Iranian Rehabilitation Journal, Vol. 11, No. 18, October 2013
Original Article
Effects of Upper Limb Exercises on Physical Capacity and Heart
Function in Quadriplegics
Kanupriya Arora
ISIC Institute of Rehabilitation Sciences, New Delhi
Majumi Mohamad Noohu
1Centre for Physiotherapy and Rehabilitation Sciences, Jamia Millia Islamia, New Delhi
Introduction: Wheelchairs are the prime mobility aid of persons with spinal cord injuries. Manual wheelchair propulsion puts a lot of demand on the cardiopulmonary as well as the skeletal system. The main purpose of the study was to compare the effects of both arm ergometry training and progressive resistance exercise training of upper limbs on resting heart rate and distance covered during wheelchair propulsion in paraplegics.
Method: A convenience sample of 30 male subjects took were randomly assigned to two groups. Participants were spinal cord injured patients recruited from the Indian Spinal Injuries Centre, New Delhi. Each group consisted of 15 subjects. Group 1 received arm ergometry training and group 2 received progressive resistance exercise training. The resting heart rate and distance covered during wheelchair propulsion in a 3 minutes task of the wheelchair circuit was measured before and after 4 weeks of training.
Results: The post intervention resting heart rate and distance covered during wheelchair propulsion after 4 weeks between the two groups showed significant differences. In group 1, resting heart rate was 77.53±3.52 beats/min and in group 2 resting heart rate was 82.33±3.69 beats/min (mean±SD). In group 1, the distance covered during wheelchair propulsion was 305.19±17.21 meters and in group 2 it was 250.71+20.59 meters.
Conclusion: The arm ergometry training may be a better choice of exercise for improving the cardiovascular and functional aspect of spinal cord injury patients who are dependent on wheelchairs for mobility.
Keywords: Paraplegia, wheelchair, endurance, ergometry, functional independence.
Submitted: 15may2013 Accepted: 20september2013
Introduction
Wheelchairs are important in achieving independent mobility as approximately 82% of persons with spinal cord injury (SCI) depend on the wheelchair for their mobility purposes [1]. Manual wheelchair propulsion is a straining form of ambulation, both for the cardiopulmonary as well as the skeletal system. Manual wheelchair propulsion is based on the use of upper extremities which are usually capable of producing less force than the lower limbs with less mechanical efficiency [2].
The normal daily locomotor patterns of wheelchair dependent individuals are insufficient to maintain or improve fitness levels. The lack of adequate fitness levels is a major concern in individuals who have lower body disablement. Therefore an upper limb
Arm ergometry is an electronic arm bicycle used for exercises of the upper limbs. It is similar to the leg bicycle with two pedals which can be propelled by subjects while in a seated position. It is the most reliable and valid exercise mode for clinical and functional evaluation of exercise performance and for optimal prescription of individualized exercise training programs in SCI individuals [4, 6]. Progressive resistance exercises in physical therapy (PRE) provide a practical application of the overload principle and form the basis of most resistance training programs [7].
Dicarlo documented the effects of arm ergometry training on wheelchair propulsion in individuals with quadriplegia[8].S.Nilsson and P.H Staff have shown a significant increase in the maximal oxygen uptake and maximal dynamic strength and endurance in 12 paraplegics who had undergone 7 weeks of intensive training [6]. Studies showing the physiological responses with an arm crank and wheelchair ergometry in SCI are well documented [9,10,11]. Studies have also shown the effects of strength training on wheelchair users [11,12].In this study there are not many studies that have compared the effects of arm ergometry training and strength training on resting heart rate and wheelchair propulsion in paraplegics.
Therefore, the main purpose of this study was to compare the effects of both arm ergometry training and progressive resistance exercise training of upper limbs on resting heart rate and distance covered during wheelchair propulsion in paraplegics.
Methods
A convenience sample of 30 male subjects was randomly assigned to two groups through the lottery method. The study was of pretest post-test experimental design. Participants were spinal cord injured patients recruited from a sub-specialty centre for treating spinal cord injuries in New Delhi. Each group consisted of 15 subjects. Group 1 received arm ergometry training. Group 2 received Progressive resistance exercise training. To avoid selection bias the following conditions were observed: the level of injury was T6-T12, patients were aged between 20-40 years, a minimum spinal cord independence measure score (SCIM) of 80, all participants should have been wheelchair users who could propel the wheelchair for at least 3 minutes, and patients should’ve been undergoing a regular rehabilitation program with no participation in any other endurance training program. The study was
approved by the research and ethics committee of the institute affiliated with the hospital.
The Standard active wheelchair and its dimensions are of: 16 inches length, 16 inches seat width, 16 inches height, standard measuring tape, standardized weighing machine for wheel chair dependent, pulse oximeter, Reck Motomed arm cycle ergometer and free weights of different kilograms were the instruments used. An informed consent was taken from all the subjects and detailed explanation of the procedure was given. The patient’s Demographic data and neurological details were collected. Preliminary measurements were taken prior to the beginning of the study which included body weight and spinal cord independence measure score.
subjects were made to relax and were well positioned according to the muscle group to be tested against gravity. 10 Repetition maximum (10 RM) was calculated for each muscle individually. Subjects were given different weights for particular muscles to be tested. So the maximum weight which was lifted for a complete range of motion for 10 times was considered as the 10 RM. Rest period was provided in-between [7]. Caution was taken to begin the training session on the following day of calculating the 10 RM. The muscles which were tested and trained included anterior and posterior deltoid, infraspinatus, pectoralis major, middle trapezius, biceps, triceps and wrist extensors. All these muscles were trained in their standardized position against gravity. Training sessions included 3 sets of exercises for multiple muscle groups; each set consisting of 10 repetitions with 3 minute rests in-between. The first set required one half of 10 RM, the second set used 3/4th the 10 RM, and the final set
used 10 RM of maximum weight. The training sessions were held 3 times a week. After the end of each week, 10 RM was again calculated and the same training procedure was followed for each muscle with the new 10 RM.
After 4 weeks of training, the resting heart rate (beats per minute) and distance covered during wheelchair propulsion (meters) were recorded. Post-training resting heart rate was measured in the morning after 4 weeks using pulse oximeter for both the groups. The distance covered during 3 minutes of wheelchair propulsion was measured using the wheelchair circuit test on a 200 meter track.
Data Analysis The data was managed on an Excel spread sheet and was analyzed using SPSS software.
A significance level of P≤0.05 was used. T-tests were used to find the differences between the effects of arm ergometry training and progressive resistance exercise training of upper limbs on resting heart rate and distance covered during wheelchair propulsion in paraplegics. Paired t-test was used for analysis within the group.
Results
Group 1 consisted of paraplegic patients with the following particulars; age: 30.6±5.31 years (mean±SD); duration of injury: 329.80±54.82 days; weight: 60.33±4.95 kg; SCIM score: 85.20±1.65. The patients in group 2 had the following particulars; age: 30.46±4.79 years; duration of injury: 329.26±55.94 days; weight: 60.66±4.77 kg; SCIM score: 85.
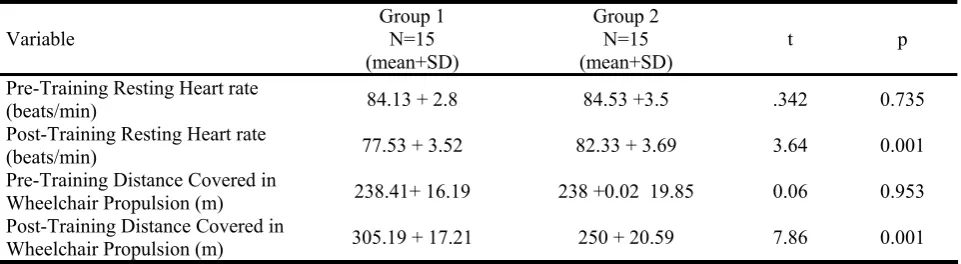
Analysis of data indicates that there were no significant differences in pre-test values of resting heart rate and distance covered during wheelchair propulsion between the two groups. The pre-test value of heart rate in group 1 was 84.13±2.87 beats/min and in group 2 was 84.53±3.50 beats/min. Pre-test values for distance covered during wheelchair propulsion in group 1 and group 2 were 238.41±16.19 and 238.02±19.85 meters. Comparison of post-intervention resting heart rate between the two groups showed significant differences; being 77.53±3.52 beats/min in group 1 and 82.33±3.69 beats/min in group 2. Comparison of post-test distance covered during wheelchair propulsion between the two groups showed a significant difference; being 305.19±17.21 meters in group 1 and 250.71+20.59 meters in group 2 table (1).
Table 1: Comparison of pre-training and post-training resting heart rate and distance covered during wheelchair propulsion between the two groups
Variable Group 1 N=15
(mean+SD)
Group 2 N=15
(mean+SD) t p
Pre-Training Resting Heart rate
(beats/min) 84.13 + 2.8 84.53 +3.5 .342 0.735
Post-Training Resting Heart rate
(beats/min) 77.53 + 3.52 82.33 + 3.69 3.64 0.001
Pre-Training Distance Covered in
Wheelchair Propulsion (m) 238.41+ 16.19 238 +0.02 19.85 0.06 0.953
Post-Training Distance Covered in
Wheelchair Propulsion (m) 305.19 + 17.21 250 + 20.59 7.86 0.001
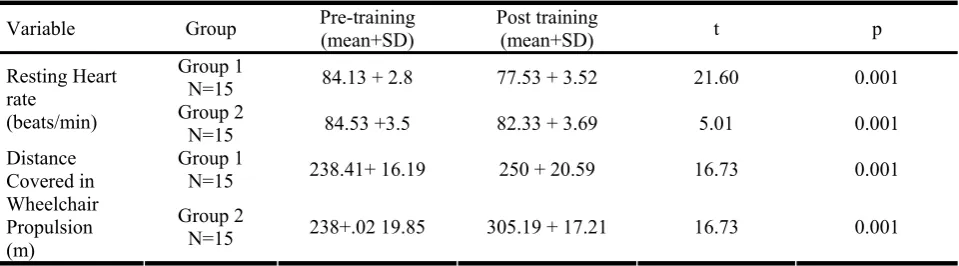
comparison of pre and post intervention scores of resting heart rate and distance covered during wheelchair propulsion within the two groups showed
week. In group 2, the resting heart rate was 84.53±3.50 beats/min at day 0 and 82.33±3.69 beats/min at the end of the 4th week. In group 1, the
distance covered during wheelchair propulsion was 238.41±16.19 meters at day 0, and 305.19±17.21
meters at the end of the 4th week. In group 2 the
same measure was 238.02±19.85 meters at day 0, and 250.71±20.59 meters at the end of the 4th week
table (2).
Table 2: Comparison of pre-training and post-training resting heart rate and distance covered during wheelchair propulsion within the two groups
Variable Group Pre-training (mean+SD) Post training (mean+SD) t p
Group 1
N=15 84.13 + 2.8 77.53 + 3.52 21.60 0.001
Resting Heart rate
(beats/min) Group 2
N=15 84.53 +3.5 82.33 + 3.69 5.01 0.001
Group 1
N=15 238.41+ 16.19 250 + 20.59 16.73 0.001
Distance Covered in Wheelchair Propulsion (m)
Group 2
N=15 238+.02 19.85 305.19 + 17.21 16.73 0.001
Discussion
Significant improvements were seen between the two groups in resting heart rate after 4 distances covered by the subjects in favor of group 1 subject. Possible explanations for the reduction in post-training heart rate values and increased distance covered by subjects can be central as well as peripheral adaptations of the body. Peripheral adaptations result in improvement of oxidative metabolic capacity, oxygen extraction and increased muscle blood flow, whereas central adaptation results in enhanced cardiac output and stroke volume with a compensatory decrease in sympathetic stimulation and alteration in the central nervous system and adaptation in the trained muscle. Central cardiac improvement after exercise results in increased volume loading and reduced heart rate because of a decreased sympathetic drive with decreased levels of epinephrine and nor epinephrine [14].
On comparing mean percentage decrease in resting heart rate after 4 weeks, there were significant differences between the two groups. Group 1 showed greater improvement with mean decreases in resting heart rate of 7.05%, versus group 2, where a mean decrease of 2.6% was observed after 4 weeks. There were also significant differences between the two groups on comparing the distance covered during wheelchair propulsion. Group 1 showed greater improvement with a mean increase of 28.00% in the distance covered, versus group 2, where a mean increase of 5.33% was observed after 4 weeks.
These results are in agreement with a previous study showing improvement in cardiopulmonary functions
in parallel with an increase in wheelchair propulsion endurance in quadriplegics [8]. This study also reported that subjects exercising on an arm ergometer were able to work more efficiently. The changes in cardiovascular functional status might have contributed to the differences seen in group 1. Another factor might be the exercise specificity which helped improve the function. The arm ergometry training simulates more of a functional activity as compared to strength training that only consists of lifting and lowering of free weights. Moreover, wheel chair propulsion is an activity which demands cardiovascular endurance rather than muscle strength alone.
The results obtained from this study suggest that arm ergometry training may be used to improve functional independence in spinal cord injured subjects who are using wheelchairs. Future studies can be carried out to assess torque or force production ability during wheelchair propulsion. Furthermore, subjects should be tested for other wheelchair skills with arm ergometry training.
Conclusions
References
1. Kilkens OJ, Post MW, van der Woude LH, Dallmeijer AJ, van den Heuvel WJ. The wheelchair circuit: reliability of a test to assess mobility in persons with spinal cord injuries. Arch Phys Med Rehabil. 2002;83(12):1783–8.
2. Spaepen AJ, Vanlandewijck YC, Lysens RJ. Relationship between energy expenditure and muscular activity patterns in handrim wheelchair propulsion. Int J Ind Ergon. 1996;17(2):163–73.
3. Sedlock DA, Knowlton RG, Fitzgerald PI. The effects of arm crank training on the physiological responses to submaximal wheelchair ergometry. Eur J Appl Physiol. 1988;57(1):55–9.
4. Glaser RM, Sawka MN, Durbin RJ, Foley DM, Suryaprasad AG. Exercise program for wheelchair activity. Am J Phys Med. 1981;60(2):67–75.
5. Pollock ML, Gaesser GA, Butcher JD, Despres J-P, Dishman RK, Franklin BA, et al. ACSM position stand: the recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc. 1998;30(6):975–91.
6. Nilsson S, Staff PH, Pruett ED. Physical work capacity and the effect of training on subjects with long-standing paraplegia. Scand J Rehabil Med. 1975;7(2):51–6.
7. McArdle WD, Katch FI, Katch VL. Exercise physiology:
nutrition, energy, and human performance. 6th ed. Lippincott Williams & Wilkins; 2006, pp:511–5.
8. DiCarlo SE. Effect of arm ergometry training on wheelchair propulsion endurance of individuals with quadriplegia. Phys Ther. 1988;68(1):40–4.
9. Glaser RM, Sawka MN, Brune MF, Wilde SW. Physiological responses to maximal effort wheelchair and arm crank ergometry. J Appl Physiol. 1980;48(6):1060–4. 10.Drory Y, Ohry A, Brooks ME, Dolphin D, Kellermann JJ.
Arm crank ergometry in chronic spinal cord injured patients. Arch Phys Med Rehabil. 1990;71(6):389–92.
11.Gass EM, Harvey LA, Gass GC. Maximal physiological responses during arm cranking and treadmill wheelchair propulsion in T4-T6 paraplegic men. Paraplegia. 1995;33(5):267–70.
12.Ambrosio F, Boninger ML, Souza AL, Fitzgerald SG, Koontz AM, Cooper RA. Biomechanics and strength of manual wheelchair users. J Spinal Cord Med. 2005;28(5):407–14.
13.Kisner C, Colby LA. Therapeutic exercise [Internet]. 3rd ed. FA Davis; 1996 [cited 2014 Feb 2]. Available from: http://sites.google.com/site/bndr4spta/1_2338_1197.pdf 14.Muller G, Odermatt P, Perret C. A new test to improve the