Based Microarray Analysis after Hematopoietic Stem Cell
Transplantation
France Debaugnies,aLaurent Busson,bAlina Ferster,cPhilippe Lewalle,dNadira Azzi,cMickael Aoun,eGodelieve Verhaegen,a Bhavna Mahadeb,bJérôme de Marchin,aOlivier Vandenberg,bMarie Hallina
Center for Molecular Diagnostic, iris-Lab, Iris-Brussels Public Hospital Network, Brussels, Belgiuma; Department of Microbiology, iris-Lab, Iris-Brussels Public Hospital Network, Brussels, Belgiumb; Department of Haematology and Oncology, Hôpital Universitaire Des Enfants Reine Fabiola, Brussels, Belgiumc; Department of Haematology, Jules Bordet Institute, Brussels, Belgiumd; Division of Infectious Diseases, Jules Bordet Institute, Brussels, Belgiume
Viral infections are important causes of morbidity and mortality in patients after hematopoietic stem cell transplantation. The monitoring by PCR ofHerpesviridaeloads in blood samples has become a critical part of posttransplant follow-up, representing mounting costs for the laboratory. In this study, we assessed the clinical performance of the multiplex PCR DNA microarray Clart Entherpex kit for detection of cytomegalovirus (CMV), Epstein-Barr virus (EBV), and human herpesvirus 6 (HHV-6) as a screening test for virological follow-up. Two hundred fifty-five blood samples from 16 transplanted patients, prospectively tested by routine PCR assays, were analyzed by microarray. Routine PCR detected single or multiple viruses in 42% and 10% of the samples, respectively. Microarray detected single or multiple viruses in 34% and 18% of the samples, respectively. Microarray results correlated well with CMV and EBV detections by routine PCR (kappa testsⴝ0.79 and 0.78, respectively), whereas a weak correlation was observed with HHV-6 (0.43). HHV-7 was also detected in 48 samples by microarray. In conclusion, the microar-ray is a reliable screening assay for a posttransplant virological follow-up to detect CMV and EBV infections in blood. However, positive samples must be subsequently confirmed and viral loads must be quantified by PCR assays. Limitations were identified regarding HHV-6 detection. Although it is promising, is easy to use as a first-line test, and allows a reduction in the cost of analy-sis without undue delay in the reporting of the final quantitative result to the clinician, some characteristics of this microarray should be improved, particularly regarding quality control and the targeted virus panel, such that it could then be used as a rou-tine test.
E
ither directly by causing end-organ damage or indirectly by facilitating bacterial or fungal infections, viral agents contrib-ute to increased morbidity and mortality in hematopoietic stem cell transplantation (HSCT) (1–3). It is during the postengraft-ment period from day 30 until day 100, marked by cell-mediated and humoral immune deficiencies, that HSCT recipients are prone to devastating diseases generated by chronic or latent vi-ruses of theHerpesviridaegroup. A close virological monitoring is therefore recommended as a preemptive strategy for early detec-tion and treatment of patients experiencing viral primary infec-tion and reactivainfec-tion, as they are at risk of developing overt dis-ease, especially from cytomegalovirus (CMV) and Epstein-Barr virus (EBV) (4–6). This strategy is based on quantitative determi-nation of viral load in blood once per week. In our institution, the cutoffs usually accepted for initiation of preemptive treatment are 10,000 copies for CMV and 1,000 copies for EBV in accordance with previously published data (7–9). As far as human herpesvirus 6 (HHV-6) infections are concerned, reactivations are associated with delayed platelet engraftment and early posttransplantation mortality. Furthermore, monitoring of HHV-6 viral load in blood could allow a differential diagnosis of graft-versus-host disease (GvHD)-like symptoms (10). Data to guide preemptive monitor-ing to prevent potential HHV-6-associated disease are lackmonitor-ing, and further studies are needed to reach more robust conclusions. Real-time quantitative PCR techniques have gradually re-placed conventional methods of virus detection for the monitor-ing of transplanted patients. These molecular techniques allow an early detection and a reliable quantification of the virus and aremore automatable and standardized. However, given the number of tests recommended in the guidelines, they represent mounting costs for the laboratories. New molecular techniques such as mul-tiplex PCR amplification followed by microarray analysis are now being developed. They allow the simultaneous detection and iden-tification of several viruses in one run. Microarrays offer an inter-esting alternative diagnostic tool, their potential benefits being the decrease in turnaround time and costs of analysis. Moreover, a larger panel of viruses can be tested simultaneously. Microarray techniques have already been evaluated in routine settings for the diagnosis of central nervous system and respiratory tract viral in-fections (11–16). To the best of our knowledge, microarrays have not yet been evaluated prospectively for the detection of Herpes-viridaein a cohort of patients undergoing HSCT.
In this study, we assessed the application of a commercial mul-tiplex PCR DNA microarray, the Clart Entherpex kit, on a routine basis in the virological surveillance of transplanted patients. This kit allows the simultaneous qualitative detection and
identifica-Received10 January 2014 Returned for modification5 February 2014
Accepted30 April 2014
Published ahead of print14 May 2014
Editor:Y.-W. Tang
Address correspondence to France Debaugnies, [email protected].
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.00061-14
on May 16, 2020 by guest
http://jcm.asm.org/
tion of theHerpesviridaeCMV, EBV, HHV-6, herpes simplex vi-rus 1 (HSV-1), HSV-2, varicella-zoster vivi-rus (VZV), HHV-7 and HHV-8. The aim of the study was to evaluate its analytical perfor-mances for the simultaneous qualitative detection of CMV, EBV, and HHV-6 in a cohort of patients undergoing HSCT compared to the PCR assays routinely used in our laboratory.
MATERIALS AND METHODS
Patients and samples.From November 2011 to May 2012, all new pa-tients undergoing HSCT from the Jules Bordet Institute (adults) and the Queen Fabiola Children’s University Hospital (pediatrics), Brussels, Bel-gium, were prospectively enrolled in the study. At least one EDTA-anti-coagulated whole-blood sample was collected per week for each patient, and these samples were tested with both real-time quantitative PCRs rou-tinely used in the laboratory and the new multiplex PCR DNA microarray. Clinical data were prospectively collected during the evaluation in the daily report of hospitalization and during weekly clinical meetings. Lab-oratory data, including neutrophil and platelet counts, C-reactive protein levels, and positive microbiological results, were also collected. The study was approved by the institutional Ethical Committees of the two hospitals.
DNA extraction.Total nucleic acid extraction was performed using the MagNA Pure LC instrument (Roche Diagnostics, Mannheim, Ger-many) with the total nucleic acid high-performance isolation kit (Roche Diagnostics, Mannheim, Germany) according to the manufacturer’s in-structions. Total nucleic acid was extracted from 200l of EDTA-whole blood and recovered in 100l of elution buffer. Aliquots were stored at
⫺80°C before use.
Routine CMV, EBV, and HHV-6 viral load assessment by quantita-tive real-time PCR.CMV and EBV DNA viral loads were determined using the Dia-CMVQ-050 and Dia-EBVQ-050 kits (Diagenode Diagnos-tics, Liège, Belgium). HHV-6 DNA viral load was determined using an in-house real-time quantitative PCR, as described previously by Locatelli et al. (17). PCRs were performed on the ABI 7500 Fast PCR instrument (Applied Biosystems, Ghent, Belgium). All samples were tested in dupli-cate. Results were given in copy number/milliliter of whole blood. The lower limit of quantification is 800 copies/ml for CMV and EBV and 1,500 copies/ml for HHV-6. The lower limit of detection observed in our labo-ratory is 500 copies/ml of whole blood for CMV and EBV and 800 cop-ies/ml for HHV-6.
Simultaneous qualitative detection of CMV, EBV, and HHV-6 by multiplex PCR DNA microarray.The Clart Entherpex assay (Genomica, Coslada, Spain) was performed according to the manufacturer’s instruc-tions. Briefly, in a first step, 5l of total nucleic acid extract of each sample is amplified in two tubes containing different reaction mixtures. An inter-nal control is added in each amplification tube to control amplification efficiency. The second step consists of hybridization of the biotinylated PCR products with target-specific binding probes. A microarray reader piloted by specific software performs the detection by colorimetric reac-tion and the interpretareac-tion of the results. The lower limit of reproducible detection, as determined by Lévêque et al. (11), is 250 copies/ml for CMV, 2,000 copies/ml for EBV, and 500 copies/ml for HHV-6.
Statistical analyses.To evaluate the analytical performances of the microarray in the detection of CMV, EBV, and HHV-6 in blood samples, the sensitivity, specificity, and negative and positive predictive values were calculated considering the routine PCR assays as the reference method. The kappa statistics were calculated to evaluate the agreement between microarray and routine PCR assays. For each virus, the viral load levels measured by PCR in samples positive by microarray were compared using a Mann-Whitney U test to the viral load levels measured by PCR in sam-ples negative by microarray. APvalue of less than 0.05 was considered significant. Data were analyzed using GraphPad Prism 5 (GraphPad Soft-ware, Inc., USA).
Definitions.“Herpesvirus infection” was defined as detection of nu-cleic acid of herpesvirus in blood sample. An “active viral replication” is confirmed by an increased viral load on the following sample(s) resulting
from a primary infection, a reinfection, or a reactivation of a latent virus. We used the term “intermittent viremia” in cases of detection of virus nucleic acid in the blood by PCR and/or microarray sporadically, at a low viral load, without an increased viral load on the next sample, which corresponded to a latent stage of infection. Patients with chromosomally integrated HHV-6 (ciHHV-6) were defined as persistent HHV-6 viral load over time greater than 5.5 log10copies/ml of whole blood (18).
Discrepant results between microarrays and routine PCR assays were interpreted as follows: positive PCR results, negative by microarray, were deemed “false negative”; negative PCR results, positive by microarray, were deemed “likely true positive” if either the previous or the next sample obtained from the same patient was positive by PCR, “possibly true pos-itive” if the result was consistent with the serological status of the patient, and “false positive” in the other cases.
RESULTS
Two hundred fifty-five blood samples were analyzed for the viro-logical follow-up of 16 patients (8 males and 8 females) who had undergone allogeneic (n⫽15) and autologous (n⫽1) HSCT. For each patient, one sample was collected before transplantation and the other samples were collected posttransplantation. Nine pa-tients were children (aged 16 years or less), and seven papa-tients were adults. One patient died before transplantation. The moni-toring period varied from 12 days for the last patient enrolled to 169 days for the first one enrolled.
Among the 255 samples, 5 were completely excluded (4 sam-ples with inhibited PCR for the 3 viruses and 1 sample with invalid microarray result).
Diagnosis and management of viral infections by quantita-tive real-time PCR.Among the 250 remaining samples, 48% (n⫽
120) were completely negative and 52% (n⫽130) were positive. Out of these positive samples, 82% (n⫽106) were positive for a single virus and 18% (n⫽24) were positive for several viruses.
CMV was detected in 27% of the samples (66 out of 249; one more PCR was excluded from the analysis as it was inhibited even after sample dilution). EBV was detected in 19% of the samples (47 out of 244; 6 PCRs were excluded as 5 were inhibited and one sample was lacking). HHV-6 was detected in 14% (35 out of 246; 4 PCRs were excluded as they were inhibited).
Fourteen episodes of active viral replication were observed (CMV,n⫽6; EBV,n⫽5; HHV-6,n⫽3) in 9 patients: CMV for 3 of the patients, CMV and EBV for 3 other patients, EBV and HHV-6 for 2 of the patients, and HHV-6 for 1 of the patients. These episodes resulted in an adaptation of the antiviral therapy for 8 of the 9 patients. Given that the viral load was low and symp-toms were absent in the last patient, his antiviral therapy was not modified.
Performances of the microarray, the Clart Entherpex assay. Forty-eight percent of samples were completely negative (n ⫽
120), and 52% (n ⫽130) were positive. Out of these positive samples, 65% (n⫽84) were positive for a single virus and 35% (n⫽46) were positive for several viruses. CMV was detected in 26% of the samples (64 out of 250). EBV was detected in 20% of the samples (50 out of 250). HHV-6 was detected in 17% (42 out of 250).
Additionally, HHV-7 was detected in 48 samples from 9 pa-tients. One sample was also positive for HSV-1 and confirmed by routine PCR assay; the other targeted viruses included in the range of the array were not found in any of the analyzed samples.
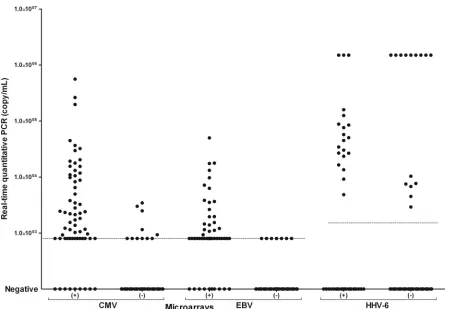
The comparison of qualitative PCR DNA microarray and quantitative real-time PCR results is shown inFig. 1. The
on May 16, 2020 by guest
http://jcm.asm.org/
ity and specificity of the microarray were 83 and 95%, 85 and 95%, and 57 and 90% for CMV, EBV, and HHV-6, respectively. The kappa coefficients between the microarray and routine PCR assays were equal to 0.8 for CMV and EBV and 0.4 for HHV-6. Thirty-three false-negative results were observed in a total of 29 samples (Table 1). Regarding CMV (n⫽11) and EBV (n⫽7), all but one false-negative case were observed for viral loads below or around
[image:3.585.69.524.62.371.2]the limit of quantification of the PCR. Only one sample had a viral load (CMV) above 1,000 copies/ml of whole blood with 2 positive replicates by PCR. CMV and EBV PCR-positive samples that were not detected by microarray had median viral loads significantly lower than those positive by PCR and microarray (852 copies/ml [500 to 3,439] versus 2,329 copies/ml [500 to 560,338],P⬍0.05 for CMV; 500 copies/ml [500 to 575] versus 1,001 copies/ml [500 FIG 1Comparison of qualitative PCR DNA microarray and quantitative real-time PCR results (CMV,n⫽249; EBV,n⫽244; HHV-6,n⫽246). The viral loads (number of copies/ml of whole blood) are plotted on theyaxis. Thexaxis indicates the positive (⫹) and negative (⫺) microarray results. The dashed lines represent the lower limits of quantification of PCR assays.
TABLE 1Summary of the blood sample results obtained with the microarray assay compared to our routine PCR assaysa
Category by routine PCR
Result by microarray
No. of samples
Kappa test (95% CI) Sensitivity (%) Specificity (%) PPV (%) NPV (%)
No. of evaluable samplesb
Virus positive
Virus negative
CMV 0.79 (0.71–0.88) 83 95 86 94 249
Positive 55 11
Negative 9 174
EBV 0.78 (0.68–0.88) 85 95 80 96 244
Positive 40 7
Negative 10 187
HHV-6 0.43 (0.28–0.58) 57 90 48 93 246
Positive 20 15
Negative 22 189
a
Abbreviations: CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value.
bSamples with inhibited PCR or an invalid microarray or that were unavailable were excluded.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.44.545.540.707.2]to 49,972],P⬍0.01 for EBV). Fifteen false-negative results were observed for HHV-6. Surprisingly, nine out of these 15 samples had, by PCR, extremely high levels of HHV-6 (above 6 log10 cop-ies/ml of whole blood). HHV-6 PCR-positive samples that were not detected by microarray had median viral loads that were not statistically different from those of samples positive by both PCR and microarray (1.5⫻106copies/ml [2,920 to 1.5⫻106] versus 47,666 [4,839 to 1.5⫻106]).
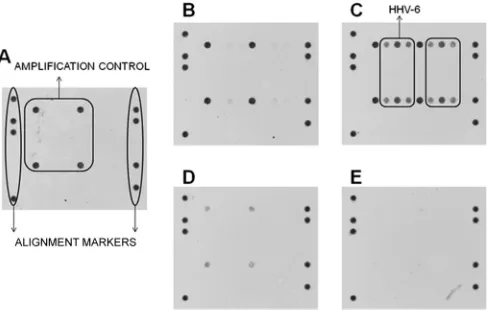
To investigate the cause of these false-HHV-6-negative results, we tested if a hybridization could be observed when diluting one of these false-negative samples before or after performing the am-plification step (dilution of the DNA extract versus dilution of the PCR product). Since the signal was recovered only when the sam-ple was diluted before amplification (Fig. 2), we inferred that the amplification step was affected by a large amount of target. This “false-negative” phenomenon was observed in 9 out of the 12 HHV-6 viral loads above 6 log10copies/ml collected during the study but was not observed with samples having similarly high CMV or EBV viral loads.
Forty-one microarray-positive results were not confirmed by PCR (Table 1). Fifteen of them, corresponding to an early detec-tion of reactivadetec-tion or collected after the initiadetec-tion of antiviral therapy, were classified as likely true positive (6 CMV and 9 HHV-6). Thirteen results were possibly true positive (3 CMV and 10 EBV), consistent with the serological status of the patient. Thir-teen results, all HHV-6 positive, were classified as false positive, serology not being available for these cases.
DISCUSSION
Technology improvements in molecular diagnostic tests (possi-bility of automation, real-time PCR amplification, and availa(possi-bility of commercial kits) have promoted their implementation in the routine diagnostic virology laboratory. These more sensitive and specific as well as time- and labor-saving tests have mostly re-placed conventional methods of virus detection (culture and se-rology), especially in the virological surveillance of transplanted patients for whom the timeliness of the results is a critical compo-nent. The main obstacle to the use of these techniques is their cost. In this context, the use of the multiplex PCR DNA microarray
Clart Entherpex kit for simultaneous qualitative detection of CMV, EBV, and HHV-6 in one run of testing could allow poten-tial turnaround time reduction and cost savings. The aim of the study was to assess the performance of this microarray method in a routine clinical laboratory setting.
In our cohort of patients, the microarray assay showed good performances for CMV and EBV detection compared to routine quantitative PCR. All clinically relevant episodes were associated with a positive microarray result. The few discrepant results were observed in cases presenting with low viral load (such as latent stage of infection, intermittent viremia, or early onset of an active replication) and thus had no major clinical consequences, i.e., no change in the antiviral therapy. The agreement was good for CMV and EBV but weaker for HHV-6 detection. Actually, 9 samples tested negative with the microarray had a very high viral load (⬎6 log10copies/ml) by PCR. These results were observed for one pa-tient with ciHHV-6 as well as for one papa-tient with active reactiva-tion. We believe that a very high HHV-6 viral load interferes with the amplification step of the microarray. This analytical glitch was even more problematic because, in these cases, the internal ampli-fication controls were not inhibited as they should have been. We also suspect that coinfections, especially when quantities of the different viruses differ greatly, could affect the analytical sensitiv-ity of the microarray and give false-negative results (data not shown).
The multiplex PCR, the hybridization of PCR products, and the reading and interpretation of the microarray were achieved within 8 h. As the same extraction step was used for the microarray analysis and quantitative PCR analysis, the microarray could in theory easily be used as a weekly screening assay for the detection ofHerpesviridaein the blood of transplanted patients. Each posi-tive result can subsequently be followed by selecposi-tive viral load measurement by a quantitative PCR. One of the main advantages of proceeding as such would be a reduction in the cost of analysis of around 22% (estimated on a retrospective series of 3,832 sam-ples collected over 5 years for CMV, EBV, and HHV-6 detection [data not shown]). Another advantage of implementing this test would be that the wide range of viruses tested could help assess the pathogenicity of neglected viruses such as HHV-7, which was the most commonly identified virus in our cohort after CMV, EBV, and HHV-6. Moreover, the delay of response incurred by the im-plementation of one supplementary first-line test would not have a critical impact, seeing that samples would be analyzed only once or twice weekly in batches.
However, the drawbacks of this algorithm would be that it would require a controlled workflow and that adding a screening test could increase the workload even if it reduces the total num-ber of samples on which PCRs would be performed. However, as this test has analytical limitations that for the moment prevent its implementation in a routine setting, the gain over workload re-mains difficult to ascertain. To ensure the place of this microarray in routine laboratories, improvements should be made by the manufacturers regarding internal quality controls. Moreover, to make the most of its potential benefits for the follow-up of HSCT patients, the additional detection of adenovirus, parvovirus B19, and JC and BK polyomaviruses would be an interesting develop-ment which could alleviate the further workload generated.
Conclusion.The evaluated multiplex PCR DNA microarray is a reliable screening assay for a posttransplant virological fol-low-up to detect CMV and EBV reactivations in the blood. How-FIG 2Microarray results for a sample with an HHV-6 viral load above 6 log10
copies/ml of blood. (A) Undiluted sample. (B and C) Sample diluted 1:100 (B) and 1:1,000 (C) before the first multiplex PCR step of the microarray. (D and E) Sample diluted 1:100 (D) and 1:1,000 (E) before the hybridization step of the microarray.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.42.287.67.222.2]ever, positive samples must be subsequently confirmed and the viral load must be quantified by PCR assays to obtain a more precise diagnosis. Several samples with high viral loads of HHV-6 testing negative with the microarray can be problematic both for the pretransplantation detection of chromosomally integrated HHV-6 and for follow-up of patients with active reactivation.
Although it is promising, some characteristics of this diagnos-tic tool should be improved, pardiagnos-ticularly for quality control and a targeted virus panel, such that it could then be adapted to be used in a routine setting.
ACKNOWLEDGMENTS
This work was supported by a grant from the Iris-Recherche fund. We thank Marie-Jeanne Stouten for her skilled technical assistance.
REFERENCES
1.Gratwohl A, Brand R, Frassoni F, Rocha V, Niederwieser D, Reusser P, Einsele H, Cordonnier C.2005. Cause of death after allogeneic haema-topoietic stem cell transplantation (HSCT) in early leukaemias: an EBMT analysis of lethal infectious complications and changes over calendar time. Bone Marrow Transplant.36:757–769.http://dx.doi.org/10.1038/sj.bmt .1705140.
2.Bjorklund A, Aschan J, Labopin M, Remberger M, Ringden O, Win-iarski J, Ljungman P.2007. Risk factors for fatal infectious complications developing late after allogeneic stem cell transplantation. Bone Marrow Transplant.40:1055–1062.http://dx.doi.org/10.1038/sj.bmt.1705856. 3.Rieger CT, Rieger H, Kolb HJ, Peterson L, Huppmann S, Fiegl M,
Ostermann H.2009. Infectious complications after allogeneic stem cell transplantation: incidence in matched-related and matched-unrelated transplant settings. Transpl. Infect. Dis.11:220 –226.http://dx.doi.org/10 .1111/j.1399-3062.2009.00379.x.
4.Tomblyn M, Chiller T, Einsele H, Gress R, Sepkowitz K, Storek J, Wingard JR, Young JA, Boeckh MJ.2009. Guidelines for preventing infectious complications among hematopoietic cell transplant recipients: a global perspective. Biol. Blood Marrow Transplant.15:1143–1238.http: //dx.doi.org/10.1016/j.bbmt.2009.06.019.
5.Emery VC, Sabin CA, Cope AV, Gor D, Hassan-Walker AF, Griffiths PD.2000. Application of viral-load kinetics to identify patients who de-velop cytomegalovirus disease after transplantation. Lancet355:2032– 2036.http://dx.doi.org/10.1016/S0140-6736(00)02350-3.
6.van Esser JW, van der Holt B, Meijer E, Niesters HG, Trenschel R, Thijsen SF, van Loon AM, Frassoni F, Bacigalupo A, Schaefer UW, Osterhaus AD, Gratama JW, Löwenberg B, Verdonck LF, Cornelissen JJ.2001. Epstein-Barr virus reactivation is a frequent event after allogeneic stem cell transplantation and quantitatively predicts EBV-lymphoproliferative disease following T-cell-depleted SCT. Blood98:
972–978.http://dx.doi.org/10.1182/blood.V98.4.972.
7.Gerna G, Lilleri D, Caldera D, Furione M, Zenone Bragotti L, Alessan-drino EP.2008. Validation of a DNAemia cutoff for preemptive therapy of cytomegalovirus infection in adult hematopoietic stem cell transplant recipients. Bone Marrow Transplant.41:873– 879.http://dx.doi.org/10 .1038/sj.bmt.1705986.
8.Lilleri D, Gerna G, Furione M, Bernardo ME, Giorgiani G, Telli S, Baldanti F, Locatelli F.2007. Use of a DNAemia cut-off for monitoring
human cytomegalovirus infection reduces the number of preemptively treated children and young adults receiving hematopoietic stem-cell transplantation compared with qualitative pp65 antigenemia. Blood110:
2757–2760.http://dx.doi.org/10.1182/blood-2007-03-080820.
9.van Esser JW, Niesters HG, van der Holt B, Meijer E, Osterhaus AD, Gratama JW, Verdonck LF, Löwenberg B, Cornelissen JJ.2002. Preven-tion of Epstein-Barr virus-lymphoproliferative disease by molecular mon-itoring and preemptive rituximab in high-risk patients after allogeneic stem cell transplantation. Blood99:4364 – 4369.http://dx.doi.org/10.1182 /blood.V99.12.4364.
10. Dulery R, Salleron J, Dewilde A, Rossignol J, Boyle EM, Gay J, de Berranger E, Coiteux V, Jouet JP, Duhamel A, Yakoub-Agha I.2012. Early human herpesvirus type 6 reactivation after allogeneic stem cell transplantation: a large-scale clinical study. Biol. Blood Marrow Trans-plant.18:1080 –1089.http://dx.doi.org/10.1016/j.bbmt.2011.12.579. 11. Lévêque N, Van Haecke A, Renois F, Boutolleau D, Talmud D,
An-dreoletti L.2011. Rapid virological diagnosis of central nervous system infections by use of a multiplex reverse transcription-PCR DNA microar-ray. J. Clin. Microbiol. 49:3874 –3879. http://dx.doi.org/10.1128/JCM .01214-11.
12. Mannonen L, Vainionpää R, Kauppinen J, Lienhard R, Tritten ML, Cannon G, Hall WW, Moilanen K, Häkkinen M, Jääskeläinen AJ, Piiparinen H, Mäki M, Järvinen AK, Lappalainen M.2012. Evaluation of multiplex polymerase chain reaction and microarray-based assay for rapid herpesvirus diagnostics. Diagn. Microbiol. Infect. Dis.73:74 –79.http://dx .doi.org/10.1016/j.diagmicrobio.2012.02.015.
13. Renois F, Talmud D, Huguenin A, Moutte L, Strady C, Cousson J, Lévêque N, Andréoletti L.2010. Rapid detection of respiratory tract viral infections and coinfections in patients with influenza-like illnesses by use of reverse transcription-PCR DNA microarray systems. J. Clin. Microbiol.
48:3836 –3842.http://dx.doi.org/10.1128/JCM.00733-10.
14. Frobert E, Escuret V, Javouhey E, Casalegno JS, Bouscambert-Duchamp M, Moulinier C, Gillet Y, Lina B, Floret D, Morfin F.2011. Respiratory viruses in children admitted to hospital intensive care units: evaluating the CLART Pneumovir DNA array. J. Med. Virol.83:150 –155.
http://dx.doi.org/10.1002/jmv.21932.
15. Huguenin A, Moutte L, Renois F, Lévêque N, Talmud D, Abely M, Nguyen Y, Carrat F, Andreoletti L.2012. Broad respiratory virus detec-tion in infants hospitalized for bronchiolitis by use of a multiplex RT-PCR DNA microarray system. J. Med. Virol.84:979 –985.http://dx.doi.org/10 .1002/jmv.23272.
16. Bierbaum S, Königsfeld N, Besazza N, Blessing K, Rücker G, Kontny U, Berner R, Schumacher M, Forster J, Falcone V, van de Sand C, Essig A, Huzly D, Rohde G, Neumann-Haefelin D, Panning M.2012. Perfor-mance of a novel microarray multiplex PCR for the detection of 23 respi-ratory pathogens (SYMP-ARI study). Eur. J. Clin. Microbiol. Infect. Dis.
31:2851–2861.http://dx.doi.org/10.1007/s10096-012-1639-1.
17. Locatelli G, Santoro F, Veglia F, Gobbi A, Lusso P, Maltani MS.2000. Real-time quantitative PCR for human herpesvirus 6 DNA. J. Clin. Mi-crobiol.38:4042– 4048.
18. Pellett PE, Ablashi DV, Ambros PF, Agut H, Caserta MT, Descamps V, Flamand L, Gautheret-Dejean A, Hall CB, Kamble RT, Kuehl U, Lass-ner D, Lautenschlager I, Loomis KS, Luppi M, Lusso P, Medveczky PG, Montoya JG, Mori Y, Ogata M, Pritchett JC, Rogez S, Seto E, Ward KN, Yoshikawa T, Razonable RR.2012. Chromosomally integrated human herpesvirus 6: questions and answers. Rev. Med. Virol.22:144 –155.http: //dx.doi.org/10.1002/rmv.715.