ARTICLE
Low Serum Immunoglobulin G
2
Levels in Infancy
Can Be Transient
Adelle R. Atkinson, MD, Chaim M. Roifman, MD
Division of Immunology and Allergy, Canadian Centre for Primary Immunodeficiency, Jeffrey Modell Research Laboratory for the diagnosis of Primary Immunodeficiency, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.The immunoglobulin G2 subclasses contain predominantly
antipolysac-charide antibodies. It was therefore believed intuitively that low immunoglobulin G2 levels could predispose individuals to infections with encapsulated bacteria.
Although many reports initially supported this notion, more recent studies chal-lenged it. Regardless of the biological significance, the natural history of low immunoglobulin G2levels has not been carefully studied.
METHODS.We studied the outcome of low serum immunoglobulin G2subclass levels
in children. Thirteen patients who were referred because of recurrent infections were found to have low immunoglobulin G2 levels. Laboratory evaluation at
presentation and follow-up visits included total serum immunoglobulins, immu-noglobulin subclasses, and specific antibodies to protein antigens and to pneumo-coccal vaccine.
RESULTS.Low immunoglobulin G2levels resolved completely within 0.6 years to 6
years (median: 1.5 years) in all patients. All 13 patients responded adequately to vaccination with protein antigens such as tetanus toxoid and polio as well as to immunization with pneumococcal vaccine. Four of 13 patients had a previous history of transient hypogammaglobulinemia, raising the possibility that the other cases may simply represent the tail end of this condition.
CONCLUSION.We have demonstrated that low immunoglobulin G2detected in early
infancy and childhood is likely to resolve completely within several months and up to 6 years from the time of presentation.
www.pediatrics.org/cgi/doi/10.1542/ peds.2006-3613
doi:10.1542/peds.2006-3613
Key Words
primary immunodeficiency, immunoglobulin IgG subclasses, childhood, infections
Abbreviations IgG—immunoglobulin G IgA—immunoglobulin A IgM—immunoglobulin M PCP—pneumococcal capsular polysaccharide
Accepted for publication Mar 22, 2007
Address correspondence to Chaim M. Roifman, MD, Division of Immunology/Allergy and Infection, Immunity, Injury and Repair Program, Hospital for Sick Children, 555 University Ave, Toronto, Ontario, Canada M5G 1X8. E-mail: [email protected]
I
MMUNOGLOBULIN G (IGG) comprises 4 distinct sub-classes that differ in structure and function.1,2IgG1is
better than IgG2and IgG3in fixing complement by the
classical pathway, whereas IgG4does not bind C1q and
therefore does not fix complement. IgG1 and IgG3also
bind Fc receptors at higher affinity than IgG2or IgG4.1–9
Antibodies to protein antigen are predominantly in the IgG1and IgG3subclasses, whereas antibodies to
poly-saccharide antigens are mostly of the IgG2 subclass.3,4
Unfortunately, IgG2antibodies are the least efficient in
crossing the placenta to the disadvantage of the new-born.5,6This disadvantage continues because production
of IgG2 is sluggish, reaching adult levels only during
adolescence, whereas IgG1levels reach adult levels at 3
to 4 years of age.7–10 Acquisition of antipolysaccharide
antibodies is also inefficient in the first 2 to 3 years of life. Beyond these physiologic variations, low levels of IgG2 with or without low IgG4 and in the presence or
absence of immunoglobulin A (IgA) deficiency have been linked to repeated infections.1,2 Patients with low
IgG2have been initially reported to have infections with
organisms such asStreptococcus pneumoniae,Haemophilus influenzae, and other encapsulated bacteria.11–14Some of
these patients were also reported to have impaired re-sponses to polysaccharide antigens.15,16However,
subse-quent studies went on to identify asymptomatic individ-uals who had reduced IgG2 but normal responses to
vaccines that contained polysaccharide antigens.17
Fur-thermore, there have been descriptions of patients who experienced recurrent bacterial infections and had a re-duced ability to produce antipolysaccharide antibodies despite normal IgG subclasses.18,19Thus, the significance
of low IgG2 levels in children and its natural history
remain unclear.20
We previously reported that low IgG2levels may
fol-low the resolution of total IgG levels in a patient with transient hypogammaglobulinemia. IgG2 levels in this
patient subsequently normalized.21Here we followed the
outcome of patients with low IgG2levels in the face of
normal total IgG levels. We found that all cases that were diagnosed in infancy or early childhood with low IgG2
levels eventually resolved.
METHODS
Patients
All patients who were referred to the immunology clinic at the Hospital for Sick Children for evaluation between 1987 and 2005 were considered. Patients with normal quantitative IgG and below-normal IgG2in the presence
or absence of low IgG4 subclass were included in the
study when they were available for appropriate follow-up. Patients with a diagnosis of a well-defined primary immunodeficiency such as chronic mucocutaneous can-didiasis, combined immunodeficiency, Wiskott Aldrich
syndrome, or ataxia telangiectasia were excluded from the evaluation.
The following was collected on patients who met the inclusion criteria: gender; age at presentation; reason for first referral; duration of follow-up; and serum IgG, IgA, and immunoglobulin M (IgM) and IgG subclasses at presentations and at each subsequent visit. Titers to po-lio, tetanus, measles, mumps, and rubella were deter-mined at presentation and periodically thereafter. Re-sponses to pneumococcal vaccine were also measured. The study protocol was approved by the Hospital for Sick Children Research Ethics Board.
Lymphocyte Markers and T Cell Proliferative Responses The surface phenotypes of blood mononuclear cells ob-tained by Ficoll-Hypaque density gradient centrifugation were determined by direct immunofluorescence with fluorescein isothiocyanate– conjugated goat anti-human immunoglobulin antibody (Tago, Burlingame, CA) or fluorescein isothiocyanate– conjugated monoclonal anti-bodies anti-CD3, CD4, CD8, CD20, and CD56 (Coulter Instruments, Mississauga, Ontario, Canada). Analysis was performed on a Coulter EPICS V flow cytometer. Lymphocyte proliferative responses to mitogens includ-ing phytohemagglutinin were determined by tritiated thymidine incorporation using the microtiter plate tech-nique. All assays were performed in triplicate and were compared with those simultaneously performed on nor-mal controls.22
Serum concentration of Immunoglobulins and IgG Subclasses Serum concentrations of immunoglobulins were mea-sured by nephelometry. Quantification of IgG subclasses was done by using the BINDARIO kit (The Binding Site Ltd, Birmingham, United Kingdom). The kit is based on single radial immunodiffusion methods that were de-rived from the work of Fahey et al23and Mancini et al.24
In short, the method detects a protein diffusing radially from a cylindrical well through an agarose gel that con-tains the appropriate antibody. The resulting immune complexes form a precipitin ring. Once the ring size reaches equilibrium, a linear relationship exists between the square of the ring diameter and the concentration of the IgG subclass. The concentration of an IgG subclass in an unknown sample may be determined by measure-ment of the ring diameter and reading off the calibration curve. Normal range was determined according to eval-uation of 40 to 50 normal infants and children for each age group: 0 to 2 years, 2 to 4 years, 4 to 6 years, 6 to 8 years, 8 to 10 years, 10 to 12 years, 12 to 14 years, and 14 to 18 years. Mean and SDs were determined using least-squares regression analysis.23,24
Determination of Specific Antibodies
immu-nosorbent assay (Vacczyme anti–tetanus toxoid IgG en-zyme immunoassay kit, Euroimmune Mumps EIA kit, Euroimmune Measles kit, and Euroimmune rubella kit; Euroimmune, Gross-Groenau, Germany). Polio anti-body titers were determined by complement fixation according to the manufacturer’s instructions and as pre-viously described.21,22 Antipneumococcal antibodies
were assessed using 2 kits, according to the manufac-turer’s instructions. Anti–pneumococcal capsular poly-saccharide (PCP) IgG enzyme immunoassay kit and anti-PCP IgG2enzyme immunoassay kit both were
man-ufactured by The Binding Site Ltd. The assays are de-signed for the in vitro measurement of specific IgG antibodies against PCP present in human serum. The kits are designed to measure antibody responses to pneumo-coccal vaccines incorporating 23 polysaccharides that are isolated fromStreptococcus pneumonia.25The PCP antigens
used include 1 to 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19F, 19A, 20, 22F, 23F, and 33F accord-ing to Danish nomenclatures.
In short, the principle of assay includes microdisks precoated with PCP antigens. Calibrators, controls, and diluted patient samples are added to the wells, and an-tibodies that recognize the PCP antigens are allowed to bind during the incubation. Purified peroxidase sheep-labeled anti-human IgG or IgG2conjugate is added. The
bound conjugate is visualized with tetramethylbenzidine substrate, which gives a blue reaction.
RESULTS
Patients
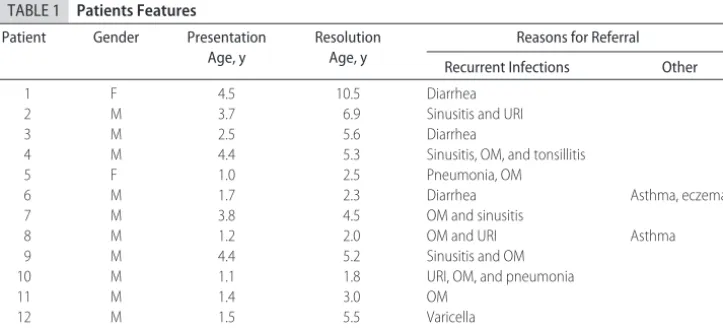
Thirteen patients who met the study inclusion criteria were 1.0 to 4.5 years of age at presentation (mean: 4 years; median: 3.7 years) and were followed for a period that ranged from 0.6 to 6.0 years (mean: 2.5 years; median: 1.5 years; Table 1).
Clinical Features
Patients were referred to the immunology clinic because of repeated infections (Table 1). Most common, recur-rent otitis media (7 patients) and repeated upper respi-ratory infections (4 patients) were reported. Two pa-tients had ⬎1 episode of pneumonia, 3 patients had a history compatible with recurrent sinusitis, and 4 were referred because of recurrent diarrhea. One patient pre-sented with recurrent varicella infections. In addition to the history of infections, 2 patients had asthma and 1 of them also had eczema. During follow-up, no major in-vasive infection was registered in the patients. Specifi-cally, no episodes of pneumonia, acute sinusitis, ab-scesses, or meningitis were recorded. However, normal frequency of upper respiratory infection or otitis media were reported in 5 patients during the follow-up period. In addition, patient 4 continued to have repeated epi-sodes of sinusitis even after IgG2levels normalized. He
experienced 3 episodes in a period of 4.5 years of follow-up.
Evaluation of the Immune System
Serum IgG and IgM levels were normal in all studied patients. IgA levels that were below normal but still detectable were found in 1 of 13 patients at presentation. Specific antibody response to tetanus vaccine was normal in 12 of 13 patients tested at presentation. The remaining patients responded normally after reimmuni-zation. Responses to polio vaccine were also normal in all patients. Isohemagglutinin levels when examined at the age of 2 years or older were also normal in 12 of 13 patients (1 patient had an AB blood group). Responses to vaccination with Pneumovax was also normal in all 13 patients.
Four patients had additional laboratory evaluation, including lymphocyte markers as well as in vitro re-sponses to mitogens and antigens. All 4 patients had normal markers and mitogenic responses.
TABLE 1 Patients Features
Patient Gender Presentation
Age, y
Resolution Age, y
Reasons for Referral
Recurrent Infections Other
1 F 4.5 10.5 Diarrhea
2 M 3.7 6.9 Sinusitis and URI
3 M 2.5 5.6 Diarrhea
4 M 4.4 5.3 Sinusitis, OM, and tonsillitis
5 F 1.0 2.5 Pneumonia, OM
6 M 1.7 2.3 Diarrhea Asthma, eczema
7 M 3.8 4.5 OM and sinusitis
8 M 1.2 2.0 OM and URI Asthma
9 M 4.4 5.2 Sinusitis and OM
10 M 1.1 1.8 URI, OM, and pneumonia
11 M 1.4 3.0 OM
12 M 1.5 5.5 Varicella
13 M 2.8 8.0 URI
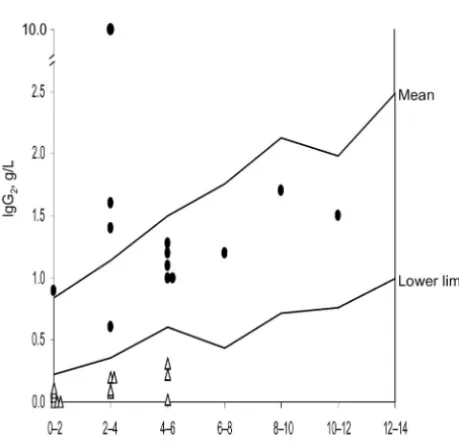
IgG Subclasses
All patients had low IgG2level, and 3 also had a reduced
IgG4 level. For the purpose of this study, only patients
with extremely low IgG2 levels were included. All
pa-tients had IgG2levels⬍95th percentile range (Fig 1); 3 of
13 had undetectable IgG2levels at presentation.
Within 0.6 years to 6.0 years (mean: 2.24 years; me-dian: 1.5 years), IgG2 levels returned to the reference
range in all 13 patients who were available for follow-up (Fig 1). All 3 patients who had low IgG4 levels also
normalized by the end of follow-up.
Transient Hypogammaglobulinemia and Low IgG2Levels
Three of 13 patients had a history of transient hypo-gammaglobulinemia. Although IgG levels normalized, the IgG2fraction remained low for a period that ranged
from 1.0 to 4.5 years. This finding raises the possibility that the other patients with low IgG2in our study may
have gone through a similar course.
DISCUSSION
We studied here the outcome of low IgG2in 13 infants
and children. The pathogenesis of “IgG2deficiency”
re-mains unknown. A delay in IgG2production in infants
seems physiologic, because IgG1 but not IgG2 reaches
near adult normal levels by 3 to 4 years of age.7–10It is
possible that in the cases reported here, there may be an exaggeration of this physiologic process.
Alternatively, the low IgG2levels observed in these
patients may be part of and perhaps the end of transient hypogammaglobulinemia. Thus, despite normalizing
to-tal IgG levels, IgG2subclass levels remain low for a while
until they reach normal values.21 Indeed, 3 patients in
this series had a history of transient hypogammaglobu-linemia. It is conceivable that in the rest of the patients, transient low IgG levels may have been missed before the identification of IgG2 subclass deficiency. Such a
scenario is plausible because both transient hypogam-maglobulinemia and low IgG2subclass levels have been
detected in asymptomatic individuals.17
Throughout the 1980s, a variety of publications cited the association of low subclasses with recurrent sino-pulmonary infections.11–16 The link was based on the
assumption that reduced IgG2, which contains
predom-inantly polysaccharide antibodies,1,2 should intuitively
be associated with an increased susceptibility to infection caused by encapsulated bacteria. Subsequent studies se-verely challenged this theory. First, asymptomatic chil-dren with low IgG2levels were found to have normal
responses to polysaccharide antigens after vaccination.17
Furthermore, children who have some inability to pro-duce antipolysaccharide antibody have been found to have normal serum levels of IgG2in isolation18,19or as a
feature of Wiskott-Aldrich syndrome.26 Finally,
heavy-chain deletion of various IgG subclasses was identified in asymptomatic individuals.27,28 Together, these findings
question the causative link between IgG2deficiency and
susceptibility to infections.
Patients in this study were referred to us because of a history of recurrent infection. Assessment of responses to polysaccharide antigens was limited to children who were older than 2.5 years because studies in younger children are inconsistent and lack reliability. Evaluation that was performed in patients who were older than 2.5 years at presentation or later during follow-up showed normal responses to unconjugated polyvalent pneumo-coccal vaccine. These results are consistent with the observation that during follow-up, patients did not re-port severe invasive infections. One patient continued to have repeated episodes of sinusitis after IgG2normalized,
suggesting that infections in these patients may not have been related to the level of serum IgG2 subclass. It is
possible that these patients had a history of infections because of a previous condition of transient hypogam-maglobulinemia, or, alternatively, the clinical history was part of a normal pattern of infections in this age group.
CONCLUSIONS
This unique follow-up of patients with low IgG2subclass
levels demonstrates that this phenomenon could be transient and is therefore of limited biological signifi-cance. In most cases, it may reflect an exaggeration of an already existing maturational delay in producing IgG2
subclass, possibly as the last stage in resolution of tran-sient hypogammaglobulinemia.
FIGURE 1
ACKNOWLEDGMENTS
This work was supported by the Canadian Immunode-ficiency Society, the Jeffrey Modell Foundation, and the Donald and Audrey Campbell Chair in Immunology.
We thank Ms Rena Roifman for collecting the data.
REFERENCES
1. Natvig JB, Kunkel HG. Human immunoglobulins: classes, sub-classes, genetic variants, and idiotypes.Adv Immunol.1973;16: 1–59
2. Morell A, Terry WD, Waldmann TA. Metabolic properties of IgG subclasses in man.J Clin Invest.1970;49:673– 680 3. Ferrante A, Beard LJ, Feldman RG. IgG subclass distribution of
antibodies to bacterial and viral antigens. Pediatr Infect Dis J.
1990;9(suppl):S16 –S24
4. Insel RA, Anderson PW. IgG subclass distribution of antibody induced by immunization with the isolated and protein conju-gated polysaccharide of H. influenzae b and G2m(n) distribu-tion of serum IgG2 in man.Monogr Allergy.1988;23:128 –137 5. Mellbye OJ, Natvig JB. Presence and origin of human IgG
subclass proteins in newborns.Vox Sang.1973;24:206 –215 6. Einhorn MS, Grranoff DM, Nahm MH, Quinn A, Shackelford
PG. Concentrations of antibodies in paired maternal and infant sera: relationship to IgG subclasses. J Pediatr. 1987;111: 783–788
7. Schur PH, Rosen F, Norman ME. Immunoglobulin subclasses in normal children.Pediatr Res.1979;13:181–183
8. French M. Serum IgG subclasses in normal adults. Monogr Allergy.1986;19:100 –107
9. Morell A, Skvaril F, Hitzig WH, Barandun S. IgG subclasses development of the serum concentrations in “normal” infants and children.J Pediatr.1972;80:960 –964
10. Plebani A, Ugazio AG, Avanzini MA, et al. Serum IgG subclass concentrations in healthy subjects at different age: age normal percentile charts.Eur J Pediatr.1989;149:164 –167
11. Schur PH, Borel H, Gelfand EW, Alper CA, Rosen FS. Selective gamma-g globulin deficiencies in patients with recurrent pyo-genic infections.N Engl J Med.1970;283:631– 634
12. Oxelius VA, Laurell AB, Lindquist B, et al. IgG subclasses in selective IgA deficiency: importance of IgG2-IgA deficiency.
N Engl J Med.1981;304:1476 –1477
13. Bass JL, Nuss R, Mehta KA, Morganelli P, Bennett L. Recurrent meningococcemia associated with IgG2-subclass deficiency.
N Engl J Med.1983;309:430
14. Shackelford PG, Granoff DM, Polmar SH, et al. Subnormal serum concentrations of IgG2 in children with frequent infec-tions associated with varied patterns of immunologic dysfunc-tion.J Pediatr.1990;116:529 –538
15. Oxelius VA. Chronic infections in a family with hereditary deficiency of IgG2 and IgG4.Clin Exp Immunol.1974;17:19 –27 16. Umetsu DT, Ambrosino DM, Quinti I, Siber GR, Geha RS. Recurrent sinopulmonary infection and impaired antibody re-sponse to bacterial capsular polysaccharide antigen in children with selective IgG-subclass deficiency.N Engl J Med.1985;313: 1247–1251
17. Shackelford PG, Granoff DM, Madassery JV, Scott MG, Nahm MH. Clinical and immunologic characteristics of healthy chil-dren with subnormal serum concentrations of IgG2.Pediatr Res.
1990;27:16 –21
18. Ambrosino DM, Siber GR, Chilmonczyk BA, Jernberg JB, Fin-berg RW. An immunodeficiency characterized by impaired antibody responses to polysaccharides.N Engl J Med.1987;316: 790 –793
19. Ambrosino DM, Umetsu DT, Siber GR, et al. Selective defect in the antibody response to Haemophilus influenzae type b in children with recurrent infections and normal IgG subclass levels.J Allergy Clin Immunol.1988;81:1175–1179
20. Buckley RH. Immunoglobulin G subclass deficiency: fact or fancy?Curr Allergy Asthma Rep.2002;2:356 –360
21. Dalal I, Reid B, Nisbet-Brown E, Roifman CM. The outcome of patients with hypogammaglobulinemia in infancy and early childhood.J Pediatr.1998;133:144 –146
22. Arpaia E, Shahar M, Dadi H, Cohen A, Roifman CM. Defective T cell receptor signaling and CD8⫹thymic selection in humans lacking Zap-70 kinase.Cell.1994;76:947–958
23. Fahey JL, McKelvey EM. Quantitative determination of serum immunoglobulins in antibody-agar plates.J Immunol.1965;94: 84 –90
24. Mancini G, Vaerman JP, Carbonara AO, Heremans JF. A single radial diffusion method for the immunological quantitation of proteins. In: Peeters H, ed. XI Colloquium on Protides of the Biological Fluids.Amsterdam, Netherlands: Elsevier Publishing Co; 1964:370 –373
25. Schauer U, Stemberg F, Rieger CH, et al. Levels of antibody specific to tetanus toxoid, Haemophilus influenzae type b, and pneumococcal capsular polysaccharide in healthy children and adults.Clin Diagn Lab Immunol.2003;10:202–207
26. Nahm MH, Blaese RM, Crain MJ, Briles DE. Patients with Wiskott-Aldrich syndrome have normal IgG2 levels.J Immunol.
1986;137:3484 –3487
DOI: 10.1542/peds.2006-3613 originally published online August 6, 2007;
2007;120;e543
Pediatrics
Adelle R. Atkinson and Chaim M. Roifman
Levels in Infancy Can Be Transient
2
Low Serum Immunoglobulin G
Services
Updated Information &
http://pediatrics.aappublications.org/content/120/3/e543
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/120/3/e543#BIBL
This article cites 27 articles, 2 of which you can access for free at:
Subspecialty Collections
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2006-3613 originally published online August 6, 2007;
2007;120;e543
Pediatrics
Adelle R. Atkinson and Chaim M. Roifman
Levels in Infancy Can Be Transient
2
Low Serum Immunoglobulin G
http://pediatrics.aappublications.org/content/120/3/e543
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.