Linking Population, Health, and
the Environment: An Overview of
Integrated Programs and
a Case Study in Nepal
Sigrid Hahn, MD, MPH,
1Natasha Anandaraja, MD, MPH,
1and Leona D’Agnes, BS
21Mount Sinai School of Medicine, New York, NY 2PATH Foundation Philippines, Inc., Makati City, Philippines
OUTLINE
METHODS
OVERVIEW OF THEPOPULATION, HEALTH, ENVIRONMENTAPPROACH
Potential Strengths of the Population, Health, Environment Approach Structure of Population, Health,
Environment Collaborations
Potential Weaknesses of the Population, Health, Environment Approach
CASESTUDY INNEPAL: INTEGRATINGPOPULATION, HEALTH ANDFORESTMANAGEMENTAGENDAS
Project Inputs and Implementation Project Activities
Interim Results Project Challenges
Keys to Success and Lessons Learned
CONCLUSION
ABSTRACT
Population, health, and environment programs are cross-sectoral development initiatives that link con-servation, health, and family planning interventions. These programs are generally located in biodiver-sity hotspots, where population pressure is among
Address Correspondence to: Sigrid Hahn
Department of Emergency Medicine
Mount Sinai School of Medicine New York, NY
Email: [email protected]
the factors contributing to environmental degrada-tion. This review describes the general structure of population, health, and environment programs and provides selected examples to highlight vari-ous aspects of this approach. We focus in depth on a case study from the Integrating Population and Health into Forestry Management Agendas program in Nepal that simultaneously addressed deforesta-tion from fuel-wood harvesting, indoor air pollu-tion from wood fires, acute respiratory infecpollu-tions related to smoke inhalation, as well as family planning in communities in Nepal’s densely pop-ulated forest corridors. Keys to the success of the Nepal project included empowerment of commu-nity forest user groups with population, health, and environment program know-how and appro-priate technology. Lessons learned in Nepal point to the critical role that nongovernmental organiza-tions can play as catalysts of cross-sectoral responses to complex development issues such as this one. The population, health, and environment approach can be an effective method for achieving sustain-able development and meeting both conservation and health objectives.Mt Sinai J Med 78:394 – 405, 2011.2011 Mount Sinai School of Medicine
Key Words:community-based forestry management, cross-sectoral development, ecohealth, family plan-ning, interdisciplinary approach, PHE, population health environment.
The pressure of human activities on natural ecosys-tems is pervasive and increasing. Human-induced changes in the global environment include climate change, deforestation and desertification, degrada-tion of freshwater sources and marine environments, introduction of pollutants, and widespread biodiver-sity loss. These changes not only negatively impact the natural world, but also have significant implica-tions for human health and well-being. The impact Published online in Wiley Online Library (wileyonlinelibrary.com).
of these changes on humans includes direct effects, such as exposure to pollutants; ecosystem-mediated health impacts, such as decreased food and water security; and indirect or deferred impacts, such as environment-mediated population displacement.1 Ecosystem-mediated health impacts and ecosystem services may be particularly important in develop-ing countries, where local communities often rely upon subsistence agriculture and hunting or fish-ing for their food supply, local rivers or lakes for potable water, timber for fuel, and forest or marine products to supplement their income. Unsustainable use of ecosystems services in low-income settings,
Ecosystem-mediated health
impacts and ecosystem services
may be particularly important in
developing countries, where local
communities often rely upon
subsistence agriculture and
hunting or fishing for their food
supply, local rivers or lakes for
potable water, timber for fuel, and
forest or marine products to
supplement their income.
however, often takes place in or near biodiversity-rich areas where unsustainable patterns of resource extraction may be contributing to biodiversity loss and environmental degradation. These problems are often exacerbated by a high population density and a rapid rate of population growth, due to both high fertility and ‘‘frontier migration.’’2 Therefore, there is a common link between the goals of many conser-vation, health, and family-planning initiatives.
There are a number of cross-sectoral approaches to conservation and health that share the same overall goals but differ somewhat in their specific focus. For example, conservation medicine seeks to ‘‘develop a scientific understanding of the rela-tionship between the environmental crisis and both human and nonhuman animal health,’’ and literature in the field is focused largely on the emergence or re-emergence of zoonotic diseases.3 The Canadian International Development and Research Centre’s ‘‘ecosystem approach to human health’’ focuses on ‘‘resource management subject to the sustainable and equitable improvement of human health, as well as the health of the ecosystem itself.’’ The ecosys-tem approach uses community-based participatory research, and puts human health and gender equity at the center of their agenda.4The One Health initiative
‘‘seeks to promote, improve, and defend the health and well-being of all species by enhancing coopera-tion and collaboracoopera-tion between physicians, veterinar-ians, [and] other scientific health and environmental professionals.’’5 The One Health movement notes that the health of wildlife, domestic animals, and humans intersects at the edge of most protected areas, as well as throughout large swaths of dry-land pastoral systems. In these areas, organizations such as the Bio-Economy Africa and Wildlife Conservation Society look for interventions that improve livestock management for the benefit of human communities as well as surrounding wildlife populations, which are vulnerable to diseases transmitted from both humans and livestock.6,7
The integrated population, health, environment (PHE) method shares similarities with the aforemen-tioned approaches, but has the main objective of simultaneously improving ‘‘access to family planning and related health services while helping commu-nities manage their natural resources, with the goals both of improving people’s health and livelihood and conserving wildlife and other biological resources.’’8 Achieving universal access to reproductive healthcare and fulfilling the unmet need for family planning,
The main objective of the
integrated population, health,
environment approach to
conservation and health is to
improve access to family planning
and related health services while
simultaneously helping
communities manage their
natural resources, with the goals
of both improving people’s health
and livelihood and conserving
wildlife and other biological
resources.
which is one of the targets of Millennium Develop-ment Goal (MDG) 5, is seen as key to achieving most of the other MDGs, including MDG 7 (achieve envi-ronmental sustainability).9 Population, health, envi-ronment programs often also incorporate a range of other development efforts, from poverty reduction to food security to gender equity. They are particu-larly well suited to areas of high biodiversity where population pressure is a central issue for conservation and/or sustainable development. The PHE approach is less efficient in areas of low population density
and less appropriate in areas of low ecological value or regions where the environment is so severely degraded that it would require restoration.10
This review describes the design of PHE pro-grams and examines selected literature in the field. A case study from the Integrating Population and Health into Forestry Management Agendas in Nepal is then discussed in detail, in order to highlight key aspects of this approach. We review keys to successful imple-mentation and lessons learned from the Nepal case.
METHODS
Peer-reviewed journal articles for this nonsystem-atic review were identified using combinations of the following MeSH terms in PubMed searches: ‘‘biodiversity,’’ ‘‘environmental health,’’ ‘‘family plan-ning services,’’ ‘‘conservation of natural resources,’’ and ‘‘forestry.’’ Reports, master’s theses, program evaluations, and other relevant scholarly writings were also identified through Google and Google Scholar searches, and via personal communication with practitioners in the field, including at US Agency for International Development (USAID), one of the major funding bodies for PHE programs. Data for the case study were analyzed using an online statis-tics calculator. Studentt tests were used to compare proportions, and a P value <0.05 was considered significant.
OVERVIEW OF THE POPULATION,
HEALTH, ENVIRONMENT APPROACH
Although integrated conservation and development projects predate the 1990s, during this decade a large number of PHE programs were launched, largely funded by grants from private philanthropies, includ-ing the Packard, Summit, MacArthur, Hewlett, and Turner foundations.8,11In 2002, USAID began to fund PHE programming in response to language included in a foreign operations appropriations bill, which stated that under the Child Survival and Health Pro-grams Fund, some portion of the funds for family planning/reproductive health should be allocated in areas where population growth threatens biodiver-sity or endangered species.12 The USAID funding complemented support from these private founda-tions, with grants going to a number of international conservation agencies, including the Jane Goodall Institute, World Wildlife Fund (WWF), Conservation International, and Madagascar Wildlife Conservation Society.8
Currently, a number of projects worldwide combine reproductive health and family planning with capacity-building for local natural resource management, often integrating alternative livelihood and poverty-alleviation programs, nonformal educa-tion, or other healthcare initiatives as well. These include projects found in the Philippines, Cambodia, India, Nepal, Cameroon, the Democratic Repub-lic of the Congo, Central African RepubRepub-lic, Kenya, Madagascar, Mozambique, Rwanda, Tanzania, Sudan, Ethiopia, and Uganda.11,13 These projects are cen-tered near high-value conservation sites, usually forests, watersheds, or coastal wetlands and marine habitats that are threatened by population pressures, weak governance, and poverty-driven unsustainable resource use.
Potential Strengths of the Population,
Health, Environment Approach
There are philosophical and practical rationales for cross-sectoral collaboration (Table 1). It has been argued that there is a natural alliance between con-servation, development, and public health, based on the idea that human and ecosystem health are inte-grally linked. Although single-sector approaches may achieve a specific outcome in their field, it may be
There are philosophical and
practical rationales for
cross-sectoral collaboration. It has
been argued that there is a
natural alliance between
conservation, development, and
public health, based on the idea
that human and ecosystem health
are integrally linked.
to the detriment of other measures of ecosystem or human health. For example, conservation initia-tives that do not take into account the well-being of local people may end up harming communities (for example, by obstructing their use of natural resources on which they depend for sustenance). In contrast, combined programs have the potential to positively impact multiple sectors at once, and ideally can provide ‘‘value added’’ or synergy when linked, resulting in greater community buy-in and inter-vention uptake.10 Conservation and public health organizations can mutually benefit from the trust and relationships they have built within the community,
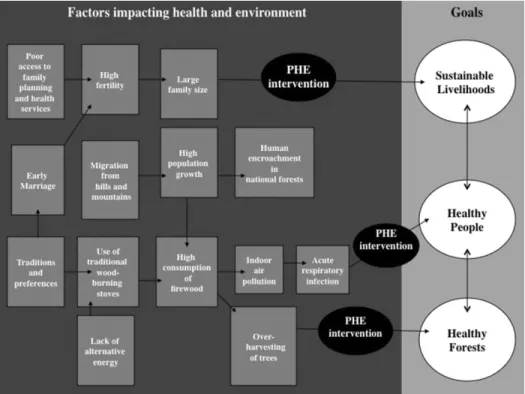
Fig 1. Conceptual framework underlying the Integrating Population and Health into Forestry Management Agendas project in Nepal.Abbreviations:PHE, population, health, and environment.
and programmatic elements such as information, edu-cation, and communication strategies can be linked. As such, the PHE approach can be cost-effective when development agencies are able to combine resources for additive benefit.11
Structure of Population, Health,
Environment Collaborations
The nature and design of PHE collaborations often varies greatly depending on local factors and stakeholders.14 In some cases, the health issues may not be directly linked to conservation concerns, but an existing health program can provide an entry point for a conservation program in the community. Con-versely, collaborations can also be beneficial when conservation groups are established in very remote areas where health and family service are sorely needed but the infrastructure is lacking for healthcare service delivery. Healthcare providers can piggyback on the structure that the conservation group has put in place. An example of this is in the buffer zone surrounding Gorongosa National Park in Mozam-bique. The Carr Foundation entered into a 20-year partnership with the government of Mozambique to restore and develop the national park as part of the Gorongosa Restoration Project. Surrounding the park
is a rural ‘‘buffer zone’’ that is home to approxi-mately 200,000 people who have very limited access to healthcare. The project launched a mobile clinic program, using conservation vehicles and staff, and is working on a community health worker program, because the government Ministry of Health does not have the capacity to outreach to these remote vil-lages on the outskirts of the national park and is relying on partners to reach these areas (personal communication).
Another benefit of cross-sectoral work is that natural resource and development programs can be a means for reaching men and adolescent boys, who otherwise may be overlooked by family planning or other health programs. For example, a nongovern-mental organization (NGO), Project Concern Interna-tional, sought to involve males in family planning.15 It worked with community-development groups to integrate family planning into water and sanitation development projects in El Salvador. A majority of Project Concern International workers were male, and prior projects had already engaged large numbers of male community members. In 13 rural villages, family-planning topics were integrated into ongoing educational activities conducted during community mobilization and the construction of water systems and latrines. Knowledge, attitudes, and behavior were evaluated, with significant increases in contraceptive
use, as well as diffusion of knowledge to community members not directly engaged in the project. This is also an example of a project that integrated its messaging and educational activities, even though the family-planning and environmental-health goals were not directly related.
In the Philippines, PATH Foundation Philippines developed a PHE program targeted to young people (aged 15–19 years) in coastal areas. The program’s information, education, and communication cam-paign encouraged youth to become ‘‘stewards’’ of the environment and their sexuality. Results indicate that youth–especially young men–were more likely to use family planning and delay early sex in the PHE program site compared with their counterparts in a comparison site where conventional reproductive health messages were delivered to youth.16
In other cases, the solutions to the health and conservation issues are symbiotic. Family planning in areas of high maternal and infant mortality and high population pressure on the environment could be an example of this, with improved child and mater-nal health as a result of birth spacing, and reduced demand and consumption of resources due to a more slowly growing population. Another example of a solution that benefits both health and conservation is when fuel-efficient cookstoves reduce the need
In many cases, the solutions to the
health and conservation issues are
symbiotic. An example is improved
child and maternal health as a
result of birth spacing, and
reduced demand and
consumption of resources due to
a more slowly growing population.
for timber harvesting while also reducing the health impact of indoor air pollution. The Integrating Popu-lation and Health into Forestry Management Agen-das project in Nepal, described in detail below, illustrates this concept.Collaborative programs may generate greater impacts on public health and conservation outcomes than independently implemented interventions. The PATH Foundation Philippines’ Integrated Population and Coastal Resource Management (IPOPCORM) ini-tiative used an interdisciplinary approach to address overfishing and high population growth in coastal Philippines.17 Its central organizing theme was food security, assuring people’s access to an affordable and sustainable supply of marine protein in these
fisherfolk households with pervasive poverty and high rates of childhood malnutrition. IPOPCORM encouraged the integration of community-based reproductive health and family-planning strategies into coastal resource–management policies and agendas. It was implemented in 33 municipalities within 12 areas ranked as extremely high priority for marine conservation. Working through people’s organizations and other local institutions, IPOPCORM also conducted operations research that used a quasi-experimental design to test the hypothesis that inte-grated PHE approaches generate synergy and higher impact than single-sector programs. Multiple regres-sion analyses found that outcomes were improved for several biodiversity conservation indicators in the areas with a combined intervention (coastal resource management plus reproductive health), compared with a decline or stagnation of these same indica-tors in the independently administered intervention areas. There were also statistically significant trends toward improved outcomes for population (declin-ing parity), family plann(declin-ing (increas(declin-ing contraceptive use), and poverty reduction in the combined inter-vention areas. To ensure the long-term sustainability of conservation gains, the policy implications of this study underscore the necessity for concurrent effort to reduce unmet need for family planning in high-growth biodiversity hotspot areas. The study also demonstrated the feasibility and benefits of working through local institutions to simultaneously deliver conservation and family-planning services to remote communities.
Potential Weaknesses of the Population,
Health, Environment Approach
There are several challenges associated with using the PHE approach. The cross-sectoral structure of these programs can make funding difficult to secure, because most grants are given within specific fields. Other challenges associated with cross-sectoral work include lack of a common terminology across disciplines, differing research and programmatic approaches, and most important, differing outcome priorities.
Regarding the family planning aspect of PHE, some have made ethical arguments against the PHE approach because of the concern that it tends to blame environmental degradation on poor commu-nities, and specifically on poor women’s fertility.8 This is particularly notable given that funding agen-cies are generally from northern countries, where unsustainable consumption is responsible for so much environmental degradation. There is, however,
a well-documented need for family planning, with an estimated 215 million women in the developing world preferring to avoid a pregnancy yet not having access to modern contraceptives.18The Demographic and Health Surveys (and the earlier World Fertility Surveys) have demonstrated that in nearly all devel-oping countries, couples are having more children than they intended.19 Since the Cairo International Conference on Population and Development in 1994, family-planning initiatives have been rooted in a needs-based and client-centered approach, with the goal of providing comprehensive reproductive health services, and have moved away from the older con-cept of ‘‘population control.’’ Finally, many PHE programs have not published quantitative impact data, and indicators documenting the added ben-efit of the integrated approach are often lacking. Because the PHE approach is cross-sectoral, impact measures are often more difficult and expensive to track than for single-sector programs. In addition, many of the family planning and environmental indi-cators are long-term, and do not fall within the shorter funding terms and life spans of PHE projects.8 The aforementioned IPOPCORM research project, how-ever, does show that it is possible to measure such data with long-term support from sponsors. In an attempt to address the limitations of monitoring and evaluating PHE programs, the MEASURE (Monitoring and Evaluation to Assess and Use Results) Evaluation and USAID published a manual outlining recom-mended indicators that are grouped in 5 categories: population, health, environment, integration, and value-added, and based on actual indicators that have been tested and used in PHE projects in the Philippines, Madagascar, and other countries.20
CASE STUDY IN NEPAL:
INTEGRATING POPULATION, HEALTH
AND FOREST MANAGEMENT
AGENDAS
The Integrating Population and Health Into Forestry Management Agendas in Nepal pilot is an example of a sustainable PHE project that is centered around interrelated health, environment, energy, and poverty issues common to developing countries, including the following:
1. The high incidence of child mortality associated with acute respiratory infections (ARIs) linked to indoor air pollution from traditional wood-burning stoves.
2. Unsustainable levels of tree harvesting leading to deforestation, loss of biodiversity, and loss of
ecosystem services, thus contributing to poverty among forest-dependent people.
3. The tradition of early marriage and childbearing, combined with an unmet need for family planning, resulting in high fertility and population growth and increasing pressure on the environment.
To effectively address these interrelated factors, the project worked with local Community Forest User Groups (CFUGs) to incorporate into their forestry-management programs a package of health and family-planning interventions that were appropriate for local conditions and culture, and promote sus-tainability through close involvement with these local institutions (Figure 1).
Community Forest User Groups emerged in Nepal in 1978 as a vehicle for a nationwide commu-nity forestry strategy aimed at preventing deforesta-tion and habitat loss. The CFUGs were composed of several households charged with protecting, manag-ing, and using a tract of state-owned forest consigned to them by the District Forestry Office according to the terms of the community forest operational plan. The plan details the community’s responsibility for the sustainable management of forest resources and the circumstances under which it is permitted to harvest forest products for its members’ use and to sell surplus to nonmembers at market rates. Twenty-five percent of income from such sales was to be directed toward forestry protection and manage-ment activities.21 The model proved successful and was operationalized across Nepal, and currently 35% of the country’s population is engaged in natural resource management through CFUGs.22
In 2006, a USAID review of one such project revealed success in promoting the capacity of CFUGs to manage forest resources in a socially inclusive and sustainable manner, and demonstrated the beneficial effect of these actions on biodiversity conservation.23 However, the report also noted several factors still negatively impacting natural-resource use and health in CFUG communities. Although alternative fuel sources had been promoted to reduce consump-tion of wood and resulting deforestaconsump-tion, the link between the use of traditional wood stoves, indoor air pollution, and respiratory infections had not been explicitly made, and death from ARIs, especially in children, remained a major concern in CFUG commu-nities. Lack of access to health services and modern family-planning methods, as well as high fertility and population density in these communities, were also noted in the assessment. In addition, migra-tion of men from the villages into India for seasonal work exacerbated human immunodeficiency virus
(HIV)/acquired immune deficiency syndrome (AIDS) transmission among this population.
Based on these findings, it was recommended that 3 areas of intervention should be integrated into the natural-resource management and governance activities of the CFUGs to enable them to meet local health needs and strengthen their conservation out-comes: ARI prevention measures, HIV/AIDS educa-tion, and promotion of family planning. Toward this end, USAID/Nepal supported a pilot project, Integrat-ing Population and Health into Forestry Management Agendas in Nepal, that used a variety of methods to establish channels within existing CFUG activities to promote awareness of and access to HIV and ARI prevention practices, and family-planning methods.
Project Inputs and Implementation
The PHE pilot was implemented by 2 local NGOs working in partnership with USAID: WWF and the Resource Identification and Management Soci-ety (RIMS). A third agency, ADRA-Nepal, assisted the 2 NGOs with family-planning activities. The third author provided technical backstopping for the PHE integration and monitoring. Because WWF’s project was examined in a previous article,24 this case high-lights the work done with RIMS, which had already implemented forestry projects with CFUGs in the Mid-hills district of Dhading, including USAID-sponsored activities to strengthen actions for good governance and utilization of natural resources. In preparation for the implementation of the Integrating Population and Health project, RIMS staff trained and mentored CFUG members to become PHE outreach workers, peer educators, improved cookstove (ICS) promoters, and community-based distributors of contraceptives. The RIMS field teams then worked directly with CFUGs in 9 Village Development Committees (VDCs) of Dhading to implement the pilot project activities.23 These activities promoted cooperation across health, forestry, and energy sectors, with the aim of minimiz-ing redundancies in services and leveragminimiz-ing available resources.25Project Activities
Initial activities focused on education at several levels within the CFUG communities. Traditional media, nonformal education channels, and inter-personal communication were utilized to advocate for the selected PHE activities among VDC leaders, CFUG executives, and staff of the local district health and forestry offices. Through these activities, RIMS
sought to promote an understanding of intercon-nected population-environment dynamics in Nepal’s forests and how family planning and clean energy use can reduce pressures on limited natural resources and improve family livelihoods through savings in time and money, and better health.25
Peer educators, versed in all intervention areas, delivered integrated messages to community mem-bers and facilitated group interactions among CFUG members that increased awareness of the need to ‘‘plan the family and protect the environment’’ in order to ensure adequate forest resources for future generations.26Street dramas, radio jingles, and school-based initiatives were utilized to good effect to reinforce integrated PHE messaging. The RIMS field
Peer educators, versed in all
intervention areas, delivered
integrated messages to community
members and facilitated group
interactions among Community
Forest User Group members that
increased awareness of the need to
‘‘plan the family and protect the
environment’’ in order to ensure
adequate forest resources for
future generations.
staff also promoted discussions with adult groups about HIV/AIDS and reproductive health rights. Non-formal education classes were used to combine liter-acy skills-building activities with reproductive health, family planning, and PHE messaging for women and girls in the communities.
Demand for, and supply of, clean energy tech-nology was increased through door-to-door stag-ing by ICS promoters who also served as family planning educators. Local men and women received training from RIMS in construction of ICS using hand-made bricks to build stoves that were more fuel efficient and had reduced emissions compared with traditional wood-burning stoves. Biogas units were installed in some households, using mixed human and animal waste to produce methane gas that was then piped to the nearby kitchen and used for cook-ing. The NGOs’ field staff also met monthly with female community health volunteers to track the numbers of child ARI cases that were seen, treated or referred, and to discuss issues of family plan-ning and general health in the community and their interrelationship with forest health.25
Table 1. Potential Strengths and•Weaknesses of the PHE Approach. Strengths
Holistic approach based on the link between healthy people and healthy ecosystems
Public health and conservation organizations may capitalize on each other’s connections and goodwill within the community
Information, education, and communication programs can be integrated, and synergistic health and conservation solutions may be identified
Can be cost-effective when NGOs are able to combine resources for additive benefit Weaknesses
Cross-sectoral nature of work does not fit within traditional funding models May be a lack of a common terminology or vocabulary across disciplines Differing research approaches across disciplines
Public health and conservation specialists may have differing priorities
Complex, cross-sectoral programs and long-term indicators make gathering impact data difficult If too broad, the PHE approach can dilute interventions and impacts
Abbreviations:NGOs, nongovernmental organizations; PHE, population, health, and environment.
Within the project, partnerships and coordina-tion activities promoted cooperacoordina-tion between dif-ferent sectors, local authorities, and programs. This level of integration reduced redundancies among the various players in the project area and leveraged additional resources to support PHE activities. Uti-lizing local resource persons who had previously been trained for conservation and governance activ-ities to work with peer educators on delivering PHE outreach education through informal communication channels contributed to the integration of health and environmental messaging at a community level.26
Interim Results
The PHE outreach workers and peer educators collected baseline data from the RIMS projects sites in October 2006 and every 6 months there-after. The data were verified and triangulated with other sources of information obtained by the dis-trict health and forestry offices, and the project information system. Follow-up data on health out-comes showed success in both increasing family planning and alternative-energy uptake and decreas-ing ARI cases and referral rates (Table 2). By March 2009, the contraceptive prevalence rate had increased from a baseline of 44% to 68.7%. An increase in adoption of family planning and clean
Follow-up data on health
outcomes have shown success in
both increasing family planning
and alternative-energy uptake
and decreasing acute respiratory
infection cases and referral rates.
energy technologies was seen by RIMS after imple-menting street drama as an educational intervention. An increase in demand for condoms occurred after peer education focusing on the dual benefit of pregnancy prevention and reduced transmission of sexually transmitted infections.26,27
Data on ARI cases reflect a seasonal cycle of peak incidence during the first 3 months of the year. By March 2009, the number of ARI cases (n=301) had dropped to<50% the number recorded in March 2007 (n=690). The declining ARI trend was inversely proportional to the trend in clean energy use, which increased from 22% of CFUG households in 2006 to 40.5% by 2009. These data suggest the possibility of reduced ARIs through better fuel-sourcing strategies, but other parallel activities may have contributed to this trend, particularly training of the female commu-nity health volunteers in ARI case management, and improved monitoring and promotion of preventive practices.26,27
The environmental impacts of the pilot project were also significant. The 2407 CFUG households that had adopted clean sources of energy were col-lectively saving an estimated 3583 metric tons of firewood annually (equivalent to 8958 trees). In addi-tion to the benefits of reducing loss of forest cover and preservation of forest biodiversity, economic and social benefits were seen as well. Beneficiaries
The 2407 Community Forest User
Group households that had
adopted clean sources of energy
were collectively saving an
estimated 3583 metric tons of
firewood annually (equivalent to
8958 trees).
Table 2. Integrating Population and Health into Forestry Management Agendas Outcome Data for RIMS Project Areas
in Nepal (October 2006–March 2009).
Outcome Indicator Baseline, October 2006 March 2007 October 2007 March 2008 October 2008
End of Project Cycle, March 2009 Eligible couples using
modern FP methods
44.0% 50.6% 54.6% 57.0% 63.1% 68.7%∗ No. of couples of
reproductive age currently using any modern FP method
2682/6050 3061/6050 3532/6473 3691/6473 4084/6473 4448/6473
No. of children aged<5 y with ARI signs and symptoms seen by FCHVs
690 337 481 365 301
ARI case referrals 55% 43% 16% 5.5% 5.0%∗ No. of ARI cases referred
for treatment/total number of ARI cases seen by the FCHVs
380/690 145/337 77/481 20/365 15/246
Households using clean energy
22.0% 26.5% 28.2% 32.3% 37.2% 40.5%∗ No. of households using
ICS or biogas/total no. of households
1175/5344 1417/5344 1677/5945 1921/5945 2213/5945 2407/5945
Estimated metric tons of firewood saved by households using ICS or biogas
2106 2348 2650 2891 3284 3583
Abbreviations:ARI, acute respiratory infection; FCHVs, female community health volunteers; FP, family planning; ICS,
improved cook stove; RIMS, Resource Identification and Management Society.
∗P<0.01 indicates statistically significant change from baseline or first available data point.
reported fewer episodes of eye and respiratory problems, resulting in less time away from work and school, reduced expenditures on medical care, reduced time and labor spent on foraging for wood, and increased household fuel efficiency.26,27
Project Challenges
The project faced several challenges during imple-mentation. Initially, district forestry office officials were concerned that the new PHE approach would distract CFUGs from their primary forest management and stewardship responsibilities. This was effectively addressed by advocacy efforts highlighting ‘‘health is wealth’’ messages linking PHE goals to reduction in consumption of forest resources.
Another issue was the communities’ expectation that the project would provide them with income-generating opportunities, which it did not have resources to support. The Resource Identification and Management Society overcame this by educating the community about the cost savings that accrue to fam-ilies that use alternative energy and practice birth spacing, explaining that the long-term benefits of
such practices were greater than the short-term gains from a dedicated income-generating activity. Another challenge related to the cost of alternative energy. The price of the biogas installation was beyond the reach of most CFUG families, even with the subsidy provided by the government. Thus most households opted for the ICS, which was still beyond the means of the poorest families in the CFUG. The Resource Identification and Management Society overcame this barrier by finding alternative funding for the most marginalized community members, convincing the CFUG Executive Committee to earmark a portion of the group’s community development funds as grants to indigent households for installation of ICS. In other villages, RIMS persuaded the local government to subsidize ICS units for poor families, and in one subdistrict they found a local development bank to sponsor ICS installation for a number of indigent families.26,27
Keys to Success and Lessons Learned
The Integrating Population and Health into Forestry Management Agendas in Nepal project was uniquein that it was able to implement the integrated PHE strategy among a large number of CFUGs and achieve significant results in a short period of time, despite limited funding. Furthermore, the mechanism needed to sustain the interventions was put in place via the CFUGs’ successful addition of the family planning and alternative-energy activities to their community forest operational plans, effective through 2012.25
The project had a positive influence on the health practices and pro-environment behaviors of people in the target communities, which can be attributed, in part, to the effective cross-sectoral collaboration catalyzed by RIMS. This played an instrumental role in bringing PHE issues to the attention of the VDCs and assisting VDC leaders to petition relevant ministries (health, forestry, and local development) for improved service delivery. By strengthening the VDCs’ capacity to coordinate the local development inputs of various actors and organizations (government, NGO, civil society, and commercial groups), RIMS also enabled a conver-gence of resources for PHE activities that otherwise would not have been feasible due to from donor funding, including resources leveraged form the VDC itself. One of the lessons learned is the critical role that NGOs can play as catalysts of cross-sectoral responses to complex development issues.26Whereas the VDCs served as the institutional mechanisms for facilitating coordination and collaboration across the PHE domains and sectors, the CFUG provided the
One of the lessons learned is the
critical role that nongovernmental
organizations can play as
catalysts of cross-sectoral
responses to complex development
issues.
mechanism for linking PHE activities at the grass-roots level, and eventually managing the multifaceted approach. Many NGOs prefer to hire their own per-sonnel to implement PHE strategies so as to assure that the deliverables anticipated by the donor are achieved. Under this initiative, the NGO propo-nent opted to transfer know-how to local CFUG institutions, which assumed responsibility for the delivery of family-planning and clean-energy options in conjunction with community forestry manage-ment and governance. Several of the CFUGs appro-priated funds from their community-development reserves to sustain the interventions after the project’s
termination, and their continued effort is generating cobenefits, such as increased community resilience to future climate-change impacts, that otherwise would not have been possible if the NGO had taken respon-sibility for service delivery.
Another factor in the project’s success was RIMS’ approach to human resource development. Most PHE projects support training inputs for community personnel, and the better ones employ competency-based methods and conduct periodic refresher train-ings. The Resource Identification and Management Society additionally provided post-training support to the PHE change agents, which was facilitated by a team of local resource persons specifically developed to mentor and coach the community volunteers in their roles as PHE change agents. The post-training support, which spanned the entire duration of the project, proved critical to the competency and reten-tion of the 375 PHE outreach workers developed under the project. Another lesson learned from this project was the necessity for post-training support in order to increasing return on investment in human resource development.26,27
The project witnessed a significant increase in people’s use of contraceptives and improved cookstoves within a relatively short period of time (30 months). This is likely due to 2 factors: better understanding and appreciation of the multiple ben-efits that accrue from such use (demand side), and
The project witnessed a significant
increase in people’s use of
contraceptives and improved
cookstoves within a relatively short
period of time (30 months).
expanded access to appropriate technology (supply side). Without the latter, it is unlikely that improved knowledge, alone, would have generated the same level of behavior change. For example, most couples in the project area were in favor of family planning and knew that contraceptives could be obtained free of change from government clinics. Transportation barriers (distance and travel cost), however, pre-cluded many from obtaining and using them. The project’s community-based distribution mechanism made it possible for couples to readily obtain sup-plies of oral contraceptive pills and condoms in their wards. In the case of improved cookstoves, access was expanded through local production and subsidy schemes that enabled even the poorest families to adopt the technology.
CONCLUSION
The PHE approach has been shown to be a success-ful approach to addressing health and development issues in areas where environmental conservation is a high priority and population pressure is a critical issue. There is significant variety in the design and implementation of PHE programs, but successful models incorporate community engage-ment and mobilization, appropriate technology, and peer-mediated behavior-change strategies in under-resourced settings. The rationale for this approach acknowledges the close links between the health of a community, including their reproductive health, and the health of the surrounding ecosystem. Moreover, integration facilitates synergies between health and conservation programming that yield added value and cobenefits for humans and the environment.
ACKNOWLEDGMENT
We thank Rishi Bastakoti and others at the Resource Identification and Management Society (RIMS) of Nepal for sharing information, lessons, and best practices from the population, health, environment project in Dhading District. We also thank the US Agency for International Development (USAID) for its support through the Building Actors and Leaders for Excellence in Community Development (BAL-ANCED) Project. The views and opinions of authors expressed here do not necessarily state or reflect those of RIMS, USAID, or theMount Sinai Journal of Medicine.
DISCLOSURES
Potential conflict of interest:Nothing to report.
REFERENCES
1. Corval´an C, Hales S, McMichael A, et al. Ecosystems and Human Well-Being, Health Synthesis: A Report of
the Millennium Ecosystem Assessment.Geneva: World
Health Organization; 2005.
2. McNally J, Poggie J, Rice M. Demographic trajecto-ries, migration and environmental impacts–Palawan Province, the Philippines as a micro-demographic lab-oratory. Presented at: 2004 Meetings of the Population Association of America; April 2004; Boston, MA. 3. Aguirre A, Ostfeld R, Tabor G, et al., eds.Conservation
Medicine: Ecological Health in Practice. New York,
NY: Oxford University Press; 2002.
4. Forget G, Lebel J. An ecosystem approach to human health. Int J Occup Environ Health 2001; 7(2 suppl): S3–S38.
5. One Health Initiative. http://www.onehealthinitiative. com/mission.php. Accessed November 1, 2010. 6. Bioeconomy Africa. http://www.bioeconomyafrica.org/
Pages/BioeconomyAfrica.aspx?Id=22. Accessed Jan-uary 19, 2011.
7. Osofsky S, Koch R, Kock M, et al. Building support for protected areas using a One Health perspective. In: McNeely JA, ed. Friends for Life: New Partners in
Support of Protected Areas.Gland, Switzerland:
Interna-tional Union for Conservation of Nature: Species Sur-vival Commission; 2005. http://www.wcs-ahead.org/ documents/friendsforlife chapter5.pdf. Accessed Jan-uary 12, 2011.
8. Anderson M.History and Future of Population-Health-Environment Programs: Evolution of Funding and
Programming[master’s dissertation]. Minneapolis, MN:
University of Minnesota Humphrey School of Public Affairs; May 13, 2010.
9. Cates W, Quarraisha A, Wafaa E, et al. Family planning and the Millennium Development Goals.Science2010; 329: 1603.
10. D’Agnes L, Margoluis C.Integrating Population, Health and Environment Projects: A Programming Manual.
Washington, DC: US Agency for International Devel-opment; 2007.
11. De Souza RM. The Integration Imperative: How to Improve Development Programs by Linking Population,
Health and Environment.Environmental Change and
Security Program FOCUS Report, Issue 19. Washing-ton, DC: The Woodrow Wilson International Center for Scholars; June 2009.
12. US Agency for International Development. Family planning: population and environment. http://www. usaid.gov/our work/global health//pop/techareas/ environment/index.html. Accessed November 2, 2010. 13. Population Reference Bureau, Population, Health, and Environment Program. Project map. http://www.prb. org/About/InternationalPrograms/Projects-Programs/ PHE.aspx. Accessed November 3, 2010.
14. Oglethorpe J, Honzak C, Margoluis C.Healthy People, Healthy Ecosystems: A Manual for Integrating Health
and Family Planning Into Conservation Projects.
Wash-ington, DC: World Wildlife Fund; 2008.
15. Lundgren RI, Gribble JN, Greene ME, et al. Cultivating men’s interest in family planning in rural El Salvador.
Stud Fam Plann2005; 36: 173–188.
16. D’Agnes L, D’Agnes H, Schwartz JB, et al. Integrated management of coastal resources and human health yields added value: a comparative study in Palawan (Philippines).Environment Conserv2010; 37: 398–409. 17. Castro J, D’Agnes L. Fishing for Families: Reproduc-tive Health and Integrated Coastal Management in the
Philippines. Environmental Change and Security
Pro-gram FOCUS Report, Issue 15. Washington, DC: The Woodrow Wilson International Center for Scholars; April 2008.
18. Singh S, Darroch J, Ashford L, et al. Adding It Up: The Costs and Benefits of Investing in Family
Planning and Maternal and Newborn Health. New
York, NY: UNFPA, United Nations Population Fund, Guttmacher Institute; 2009. http://www.unfpa.org/ public/site/global/pid/4461. Accessed March 4, 2011. 19. US Agency for International Development.New
Esti-mates of Unmet Need and the Demand for Family
Planning. DHS Comparative Reports 14. Calverton,
www.measuredhs.com/pubs/pdf/CR14/CR14.pdf. Accessed January 13, 2011.
20. Finn T. A Guide for Mentoring and Evaluation
Population-Health-Environment Programs. Chapel
Hill, NC: MEASURE Evaluation, US Agency for Inter-national Development; October 2007. http://www.cpc. unc.edu/measure/publications/pdf/ms-07-25.pdf. 21. Kanal KR, Bendel BR. Community forestry in Nepal:
achievements and challenges.J Forest Livelihood2004; 4: 55–63.
22. Kanel K. Nepal’s forest policies on community forestry development: the government perspective. In: Gyamt-sho P, Singh BK, Rasul G.Capitalisation and Sharing of Experiences on the Interaction Between Forest Poli-cies and Land Use Patterns in Asia: Linking People
With Resources. Volume 2: Technical Papers.
Interna-tional Centre for Integrated Mountain Development (ICIMOD); 2006. Accessed January 22, 2011.
23. Schweithelm J, Kanel K, D’Agnes L, et al.; for ARD,
Inc. Nepal Natural Resource User Groups/Population,
Health, and Environment Assessment, Final Report.
Washington, DC: US Agency for International Devel-opment/Nepal Mission; July 2006. http://nepal.usaid.
gov/downloads/all-downloads/category/10-business- opportunities.html?download=163%3Anepal-nrm-and-phe-assessment-final.
24. D’Agnes L, Oglethorpe J, Thapa S, et al. Forest for the Future: Family Planning in Nepal’s Terai Region.
Environmental Change and Security Program FOCUS Report, Issue 18. Washington, DC: The Woodrow Wil-son International Center for Scholars; 2009.
25. Bastakoti RR. Population, Health and Environment (PHE) in Nepal: Successes, challenges and lessons from the RIMS Project. http://www.wilsoncenter.org/ events/docs/Bastakoti.pdf. Published 2009. Accessed January 22, 2011.
26. D’Agnes L. The Population, Health and Environment (PHE) Pathway to Sustainable Livelihoods
Improve-ment: Lessons and Best Practices from Nepal.
Washing-ton, DC: US Agency for International Development/ Nepal Mission; September 2009. http://www.k4health. org/system/files/sites%252Fdefault%252Ffiles%252F Nepal PHE Report October%2B2009.pdf.
27. Bastakoti R. Healthy People, Healthy Ecosystem: PHE