Apparent Diffusion Coefficient in the Posterior Limb of the Internal
Capsule Predicts Outcome After Perinatal Asphyxia
Rod W. Hunt, FRACP*; Jeffrey J. Neil, MD, PhD‡; Lee T. Coleman, FRANZCR§; Michael J. Kean, Dip App Sci§; and Terrie E. Inder, MD*
ABSTRACT. Objective. Predicting long-term outcome in infants with hypoxic-ischemic encephalopathy (HIE) is a difficult task. Magnetic resonance imaging, particu-larly diffusion imaging, holds promise in this regard as it is more sensitive to brain injury than any other available imaging modality. Previous studies have suggested that abnormal signal intensity in the posterior limb of the internal capsule (PLIC), detectable on inversion-recovery T1-weighted imaging, is a strong predictor of outcome. The aim of this study was to assess the relationship between apparent diffusion coefficient (ADC) values from the PLIC, measured by diffusion imaging, and neu-romotor outcome in term infants with HIE.
Methods. Twenty-eight term infants with a clinical diagnosis of HIE underwent magnetic resonance imaging as soon as practicable after birth (mean age: 5.6 days), including diffusion-weighted imaging, from which ADC values in the PLIC were measured. Motor outcome was assessed in 12 of 16 survivors.
Results. The ADC value in the PLIC was significantly associated with survival in term infants with HIE. For survivors, the mean ADC value in the PLIC was 0.89ⴞ 0.17m2/ms, whereas the mean ADC value for nonsur-vivors was 0.75ⴞ0.17m2/ms (tⴝ2.25). Among survi-vors, the ADC value in the PLIC was also associated with neuromotor outcome (Fⴝ5.60).
Conclusion. The ADC value in the PLIC is an indica-tor of ischemic injury and may be of use as an objective prognostic marker for infants with HIE.Pediatrics2004; 114:999–1003;apparent diffusion coefficient, perinatal as-phyxia, magnetic resonance imaging.
ABBREVIATIONS. MRI, magnetic resonance imaging; HIE, hy-poxic-ischemic encephalopathy; PLIC, posterior limb of internal capsule; DWI, diffusion weighted imaging; ADC, apparent diffu-sion coefficient.
M
agnetic resonance imaging (MRI) isestab-lished as the most useful neuroimaging mo-dality in assessing the extent of neurologic injury in term infants with hypoxic-ischemic
enceph-alopathy (HIE).1,2 The patterns of cerebral ischemic
injury on conventional MRI in the term encephalo-pathic infant have been described and linked with both the type of ischemic insult3 and later
impair-ments in neurologic outcome.4 The prediction of
long-term neurodevelopmental outcome in these in-fants, particularly for those with moderate disease,5
remains problematic. Early studies focused on con-ventional MRI for detection of injury within the first 10 days after an ischemic insult,6and these changes
were correlated with neonatal neurologic examina-tion4 and later childhood neurodevelopmental
out-comes.7 More recently, changes in the signal in the
posterior limb of the internal capsule (PLIC), de-tected by T1-weighted inversion-recovery imaging, have been found to be highly predictive of poor neurodevelopmental outcome after an asphyxial in-sult in the term infant.8
One of the limitations of conventional MRI in eval-uating the term encephalopathic infant is the delay of 5 to 7 days for abnormalities to become reliably apparent on conventional T1- and T2-weighted im-aging after an ischemic insult. In contrast to this delay, other MR techniques, such as MR spectrosco-py9and diffusion-weighted imaging (DWI), provide
a means for the earlier detection of injury.10 For
example, DWI detects ischemic changes within 24 hours of an ischemic insult in the term newborn brain.9,11–13 The explanation for the differences
be-tween conventional MRI and DWI for detection of injury may lie in fundamental differences in the source of image contrast between the 2 methods. For conventional MR images, contrast derives from dif-ferences in water MR relaxation properties (ie, T1 and T2 relaxation time constants for the1H nuclei of
water in different brain areas), whereas for DWI, the contrast is based on differences in the translational motion of water molecules. This motion can be de-scribed quantitatively as a water apparent diffusion coefficient (ADC). Water ADC values decrease within minutes after a variety of central nervous system insults, including stroke, HIE, seizure, and excitotoxic injury. In addition, water diffusion within the brain is dependent on both maturation and re-gion14 in infants, with normative data documented
from infants of 38 to 42 weeks’ gestation.15,16
In this study, ADC values from the PLIC were evaluated. Because it has been reported that qualita-tive changes in water T1 relaxation properties of the PLIC are predictive of neuromotor outcome in
in-From the *Department of Neonatal Neurology, Royal Children’s and Royal Women’s Hospitals, Murdoch Children’s Research Institute, University of Melbourne, Melbourne, Australia; ‡Paediatric Neurology, St Louis Chil-dren’s Hospital, St Louis, Missouri; and §Department of Medical Imaging, Royal Children’s Hospital, Melbourne, Australia.
Accepted for publication Feb 17, 2004. doi:10.1542/peds.2003-0935-L
Reprint requests to (T.E.I.) Department of Neonatal Neurology, Level 2, Royal Children’s Hospital, Flemington Road, Parkville, VIC 3052, Australia. E-mail: [email protected]
fants with HIE,8we sought to determine whether the
more quantitative measure of water ADC is also predictive.
METHODS Subjects
From January 2001 to September 2002, infants who were ad-mitted to the Women’s and Children’s Health Network in Mel-bourne with a clinical diagnosis of HIE were considered for this observational study. The clinical diagnosis of HIE was made on the grounds of clinical encephalopathy and evidence of perinatal compromise, with or without a sentinel hypoxic event. Perinatal compromise was defined as fetal distress detected by cardiotoco-graph, Apgar score⬍6 at 5 minutes, and fetal or neonatal aci-demia (base excess⬎12 mmol/L). The severity of the encephalop-athy was staged according to Sarnat criteria.5Perinatal data were
collected from the mothers’ and infants’ medical records. All subjects were followed up in a dedicated neonatal neurol-ogy outpatient clinic by 2 of the investigators (T.E.I. and R.W.H.). Outcomes were classified as survival or death. Survivors were assessed for severity of developmental disability. Disability was defined as mild (abnormal neuromotor tone), moderate (hemipa-resis or dipa(hemipa-resis), or severe (spastic quadripa(hemipa-resis).
Image Acquisition
Infants with HIE were underwent MRI as soon as practicable after birth, at a time determined by the treating physician as a standard of clinical care. The images were obtained with a 1.5-Tesla General Electric LX Echospeed system (version 9.0). Trans-verse T1 fast spin echo (TR/TE 1400/10, ETL 2, BW⫾20 kHz, FOV 20 cm, slice thickness 3.5 mm; 256⫻224 matrix, 2 averages) and transverse fast spin echo T2 (TR/TE 3600/16, ETL 18, BW⫾ 20.83 kHz, FOV 18 cm, slice thickness 3.0 mm, 256⫻224 matrix, 3 averages), epi-DWI (3 directions, b⫽1 ms/m2, TR/TE 10 000/
104, BW⫾100 kHz, FOV 25 cm, slice thickness 4.0 mm, 192⫻128 matrix, 2 averages) were obtained. Conventional images were graded on a systematic scale by 3 independent reviewers (T.E.I., L.C., and R.W.H.) for the extent of injury. The integrity of the PLIC was also assessed on conventional images as normal, impaired (being half or less of the expected signal intensity), or absent.
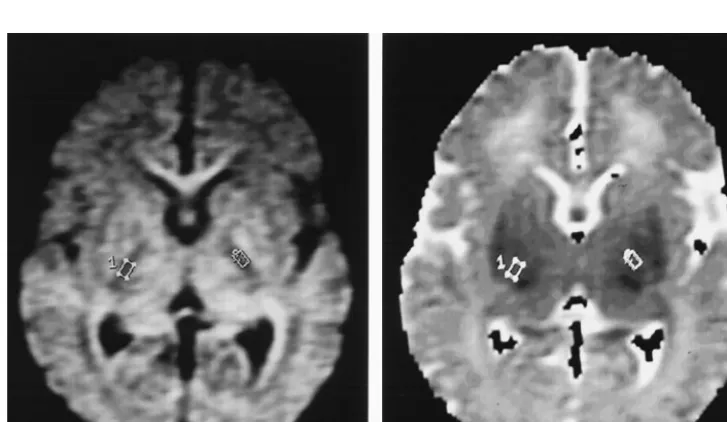
An ADC map was generated from the diffusion-weighted im-ages using Functool (ADW 3.0, GEMS). A region of interest with standardized size (15-20 mm2) was placed over the middle third of
the left and right PLIC, and the ADC values were measured (Fig 1).
Statistical Analysis
Statistics were performed using SPSS. Means were compared withttest or analysis of variance. Correlation was sought, using univariate linear regression, between the lowest ADC value from the left or right PLIC and a number of continuous perinatal variables, including Apgar scores at 1, 5, and 10 minutes and time to first breath. Univariate logistic regression was used for categor-ical variables such as need for mechancategor-ical ventilation, first pH, seizures in the perinatal period, and Sarnat staging. In addition, appearance of the PLIC on conventional MRI was correlated with neuromotor outcome.P⬍.05 was considered statistically signif-icant.
RESULTS Subject Population
During the study period, 34 infants were admitted to our unit with a diagnosis of HIE. Of these, 2 infants died before acquisition of an MRI scan, and an additional 4 infants were found to have a diagno-sis other than HIE (cerebral dysgenediagno-sis [n ⫽ 2] or established in utero injury [n ⫽2]).
Perinatal Characteristics
The remaining 28 infants had a mean birth weight of 3488 g (SD: 461 g) and median gestation of 40 weeks (range: 37– 42 weeks). Ten infants were deliv-ered by unassisted vaginal delivery, 5 by assisted vaginal delivery (1 Ventouse, 2 Neville Barnes for-ceps, and 1 midcavity rotational forceps delivery), and 13 by emergency cesarean section. The median Apgar score at 1 minute was 1 (minimum, 0; maxi-mum, 7) and at 5 minutes was 4 (minimaxi-mum, 0; max-imum, 8). The median pH at first blood gas (cord or arterial) was 7.14 (range: 6.55–7.42). Nineteen of the 28 infants had seizures in the perinatal period, and of these, 6 received only 1 anticonvulsant, 3 received 2 anticonvulsants, 8 required 3 anticonvulsants, and 2 required 4 anticonvulsants. According to Sarnat stag-ing criteria, 9 infants had stage 1 HIE, 4 had stage 2, and 15 had stage 3.
MRI Findings
Infants were scanned at a mean age of 5.6 days (range: 1–12 days; SD: 2.8 days). There was no sig-nificant difference in the time of scan for infants with stage 1, 2, or 3 HIE. Patterns of injury on MRI scan-ning were as follows: 2 infants had a normal scan, 4 infants had isolated basal ganglia injury, 3 had iso-lated white matter injury, 2 had cortical and white matter injury only, and 17 infants had evidence of injury in 3 or more anatomic structures.
Neurodevelopmental Outcome
Of these 28 infants, 16 survived and 12 died in the perinatal period. Follow-up data are currently avail-able for 12 of the 16 survivors. Three have normal outcome, 4 have mild or moderate impairment, and 5 are left with severe neuromotor impairment. The mean age at follow-up was 12.9 months (SD: 7 months).
ADC Values
There was no clear relationship between age at scan and the lowest ADC value in the PLIC among study infants. The ADC value (mean ⫾ SD) in the PLIC was significantly greater for infants who sur-vived (0.89 ⫾ 0.17 m2/ms) compared with those
who died (0.75 ⫾ 0.17 m2/ms; t ⫽ 2.25, P ⫽ .03).
When ADC values for surviving infants were ana-lyzed according to their neuromotor outcome, a sig-nificant difference was found between the groups (Fig 2). The lowest ADC values in the PLIC were significantly different between infants in relation to the pattern of injury on conventional MRI, with global injury associated with lowest ADC values (F
⫽5.53,df⫽4, P⫽.003; Fig 3).
The appearance of the right PLIC on conventional imaging was compared with both outcome and ADC values in the right PLIC. (The right PLIC was chosen
to ensure consistent comparison for this part of the analysis.) Fifteen infants had a normal PLIC, 2 had an abnormal PLIC, and 11 had an absent PLIC on con-ventional MRI. The mean ADC values for each of these groups were significantly different, reflecting some degree of consistency between subjective inter-pretation of conventional imaging and ADC values (F⫽4.65,P⬍.02; Fig 4). Appearance of the PLIC on conventional MRI was strongly associated with mo-tor outcome (F⫽6.69,df⫽2,P⫽.008). There was no significant relationship between the ADC value and any clinical perinatal variable, with the exception of Sarnat staging (F⫽5.53, df ⫽4,P ⫽.003).
A receiver operator curve was generated to deter-mine which lowest ADC value had the greatest util-ity as a predictor of survival with or without severe neurodevelopmental impairment. At a lowest ADC value of 0.74m2/ms, this parameter predicted
out-Fig 2. The lowest ADC value in the PLIC grouped according to neuromotor outcome; the line in each box represents the median value, the upper and lower bounds of each box represent the 25th and 75th quartiles, and the horizontal lines represent the maxi-mum and minimaxi-mum values.
Fig 3. The ADC value in the PLIC for the differing patterns of injury on conventional MRI; BG, basal ganglia injury; WM, white matter injury.
come with a sensitivity of 80% and a specificity of 100%. This relationship was statistically significant using the Fisher exact test (P⫽.01).
DISCUSSION
ADC in the PLIC is a quantitative assessment cor-relating with changes on conventional MRI and neu-romotor outcome. We have demonstrated that the ADC value in the PLIC, as well as the appearance of the PLIC on conventional imaging, is significantly associated with survival in a cohort of infants with HIE. In surviving infants, ADC in the PLIC is signif-icantly associated with motor outcome.
One potential confounding factor in our analysis of the relationship of the MRI findings to outcome relates to the fact that the findings on MRI are con-sidered in the decision-making process with regard to withdrawal of care. Despite this limitation, we found a significant relationship between ADC values and later neuromotor outcome in survivors. This highlights the potential importance of measuring ADC values to assist in the long-term prognosis of term infants with HIE. Our findings suggest that
infants who have an ADC in the PLIC of ⬍0.74
m2/ms and survive will be left with severe
neuro-motor impairment. This is in keeping with findings of Wolf et al.17 In their study, control subjects had
ADC values⬎1.0m2/ms in the PLIC. None of the
infants in our cohort who had severe neuromotor
impairment had an ADC value in the PLIC ⬎1.0
m2/ms. Although these findings should be
vali-dated with greater numbers and with outcome data over a longer period, their significance is encourag-ing.
Within our study, the group of infants who had HIE and remain problematic are those who subse-quently developed moderate neurodevelopmental impairment. It is important to note that our study population was skewed, with ⬎50% of the infants having severe encephalopathy (Sarnat stage 3). Thus, in relationship to the moderate neurodevelopmental impairment group, we found a wider spread of ADC values than for the other 2 groups (mean: 0.98; SD: 0.13m2/ms; see Fig 2), suggesting that ADC in the
PLIC may be less useful in clearly defining this pop-ulation. A greater sample size with a single defined time point of MRI scanning may well assist in nar-rowing the range for this group. Until the optimal time for scanning can be better defined for the mod-erate group, the value of the ADC in the PLIC may lie with the severe group, for whom a clear cutoff has been established, below which severe neuromotor outcome can be predicted.
Previous studies of ADC values in the newborn brain after HIE have demonstrated the phenomenon of pseudonormalization, in which ADC values are depressed in the first few days after injury and then recover to within the normal range toward the end of the first week.13There was no such trend observed in
the ADC values of the PLIC in our study. We pos-tulate that pseudonormalization was not observed because the axonal fiber tracts that constitute the PLIC undergo a more prolonged secondary injury as
a result of Wallerian degeneration. In the study by McKinstry et al,13 ADC values were measured in
areas of brain directly injured, rather than those un-dergoing Wallerian degeneration. The phenomenon of a reduced ADC in white matter as a consequence of Wallerian degeneration has been previously re-ported in a case report18and a series of term infants
with ischemic brain injury.19
We demonstrated a strong relationship between the ADC value in the PLIC and observed changes on conventional MRI within the PLIC. This raises the possibility that the signal abnormality within the PLIC, first reported by Rutherford et al,8is related to
Wallerian degeneration of the motor pathway after ischemic injury to the parasagittal motor cortex, a lesion that common occurs in term newborn infants who sustain HIE.20
In summary, we presented a cohort of infants who had HIE and for whom the ADC value in the PLIC was predictive of both survival and neuromotor dis-ability among survivors. Furthermore, we showed a significant association between the ADC value in the PLIC and appearance of the PLIC on conventional MRI. The ADC value in the PLIC is an objective measure of ischemic injury and may be of use as an objective prognostic marker for infants with HIE.
REFERENCES
1. Barkovich AJ, Hajnal BL, Vigneron D, et al. Prediction of neuromotor outcome in perinatal asphyxia: evaluation of MR scoring systems.AJNR Am J Neuroradiol.1998;19:143–149
2. Ment LR, Bada HS, Banres P, et al. Practice parameter: neuroimaging of the neonate: report of the Quality Standards Subcommittee of the Amer-ican Academy of Neurology and the Practice Committee of the Child Neurology Society.Neurology.2002;58:1726 –1738
3. Sie LT, van der Knaap MS, Oosting J, de Vries LS, Lafeber HN, Valk J. MR patterns of hypoxic-ischemic brain damage after prenatal, perinatal or postnatal asphyxia.Neuropediatrics2000;31:128 –136
4. Mercuri E, Guzzetta A, Haataja L, et al. Neonatal neurological exami-nation in infants with hypoxic ischaemic encephalopathy: correlation with MRI findings.Neuropediatrics.1999;30:83– 89
5. Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal dis-tress.Arch Neurol.1976;33:697– 670
6. Barkovich AJ, Westmark K, Partridge C, Sola A, Ferriero DM. Perinatal asphyxia: MR findings in the first 10 days.AJNR Am J Neuroradiol.
1995;16:427– 438
7. Coskun A, Lequin M, Segal M, Vigneron DB, Ferriero DM, Barkovich AJ. Quantitative analysis of MR images in asphyxiated neonates: cor-relation with neurodevelopmental outcome.AJNR Am J Neuroradiol.
2001;22:400 – 405
8. Rutherford MA, Pennock JM, Counsell SJ, et al. Abnormal magnetic resonance signal in the internal capsule predicts poor neurodevelop-mental outcome in infants with hypoxic-ischemic encephalopathy. Pe-diatrics.1998;102:323–328
9. Barkovich AJ, Westmark KD, Bedi HS, Partridge JC, Ferriero DM, Vigneron DB. Proton spectroscopy and diffusion imaging on the first day of life after perinatal asphyxia: preliminary report.AJNR Am J Neuroradiol.2001;22:1786 –1794
10. Robertson RL, Ben-Sira L, Barnes PD, et al. MR line-scan diffusion-weighted imaging of term neonates with perinatal brain ischemia.AJNR Am J Neuroradiol.1999;20:1658 –1670
11. Cowan FM, Pennock JM, Hanrahan JD, Manji KP, Edwards AD. Early detection of cerebral infarction and hypoxic ischemic encephalopathy in neonates using diffusion-weighted magnetic resonance imaging. Neu-ropediatrics.1994;25:172–175
13. McKinstry RC, Miller JH, Snyder AZ, et al. A prospective, longitudinal diffusion tensor imaging study of brain injury in newborns.Neurology.
2002;59:824 – 833
14. Forbes KPN, Pipe JG, Bird CR. Changes in brain water diffusion during the 1st year of life.Radiology.2002;222:405– 409
15. Neil JJ, Shiran SI, McKinstry RC, et al. Normal brain in human newborns: apparent diffusion coefficient and diffusion anisotropy measured by using diffusion tensor MR Imaging.Radiology.1998;209: 57– 66
16. Huppi PS, Maier SE, Peled S, et al. Microstructural development of human newborn cerebral white matter assessed in vivo by diffusion tensor magnetic resonance imaging.Pediatr Res.1998;44:584 –590
17. Wolf RL, Zimmerman RA, Clancy R, Haselgrove JH. Quantitative ap-parent diffusion coefficient measurements in term neonates for early detection of hypoxic-ischemic brain injury: initial experience.Radiology.
2001;218:825– 833
18. Neil JJ, Inder TE. Detection of Wallerian degeneration in a newborn by diffusion MR imaging.Pediatr Res.2003;53:544A
19. Mazumdar A, Mukherjee P, Miller JH, Malde H, McKinstry RC. Diffu-sion-weighted imaging of acute corticospinal tract injury preceding Wallerian degeneration in the maturing human brain. AJNR Am J Neuroradiol.2003;24:1057–1066
20. Campistol J, Poo P, Fernandez Alvarez E. Parasagittal cerebral injury: magnetic resonance findings.J Child Neurol.1999;14:683– 685
DRUGS IN OUR WATER?
“[Britain’s Environment Agency recently announced] that it had found traces of the antidepressant drug Prozac in rivers and groundwater. The idea of someone dumping mood-altering pharmaceuticals into the water supply sounds suitably Strangelovian, but the source in this case is humans, whose consumption of antidepressants has risen at an alarming rate—to 24 million prescriptions in Britain in 2001 from some 9 million in 1991. The actual level of contamination was not announced. It’s likely to be very low, but there is not much reassurance in that. In fact, there’s something genuinely depressing about finding a nation’s water supply to be contaminated by antidepressants. Britain is hardly alone in finding weird stuff coming out of the tap. Surveys of some American water supplies have turned up traces of everything from hormones to antibiotics. It makes you wonder what other drugs are lurking in the water and in what proportions. If Prozac is present, can Viagra be far behind?”
New York Times. August 11, 2004
DOI: 10.1542/peds.2003-0935-L
2004;114;999
Pediatrics
Rod W. Hunt, Jeffrey J. Neil, Lee T. Coleman, Michael J. Kean and Terrie E. Inder
Predicts Outcome After Perinatal Asphyxia
Apparent Diffusion Coefficient in the Posterior Limb of the Internal Capsule
Services
Updated Information &
http://pediatrics.aappublications.org/content/114/4/999
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/114/4/999#BIBL
This article cites 20 articles, 10 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2003-0935-L
2004;114;999
Pediatrics
Rod W. Hunt, Jeffrey J. Neil, Lee T. Coleman, Michael J. Kean and Terrie E. Inder
Predicts Outcome After Perinatal Asphyxia
Apparent Diffusion Coefficient in the Posterior Limb of the Internal Capsule
http://pediatrics.aappublications.org/content/114/4/999
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.