Abstract
The existing literature disagrees in terms of treatment options and alternatives for
individuals dealing with Alcohol Use Disorder (AUD), but agree on the need to solve this
public health concern. This paper seeks to first understand the disease and the drugs
available for its treatment and secondly reviews the guidelines and regulations that
either restrict or encourage the market authorization (MA) of a drug. Those will be the
foundations for suggesting the implementation of a temporary recommendation for use
of the Baclofen in the treatment of AUD. A review of positive and negative outcomes
from peer-reviewed Randomized Controlled Trials (RCT) is provided to demonstrate
Baclofen’s success in the treatment of AUD and support the implementation of a
temporary recommendation for use (TRU) in the United States.
Keywords:
Alcohol Use DisorderGamma Aminobutyric Acid (GABA)
Baclofen
Acknowledgements:
UNC Gillings School of Global Public Health;
The Public Health Leadership Program at the Gillings School of Global Public
Health;
Professor Lori Evarts from the Gillings School of Global Public Health for her
continuous support;
Dr Krupitsky for initiating this incredible journey;
Dr Ameisen for lobbying for the Baclofen in the treatment of AUD;
Dr. Garbutt for his contribution in treatment options for recovering addicts;
Dr. Thorp for his contribution in this present report as a second reader and a
leader in recovery treatment facilities;
My wife for her multiple contributions to this project.
I want to dedicate this paper to Dr Olivier Ameisen who passed in 2013 after leading
the case of Baclofen in the treatment of AUD and to all those individuals who fight
Table of Contents
Introduction 1
Methodology 1
Biological Description of AUD 2
Existing AUD treatment options in the United States 7
FDA Guidance 7
FDA Approved Medications in the Treatment of AUD 8
Drugs Currently Under Investigation in the Treatment of AUD 14
Negative outcomes observed in RCTs 20
American Trials 20
French Trial 20
Israeli Trial 21
Hypotheses for negative observations in RCT 21
Prominent Ongoing Trials 24
French RCT 24
American RCTs 24
Regulations and Processes for Drug Approval 26
FDA Regulations in the United States 26
EMA and the ANSM Regulations in France 29
Discussion 31
Implementing a TRU in the United States 31
Positive outcomes observed in RCTs and case reports 32
Comparison of Costs of Drugs in the United States 37
Creating a coalition 38
Appendices
Page
1. DSM-5 criteria to be diagnosed with AUD 48
2. Long-term implications of AUD 49
3. List of FDA approved manufacturers for the distribution of generic Baclofen in the United States
50
4. Summary of trials with positive outcomes 51
5. Summary of trials with negative outcomes 55
List of Figures
Figure 1: Flow of ethanol in the body Page 3
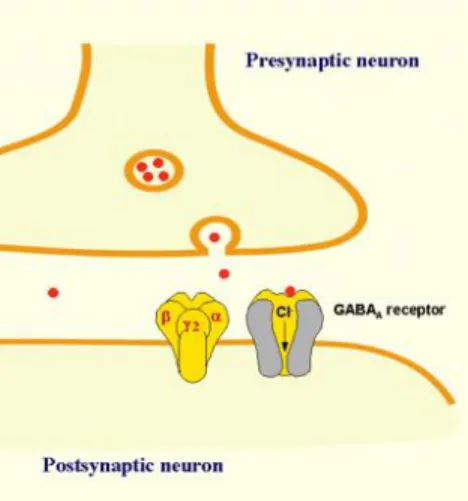
Figure 2: GABA’s role in the synaptic cleft Page 4
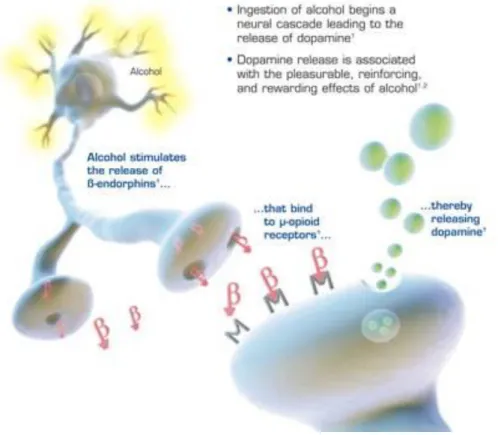
Figure 3: How alcohol releases dopamine Page 5
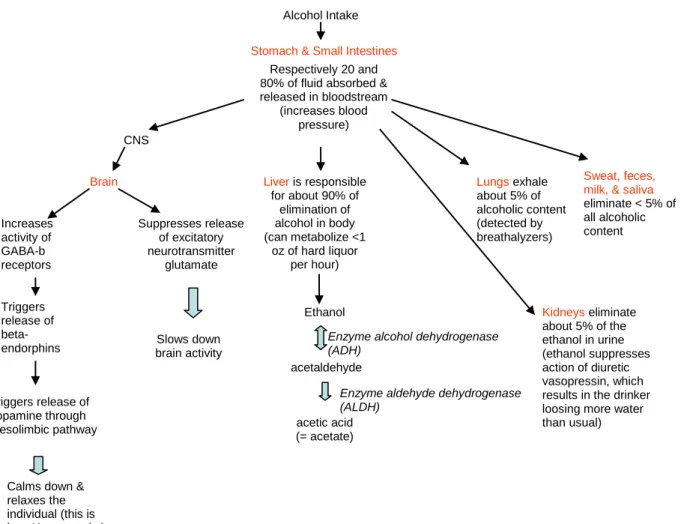
Figure 4: Summary of biology related to alcohol intake Page 6
Figure 5: Drugs approved by the US FDA to treat AUD Page 8
Figure 6: How Disulfiram works Page 10
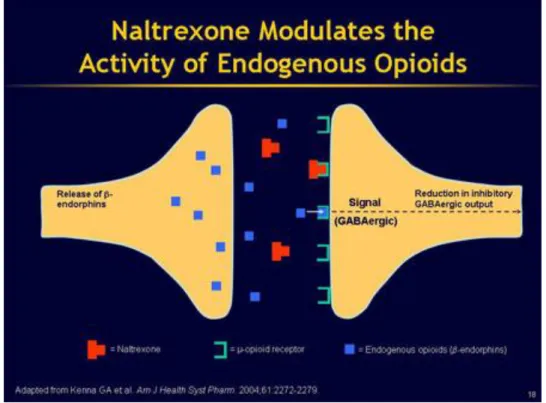
Figure 7: How Naltrexone works Page 11
Figure 8: How Acomprosate works Page 13
Figure 9: Baclofen – From its discovery to present time Page 17
Figure 10: How Baclofen works Page 18
Figure 11: Evolution of baclofen’s sales in France Page 31
List of Abbreviations
ADH Alcohol Dehydrogenase
ALDH Aldehyde Dehydrogenase
ANDA Abbreviated New Drug Application
ANSM The French National Agency for Medicines and Health Products Safety
AUD Alcohol Use Disorder
BAC Blood Alcohol Content
BRENDA Biopsychosocial evaluation, Report to the patient on assessment,
Empathic understanding of the patient’s situation, Needs collaboratively identified by the patient and treatment provider, Direct advice to the patient on how to meet those needs, Assess reaction of the patient to advice and adjust as necessary for best care
CNS Central Nervous System
DSM Diagnostic and Statistical Manual
EMA European Medicines Agency
FDA Food and Drug Administration
GABA Gamma Aminobutyric Acid
GSK GlaxoSmithKline
HDB High Dose Baclofen
HSL Health Sciences Library
IBIS International Baclofen Intervention Study
IND Investigational New Drug
MA Market Authorization
NCBI National Center for Biotechnology Information
NIH National Institutes of Health
NMDA N-methyl-D-aspartate receptor
RCT Randomized Controlled Trial
TRU Temporary Recommendation for Use
Introduction
According to the National Institute on Alcohol Abuse and Alcoholism, over 17
million Americans over 18 years of age are currently identified as having an alcohol use
disorder (AUD). (Alcohol Facts and Statistics, 2014) AUD is an internationally
recognized medical condition that can be attributed to anyone who meets any two of the
eleven criteria established by the Diagnostic and Statistical Manual, fifth edition
(DSM-5). (Appendix 1)
In 2010, Lim and colleagues reported that “[g]lobally, alcohol misuse is the fifth
leading risk factor for premature death and disability; among people between the ages
of 15 to 49, it is the first.” (as cited in Alcohol Facts and Statistics, 2014) In the United
States, alcohol is responsible for 88,000 preventable deaths annually. (Alcohol Facts
and Statistics, 2014) AUD leads to diseases such as cirrhosis, hepatitis, cancer, and
type 2 diabetes as shown in Appendix 2. (A-Team Alcohol Services, n.d.)
This paper will examine Baclofen as a drug to treat alcohol addiction, focusing on
the reduction of cravings and anxiety. Information from published medical results of
human trials will be discussed. It should be noted that this paper will not examine AUD
treatments that address alcohol withdrawal since this would constitute another area of
study.
Methodology
Review of online literature was accomplished using PubMed and NCBI electronic
databases, followed by Google Scholar searches through the University of North
the following: “alcoholism,” “Baclofen,” “dependence,” “addiction,” “clinical trial,”
“treatment,” “AUD,” and “review.” Since the treatment of AUD with Baclofen varies by
country, no limitation in terms of place and time was applied for this research.
Unpublished works, inaccessible articles due to registration or subscription services,
and articles not available in English were not included. Since “review” was part of the
inclusion criteria, meta-analysis and systematic reviews were selected based on
relevancy. Multiple professional domains including the National Institutes of Health
(NIH), the Food and Drug Administration (FDA), ClinicalTrials.gov, and the French
National Agency for Medicines and Health Products Safety (ANSM), were searched for
relevant data. The literature review was supplemented with cited sources within the
publications identified, as well as included grey literature.
Biological Description of AUD
When an individual drinks alcohol, the body will first metabolize the ethanol (main
molecule found in alcoholic beverages) and before any other nutrient because the
ethanol cannot be stored in the body. Upon intake of alcohol, the fluid goes straight to
the stomach and then the small intestine where up to 20% and 80%, respectively, of its
content will be absorbed into the bloodstream. (Altounian, 2014) After being absorbed
into the bloodstream, the ethanol goes to the liver as illustrated in Figure 1. (Duke
University - How does ethanol get to the lungs?, n.d.)The liver can only metabolize
ethanol at a rate of about one ounce of hard liquor per hour. (Alcohol Alert, 1997) The
leftover alcohol in the stomach will travel in cycles through the body (Figure 1) until the
- can take care of it and break the remaining ethanol down to the detoxified molecule
acetate that will eventually return into the bloodstream. (Duke University - How does
ethanol get to the lungs?, n.d.) This process of oxidation in the liver is responsible for
the detoxification of the drug in the body. While the excess ethanol travels through the
body, it goes to the lungs via the right side of the heart. (Duke University - How does
ethanol get to the lungs?, n.d.) At that point, about 5% of the alcoholic content is
exhaled by the lungs. (Duke University - How does ethanol get to the lungs?, n.d.) The
remaining ethanol will travel to the central nervous system (brain and spinal cord) and
then eventually finds its way back to the liver where more ethanol will be oxidized.
(Duke University - How does ethanol get to the lungs?, n.d.)
Figure 1: Flow of ethanol in the body
Source: Duke University - How does ethanol get to the lungs? (n.d.) Adapted from the www.thepepproject.net
There are billions of cells in the nervous system, called neurons, communicating
on Figure 2). (Benzodiazepines: How they provide their anxiolytic and hypnotic effects,
2012)In a healthy individual, Gamma-Aminobutyric Acid (GABA), an inhibitory
neurotransmitter (molecule that inhibits the generation of a signal in between neuron
cells), only will let a certain amount of negatively charged ions to pass through it after it
binds to the postsynaptic neuron as illustrated in Figure 2. (Benzodiazepines: How they
provide their anxiolytic and hypnotic effects, 2012)
Figure 2: GABA’s role in the synaptic cleft
Source: Benzodiazepines: How they provide their anxiolytic and hypnotic effects. (2012).
After consuming an alcoholic beverage, the ethanol binds to the GABA receptor
at the postsynaptic neuron and allows more activity going through. Within minutes of
alcohol intake, the individual will start feeling its effects on the brain as the larger than
normal intake of negatively charged ions going through the GABA receptors will
stimulate the release of beta-endorphins (another kind of neurotransmitter). (Altounian,
2014) Those beta-endorphin molecules will travel across the synapse and bind to
post-synaptic receptors, releasing the dopamine molecules that make individuals “feel good”.
neuron cells where the signals travel in loop to achieve a desire of satisfaction.
(Altounian, 2014)
Figure 3: How alcohol releases dopamine
Source: Naltrexone, 2014; Naltrexone With Without Prescription!,(n.d.)
Dopamine’s main characteristic is that it needs a continuously increasing intake of
alcohol to keep its effects steady since the GABA receptors, key to the release of
dopamine, become desensitized over time. (Altounian, 2014) Concurrently, the
molecules of alcohol will suppress the release of an excitatory neurotransmitter, the
glutamate, which in turn will slow down the brain activity. (DiSalvo, 2012) The alcoholic
therefore will increase his or her intake of alcohol in a quest to keep this “good feeling”
going. A larger intake of alcohol results in proportionally less absorption of the
be metabolized before being excreted. (Altounian, 2014) In the liver, the alcohol
molecule is broken down and converted into acetaldehyde and then acetic acid.
Retention of acetaldehyde during the acetaldehyde dehydrogenase is what individuals
feel as a hangover. Figure 4 provides a summary of the biology related to the intake of
alcohol.
Figure 4:Summary of biology related to alcohol intake:
Source: based on aforementioned methodology
An individual’s Blood Alcohol Content (BAC) increases when the body absorbs
alcohol faster than it can eliminate it. (Zakhari, n.d.) Binge drinking therefore increases
the potential for overdose of acetaldehyde that accumulates in the liver (as well as an Alcohol Intake
Stomach & Small Intestines Respectively 20 and 80% of fluid absorbed & released in bloodstream
(increases blood pressure) CNS Brain Increases activity of GABA-b receptors Triggers release of beta-endorphins
Triggers release of dopamine through mesolimbic pathway
Calms down & relaxes the individual (this is how Xanax works)
Suppresses release of excitatory neurotransmitter glutamate Slows down brain activity
Liver is responsible for about 90% of
elimination of alcohol in body (can metabolize <1
oz of hard liquor per hour) Ethanol acetaldehyde acetic acid (= acetate) Sweat, feces, milk, & saliva
eliminate < 5% of all alcoholic content
Lungs exhale about 5% of alcoholic content (detected by breathalyzers)
Kidneys eliminate about 5% of the ethanol in urine (ethanol suppresses action of diuretic vasopressin, which results in the drinker loosing more water than usual)
Enzyme alcohol dehydrogenase (ADH)
accumulation of the fatty acids that are no longer the liver’s priority for metabolism).
(Zakhari, n.d.) Binge drinking is also associated with the retention of alcohol in the
stomach that induces vomiting. (Zakhari, n.d.)
Existing AUD treatment options in the United States
FDA Guidance
Clinical trials lacked consistent guidance for defining and recruiting patients with
AUD. Most scientists refer to the DSM models, fourth and fifth editions, to recruit their
patients, but other characteristics such as the length of the study vary. In the United
States several clinical trials have been conducted but varying endpoints were used to
determine outcomes, not allowing for aggregation of efficacy and safety results across
trials. In February 2015, the FDA therefore published draft guidance for industry on the
approval of medications for the treatment of alcoholism and the population of those with
AUD. This guidance is currently being reviewed and updated by stakeholders involved
in the treatment of alcoholism. (US Department of Health and Human Services et al,
2015) The focus of this governmental paper is as follows.
We are issuing this guidance to better communicate our current thinking on the appropriate endpoints for clinical trials of drugs to treat alcoholism, and to apprise sponsors of possible alternatives to abstinence-based endpoints, which have often been considered an unattainable threshold in the clinical trial setting, and which may be considered a hindrance to clinical development for drugs to treat alcoholism. (US Department of Health and Human Services et al, 2015, p. 1) With this important aspect in mind, the draft guidance also suggests:
(women). Standard drinks are defined in the United States as containing 14 grams of alcohol, such as would be found in a standard shot of hard liquor, a 12 ounce bottle of beer, or a 5-ounce glass of wine. An analysis of the proportion of patients who attain and sustain a pattern of drinking that never exceeds the heavy drinking definitions may be appropriate.
. . .
DAAAP’s current recommendation is for trials of 6 months’ duration, with a primary endpoint of the proportion of patients who do not have any heavy drinking days during the observation period (percent no heavy drinking days). (US Department of Health and Human Services et al, 2015, p. 2-3)
The FDA has approved drugs for the American market for the treatment of AUD.
The next section will describe both approved and “off-label” drugs for the treatment of
AUD in the United States.
FDA approved medications in the treatment of AUD
As of the writing of this paper, three drugs -- Disulfiram, Naltrexone, and
Acamprosate – are approved by FDA for the treatment of AUD as shown in Figure 5.
Source: FDA-approved Pharmacological Treatments for Alcohol Dependence (Wilkins, n.d)
Disulfiram
The generic drug Disulfiram, first introduced by Danish scientists to North
America in 1949, received its FDA approval for the treatment of AUD in 1951. (Kragh,
2008) This drug has no labeling authorization other than for AUD treatment. Disulfiram
(brand name is Antabuse) works in the liver by inhibiting the process of alcohol
dehydrogenase in which acetaldehyde accumulates at an average of a tenfold
compared to the regular metabolism of alcohol without the drug. (Figure 6) The patient
outcome is an adverse reaction when the drug encounters alcohol with symptoms
ranging from nausea to vomiting, and headaches.
Even though Disulfiram is often prescribed, it is limited due to non-compliant
patients who do not take their medicine to be able to drink. Recently, the European
market saw the emergence of an Antabuse implant that goes under the skin to increase
compliance with treatment. This form of Antabuse has not yet been proposed to the
FDA for the treatment of AUD in the United States. (Weighing The Pros And Cons Of
Antabuse For Alcoholics, 2014) The FDA approved recommended daily dose is from
125 mg up to 500 mg per day, which can damage the liver if taken on a regular basis
(Incorporating Alcohol Pharmacotherapies Into Medical Practice – Chapter 3 -
Disulfiram, 2009).
Source: Disulfiram: An aversion-based Pharmacotherapy (Wilkins, n.d)
The positive aspects of using Disulfiram as a medication in the treatment of AUD
include over sixty years worth of evidence based results and the fact that the drug does
deter the patient from taking alcohol. On the other hand, the drug does not stop the
cravings nor does it normalize the brain activity. Additionally, by initiating an adverse
reaction, the drug faces the issue of compliance and the potential interaction from
non-intentional ingestion of food containing alcohol. The major disadvantage for this
medication is that it only works at high doses, putting additional stress on the liver and
therefore is not compatible with patients with hepatic concerns.
Naltrexone hydrochloride
Vivitrol (brand name) was approved by the FDA in 1994. (Vivitrol, n.d.) This drug
brain by binding to GABA receptors at the postsynaptic neurons in order to inhibit the
activity of endorphins and release of dopamine as illustrated in Figure 7. (Wilkins, n.d )
Inhibiting this activity results in decreased cravings for alcohol and makes the use of
alcohol less rewarding by decreasing the effects of euphoria. (Incorporating Alcohol
Pharmacotherapies Into Medical Practice - Chapter 4—Oral Naltrexone, 2009)
Figure 7: How Naltrexone works
Source: Naltrexone Modulates the Activity of Endogenous Opioids (Wilkins, n.d)
The recommended dose is 50 mg daily for 12 consecutive weeks. (Naltrexone - FDA
prescribing information, side effects and uses, 2014) Until 2006 when the FDA
approved the extended-release injectable Naltrexone, Naltrexone in tablets was facing
issues with compliance in outpatient treatment settings, due to the disease taking over
the individual’s behavior. Injectable Naltrexone only requires one shot of 380 mg a
Pharmacotherapies Into Medical Practice - Chapter 5 - Extended-Release Injectable
Naltrexone, 2009)
A placebo controlled, outpatient, double blind clinical trial, involving 104 cases,
found a 51% abstention rate (versus 23% for the Placebo) and a relapse rate at 31%
(compared to 60% for the Placebo). (Naltrexone - FDA prescribing information, side
effects and uses, 2014) An advantage of Naltrexone is that the drug does not induce an
adverse reaction, but instead blocks brain receptors to remove the feeling of pleasure
from alcohol. It was also associated with lower patient cravings compared to the
patients in the placebo group. (Naltrexone - FDA prescribing information, side effects
and uses, 2014) Thompson concluded that “Naltrexone has a greater effect on
reducing relapse to heavy drinking than it does on maintaining abstinence.”(Thompson,
2014) The label also includes a warning for hepatotoxicity. (Vivitrol, n.d.) Since most
patients with AUD have liver issues, Krishnan-Sarin and colleagues noted “the potential
risk of hepatotoxicity at high doses requires caution when treating patients with liver
disease”. Naltrexone is not indicated in the treatment of AUD in those with a
co-addiction to opiates since the drug is an opiate antagonist. (Krishnan-Sarin et al, n.d.)
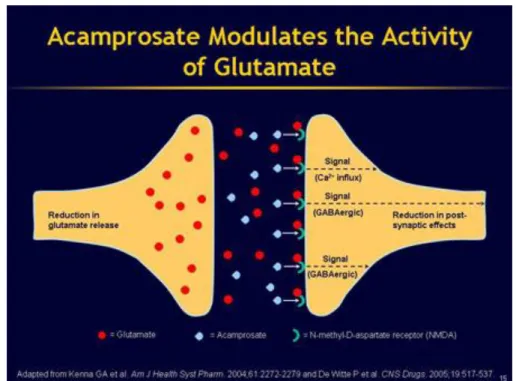
Acamprosate calcium
Campral (brand name) was approved by the FDA for the treatment of AUD in
2004 and works in the brain by modulating and normalizing brain activity. (FDA - Drug
Approval Package, n.d.) Acamprosate specifically targets levels of glutamate and
GABA receptors, responsible for the release of NMDA, as illustrated in Figure 8.
(Wilkins, n.d) NMDA are glutamate receptors that increase over time in alcoholic
significantly modulate the function of these receptors and ion channels at clinically
relevant concentrations. Thus, the clinical effectiveness of Acamprosate in the
treatment of alcoholism is not likely due to direct effects on these receptors or ion
channels.” (Reilly et al, 2008, p. 1) The drug is primarily used for the treatment of
withdrawals. When the patient is withdrawing from alcohol, there is an increase in
activity of neurotransmitters, which the drug Acamprosate helps to regulate.
(Krishnan-Sarin et al, n.d.)
Figure 8: How Acamprosate works
Source: Acamprosate Modulates the Activity of Glutamate (Wilkins, n.d)
Campral is “not known to cause alcohol aversion and does not cause a
disulfiram-like reaction as a result of ethanol ingestion”, and the drug’s efficacy was
supported by three out of four placebo controlled studies. (Campral [Acamprosate
metabolized in the liver but in the kidneys affording a treatment option for patients with
liver cirrhosis, but not in those with renal impairment. (Campral [Acamprosate Calcium]
Delayed-Release Tablets, n.d) Since this medication does not reproduce the ill effects
of Disulfiram, Acamprosate does not deter alcohol consumption but is promoted for
alcohol abstinence. (Mann et al., 2004; Kranzler and Gage 2008)
Drugs currently under investigation in the treatment of AUD
To date, and as noted by Krishnan-Sarin et al, the FDA approved medications in
the treatment of AUD
have modest efficacy, and there is a great need for newer medications that target different neurochemical systems and which could be used either as adjunctive treatments or to treat subpopulations of drinkers. Furthermore, it also is important to improve current treatment options by understanding and incorporating
differences in how people with certain genes respond to medication (i.e., pharmacogenetic differences).
(Krishnan-Sarin et al, n.d., p. 1)
NIH recently published a list of drugs that are being researched for the treatment of
AUD. These potential therapies are Varenicline, Gabapentin, Topiramate, Ondansetron,
Nalmefene, and Baclofen. (NIH - Research on Promising Medications not approved by
the U.S. Food and Drug Administration [FDA]) to Treat Alcohol Use Disorder (AUD),
n.d.) Other medications being investigated in preliminary animal trials include
Ezogabine that has shown some positive results. (Knapp et al, 2014)
Varenicline
Chantix (brand name) was approved by the FDA in 2006 for smoking cessation
treatment. (Chantix - Highlights of Prescribing Information, 2014) Varenicline belongs to
though definite results are not published. (Krishnan-Sarin et al, n.d) The FDA recently
corrected the drug’s labeling by noting that those taking Chantix “experiencing
increases intoxicating effects of alcohol…Some cases described unusual and
sometimes aggressive behavior, and were often accompanied by amnesia for the
events.” (Chantix - Highlights of Prescribing Information, 2014, p. 3) Therefore, this
noted interaction with alcohol limits its use for AUD treatment to a sub-population
already sober prior to enrolling in a treatment plan.
Gabapentin
Neurontin (brand name) was approved by the FDA for the treatment of epilepsy,
seizures, and pain management of shingles or the herpes virus in 1993. (Gabapentin -
FDA prescribing information, side effects and uses, 2015) A recent dose-ranging clinical
trial that was funded by NIH showed promising results in the treatment of AUD. (Mason
et al, 2014) Mason’s team showed that "Gabapentin (particularly the 1800-mg dosage)
was effective in treating alcohol dependence and relapse-related symptoms of insomnia,
dysphoria, and craving, with a favorable safety profile." (Mason et al, 2014) Its use for
the treatment of AUD has not been reviewed and approved by the FDA as of the writing
of this paper. At present, a contraindication exists:
Using gabapentin together with ethanol can increase nervous system side effects such as dizziness, drowsiness, and difficulty concentrating. Some people may also experience impairment in thinking and judgment. You should avoid or limit the use of alcohol while being treated with gabapentin.
(Gabapentin - FDA prescribing information, side effects and uses, 2015, p. “Gabapentin and Alcohol / Food Interactions”)
Since Gabapentin is absorbed and not metabolized, patients with severe renal
dysfunction should not take the medication. Gabapentin is another GABA drug of
“showed similar or greater positive outcomes when compared to existing FDA approved
treatments for alcohol dependence”. (as cited in NIH-funded study finds that gabapentin
may treat alcohol dependence, 2013)
Topiramate
Topiramate, an anti-seizure medication, received its FDA approval in 2009.
(Topiramate - FDA prescribing information, side effects and uses, 2014) The drug acts
on both GABA-a and glutamate receptors in the brain. (NIH - Research on Promising
Medications (not approved by the U.S. Food and Drug Administration [FDA]) to Treat
Alcohol Use Disorder (AUD), n.d.)
Ondansetron
Zofran (brand name) was first approved by the FDA in 1991 and the generic form
followed in 1996. (Ondansetron - FDA Approved Drug Products, n.d.) According to
Johnson et al. and Kranzler et al., both teams who conducted similar studies and were
cited by Krishnan-Sarin and colleagues in a NIH document found, “Clinical trials of this
medication have shown efficacy in reducing drinking behavior, especially in drinkers
with early-onset (type B) alcoholism”. (Johnson et al., 2000; Kranzler et al., 2003, as
cited in Krishnan-Sarin et al, n.d) This information would imply a targeting of this product
to those diagnosed with early-onset alcoholism.
Nalmefene
Nalmefene was authorized by the European Medicine Agency in 2013 to treat
AUD. However, it is not FDA approved for the treatment of AUD. (Nalmefene - EPAR
summary for the public, 2012) The drug works by attaching “to certain opioid receptors
those who use opioids and “[i]t must also not be used in patients with severe liver or
kidney impairment or a recent history of acute alcohol withdrawal syndrome …”.
(Nalmefene - EPAR summary for the public, 2012, p. 2,3)
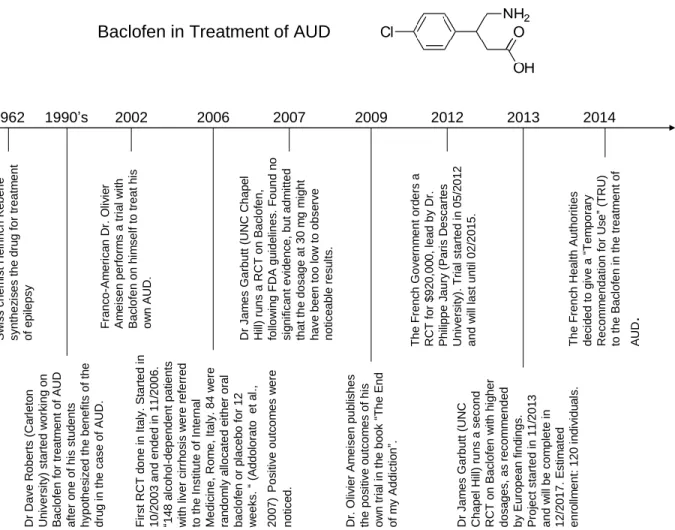
Baclofen
Baclofen is a potential drug for the treatment of AUD. Since its first discovery in
1962 for the treatment of epilepsy, the drug has shown promise for recovering addicts
suffering from AUD. Figure 9 shows the timeline from the molecule’s discovery in 1962
to its TRU in France in 2014.
Figure 9: Baclofen – From its discovery to present time
1962 S w iss ch e m ist Hein ri ch K e b e rl e syn th e z is e s th e d ru g f o r t re a tm e n t o f e p ile p sy 1990’s Dr Da ve R o b e rts (Ca rl e to n Un ive rs ity ) st a rt e d w o rk in g o n B a clof e n fo r t re a tm e n t o f A UD a ft e r o n e o f h is st u d e n ts h yp o th e s ize d t h e b e n e fi ts o f th e d ru g i n t h e ca se o f A UD . 2002 F ra n c o -A m e ri ca n Dr . O liv ie r A m e ise n p e rf o rm s a t ri a l w it h B a clof e n o n h im se lf to t re a t h is o w n A UD . 2009 Dr . Oli v ier A m e ise n p u b lish e s th e p o s it ive o u tco m e s o f h is o w n t ria l in t h e b o o k “T h e E n d o f m y A d d ict io n ”.
Baclofen in Treatment of AUD
Approved by FDA in 1977 for the treatment of spasticity, the generic drug
Baclofen (former brand name was Lioresal) works in the CNS by mimicking the naturally
occurring inhibitors GABA-b neurotransmitters. (Brennan et al, 2013) The synthetic drug
binds to GABA receptors at the postsynaptic neuron so that alcohol molecules have no
or fewer binding sites and less stimuli results from this action. Less activity
(neurotransmitters) going through those binding sites translates into a decrease in
activity in the nerves that control muscle contraction and relaxation. (Brennan et al,
2013) In a healthy individual, GABA-b (only GABA-b neurotransmitters seem to have
the desired effect with Baclofen) are sufficiently present to keep that individual calm and
relaxed by causing the activity of other nerves to decrease. (Brennan et al, 2013) A
patient lacking those GABA-b neurotransmitters will begin to feel the effects of anxiety
and possibly feel his or her muscles involuntarily contracting, which is the case in
multiple sclerosis for which Baclofen has demonstrated the ability to address (Figure 10)
Figure 10: How Baclofen works
Source: Alcoholism 'cured' By Baclofen - Spinal Cord Injury Health Issues, n.d.
The FDA suggests a recommended maintenance dosage for the treatment of
muscle spasms not to exceed 80 mg per day. (FDA Approved Drugs - KEMSTRO -
suggested that this drug would not be efficacious in the treatment of AUD at a dose
equal to or lower than 80 mg per day, since “doses exceeding 250 or 300 mg/day are
often necessary to produce a state of complete indifference to alcohol”. (DeBeaurepaire,
2014, Introduction) While treating his own AUD, Dr Olivier Ameisen was taking a
maintenance dose of up to 270 mg per day. (Rolland, et al, 2012, p. 1) Similar results
were observed by Dr Garbutt when his first American trial in 2007 studied the use of
Baclofen at a dosage of 30 mg per day. This study did not demonstrate support for
Baclofen in the treatment of AUD. (Garbutt et al, 2010) However, Garbutt et al
concluded, “Baclofen was associated with a significant reduction in state anxiety
(F(1,73)=5.39, p=0.02).” (Garbutt et al, 2010, p. 1)
Ezogabine
Potiga (brand name) was approved by the FDA for the treatment of seizure
disorders in 2011. (Potiga - FDA Approved Drug Products, n.d.) A recent study lead by
researchers at Boston University School of Medicine found positive outcomes with
Ezogabine in the treatment of AUD. (Knapp et al, 2014) However, its use for the
treatment of AUD has not been reviewed by the FDA.
Psychiatric drugs
Physicians might prescribe other pharmaceutical drugs in the treatment of AUD,
especially when it comes to dual-diagnosis including a psychiatric aspect. Such
medicines include diazepam (valium) or amitriptyline (antidepressant). (Krupitsky et al,
1993) Those drugs can be taken concurrently with most prescribed AUD medicines. To
date, only one study has evaluated the effectiveness of diazepam, amitriptyline, and
effective drug for affective disturbances in alcoholic patients, with efficacy superior to
placebo and equal to diazepam and amitriptyline.” (Krupitsky et al, 1993, p.157)
Negative outcomes observed in RCT and study cases
Despite encouraging studies performed worldwide, the replication of confirmatory
positive outcomes has failed to confirm the efficacy of Baclofen in the treatment of AUD.
Some of the most influential studies are described below. Those trials with negative
outcomes are listed chronologically.
American Trial
For his first trial, Dr Garbutt, affiliated with the University of North Carolina at
Chapel Hill, intended to reproduce the Italian trials lead by Dr Addolorato to confirm the
positive outcomes observed at a dosage of 30 mg per day. His aim was “to test the
efficacy and tolerability of baclofen in alcohol dependence in the United States.”
(Garbutt et al, 2010, p. 1849) The study screened 121 individuals to obtain 80
randomized subjects (balanced for gender) and followed them for twelve consecutive
weeks. (Garbutt et al, 2010) His findings did not support Dr Addolorato’s outcomes as
he stated: “Despite encouraging preclinical data and prior positive clinical trials with
baclofen in Italy, the current trial did not find evidence that baclofen is superior to
placebo in the treatment of alcohol dependence.” (Garbutt et al, 2010, p. 1849)
French Meta-analysis
A meta-analysis undertaken by French scientist Dr Lesouef from the French
Pharmacology and Therapeutic Society, confirmed the results found by Dr Garbutt.
maintenance of abstinence and the decrease of craving in alcohol-dependent patients.”
(Lesouef et al, 2014) He found that treatment with a low dosage of Baclofen (30 mg per
day) “[c]ompared to placebo, baclofen was associated with a significant increase of
179% in the percentage of abstinent patients at the end of the trial, without
heterogeneity. For secondary outcome measures, based on a random-effect model, no
significant effect of baclofen was observed compared to placebo.” (Lesouef, et al, 2014)
Israeli Trial
Dr Ponizovsky, from the Sha'ar Menashe Mental Health Center at the Bruce
Rappaport Medical Faculty in Haifa, Israel, undertook a multi-site, placebo controlled
clinical trial with the aim “to test the efficacy and tolerability of baclofen in alcohol
dependent patients in Israel.” (Ponizovsky, et al, 2014, p. 24) Sixty-four patients were
randomized to receive either baclofen 50 mg/day (n=32) or placebo (n=32), from which
a total of 62% completed (72% in the baclofen group and 53% in the placebo group) the
12-week trial and 37% completed the 52-week follow-up (34% baclofen; 41% placebo).
(Ponizovsky, et al, 2014) Dr Ponizovsky concluded that “[a] significant reduction in
levels of distress, depression and craving and improved HRQL occurred for both arms”
and that “[u]nlike previous positive trials in Italy, and similarly to a negative trial in the
USA, we found no evidence of superiority of baclofen over placebo in the treatment of
alcohol dependence. However, the high placebo response undermines the validity of
this conclusion.” (Ponizovsky, et al, 2014, p. 24)
Hypotheses for negative observations in RCTs
Dr. Leggio reported that “the Italian study recruited patients with more severe
AUD than the study conducted in the US. These differences suggest that baclofen may
be more potent and effective in the treatment of severe AUD, rather than moderate
AUD”. (Leggio et al., 2010 as cited in Agabio & Colombo, 2014, p.7) Even if this held
true, it would seem that Italian patients would therefore require higher dosages than the
minimal 10 mg t.i.d to show an overall improvement of their health.
Most of the patients recruited by the clinical trials discussed are patients who
have tried other treatment options including FDA approved Disulfiram, Naltrexone, and
Acamprosate, with or without a combination of other drugs and/or therapies to treat their
AUD. I hypothesize that some of these patients might also have developed some
immunity and resistance to treatment options – including Baclofen - with their drinking
habits.
Length of study participant treatment
Most clinical studies discussed in this paper that evaluated the efficacy of
Baclofen in the treatment of AUD, lasted 12 weeks (=84 days). As reported by Dr
Ameisen himself in the journal Alcohol and Alcoholism, it took him at least 37 days to
titrate to the dose of 270 mg/day, based on a starting dose of 15 mg/day with
increments of 20 mg/day every third day. (Ameisen, 2004, p.148) In fact, Dr. Ameisen
may have reached a plateau for a while based on increasing side-effects and thereby
increasing the timing by which he reached the maximal dosage of 270 mg/day.
(Ameisen, 2004, p.147) Also, after noticing that side-effects outweigh the benefits of the
Baclofen, Dr Ameisen decreased his intake of the Baclofen, but did it slowly to avoid
maintenance dosage of 120 mg/day at 9 weeks while still experiencing alcohol cravings
for which he temporarily increased his daily intake by 40 mg and stabilized his behavior
with no additional intake of Baclofen at week 12. (Ameisen, 2004, p.148) Thus, I
suggest that upcoming trials and interventions shall last more than 12 weeks in order to
further study Bacolfen’s efficacy and safety for the treatment of AUD.
Dosage
Dosage factors to consider in the use of the Baclofen include the following:
typology of the patient (severe versus moderate AUD), inpatient versus outpatient,
gender, comorbid mental disorder, renal function (since Baclofen is discarded via the
kidney). For example, inpatient study participants may be able to undergo stronger
treatments and are more inclined to be compliant with the drug intake. Outpatient
participants have greater access to alcohol and can be less compliant with their drug
intake as there is no one to supervise their compliance. Further one should not undergo
large dose increments without close medical supervision. In addition, the half-life of
Baclofen is short lived, requiring patients to take the drug on a t.i.d. (3 times per day)
protocol. As Dr. DeBeaurepaire suggested, "Significant relationships were found
between the amount in grams of alcohol taken before treatment and the maximal dose
of baclofen required, and between the existence of a mental disorder and a lesser effect
of baclofen." (DeBeaurepaire, 2012, p.103) This finding coincides with Dr Addolorato’s
findings reported in 2011.
AUD is a chronic disease that quite often is associated with mental disorders.
There might be a different assimilation of the drug when mixed with other psychotic
often show a bad compliance with treatments.” (as cited in DeBeaurepaire, 2012, p.
103) DeBeaurepaire concluded,
Potential limitations in the effectiveness of baclofen include the coexistence of a mental disorder, the concomitant use of other psychotropic drugs, a lack of real motivation in patients to stop drinking, and the impossibility to reach the optimal dose of baclofen because of unbearable side-effects (sometimes possibly related to too sharp a protocol of dose escalation). (DeBeaurepaire, 2012, p.103)
Prominent Ongoing Trials
Since the previous trials have been challenged, ongoing trials are taking into
account the identified flaws to further investigate the efficacy of Baclofen in the
treatment of AUD.
French RCT
An ongoing trial is being led by Dr. Philippe Jaury from Assistance Publique in
Hôpitaux de Paris, France. His aim is “to show the effectiveness to a year of baclofen
compared to placebo, on the proportion of patients with a low risk alcohol consumption
or no, according to the WHO standards.” (Jaury, 2015) The study plan is to enroll 330
adults. Enrollment began in May 2012 and recruitment has concluded. Study
participants were followed for 12 months, with the participants in the baclofen treatment
group receiving up to 300 mg per day (that can be titrated down as medically indicated)
to test the efficacy of high dose Baclofen in the treatment of AUD. (Jaury, 2015)
American RCTs
Dr Garbutt’s trial
Dr Garbutt, who first led a clinical trial to replicate Dr Addolorato’s outcomes
(results published in 2010), has undertaken another trial to test high dose Baclofen
test the hypothesis that a robust dose of baclofen (90 mg/day) has efficacy and is safe in individuals with alcohol dependence. Furthermore, the proposal will test whether an indicator of physical dependence, i.e. drinks/drinking day, predicts response to baclofen. Additionally, the proposal will examine the anti-anxiety effects of baclofen within an alcohol dependent population and ascertain whether baseline levels of anxiety predict response to baclofen. (Garbutt, 2014)
The clinical trial has an estimated enrollment of 120 adults. Recruitment began in
November 2013 and is continuing as of the writing of this paper. The study’s overall
estimated completion date is October 2017. (Garbutt, 2014)
One of the pitfalls to consider in this study is the root definition of HDB. In this
study, Dr Garbutt is administering doses up to 90 mg per day before decreasing the
dosage to match the threshold of tolerance of the side-effects for the patients. (Garbutt,
2014) In a recent publication, Dr DeBeaurepaire mentioned that drug summaries
recommend not exceeding the daily dose of 75–80 mg, which agrees with the FDA
labeling of Baclofen for the treatment of spasticity. (DeBeaurepaire, 2014) Anything
above this dosage would be considered HDB, although “long-term studies have shown
that doses exceeding 250 or 300 mg/day are often necessary to produce a state of
complete indifference to alcohol”. (DeBeaurepaire, 2014, p. 143) For this reason,
the French Health Safety Agency released a recommendation allowing for the prescription of baclofen to be given up to 300 mg/day, but not beyond, for the treatment of alcohol dependence (French Ministerial decree of June 13, 2014). (DeBeaurepaire, 2014, p.143)
Dr Leggio’s trial
Another American study has been undertaken by Dr Leggio for the NIH. (Leggio,
2014) This clinical trial’s aim is to “see if baclofen is safe and helpful for people who
to 65). Enrollment began in December 2012 and the overall study completion is
targeted for September 2020. (Leggio, 2014) This study is unique as note by Leggio:
The present project proposes investigating baclofen using a design similar to that used in the previous pilot study (thus, an already validated paradigm), thus
representing not only the first study testing baclofen in alcoholic individuals with high anxiety levels, but also the first study investigating baclofen s biobehavioral mechanisms in such a population for which baclofen may hypothetically show a very robust effect. (Leggio, 2014)
Regulations and processes for drug approval
FDA regulations in the United States
In the United States, the FDA has not considered the approval of the Baclofen in
the treatment of AUD. Conflicting efficacy results compounded with side-effects that
include drowsiness, dizziness, and memory trouble as observed in RCTs do not support
the efficacy of Baclofen to expand its labeling for the treatment of AUD. (Ponizovsky et
al, 2014, p.24)
How to get the FDA’s approval?
The FDA's Center for Drug Evaluation and Research (CDER)’s mission is to
“ensure that drugs marketed in this country are safe and effective”. (FDA - How Drugs
are Developed and Approved, 2014) The CDER is composed of representative
members of the diverse medical professions, including physicians, pharmacists,
chemists, biostatisticians, to name a few. Their mission is to review Investigational New
Drugs (IND) applications and New Drug Applications (NDA) submitted by the drug’s
pharmaceutical sponsor. (FDA - How Drugs are Developed and Approved, 2014) The
sponsor will have to wait for the CDER’s review and approval before starting clinical
IND (Investigational New Drug)
After researchers proved the efficacy of a molecule in the treatment of a specific
medical condition on animals, a physician can make a request to the FDA to further
investigate the compound through a pre-clinical human study. (FDA - Investigational
New Drug (IND) Application, 2014) The sponsor will request an IND and wait 30 days
before beginning the trial. (FDA - Investigational New Drug (IND) Application, 2014)
During this time frame, the FDA will review the literature provided by the drug’s sponsor
and can decide to refuse the right to do any human experimentation if they believe the
risk of harm to humans is too high. (FDA - Investigational New Drug (IND) Application,
2014)
NDA (New Drug Application)
In place since 1938, the NDA allows the drug’s sponsor to be considered for the
sale and marketing of the drug that previously received an IND approval. (FDA - New
Drug Application (NDA), 2015) During this process, CDER reviews the scientific
evidence that confirms both safety and effectiveness of the medicine for the proposed
labeling. CDER can approve or deny the sponsor’s request for approval in the
American market based on the principle of beneficence. (FDA - New Drug Application
(NDA), 2015) Among other key elements reviewed by the FDA, the process of
manufacturing the drug also is taken into account as it must match current FDA’s
standards. (FDA - New Drug Application (NDA), 2015)
ANDA (Abbreviated New Drug Application)
When the patent of an existing innovator drug comes to expiration, a drug
(FDA - Abbreviated New Drug Application (ANDA): Generics, 2014) In its application,
the sponsor has to prove that its intended generic drug is bioequivalent, meaning that its
composition and biological use are similar to those of the innovator drug. (FDA -
Abbreviated New Drug Application (ANDA): Generics, 2014)
Off-label use in the United States
Physicians are often considered the “learned intermediaries” in between the
manufacturers of the drug and the patients. (Salbu, 1999) Physicians shall respect the
description and recommendations of use as presented on the drug’s label before
prescribing it to their patients. The FDA’s labeling requirements, in place since 1938,
confers safety to the patient as an end-user of the product. (FDA - New Drug
Application (NDA), 2015) If the physician were to prescribe a drug other than for the
recommended use that has been approved by the FDA, he or she would do so
“off-label”. If a manufacturer wants one of their drugs to be considered for use under a
different label, meaning a different use, the sponsor would have to submit under the
NDA process. (Salbu, 1999) The legal use of Baclofen in the treatment of AUD in the
United States would fall into this category. According to Salbu, “It would be logistically
impracticable, although not technically impossible, for Congress or the FDA to ban the
off-label use of drugs.” (Salbu, 1999, p.188) To this day, the “off-label prescription was
permissible before Congress’s 1997 liberalizations.” (Salbu, 1999, p.190) In fact, the
FDA only has legal authority on manufacturers, not physicians. (Salbu, 1999, p.190)
Legally, the prescription of an off-label drug without the patient’s consent is not
medical ethics and provide care for their patients in their best interest, which I propose
can sometimes include the thoughtful use of an off-label prescription.
EMA and ANSM regulations in France
In France, Baclofen has recently been authorized for the treatment of AUD under
the Temporary Recommendation for Use (TRU) decree.
French National Agency for Medicines and Health Products Safety (ANSM)
In France, pharmaceutical companies have the choice to either seek national
market authorization (MA) through the ANSM or obtain European approval via the
European Medicines Agency (EMA), the European FDA equivalent. (Rémuzat et al,
2013) In 2011, two bills drastically changed the conditions of access of pharmaceutical
drugs to the market and their conditions for reimbursement. (Rémuzat et al, 2013)
Those laws also saw the emergence of the ANSM. (Jeannet & Maraninchi, 2013)
Before then, pharmaceutical companies only could have a MA for the French territory
through the EMA. (Jeannet & Maraninchi, 2013) The newly created ANSM made it a
priority to implement a new framework for off-label prescribing via the emergence of the
Temporary Recommendation for Use (TRU). (Rémuzat et al, 2013)
Temporary Recommendation for Use
In 2014, after noticing the increasing evidence that supports the drug Baclofen in
the treatment of AUD, French health authorities decided to regulate its use under a
“temporary recommendation for use” (TRU). In France, when evidence-based trials
prove that a drug’s benefits outweigh the risks involved, it can receive a Market
Authorization (MA) – equivalent to the FDA approval for labeling in the United States.
diseases for which the drug has proven to be efficacious. In some instances, some
medicines are prescribed off-label “to fulfill a public health need not covered within the
scope of an existing MA”. (Temporary Recommendation for Use (TRUs), 2012) Two
conditions need to be fulfilled in order for the drug to receive a TRU: “there is an unmet
therapeutic need” and “the benefit/risk ratio of the medicine is assumed to be favorable
based on the available scientific efficacy and safety data.” (Temporary
Recommendation for Use (TRUs), 2012) A TRU is temporary as the acronym suggests
and has a maximum length of approval of three years. During these three years, public
health authorities will gather accumulated data and either dismiss the drug’s use or
evaluate alternatives such as labeling it for the disease it received a TRU approval.
Baclofen fell into this category and is now regulated by the French Public Health
authorities under a TRU.
Figure 11 shows the drastic increase in sales of Baclofen after the release of the
notoriously famous book “The End of my Addiction” from Dr. Olivier Ameisen in 2008.
(Figure 11)
Source: Rolland, et al, 2012
Discussion
Implementing a TRU in the United States
Due to the lengthily and costly process required for a drug to be approved in the
United States, one should consider implementing the framework of TRU successfully
developed in France a few years ago. In the case of Baclofen, even though the drug
might be considered for approval in the treatment of AUD within the next few years, to
date, only three prescription drugs are currently legally available to patients suffering
from AUD in the United States. For many patients, the drugs Naltrexone, Disulfiram,
and Acamprosate are not a treatment option because of the hepatic concerns
emanating from ingesting alcohol. For other patients, those treatments have proven to
Since prescribing “off-label” is legal in the United States but still not popular,
consideration of a TRU would legally protect and encourage physicians to prescribe
Baclofen as a treatment option when all others have failed, and while still following the
guidelines of the medical code of ethics. Since 88,000 deaths due to alcoholism are
preventable each year in the United States, using a TRU to frame the legal distribution
of Baclofen would potentially save thousands of American lives before the FDA
considers it for labeling authorization for the treatment of AUD. (Alcohol Facts and
Statistics, 2014)
Positive outcomes observed in RCTs and study cases
As noticed in Appendix 4, there have been at least twelve relevant worldwide
studies attempting to prove the benefits related to the use of Baclofen for the treatment
of AUD. Most of the studies might be limited to broad application due to the inability to
detect both statistically and clinically meaningful results due to the small sample sizes.
They shall therefore be discussed to provide support of a trend that requires the
involvement of more statistically rigorous studies. The following trials are sorted in
chronological order.
Russian Trial
Nearly a decade before Dr Ameisen shared with the rest of the world his
discoveries based on self-administered Baclofen in the treatment of his AUD, Dr
Krupitsky explored the positive effect of the drug in the context of AUD. Dr.Krupitsky,
from the Leningrad Regional Dispensary of Narcology in Russia, was the lead
investigator in a clinical trial that involved “ninety alcoholic patients with the secondary
study arms in this trial, namely one group of patients receiving 37.5 mg per day of
Baclofen, another group receiving diazepam 15 mg per day, a third group receiving
amitriptyline 75 mg per day and the last group received a placebo tablet. (Krupitsky et al,
1993) The aim of the study was to identify which drug was more efficient in the
treatment of AUD. (Krupitsky et al, 1993) His findings were that “baclofen is an effective
drug for affective disturbances in alcoholic patients, with efficacy superior to placebo
and equal to diazepam and amitriptyline. At the same time baclofen does not have the
side-effects and complications of the latter.” (Krupitsky et al, 1993, p. 157)
Even though those results are encouraging, the methods used in this study do
not allow for generalization since there were too few individuals in each group to detect
statistically significant differences. Also, the study suffered from another flaw, the fact
that it was not a double-blinded experiment. (Krupitsky et al, 1993)
Italian Trials
Dr. Addolorato et al: 2002
The first European study was lead by the investigator Dr. Addolorato from the
Institute of Internal Medicine, Catholic University of Rome in Italy. (Addolorato et al,
2002) This study’s aim was to provide “a first evaluation of the efficacy of baclofen in
inducing and maintaining abstinence and reducing craving for alcohol in
alcohol-dependent patients in a double-blind placebo-controlled design.” (Addolorato et al, 2002,
p. 504) In this context, Dr Addolorato recruited 39 alcohol-dependent patients. These
patients were administered a dose of 15 mg/day for the first 3 days of the study and 30
mg/day for the subsequent 27 days. (Addolorato et al, 2002, p.505) His findings were as
A higher percentage of subjects totally abstinent from alcohol and a higher
number of cumulative abstinence days throughout the study period were found in the baclofen, compared to the placebo, group. A decrease in the obsessive and compulsive components of craving was found in the baclofen compared to the placebo group; likewise, alcohol intake was reduced in the baclofen group. A decrease in state anxiety was found in the baclofen compared to the placebo group. (Addolorato et al, 2002, p.504).
The same way Dr Krupitsky’s trial suffered from flaws in the design of his study, Dr
Addolorato’s first trial included a sample size too small that the results cannot be
generalized to a population due to the inability to detect statistically significant along
with clinically relevant findings.
Dr. Addolorato et al: 2007
Dr. Addolorato’s second study was designed “to investigate the effectiveness and
safety of baclofen in achieving and maintaining alcohol abstinence in patients with liver
cirrhosis.” (Addolorato, et al, 2007, p. 1915) This trial included “148 alcohol-dependent
patients with liver cirrhosis”. (Addolorato et al, 2007, p. 1915) The dosage administered
remained equal to that of the first trial at 30 mg per day. (Addolorato et al, 2007, p.
1916) The findings followed the same positive trend observed five years prior: “Of 42
patients allocated baclofen, 30 (71%) achieved and maintained abstinence compared
with 12 (29%) of 42 assigned placebo”. (Addolorato, et al, 2007, p. 1915) Though a
positive clinical trend was observed, the study was disregarded by most healthcare
professionals because of the small cohort used in the study.
French Trial
A three year investigation, lead by French doctor DeBeaurepaire from Groupe
Hospitalier Paul-Guiraud in Villejuif, France included “[a] hundred patients with alcohol
study participants were patient referrals from Dr Ameisen’s practice. (DeBeaurepaire,
2012) The aim of the study was “to examine the long-term effects of baclofen in a large
cohort of alcohol-dependent patients compliant to baclofen treatment.” (DeBeaurepaire,
2012, p. 1) Dosing ranged from 30 to 330 mg of baclofen per day with an average dose
at 147 mg per day. (DeBeaurepaire, 2012, p.3). In his study, Dr DeBeaurepaire
admitted that “there was a significant relationship between the amount of alcohol (in
grams) consumed before treatment and the maximal dose of baclofen needed by
patients”. (DeBeaurepaire, 2012, p. 3) Dr DeBeaurepaire concluded:
Ninety-two patients (92%) reported a decrease in their motivation to drink at one time or another during the follow-up. At baseline, all patients belonged to the WHO “at high risk” category. At 3 months, 50% of the responses were classified as “at low risk,” 34% “at medium risk,” and 16% “at high risk”; at 6 months, the percentages were respectively 52, 18, and 27%, they were 48, 15, and 29% at 1 year, and 50, 12, and 25 at 2 years. (DeBeaurepaire, 2012, p. 3)
All patients entering the study were for “treatment resistant alcoholism”, meaning that
“all patients have been treated before for their alcoholism, in various ways, including
medications, hospitalizations, rehab centers, Alcoholics Anonymous, and
psychotherapies, and that these treatments failed.” (DeBeaurepaire, 2012, p. 2)
Even though this clinical trial was the first undertaken at a larger scale, the
sample size issue remains since this was a dose ranging study, or considered a Phase
II trial by the US FDA. In addition, to ensure that appropriate statistical and clinical
significance could be determined, more participants in each group would have been
optimal to move this conclusion forward.
This clinical trial was reviewed by Dr Addolorato, lead investigator in both the
2002 and the 2007 Italian trials. In fact, Dr Giovanni Addolorato, besides being a
Editor of "Frontiers in Addictive Disorders", where Dr DeBeaurepaire’s paper got
published in 2012. (Professor Giovanni Addolorato, n.d.)
Australian Trial
Another study exploring the use of Baclofen in the treatment of AUD was led by
the Australian investigator, Dr. Morley from the NHMRC Centre of Research Excellence
in Mental Health and Substance Use, Discipline of Addiction Medicine of the University
of Sydney in Australia. (Morley, et al, 2014) The study’s aim was “To conduct a
double-blind, placebo-controlled randomized clinical trial of baclofen in the treatment of alcohol
dependence.” (Morley, et al, 2014, p. 654) Sixty-nine individuals were referred to the
study, with a total of 42 patients randomized to one of three arms: Baclofen 30 mg/day
(n=14); Baclofen 60 mg/day (n=14); Placebo (n=14). Study participants were followed
for twelve consecutive weeks. “Randomized participants received upward and
downward titrations of medicine … to reduce the likelihood of side effects.” (Morley, et al,
2014, p. 655-656) The team’s findings were stated as follows:
Intention-to-treat analyses revealed that alcohol consumption (heavy drinking days, drinks per drinking day) significantly reduced across all three groups during the treatment period. … A post hoc analysis stratifying according to whether there had been a comorbid anxiety disorder, revealed a beneficial effect of baclofen 30 mg/day versus placebo on time to lapse and relapse (P < 0.05). There was also a beneficial effect for baclofen 60 mg/day relative to placebo on time to relapse in this comorbid group (P < 0.05). (Morley, et al, 2014, p.654)
Even though this clinical trial might confirm a positive trend observed in prior
trials, the "post hoc" analysis was not planned and Morely et al concluded “In spite of
the small sample for a 3-arm clinical trial, this study suggests a specific role of baclofen
in alcohol-dependent individuals with comorbid anxiety. Replication in larger,
lasted twelve weeks, which is under the “grace period” of three months defined by a
2006 FDA report cited in Dr DeBeaurepaire’s paper, where the grace period “is an early
period in a trial where outcome is not considered in the analysis because the effect of
the treatment during this period does not represent the full potential of the drug”. (as
cited in DeBeaurepaire, 2012) As a reminder, Dr DeBeaurepaire’s trial lasted 24 months.
(DeBeaurepaire, 2012) Further, it is interesting to notice that Drs Addolorato, Leggio,
and Haber, from the Italian RCT in 2007, were also involved in this Australian trial.
Comparison of costs of drugs in the United States
One can make a case for the support of Baclofen over other drugs for the
treatment of AUD in the US from a consumer purchase perspective. The following table
shows how Baclofen is less than the daily cost associated with any other treatment for
AUD on the American market.
Drug’s name Maintenance
recommended dosages
Daily cost* – generic drug
Daily cost* – brand’s name
drug
Acamprosate*2 666 mg, 3 times per day $8.40 $10.16
Baclofen:
FDA guidelines 40 mg / day $0.53 N/A
Dr Garbutt’s new
American trial 90 mg / day $1.20 Dr. DeBeaurepaire 2014
French trial 300 mg / day $4.00
Disulfiram *2
500 mg per day $5.90 $10.65
Ezogabine
200 mg, 3 times per day N/A $30.92
Gabapentin
300 mg, 3 times per day $0.96 $10.47
Naltrexone *2
50 mg per day $3.80 $ 3.53
quoted as of 02/10/2015, in the zip code 27514 (Chapel Hill, NC). (Prices, Coupons and Information – GoodRx, n.d.)
*2 Denotes that the drug is approved by the FDA in the treatment of AUD.
As seen above, the generic drug Baclofen is currently five times less expensive than its
main competitor Disulfiram in its generic form. Based on the fact that Baclofen exists in
a generic form, I have assumed that prices would not rise disproportionally after the
drug’s FDA approval. I propose that approval of Baclofen for AUD would also relieve
insurance companies from large claims resulting from the treatment of addictions.
Instead, insurance companies would see a rise in claims in the near future but these
would be less expensive claims related to prescriptions for the use of Baclofen in the
treatment of AUD.
Creating a coalition
Another consideration should be brought to light: the creation of a coalition
among investigators who research AUD treatments. In fact, by joining forces,
investigators could develop a master protocol with calculated sample sizes for a
multi-center RCT to demonstrate efficacy of the drug being tested. Such coalition was once
proposed by Dr Addolorato when he “originally planned as a multisite double-blind
placebo-controlled randomized clinical trial to assess the effects of two doses of
baclofen (30 mg/day, 60 mg day and placebo) in alcoholism.” (Morley et al, 2014) The
name of this alliance was the International Baclofen Intervention Study (IBIS) as
illustrated in Figure 12. (Morley et al, 2014) Unfortunately, this international effort did not
succeed as expected and only half of the participating countries ended up collecting
data, rendering the study “significantly underpowered”. (Morley et al, 2014)
Source: Addolorato, 2007
The principle of beneficence
Converging evidence suggests that the drug Baclofen fulfills its ambition to stop
AUD patients’ cravings and promote sobriety, as detailed in the studies discussed. I am
of the opinion that it is a safe drug that patients with liver issues can take without an
established risk to their liver, as opposed to the Disulfiram and other FDA approved
drugs. Low dose Baclofen is also safe for patients to take while intending to reduce their
intake of alcohol without formally quitting drinking. (Agabio & Colombo, 2014) Also, “to
date, baclofen has not displayed addictive properties in patients affected by AUD.”
(Agabio & Colombo, 2014) It should be noted that every patient is different and should
be treated as such. Regardless of the known tolerance of the patient to a drug, patients
taking HDB should be medically supervised to address the potentially dangerous
side-effects that can arise from overdoses. In fact, the DSM-5 model (Appendix 1) shows
terms of alcohol abuse, a different dosage would be prescribed. A concomitance of
other medications should be considered in the case of AUD and dual-diagnosis. Also, it
is widely known that alcoholism is first and foremost a health behavioral issue that
should be followed by a psychiatrist and a support group in order to make the success
of Baclofen as treatment for AUD attainable. The psychiatrist should keep the patient
under observation for the time required to reach an optimal maintenance dose of
Baclofen. Recent trials included the BRENDA program, a psychiatric support designed
to help individuals in their recovery. (Starosta et al, 2006) At last, the most important
component in the success of the drug itself is the desire of the patient to actually quit.
Without this ambitious goal and the adherence to the program, I believe that no
prescription drug can make a patient quit his or her drug of choice.
Any drug prescribed in the treatment of AUD will face some obstacles to its
success. “A reduced efficacy of baclofen may also theoretically be related to a number
of other factors (i.e., genes, environment, motivation, enduring habits, severity of
alcohol dependence, severity of side-effects, treatment observance), which remain to be
References
Addolorato, G., Caputo, F., Capristo, E., Domenicali, M., Bernardi, M., Janiri, L., ... Gasbarrini, G. (2002). Baclofen efficacy in reducing alcohol craving and intake: A preliminary double-blind randomized controlled study. Retrieved February 12, 2015, from http://www.ncbi.nlm.nih.gov/pubmed/12217947
Addolorato, G., Leggio, L., & Ferrulli, A. (2007). Effectiveness and safety of baclofen for maintenance of alcohol abstinence in alcohol-dependent patients with liver
cirrhosis: Randomised, double-blind controlled study. Retrieved February 6, 2015, from http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(07)61814-5/abstract
Addolorato, G. (2007). Nuove frontiere nella terapia dell’abuso alcolico. Retrieved March 27, 2015, from
http://www.paradigmenwandel.org/Links_files/Addolorato2007.pdf
Agabio, R., & Colombo, G. (2014). GABAB receptor ligands for the treatment of alcohol use disorder: Preclinical and clinical evidence. Retrieved March 24, 2015, from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047789/
Alcoholism 'cured' By Baclofen - Spinal Cord Injury Health Issues. (n.d.). Retrieved February 11, 2015, from http://www.apparelyzed.com/forums/topic/10859-alcoholism-cured-by-baclofen/
Alcohol Alert. (1997). Retrieved March 25, 2015, from http://pubs.niaaa.nih.gov/publications/aa35.htm
Alcohol Facts and Statistics. (2014). Retrieved February 5, 2015, from
http://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/alcohol-facts-and-statistics
Alcohol Use Disorder: A Comparison Between DSM–IV and DSM–5. (2013). Retrieved February 6, 2015, from
http://pubs.niaaa.nih.gov/publications/dsmfactsheet/dsmfact.htm
Altounian, V. (2014). Effects of Alcohol on the Brain. Retrieved March 4, 2015, from https://vimeo.com/61477736
Ameisen, O. (2004). Complete and Prolonged Suppression of Symptoms and
Consequences of Alcohol-Dependence Using High-Dose Baclofen: A Self-Case Report of a Physician. Retrieved April 6, 2015, from
http://alcalc.oxfordjournals.org/content/alcalc/40/2/147.full.pdf
A-Team Alcohol Services (n.d.). Retrieved March 23, 2015, from