000;5(7):A26-31.
(6) Gebhardt M, Rickenbach M, Egger M. Impact of antiretroviral combination therapies on AIDS surveillance reports in Switzerland. Swiss HIV Cohort Study. AIDS .
1998;12(10):1195-1201.
(7) Murphy EL, Collier AC, Kalish LA et al. Highly active antiretroviral therapy decreases mortality and morbidity in patients with advanced HIV disease. Ann Intern Med . 2001;135(1):17-26.
(8) Tiozzo E, Jayaweera D, Rodriguez A et al. Short-term combined exercise training improves the health of HIV-infected patients . Journal of AIDS and HIV Research . 2013;5(3):80-89.
(9) Lichtfuss GF, Hoy J, Rajasuriar R, Kramski M, Crowe SM, Lewin SR. Biomarkers of immune dysfunction following combination antiretroviral therapy for HIV infection. Biomark Med . 2011;5(2):171-186.
(10) Leow MK, Addy CL, Mantzoros CS. Clinical review 159: Human
immunodeficiency virus/highly active antiretroviral therapy-associated metabolic syndrome: clinical presentation, pathophysiology, and therapeutic strategies. J Clin Endocrinol Metab . 2003;88(5):1961-1976.
(11) Pearson TA, Mensah GA, Alexander RW et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: A statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation . 2003;107(3):499-511.
21 (12) Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest . 2003;111(12):1805-1812.
(13) Nixon DE, Landay AL. Biomarkers of immune dysfunction in HIV. Curr Opin HIV AIDS . 2010;5(6):498-503.
(14) Neuhaus J, Jacobs DR,Jr, Baker JV et al. Markers of inflammation, coagulation, and renal function are elevated in adults with HIV infection. J Infect Dis .
2010;201(12):1788-1795.
(15) Baker J, Ayenew W, Quick H et al. High-density lipoprotein particles and markers of inflammation and thrombotic activity in patients with untreated HIV infection. J Infect Dis . 2010;201(2):285-292.
(16) Boulware DR, Hullsiek KH, Puronen CE et al. Higher levels of CRP, D-dimer, IL-6, and hyaluronic acid before initiation of antiretroviral therapy (ART) are associated with increased risk of AIDS or death. J Infect Dis . 2011;203(11):1637-1646.
(17) Lau B, Sharrett AR, Kingsley LA et al. C-reactive protein is a marker for human immunodeficiency virus disease progression. Arch Intern Med . 2006;166(1):64-70. (18) Rodger AJ, Fox Z, Lundgren JD et al. Activation and coagulation biomarkers are independent predictors of the development of opportunistic disease in patients with HIV infection. J Infect Dis . 2009;200(6):973-983.
(19) O'Brien K, Nixon S, Tynan AM, Glazier R. Aerobic exercise interventions for adults living with HIV/AIDS. Cochrane Database Syst Rev . 2010;(8):CD001796.
doi(8):CD001796.
(20) O'Brien K, Tynan AM, Nixon S, Glazier RH. Effects of progressive resistive exercise in adults living with HIV/AIDS: systematic review and meta-analysis of randomized trials. AIDS Care . 2008;20(6):631-653.
(21) ACSM's Guidelines for Exercise Testing and Prescription. Ninth ed. Baltimore, MD: Wolters Kluwer|Lippincott Williams & Wilkins . 2009.
(22) Arikawa AY, Thomas W, Schmitz KH, Kurzer MS. Sixteen weeks of exercise reduces C-reactive protein levels in young women. Med Sci Sports Exerc .
2011;43(6):1002-1009.
(23) Ford ES. Does exercise reduce inflammation? Physical activity and C-reactive protein among U.S. adults. Epidemiology . 2002;13(5):561-568.
22 (24) Kohut ML, McCann DA, Russell DW et al. Aerobic exercise, but not
flexibility/resistance exercise, reduces serum IL-18, CRP, and IL-6 independent of beta-blockers, BMI, and psychosocial factors in older adults. Brain Behav Immun .
2006;20(3):201-209.
(25) Campbell PT, Campbell KL, Wener MH et al. A yearlong exercise intervention decreases CRP among obese postmenopausal women. Med Sci Sports Exerc . 2009;41(8):1533-1539.
(26) Kelley GA, Kelley KS. Effects of aerobic exercise on C-reactive protein, body composition, and maximum oxygen consumption in adults: a meta-analysis of randomized controlled trials. Metabolism . 2006;55(11):1500-1507.
(27) Kline GM, Porcari JP, Hintermeister R et al. Estimation of VO2max from a one-mile track walk, gender, age, and body weight. Med Sci Sports Exerc . 1987;19(3):253-259. (28) Maruf FA, Akinpelu AO, Salako BL. Self-reported quality of life before and after aerobic exercise training in individuals with hypertension: a randomised-controlled trial. Appl Psychol Health Well Being . 2013;5(2):209-224.
(29) National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation . 2002;106(25):3143-3421.
(30) United States Census Bureau. State and County QuickFacts. Available at: http://quickfacts.census.gov/qfd/states/00000.html. Accessed 05/18, 2014.
(31) Meredith K, Delaney J, Horgan M, Fisher E,Jr, Fraser V. A survey of women with HIV about their expectations for care. AIDS Care . 1997;9(5):513-522.
(32) Kelly PJ, Cordell JR. Recruitment of women into research studies: a nursing perspective. Clin Nurse Spec . 1996;10(1):25-28.
(33) MacArthur RD, Levine SD, Birk TJ. Supervised exercise training improves cardiopulmonary fitness in HIV-infected persons. Med Sci Sports Exerc . 1993;25(6):684-688.
(34) Neidig JL, Smith BA, Brashers DE. Aerobic exercise training for depressive symptom management in adults living with HIV infection. J Assoc Nurses AIDS Care . 2003;14(2):30-40.
(35) Miller M, Zhan M, Havas S. High attributable risk of elevated C-reactive protein level to conventional coronary heart disease risk factors: the Third National Health and Nutrition Examination Survey. Arch Intern Med . 2005;165(18):2063-2068.
23 (36) Smith BA, Neidig JL, Nickel JT, Mitchell GL, Para MF, Fass RJ. Aerobic exercise: effects on parameters related to fatigue, dyspnea, weight and body composition in HIV-infected adults. AIDS . 2001;15(6):693-701.
(37) Lindegaard B, Hansen T, Hvid T et al. The effect of strength and endurance training on insulin sensitivity and fat distribution in human immunodeficiency virus-infected patients with lipodystrophy. J Clin Endocrinol Metab . 2008;93(10):3860-3869.
(38) Gomes Neto M, Ogalha C, Andrade AM, Brites C. A systematic review of effects of concurrent strength and endurance training on the health-related quality of life and cardiopulmonary status in patients with HIV/AIDS. Biomed Res Int . 2013;2013:319524. (39) Hand GA, Lyerly GW, Jaggers JR, Dudgeon WD. Impact of aerobic and resistance exercise on the health of HIV-infected persons. Am J Lifestyle Med . 2009;3(6):489-499. (40) DAD Study Group, Friis-Moller N, Reiss P et al. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med . 2007;356(17):1723-1735.
(41) Fontas E, van Leth F, Sabin CA et al. Lipid profiles in HIV-infected patients
receiving combination antiretroviral therapy: are different antiretroviral drugs associated with different lipid profiles? J Infect Dis . 2004;189(6):1056-1074.
(42) Borato DC, Parabocz GC, Ribas SR et al. Changes of metabolic and inflammatory markers in HIV infection: glucose, lipids, serum Hs-CRP and myeloperoxidase.
Metabolism . 2012;61(10):1353-1360.
(43) Jacobson DL, Tang AM, Spiegelman D et al. Incidence of metabolic syndrome in a cohort of HIV-infected adults and prevalence relative to the US population (National Health and Nutrition Examination Survey). J Acquir Immune Defic Syndr .
2006;43(4):458-466.
(44) Wand H, Calmy A, Carey DL et al. Metabolic syndrome, cardiovascular disease and type 2 diabetes mellitus after initiation of antiretroviral therapy in HIV infection. AIDS . 2007;21(18):2445-2453.
(45) Palacios R, Santos J, Gonzalez M, Ruiz J, Marquez M. Incidence and prevalence of the metabolic syndrome in a cohort of naive HIV-infected patients: prospective analysis at 48 weeks of highly active antiretroviral therapy. Int J STD AIDS . 2007;18(3):184-187. (46) Worm SW, Friis-Moller N, Bruyand M et al. High prevalence of the metabolic syndrome in HIV-infected patients: impact of different definitions of the metabolic syndrome. AIDS . 2010;24(3):427-435.