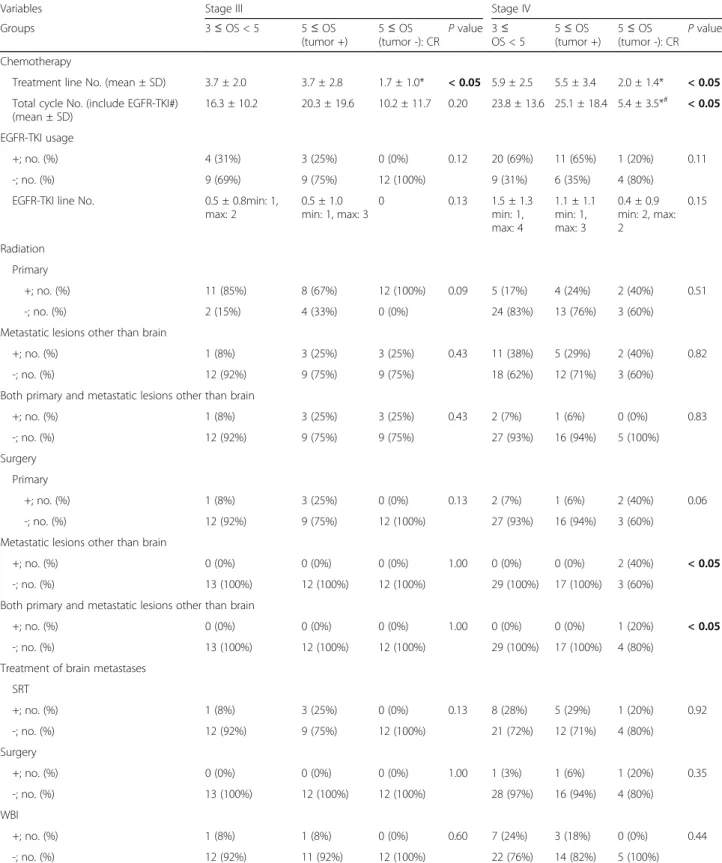
Analysis of key clinical features for achieving complete remission in stage III and IV non-small cell lung cancer patients
Full text
Figure





Related documents
The Court stressed that Congress intended that the FCC's regulation of broadcasters would preserve as much of the broadcasters' editorial discretion as pos- sible.' In
BC: Proposed model using Box-Cox transformation without sign inversion; BC-SI: Proposed model using Box-Cox transformation with sign inversion; EXP: Shifted exponential
In Albany, negative fiscal impacts increase as the number of charter school students drawn from the private sector increases because the additional state aid those students
We have proved the existence and uniqueness result of the nonlocal Robin boundary prob- lem for a fractional Hahn integrodifference equation (1.7) by using the Banach fixed point
Figure 5 – As in the previous Figure, this graph is showing the occurrence in the first five canti of Paradiso of the words Amore, Paura, Lume, Notte, Pena, Luce, Dolore, Fede,
has studied medicine in a medical school located outside the United States which is recognized by the World Health Organization; has completed all of the formal requirements of the
level of maturity shows an average value of 12.4 which indicate that studied samples of the area are immature.. The implication, therefore, is
Based on sharia banking products, shariah banking users mostly know the sharia banking products well, while the rest only know but not specifically sharia banking products.
