REVIEW
Strategies to increase implementation
of pharmacotherapy for alcohol use
disorders: a structured review of care delivery
and implementation interventions
Emily C. Williams
1,2*, Theresa E. Matson
1,2,3and Alex H. S. Harris
4,5Abstract
Background: Effective medications for treating alcohol use disorders (AUD) are available but underutilized. Multiple
barriers to their provision have been identified, and optimal strategies for addressing and overcoming barriers to use of medications for AUD treatment remain elusive. We conducted a structured review of published care delivery and implementation studies evaluating interventions that aimed to increase medication treatment for patients with AUD to identify interventions and component strategies that were most effective.
Methods: We reviewed literature through May 2018 and used networking to identify intervention studies with AUD
medication receipt reported as a primary or secondary outcome. Studies were identified as care delivery studies, characterized by patient-level recruitment and willingness to be randomized to candidate treatment options, and implementation studies, characterized by inclusion of all patients treated at sites involved in the study. Each identi-fied study was independently coded by two investigators for strategies used, guided by a published taxonomy of implementation strategies. All authors reviewed coding discrepancies and revised codes based on consensus. After reaching internal consensus, we solicited feedback from lead investigators on studies to code additional strategies. We reviewed implementation strategies used across studies to assess their relationship with medication receipt, as well as alcohol use outcomes, as available.
Results: Nine studies were identified: four RCTs of care delivery interventions, four quasi-experimental evaluations of
large-scale implementation interventions, and one quasi-experimental evaluation of a targeted single-site implemen-tation intervention. Implemenimplemen-tation strategies used were variable across studies; no strategy was universally used. Effects of the interventions on receipt of AUD pharmacotherapy and alcohol use outcomes also varied. Three of four care delivery interventions resulted in increased receipt of AUD medications, but only one of these three improved alcohol use outcomes. One large-scale and one single-site implementation intervention were associated with increased AUD medication receipt, and these studies did not assess alcohol use outcomes. Patterns of implementa-tion strategies did not clearly distinguish studies that successfully increased use of pharmacotherapy versus those that did not.
© The Author(s) 2019. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creat iveco mmons .org/licen ses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creat iveco mmons .org/ publi cdoma in/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Open Access
*Correspondence: [email protected]
1 Health Services Research and Development (HSR&D) Center
of Innovation for Veteran-Centered and Value-Driven Care, Veterans Affairs (VA) Puget Sound Health Care System, 1660 South Columbian Way, Seattle, WA 98108, USA
Introduction
Alcohol use disorders (AUD) are common and associ-ated with significant morbidity and mortality [1–3], but are substantially undertreated. In 2013, 16.6 million U.S. adults met diagnostic criteria for an AUD, but research suggests only 7.8% received any formal treatment [4]. One of the major gaps in treatment for AUD is the signif-icant under-utilization of medications that are effective for treating AUD [1, 5, 6]. Three medications— disulfi-ram, acamprosate, and naltrexone (both oral and inject-able)—have FDA approval specifically for the treatment of AUD, and topiramate has strong meta-analytic sup-port [7]. Efforts to increase treatment of AUD with medi-cations is motivated in part because the modality may address many reported barriers to receiving any formal AUD treatment [4, 8]. For instance, psychosocial treat-ments are often offered in group settings, heightening stigma-related issues for some patients, whereas medica-tions can be provided on an individual basis [9]. In addi-tion, patients may not be ready to abstain [8, 10]. Further, though this may be shifting over time [11, 12], many treatment programs view abstinence as the ultimate goal [8], whereas abstinence is not required with all medica-tions and reduced drinking can be a goal of medication treatment [9]. Finally, AUD medications can be offered across healthcare settings, including primary care, which has been highlighted as an optimal setting for expansion of care for AUD [8, 13, 14].
Despite the promise of medication treatment for addressing several known barriers to AUD treatment and national recommendations encouraging medications be made available to all patients with AUD [15, 16], rates of pharmacotherapy for AUD remain extremely low. Among patients with AUD, 4-12% are treated pharmacologically [1, 6, 17–21]. Among subsets of patients with AUD and co-occurring schizophrenic, bipolar, posttraumatic stress or major depressive disorder, receipt of medications for AUD ranged from 7 to 11%, whereas receipt of medica-tions for the comorbid disorder ranged from 69 to 82% [19]. This gap in the quality of AUD treatment is well known, and the substantial barriers to provision of AUD medications in diverse contexts have been described [22–27]. However, the optimal strategies for addressing
these barriers and increasing use of medications for AUD treatment remain elusive.
In recent years, two related lines of research have con-tributed to knowledge regarding strategies to increase use of medications to treat AUD: evaluations of care delivery interventions and evaluations of implementa-tion intervenimplementa-tions. Care delivery intervenimplementa-tions typically focus on improving patient-level clinical outcomes (e.g., reduction in heavy drinking days or abstinence from alcohol use), but often secondarily assess patient- or clinician-level process outcomes focused on treatment receipt (e.g., engagement in pharmacotherapy for AUD). Implementation interventions are typically designed to improve patient- or clinician-level process outcomes, but sometimes secondarily include patient-level clinical out-comes when the evidence for the effects of the underlying practice is weak (so called Hybrid I studies) [28]. Other key differences exist between these types of research that may influence both clinical and process outcomes. Most importantly, care delivery interventions typically involve recruitment of patients who are willing to be randomized to the treatment arms contained within the new care delivery model. Thus, these trials may be restricted to patients who are at least open to, if not actively interested in, treatment for AUD. On the other hand, evaluations of implementation interventions typically recruit and inter-vene on clinical entities (e.g., providers, clinics, hospitals) who serve large groups of patients who likely have more variable interest in treatment. Further, evaluations of care delivery interventions are typically designed to estab-lish the effectiveness (or lack thereof) of particular care delivery models. Thus, these studies generally put sig-nificant effort and resources into ensuring fidelity to the care delivery model. On the other hand, implementation evaluations are often trying to establish the effectiveness of bundles of strategies (interventions) to increase uptake of practices that do not depend on external research resources. Thus, evaluations of implementation interven-tions may measure fidelity as a process outcome but typi-cally exert less direct control [29].
Even though care delivery and implementation inter-ventions differ in terms of methodology, patient inclu-sion criteria, and primary outcomes, they may evaluate the effectiveness of the same underlying implementation
Conclusions: Our review did not reveal strategies most effective for implementing AUD medications. Interventions
designed to overcome identified barriers may have missed the mark, or differences in the intensity or targets of strate-gies may matter more than differences in stratestrate-gies. Further research is needed to understand effective implementa-tion methods and to better understand patient-level perspective, preferences and barriers to receipt of medicaimplementa-tions.
Keywords: Alcohol use disorders, Medication assisted treatment, Pharmacotherapy, Naltrexone, Acamprosate,
strategies, such as reorganizing, supplementing, or inter-vening on existing models of care [29]. The fact that the same component implementation strategies (e.g., audit and feedback) have been evaluated by these different research designs with very different patient populations affords an opportunity to take stock of the effectiveness of these interventions, and to distill insights into which designs, contexts, and component strategies appear to drive outcomes. Therefore, our goal was to conduct a structured review of published evaluations of care deliv-ery and implementation interventions that have either primarily or secondarily aimed to increase use of phar-macotherapy for patients with AUD, with the goal of identifying component strategies that may be effective in increasing pharmacologic treatment of AUD. Our review was guided by an existing taxonomy of implementation strategies and terms identified via a three-round modi-fied-Delphi process [30]. The purpose of our review was to learn which components have been tried most com-monly and which strategies might be associated with larger effects. Also, due to the fact that evaluations of care delivery interventions exert greater efforts to ensure fidelity and include patients willing to be randomized, we hypothesized that higher adoption of medications for AUD will be observed in those contexts compared to implementation interventions, which typically aim to intervene on clinician and patient populations with greater variability in treatment motivation, knowledge, and preferences.
Methods
For this structured literature review, we sought to identify published evaluations of care delivery and implementa-tion intervenimplementa-tions reporting effects on receipt of medi-cation treatments for patients with AUD. We reviewed literature through May 2018. Studies were identified via searching PubMed, Google Scholar, and PsychInfo with relevant search terms (e.g., pharmacotherapy, alcohol use disorder medications, AUD medications, naltrexone, Acamprosate, disulfiram, medication-assisted treatment). We also reviewed reference lists from identified studies to identify additional studies that may have been missed by our search. Finally, because we have personally con-ducted and/or served as co-investigators on related stud-ies, additional studies were also identified via networking. Once identified, each individual article was coded for implementation strategies used, as guided by Powell et al.’s refined compilation of implementation strategies resulting from the Expert Recommendations for Imple-menting Change (ERIC) project [30]. All articles were independently reviewed and coded by two investigators (EW and TM). When multiple articles and/or published protocols or commentaries were identified that described
a single intervention and/or implementation effort, these articles were aggregated to the level of the intervention (e.g., three studies had adjoining published protocol papers, which were coded under the umbrella of a single study). Once coded, all authors met to review coding dis-crepancies, discuss interpretation of codes, arrive at con-sensus, and revise individual codes based on consensus.
After reaching internal consensus on coding, we reached out to the lead or senior author of each study to ask whether our codes aligned with their understand-ing/interpretation of their study and associated report. We shared Powell et al’s description of strategies and asked them to review our coding to see if they thought we had missed or miscoded anything. Finally, process (e.g., rates of prescribed AUD pharmacotherapy) and alcohol use outcome data were extracted from each study and described. All authors reviewed the coding of implementation strategies against study outcomes data to qualitatively identify sets of implementation strate-gies that might have been be most effective for increas-ing provision of AUD medications and report whether interventions that increased AUD pharmacotherapy also improved alcohol use outcomes.
Results
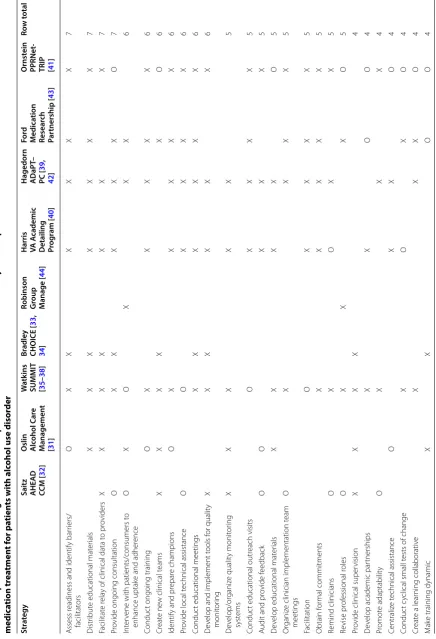
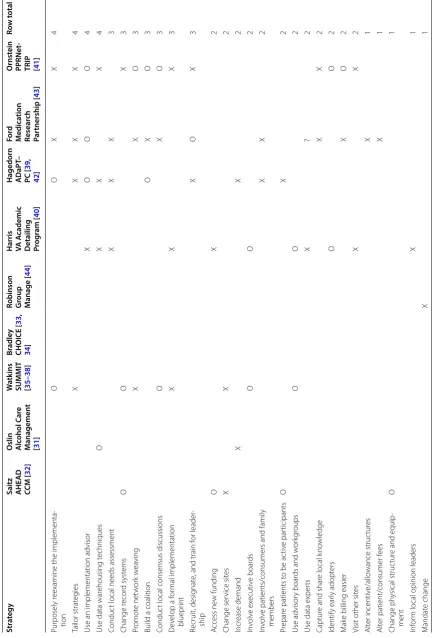
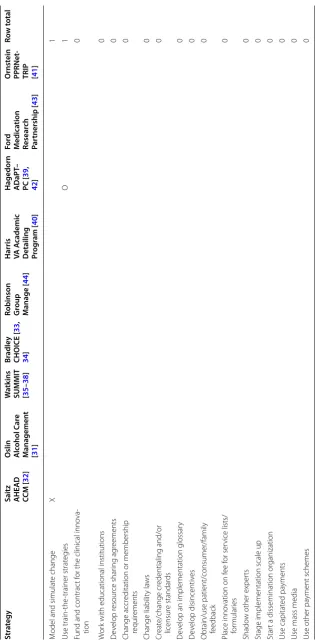
Our literature review identified nine studies that evalu-ated interventions to primarily or secondarily increase utilization of pharmacotherapy for AUD. Four were randomized clinical trials of care delivery interventions designed to improve alcohol-related outcomes [31–38]. Four were quasi-experimental evaluations of large-scale implementation interventions designed to increase medi-cation receipt [39–43], and one was a quasi-experimen-tal evaluation of targeted implementation intervention in a single-site [44]. Two additional studies were iden-tified but not included. The first reported on a large-scale implementation intervention designed to increase screening and brief intervention for unhealthy alcohol use and secondarily assessed whether the implemen-tation was associated with increased receipt of AUD medications among those who screened positive [45]. However, it was not clear how many of the patients who screened positive met diagnostic criteria for AUD and thus would have been eligible for medication treatment, and, though findings regarding medication use were summarized, detailed data were not reported. The sec-ond report was a description of a demonstration project to implement extended release naltrexone in Los Ange-les County, but no evaluation of the program’s effect on receipt of medication treatment among patients with AUD was reported [46].
Table 1 I mplemen ta tion str at egies iden tified in published e valua tions of car e deliv er y and implemen ta tion in ter ven tions tha t ha
ve aimed t
o incr ease medic ation tr ea tmen t f or pa tien ts with alc
ohol use disor
der
Str
at
egy
Saitz AHEAD CCM [
32
]
Oslin Alc
ohol C ar e M anagemen t [ 31 ] W atk ins
SUMMIT [35
– 38 ] Br adle y CHOICE [ 33 , 34 ]
Robinson Group Manage [
44
]
Harris VA A
cademic
Detailing Prog
ram [ 40 ] Hagedorn ADaPT – PC [ 39 , 42 ] Fo rd M edica tion Resear ch Par tnership [ 43 ] O rnst ein PPRNet
-TRIP [41
] Ro w t otal A ssess r
eadiness and identify bar
riers/ facilitat ors O X X X X X X 7 Distr ibut
e educational mat
er ials X X X X X X X 7 Facilitat e r ela
y of clinical data t
o pr oviders X X X X X X X 7 Pr
ovide ongoing consultation
O X X X X X O 7 Int er
vene with patients/consumers t
o
enhance uptak
e and adher
ence O X O X X X 6 Conduc
t ongoing training
O X X X X X 6 Cr eat e ne
w clinical t
eams X X X X X O 6
Identify and pr
epar e champions O X X X X X 6 Pr
ovide local t
echnical assistance O O X X X X 6 Conduc
t educational meetings
X X X X X X 6 D ev
elop and implement t
ools f or qualit y monit or ing X X X X X X 6 D ev elop/or ganiz e qualit y monit or ing syst ems X X X X X 5 Conduc
t educational outr
each visits O X X X X 5 A
udit and pr
ovide f eedback O O X X X 5 D ev
elop educational mat
er ials X X X X O 5 Or ganiz
e clinician implementation t
eam meetings O X X X X 5 Facilitation O X X X X 5 Obtain f or mal commitments X X X X X 5 Remind clinicians O X O X X 5 Re vise pr of essional r oles O X X X O 5 Pr
ovide clinical super
vision X X X X 4 D ev
elop academic par
tnerships X X O O 4 Pr omot e adaptabilit y O X X X 4 Centraliz e t echnical assistance O X X O 4 Conduc t c
yclical small t
ests of change
X O X O 4 Cr eat
e a lear
ning collaborativ e X X X O 4 M ak
e training dynamic
X
X
O
O
Table
1
(c
on
tinued)
Str
at
egy
Saitz AHEAD CCM [
32
]
Oslin Alc
ohol C
ar
e
M
anagemen
t
[
31
]
W
atk
ins
SUMMIT [35
–
38
]
Br
adle
y
CHOICE [
33
,
34
]
Robinson Group Manage [
44
]
Harris VA A
cademic
Detailing Prog
ram [
40
]
Hagedorn ADaPT
–
PC [
39
,
42
]
Fo
rd
M
edica
tion
Resear
ch
Par
tnership [
43
]
O
rnst
ein
PPRNet
-TRIP [41
]
Ro
w t
otal
Pur
posely r
eexamine the implementa
-tion
O
O
X
X
4
Tailor strat
eg
ies
X
X
X
X
4
Use an implementation advisor
X
O
O
O
4
Use data war
ehousing t
echniques
O
X
X
X
4
Conduc
t local needs assessment
X
X
X
3
Change r
ecor
d syst
ems
O
O
X
3
Pr
omot
e net
w
or
k w
ea
ving
X
X
O
3
Build a coalition
O
X
O
3
Conduc
t local consensus discussions
O
X
O
3
D
ev
elop a f
or
mal implementation
bluepr
int
X
X
X
3
Recruit, desig
nat
e, and train f
or leader
-ship
X
O
X
3
A
ccess ne
w funding
O
X
2
Change ser
vice sit
es
X
X
2
Incr
ease demand
X
X
2
In
volv
e ex
ecutiv
e boar
ds
O
O
2
In
volv
e patients/consumers and family
members
X
X
2
Pr
epar
e patients t
o be ac
tiv
e par
ticipants
O
X
2
Use advisor
y boar
ds and w
or
kg
roups
O
O
2
Use data exper
ts
X
?
2
Captur
e and shar
e local k
no
wledge
X
X
2
Identify ear
ly adopt
ers
O
O
2
M
ak
e billing easier
X
O
2
Visit other sit
es
X
X
2
Alt
er incentiv
e/allo
wance struc
tur
es
X
1
Alt
er patient/consumer f
ees
X
1
Change ph
ysical struc
tur
e and equip
-ment
O
1
Inf
or
m local opinion leaders
X
1
M
andat
e change
X
Table
1
(c
on
tinued)
Str
at
egy
Saitz AHEAD CCM [
32
]
Oslin Alc
ohol C
ar
e
M
anagemen
t
[
31
]
W
atk
ins
SUMMIT [35
–
38
]
Br
adle
y
CHOICE [
33
,
34
]
Robinson Group Manage [
44
]
Harris VA A
cademic
Detailing Prog
ram [
40
]
Hagedorn ADaPT
–
PC [
39
,
42
]
Fo
rd
M
edica
tion
Resear
ch
Par
tnership [
43
]
O
rnst
ein
PPRNet
-TRIP [41
]
Ro
w t
otal
M
odel and simulat
e change
X
1
Use train-the
-trainer strat
eg
ies
O
1
Fund and contrac
t f
or the clinical inno
va
-tion
0
W
or
k with educational institutions
0
D
ev
elop r
esour
ce shar
ing ag
reements
0
Change accr
editation or membership
requir
ements
0
Change liabilit
y la
ws
0
Cr
eat
e/change cr
edentialing and/or
licensur
e standar
ds
0
D
ev
elop an implementation glossar
y
0
D
ev
elop disincentiv
es
0
Obtain/use patient/consumer/family feedback
0
Place inno
vation on f
ee f
or ser
vice lists/
for
mular
ies
0
Shado
w other exper
ts
0
Stage implementation scale up
0
Star
t a dissemination or
ganization
0
Use capitat
ed pa
yments
0
Use mass media
0
Use other pa
yment schemes
study (labelled with X). All lead or senior authors of stud-ies responded to our request for review of the codes and added additional codes (labelled with an O). Implemen-tation strategies used were variable across the studies, and no strategy was used across all studies (Table 1). The most frequently used strategies were assessing readi-ness and identifying barriers and facilitators, distributing educational materials, facilitating relay of clinical data to providers (audit and feedback), and providing ongo-ing consultation. Strategies less frequently used involved payment and/or incentives or changes in laws and/or cre-dentialing and licensing.
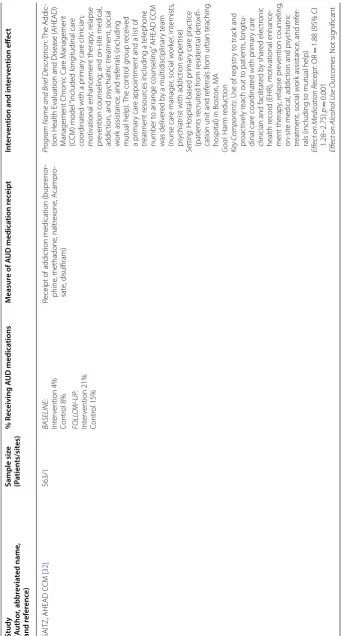
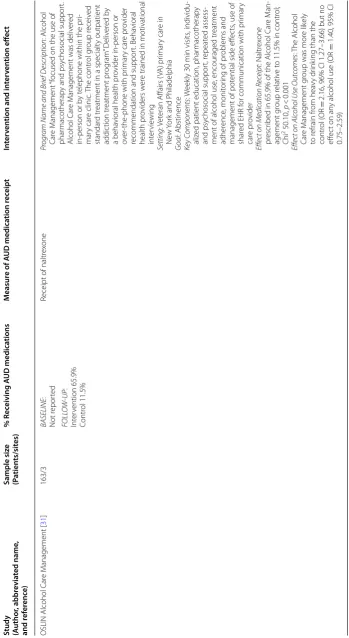
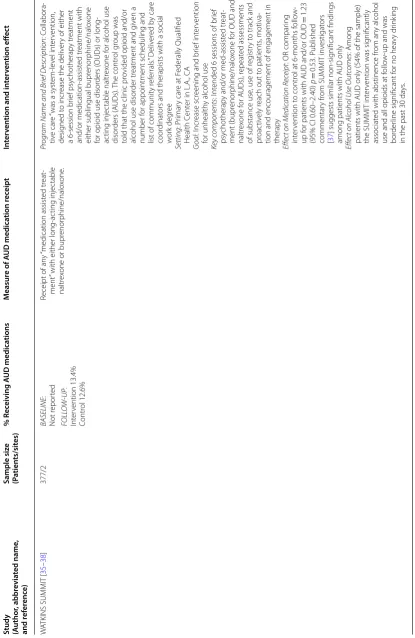
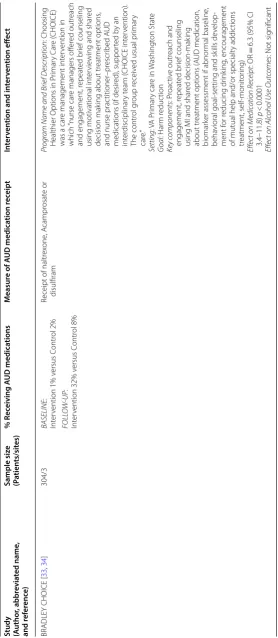
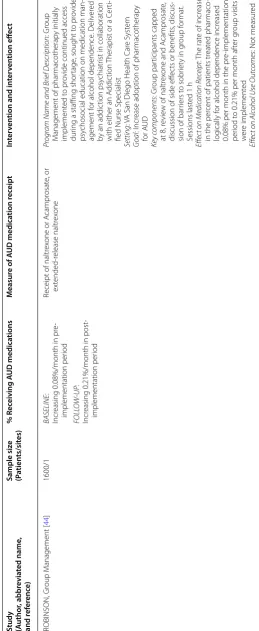
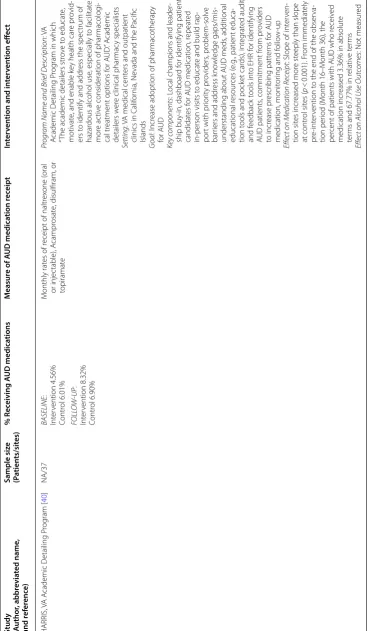
The effects of the interventions on receipt of AUD pharmacotherapy were also variable across studies (Table 2). In three of the four randomized evaluations of care delivery models [31–33], the interventions were associated with varying magnitude of increased receipt of AUD medications. At follow-up, treatment group rates of medication receipt ranged from 13 [36] to almost 70% [31]. The latter study, Oslin’s Alcohol Care Man-agement model [31], was the only approach to signifi-cantly increase receipt of AUD medications and improve patient-level alcohol use outcomes (Table 2). Two of the four implementation interventions [40, 41] were asso-ciated with increased AUD medication receipt. While Ornstein’s Practice Partner Research Network-Trans-lating Research Into Practice (PPRNet-TRIP) interven-tion appeared to have small early effects, proporinterven-tions of patients receiving medications were so low that contin-ued evaluation over time was not possible [41]. The Vet-erans Health Administration’s (VA) Academic Detailing Program appeared to increase rates of AUD medication receipt from 4.6 to 8.3% among patients with AUD [40]. Receipt of AUD medications also appeared to increase in in a single VA facility after implementation of a group medication management program attended by patients taking and considering medication treatment [44].
Patterns of implementation strategies did not clearly distinguish studies that successfully increased use of pharmacotherapy versus those that did not.
Discussion
Nine studies have evaluated the effects of care delivery or implementation interventions designed to increase active consideration and use of pharmacologic treatment options for patients with AUD. The interventions var-ied widely in context, intensity, target populations, and the underlying strategies, though many strategies were shared across studies, regardless of design (care delivery or implementation intervention). As hypothesized, care delivery interventions, targeted on patients willing to be randomized, were associated with much larger and more consistent improvements in rates of medication receipt
compared to implementation interventions targeted at the overall population of patients with AUD. Among the care delivery interventions evaluated, three out of four increased use of medications. However, of these three, only Oslin’s Alcohol Care Management intervention improved initiation of medications for AUD with more than one third of enrolled patients (69%) and improved in patient-level alcohol use. This trial may have been distinct from the others in its recruitment approaches—patients were recruited with the knowledge that the intervention aimed to provide pharmacologic treatment [31].
Among the implementation interventions evaluated, only the VA Academic Detailing Program [40] showed significant promise in increasing rates of medication receipt. It may be noteworthy that, compared to the other implementation interventions, the VA Academic Detail-ing Program was very labor intensive and targeted to diverse clinical settings with a high density of patients with AUD, not just primary care. The study of group medication management visits, intended as a means to increase prescribing capacity and educate patients who were considering medication treatment, [44] showed signals of effectiveness in one VA facility with a highly motivated champion. Interestingly, group settings have previously been identified as a barrier to receiving ment for AUD, but appeared to facilitate increased treat-ment receipt among persons already seeking treattreat-ment. This intervention should be more rigorously evaluated in contexts where the primary barrier is low capacity to pro-vide medication management.
Table
2
S
tudy designs and in
ter
ven
tion eff
ec
ts on A
UD medic
ation r
ec
eipt
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
SAITZ, AHEAD C
CM [
32
]
563/1
BA
SELINE
:
Int
er
vention 4%
Contr
ol 8%
Receipt of addic
tion medication (bupr
enor
-phine
, methadone
, naltr
ex
one
, A
campr
o-sat
e, disulfiram)
Pr
ogr
am Name and Brief D
escription
: T
he
A
ddic
-tion Health E
valuation and Disease (
AHEAD)
M
anagement Chr
onic C
ar
e M
anagement
(C
CM) model
“included long
itudinal car
e
coor
dinat
ed with a pr
imar
y car
e clinician;
motivational enhancement therap
y; r
elapse
pr
ev
ention counseling; and on-sit
e medical
,
addic
tion, and psy
chiatr
ic tr
eatment, social
w
or
k assistance
, and r
ef
er
rals (including
mutual help).
The contr
ol g
roup r
eceiv
ed
a pr
imar
y car
e appointment and a list of
tr
eatment r
esour
ces including a t
elephone
number t
o ar
range counseling
.” AHEAD C
CM
was deliv
er
ed b
y a multidisciplinar
y t
eam
(nurse car
e manager
, social w
or
ker
, int
er
nists
,
psy
chiatr
ist with addic
tion exper
tise)
Setting
: Hospital-based pr
imar
y car
e prac
tice
(patients r
ecruit
ed fr
om r
esidential det
oxifi
-cation unit and r
ef
er
rals fr
om ur
ban t
eaching
hospital) in Bost
on, M
A
G
oal
: Har
m r
educ
tion
Ke
y C
omponents
: Use of r
eg
istr
y t
o track and
pr
oac
tiv
ely r
each out t
o patients
, long
itu
-dinal car
e coor
dinat
ed with pr
imar
y car
e
clinician and facilitat
ed b
y shar
ed elec
tr
onic
health r
ecor
d (EHR), motivational enhance
-ment therap
y, r
elapse pr
ev
ention counseling
,
on-sit
e medical
, addic
tion and psy
chiatr
ic
tr
eatment, social w
or
k assistance
, and r
ef
er
-rals (including t
o mutual help)
Effect on Medic
ation Rec
eipt
: OR
=
1.88 (95% CI
1.28–2.75)
p
=
0.001
Effect on Alc
ohol Use O
utc
omes
: Not sig
nificant
FOLL
O
W
-UP
:
Int
er
vention 21%
Contr
Table
2
(c
on
tinued)
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
OSLIN Alcohol C
ar
e M
anagement [
31
]
163/3
BA
SELINE
:
Not r
epor
ted
Receipt of naltr
ex
one
Pr
ogr
am Name and Brief D
escription
: Alcohol
Car
e M
anagement
“focused on the use of
phar
macotherap
y and psy
chosocial suppor
t.
Alcohol C
ar
e M
anagement was deliv
er
ed
in-person or b
y t
elephone within the pr
i-mar
y car
e clinic
. T
he contr
ol g
roup r
eceiv
ed
standar
d tr
eatment in a specialt
y outpatient
addic
tion tr
eatment pr
og
ram
” D
eliv
er
ed b
y
a beha
vioral health pr
ovider in-person or
ov
er
-the
-phone with pr
imar
y car
e pr
ovider
recommendation and suppor
t. Beha
vioral
health pr
oviders w
er
e trained in motivational
int
er
vie
wing
Setting
: V
et
eran A
ffairs (
VA) pr
imar
y car
e in
Ne
w
Yor
k and P
hiladelphia
G
oal
: Abstinence
Ke
y C
omponents
: W
eek
ly 30
min visits
, individu
-aliz
ed patient education, phar
macotherap
y
and psy
chosocial suppor
t, r
epeat
ed assess
-ment of alcohol use
, encouraged tr
eatment
adher
ence
, monit
or
ing of pr
oblems and
management of pot
ential side eff
ec
ts
, use of
shar
ed EHR f
or communication with pr
imar
y
car
e pr
ovider
Effect on Medic
ation Rec
eipt
: Naltr
ex
one
pr
escr
ibed in 65.9% of the Alcohol C
ar
e M
an
-agement g
roup r
elativ
e t
o 11.5% in contr
ol;
Chi
2 50.10,
p
<
0.001
Effect on Alc
ohol Use O
utc
omes
: T
he
Alcohol
Car
e M
anagement g
roup was mor
e lik
ely
to r
efrain fr
om hea
vy dr
ink
ing than the
contr
ol (
OR
=
2.16, 96% CI 1.27–3.66) but no
eff
ec
t on an
y alcohol use (
OR
=
1.40, 95% CI
0.75–2.59)
FOLL
O
W
-UP
:
Int
er
vention 65.9%
Contr
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
W
ATKINS SUMMIT [
35
–
38
]
377/2
BA
SELINE
:
Not r
epor
ted
Receipt of an
y
“medication assist
ed tr
eat
-ment
” with either long-ac
ting injec
table
naltr
ex
one or bupr
enor
phine/nalo
xone
.
Pr
ogr
am Name and Brief D
escription
: C
ollabora
-tiv
e car
e
“was a syst
em-le
vel int
er
vention,
desig
ned t
o incr
ease the deliv
er
y of either
a 6-session br
ief psy
chotherap
y tr
eatment
and/or medication-assist
ed tr
eatment with
either sublingual bupr
enor
phine/nalo
xone
for opioid use disor
ders (
OUDs) or
long-ac
ting injec
table naltr
ex
one f
or alcohol use
disor
ders (
AUDs).
The contr
ol g
roup was
told that the clinic pr
ovided opioid and/or
alcohol use disor
der tr
eatment and g
iv
en a
number f
or appointment scheduling and
list of communit
y r
ef
er
rals
.” D
eliv
er
ed b
y car
e
coor
dinat
ors and therapists with a social
w
or
k deg
ree
Setting
: P
rimar
y car
e at F
ederally Qualified
Health C
ent
er in L.A., CA
G
oal
: I
ncr
ease scr
eening and br
ief int
er
vention
for unhealth
y alcohol use
Ke
y c
omponents
: I
nt
ended 6 sessions of br
ief
psy
chotherap
y and/or med-assist
ed tr
eat
-ment (bupr
enor
phine/nalo
xone f
or OUD and
naltr
ex
one f
or A
UDs), r
epeat
ed assessments
of substance use
, use of r
eg
istr
y t
o track and
pr
oac
tiv
ely r
each out t
o patients
, motiva
-tion and encouragement of engagement in therap
y
Effect on Medic
ation Rec
eipt
: OR compar
ing
int
er
vention t
o contr
ol at 6-months f
ollo
w-up f
or patients with A
UD and/or OUD
=
1.23
(95% CI 0.60–2.40)
p
=
0.53.
Published
commentar
y fr
om SUMMIT in
vestigat
ors
[
37
] suggests similar non-sig
nificant findings
among patients with A
UD only
Effect on Alc
ohol Use O
utc
omes
: Among
patients with A
UD only (54% of the sample)
the SUMMIT int
er
vention was sig
nificantly
associat
ed with abstinence fr
om an
y alcohol
use and all opioids at f
ollo
w-up and was
bor
der
line sig
nificant f
or no hea
vy dr
ink
ing
in the past 30
da
ys
.
FOLL
O
W
-UP
:
Int
er
vention 13.4%
Contr
ol 12.6%
Table
2
(c
on
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
BRADLEY CHOICE [
33
,
34
]
304/3
BA
SELINE
:
Int
er
vention 1% v
ersus C
ontr
ol 2%
Receipt of naltr
ex
one
, A
campr
osat
e or
disulfiram
Pr
ogr
am Name and Brief D
escription
: Choosing
Healthier Options in P
rimar
y C
ar
e (
CHOICE)
was a car
e management int
er
vention in
which
“nurse car
e managers off
er
ed outr
each
and engagement, r
epeat
ed br
ief counseling
using motivational int
er
vie
wing and shar
ed
decision mak
ing about tr
eatment options
,
and nurse prac
titioner
–pr
escr
ibed A
UD
medications (if desir
ed), suppor
ted b
y an
int
er
disciplinar
y t
eam (
CHOICE int
er
vention).
The contr
ol g
roup r
eceiv
ed usual pr
imar
y
car
e.”
Setting
: V
A P
rimar
y car
e in
W
ashingt
on Stat
e
G
oal
: Har
m r
educ
tion
Ke
y c
omponents
: P
roac
tiv
e outr
each and
engagement, r
epeat
ed br
ief counseling
using MI and shar
ed decision-mak
ing
about tr
eatment options (
AUD medication,
biomar
ker assessment if abnor
mal baseline
,
beha
vioral goal-setting and sk
ills de
velop
-ment f
or r
educing dr
ink
ing
, encouragement
of mutual help and/or specialt
y addic
tions
tr
eatment, self-monit
or
ing)
Effect on Medic
ation Rec
eipt
: OR
=
6.3 (95% CI
3.4–11.8)
p
<
0.0001
Effect on Alc
ohol Use O
utc
omes
: Not sig
nificant
FOLL
O
W
-UP
:
Int
er
vention 32% v
ersus C
ontr
ol 8%
Table
2
(c
on
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
ROBINSON, Gr
oup M
anagement [
44
]
1600/1
BA
SELINE
:
Incr
easing 0.08%/month in pr
e-implementation per
iod
Receipt of naltr
ex
one or A
campr
osat
e, or
ex
tended-r
elease naltr
ex
one
Pr
ogr
am Name and Brief D
escription
: Gr
oup
M
anagement of phar
macotherap
y initially
implement
ed t
o pr
ovide continued access
dur
ing a staffing shor
tage
, sought t
o pr
ovide
psy
chosocial education on medication man
-agement f
or alcohol dependence
. D
eliv
er
ed
by an addic
tion psy
chiatr
ist in collaboration
with either an A
ddic
tion
Therapist or a C
er
ti-fied Nurse Specialist
Setting
: V
A San Diego Health C
ar
e Syst
em
G
oal
: I
ncr
ease adoption of phar
macotherap
y
for A
UD
Ke
y c
omponents
: Gr
oup par
ticipants capped
at 8, r
evie
w of naltr
ex
one and A
campr
osat
e,
discussion of side eff
ec
ts or benefits
, discus
-sion of bar
riers t
o sobr
iet
y in g
roup f
or
mat.
Sessions last
ed 1
h
Effect on Medic
ation Rec
eipt
: T
he rat
e of incr
ease
in the per
cent of patients tr
eat
ed phar
maco
-log
ically f
or alcohol dependence incr
eased
0.08% per month in the pr
e-implementation
per
iod t
o 0.21% per month af
ter g
roup visits
w
er
e implement
ed
Effect on Alc
ohol Use O
utc
omes
: Not measur
ed
FOLL
O
W
-UP
:
Incr
easing 0.21%/month in post
-implementation per
iod
Table
2
(c
on
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
HARRIS,
VA A
cademic D
etailing P
rog
ram [
40
]
NA/37
BA
SELINE
:
Int
er
vention 4.56%
Contr
ol 6.01%
M
onthly rat
es of r
eceipt of naltr
ex
one (
oral
or injec
table), A
campr
osat
e, disulfiram, or
topiramat
e
Pr
ogr
am Name and Brief D
escription
: V
A
A
cademic D
etailing P
rog
ram in which
“T
he academic detailers str
ov
e t
o educat
e,
motivat
e, and enable k
ey health car
e pr
ovid
-ers t
o identify and addr
ess the spec
trum of
hazar
dous alcohol use
, especially t
o facilitat
e
mor
e ac
tiv
e consideration of phar
macolog
i-cal tr
eatment options f
or A
UD
.” A
cademic
detailers w
er
e clinical phar
mac
y specialists
Setting
: V
A medical cent
ers and outpatient
clinics in C
alif
or
nia, Ne
vada and the P
acific
Islands
G
oal
: I
ncr
ease adoption of phar
macotherap
y
for A
UD
Ke
y c
omponents
: L
ocal champions and leader
-ship buy-in, dashboar
d f
or identifying patient
candidat
es f
or A
UD medication, r
epeat
ed
in-person visits t
o educat
e and build rap
-por
t with pr
ior
ity pr
oviders
, pr
oblem-solv
e
bar
riers and addr
ess k
no
wledge gaps/mis
-understanding about A
UD meds
, additional
educational r
esour
ces (
e.g
., patient educa
-tion t
ools and pock
et car
ds), int
eg
rat
ed audit
and f
eedback t
ools int
o EHR f
or identifying
AUD patients
, commitment fr
om pr
oviders
to incr
ease pr
escr
ibing patt
er
ns f
or A
UD
medication, monit
or
ing and f
ollo
w-up
Effect on Medic
ation Rec
eipt
: Slope of int
er
ven
-tion sit
es incr
eased mor
e st
eeply than slope
at contr
ol sit
es (
p
<
0.001).
Fr
om
immediat
ely
pr
e-int
er
vention t
o the end of the obser
va
-tion per
iod (M
onth 16–M
onth 36), the
per
cent of patients with A
UD who r
eceiv
ed
medication incr
eased 3.36% in absolut
e
ter
ms and 67.77% in r
elativ
e t
er
ms
Effect on Alc
ohol Use O
utc
omes
: Not measur
ed
FOLL
O
W
-UP
:
Int
er
vention 8.32%
Contr
ol 6.90%
Table
2
(c
on
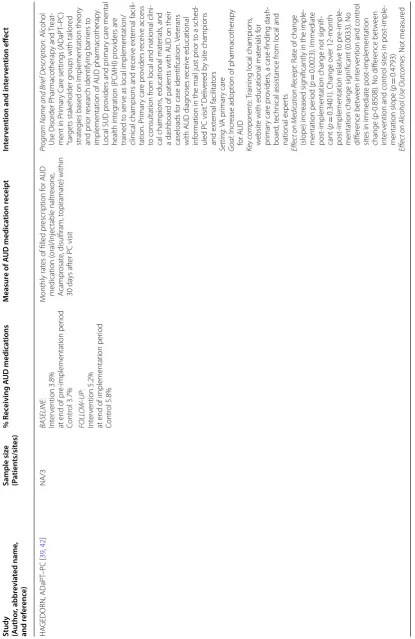
Study (Author , abbr evia ted name , and r ef er enc e) Sample siz e (P atien ts/sit es) % R ec eiving A UD medica tions M easur e of A UD medica tion r ec eipt In ter ven tion and in ter ven tion eff ec t HA GEDORN, ADaPT –PC [ 39 , 42 ] NA/3 BA SELINE : Int er vention 3.8%
at end of pr
e-implementation per iod Contr ol 3.7% M onthly rat
es of filled pr
escr iption f or A UD medication ( oral/injec table naltr ex one , A campr osat
e, disulfiram, t
opiramat
e) within
30
da
ys af
ter PC visit
Pr
ogr
am Name and Brief D
escription : Alcohol Use Disor der P har macotherap y and Tr eat
-ment in P
rimar
y C
ar
e settings (
ADaPT –PC ) “tar gets stak eholder g
roups with tailor
ed
strat
eg
ies based on implementation theor
y
and pr
ior r
esear
ch identifying bar
riers t
o
implementation of A
UD phar
macotherap
y.
Local SUD pr
oviders and pr
imar
y car
e mental
health int
eg
ration (PCMHI) pr
oviders ar
e
trained t
o ser
ve as local implementation/
clinical champions and r
eceiv e ex ter nal facili -tation. P rimar y car e pr oviders r eceiv e access
to consultation fr
om local and national clini
-cal champions
, educational mat
er
ials
, and
a dashboar
d of patients with A
UD on their
caseloads f
or case identification.
Vet erans with A UD diag noses r eceiv e educational inf or
mation in the mail just pr
ior t
o a sched
-uled PC visit.
” D eliv er ed b y sit e champions and ex ter nal facilitat ors Setting : V A pr imar y car e G oal : I ncr
ease adoption of phar
macotherap y for A UD Ke y c omponents : T
raining local champions
,
w
ebsit
e with educational mat
er ials f or pr imar y car e pr oviders
, a case
-finding dash
-boar
d, t
echnical assistance fr
om local and
national exper
ts
Effect on Medic
ation Rec
eipt
: R
at
e of change
(slope) incr
eased sig
nificantly in the imple
-mentation per iod ( p = 0.0023). Immediat e post
-implementation change not sig
nifi
-cant (
p
=
0.3401). Change o
ver 12-month post -implementation r elativ e t o pr e-imple
-mentation change sig
nificant (0.0033). No
diff er ence bet w een int er
vention and contr
ol
sit
es in immediat
e post
-implementation
change (p
-0.8508). No diff
er ence bet w een int er
vention and contr
ol sit
es in post
-imple
-mentation slope (
p
=
0.4793)
Effect on Alc
ohol Use O
utc
omes
: Not measur
ed FOLL O W -UP : Int er vention 5.2%
at end of implementation per
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
FORD Medication R
esear
ch P
ar
tnership [
43
]
3887/9
BA
SELINE
:
Int
er
vention 9.0%
Contr
ol 11.4%
Receipt of A
UD medication dur
ing an epi
-sode of car
e
Pr
ogr
am Name and Brief D
escription
: M
edica
-tion R
esear
ch P
ar
tnership
, “a collaboration
bet
w
een a national commer
cial health plan
and nine addic
tion tr
eatment cent
ers
, imple
-ment
ed or
ganizational and syst
em changes
to pr
omot
e use of f
ederally appr
ov
ed medi
-cations f
or tr
eatment of alcohol and opioid
use disor
ders
.” D
eliv
er
ed b
y commer
cial
health plan,
“nationally r
ecog
niz
ed exper
ts
in the substance abuse field
,” and
“change
leaders
.”
Setting
: Specialt
y addic
tion tr
eatment cent
ers
locat
ed on Nor
theast
er
n seaboar
d of the U
.S.
G
oal
: P
romot
e use of f
ederally appr
ov
ed medi
-cations f
or A
UD/OUD
Ke
y c
omponents
: “Change
leaders
” and “
change
teams
,” ex
ter
nal coaches
, rapid change c
ycles
to t
est strat
eg
ies t
o pr
omot
e medication use
,
pr
ovider training and t
echnical assistance
Effect on Medic
ation Rec
eipt
: Diff
er
ence in diff
er
-ences at
Year 3:
Unadjust
ed: 5.8%; A
djust
ed: 5.2% (95% CI
−
4.1
to 14.5)
p
=
0.27
Effect on Alc
ohol Use O
utc
omes
: Not measur
ed
3-YEAR FOLL
O
W
-UP
:
Int
er
vention 26.5%
Contr
ol 23.1%
Table
2
(c
on
Study (Author
, abbr
evia
ted name
,
and r
ef
er
enc
e)
Sample siz
e
(P
atien
ts/sit
es)
% R
ec
eiving A
UD medica
tions
M
easur
e of A
UD medica
tion r
ec
eipt
In
ter
ven
tion and in
ter
ven
tion eff
ec
t
ORNSTEIN PPRNet
-TRIP [
41
]
15053/19
EARL
Y INTER
VENTION CLINICS:
Phase 1: 2.6% Phase 2: 5.5%
Pr
escr
iption f
or disulfiram, naltr
ex
one (
oral or
injec
table), A
campr
osat
e, or t
opiramat
e
Pr
ogr
am Name and Brief D
escription
: P
rac
tice
Par
tner R
esear
ch Net
w
or
k-Translating
Resear
ch I
nt
o P
rac
tice (PPRNet
-TRIP) in
volv
ed
“prac
tice sit
e visits f
or academic detailing
and par
ticipat
or
y planning and net
w
or
k
meetings f
or
‘best prac
tice
’ dissemination
”
Setting
: P
rimar
y car
e prac
tices fr
om 15 U
.S.
Stat
es
G
oal
: I
ncr
eased pr
escr
iption f
or disulfiram,
naltr
ex
one (
oral or injec
table), A
campr
osat
e,
or t
opiramat
e f
or those with an A
UD
Ke
y c
omponents
: EHR t
emplat
e, per
for
mance
repor
ts
, pr
ovider education, and de
velop
-ment of an imple-mentation plan
Effect on Medic
ation Rec
eipt
: Due t
o small
pr
opor
tions of subjec
ts r
eceiving medica
-tions
, pr
e-post (phase 1 v
ersus phase 2)
compar
ison of medication r
eceipt was only
estimable in the ear
ly int
er
vention clinics
.
The adjust
ed OR f
or phase 1 v
ersus phase 2
in the ear
ly int
er
vention clinics was 2.24 (95%
CI 1.03 -4.88)
p
<
0.05
Effect on Alc
ohol Use O
utc
omes
: Not measur
ed
DEL
AY
ED INTER
VENTION CLINICS
:
Phase 1: 0% Phase 2: 2.4%
Table
2
(c
on
medication treatment for AUD—a substantially under-utilized treatment. Unfortunately, our review did not reveal which strategies are most effective for imple-menting AUD medications. However, we cataloged the use of specific strategies, perhaps suggesting candidates for future study. Further work is needed to understand why rates of medication treatment of AUD continue to be so low, even after patients are enrolled in care management interventions and/or receiving care in a healthcare setting that has been targeted by a multifac-eted intervention. It is entirely possible that previous examinations of barriers, and interventions designed to overcome them have missed the mark. To further assess this, research will be needed to better under-stand patient-level perspective, preferences and barri-ers to receipt of medications.
Abbreviations
VA: U.S. Veterans Health Administration; AUD: alcohol use disorder; ERIC: Expert Recommendations for Implementing Change project; PPRNet-TRIP: Practice Partner Research Network-Translating Research Into Practice; AHEAD: Addic-tion Health EvaluaAddic-tion and Disease; CCM: Chronic Care Model; EHR: electronic health record; SUMMIT: Substance Use Motivation and Medication Integrated Treatment; CHOICE: Choosing Healthier Drinking Options in Primary Care; ADaPT–PC: Alcohol Use Disorder Pharmacotherapy and Treatment in Primary Care Settings; OUD: opioid use disorder; PCMHI: primary care mental health integration.
Authors’ contributions
AHSH and ECW collaborated on the conception of the manuscript. All authors reviewed the literature, coded implementation strategies, and participated in drafting the manuscript. All authors read and approved the final manuscript.
Author details
1 Health Services Research and Development (HSR&D) Center of Innovation
for Veteran-Centered and Value-Driven Care, Veterans Affairs (VA) Puget Sound Health Care System, 1660 South Columbian Way, Seattle, WA 98108, USA.
2 Department of Health Services, University of Washington School of Public
Health, Seattle, WA, USA. 3 Kaiser Permanente Washington Health Research
Institute, Seattle, WA, USA. 4 Center for Innovation to Implementation, VA
Palo Alto Health Care System, Menlo Park, CA, USA. 5 Department of Surgery,
Stanford University School of Medicine, Stanford, CA, USA.
Acknowledgements
The authors would like to acknowledge the lead and/or senior investigators of publications included in this review for coding additional implementation strategies that may not have been apparent in the published article.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Consent for publication
Not applicable.
Ethics approval
Not applicable.
Funding
This study was supported in part by a VA HSR&D Research Career Scientist award (RCS 14-132) to Dr. Harris and a VA HSR&D Career Development award were not fully described in the published reports. These
findings suggest that an improved compilation of imple-mentation strategies may be needed to enable accurate and reliable identification of distinct strategies. Efforts to refine such a compilation should consider designat-ing umbrella strategies and sub-categories within them or providing a list of strategies that are similar but vari-able with regard to naming or minor procedural variants. Findings from our study also make clear the importance of comprehensive reporting of strategies used. While providing full descriptions of multi-faceted implementa-tion strategies can be difficult in a single outcomes paper, authors should be encouraged to publish more detailed study protocols (as several did in the present study [34,
35, 38, 39]), and reviewers may, nonetheless, need to query intervention developers as a final validity check.
Perhaps more importantly, no method has been devel-oped to characterize the intensity of strategies or cross-classify strategies with targets. Oslin’s Alcohol Care Management used many of the same strategies as other care delivery models but was targeted on patients willing to participate in an intervention focused on pharmaco-logic treatment. VA’s Academic Detailing Program did not differ from other implementation interventions in terms of component strategies so much as intensity and diversity of targets. Developing methods to more fully characterize interventions beyond component strategies may lead to insights that have greater utility for creating generalizable knowledge. In addition, because effective-ness of implementation interventions and strategies often depends on context, methods to cross-classify strategies with context and/or setting should be developed.
Beyond the aforementioned limitations of the existing implementation science tools used in this study, other limitations are worth noting. Although we searched mul-tiple data sources and used reference lists from identified studies and networking to ensure comprehensive capture of existing studies, it is possible we missed intervention studies that aimed at increasing pharmacologic treatment of AUD. Second, our review identified only a small num-ber of studies that reported receipt of AUD medication as a primary or secondary outcome. The small number of studies to date may limit the ability to identify generaliz-able information about the effectiveness of specific strat-egies. Moreover, of the nine studies that met inclusion criteria for this review, four were care delivery interven-tions tested in trials that were powered on main (clinical) outcomes. These studies may have been underpowered to detect differences in secondary outcomes, such as medi-cation receipt.