ARTICLE
Maternal Microchimerism in Underlying Pathogenesis
of Biliary Atresia: Quantification and Phenotypes of
Maternal Cells in the Liver
Toshihiro Muraji, MDa, Naoki Hosaka, MDb, Naoki Irie, PhDc, Makiko Yoshida, MDd, Yukihiro Imai, MDe, Kohichi Tanaka, MDf, Yasutsugu Takada, MDg, Seisuke Sakamoto, MDg, Hironori Haga, MDh, Susumu Ikehara, MDb
Departments ofaSurgery anddPathology, Kobe Children’s Hospital, Kobe, Japan;bFirst Department of Pathology, Kansai Medical University, Osaka, Japan;cInstitute for
Frontier Medical Sciences, Kyoto University, Kyoto, Japan; Departments ofgSurgery andhClinical Pathology, Kyoto University Gradate School of Medicine, Kyoto, Japan; eDepartment of Pathology, Kobe City General Hospital, Kobe, Japan;fInstitute for Biomedical Research and Innovation, Kobe, Japan
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.The goal was to examine whether microchimerism plays a crucial role in the pathogenesis of biliary atresia; we analyzed the localization of maternal microchi-meric cells and their phenotypes.
METHODS.Liver biopsy specimens from 8 male infants with biliary atresia and 6 control subjects with other liver diseases were investigated for maternal chimeric cells and their phenotypes through double-staining fluorescence in situ hybridization and immunohistochemical analyses.
RESULTS.Significantly larger numbers of maternal XX⫹cells were found in the portal
area and sinusoids of patients with biliary atresia, in comparison with control
patients. In phenotypic analyses of XX⫹ cells, CD8⫹ T cells, CD45⫹ cells, and
cytokeratin-positive cells were found, and the numbers and proportions among total
CD8⫹T cells were significantly higher than those in control patients.
CONCLUSIONS.Significantly more maternal chimeric CD8⫹T cells in the livers of patients with biliary atresia suggest that maternal immunologic insults represent the under-lying pathogenesis in biliary atresia. The findings support the recently postulated mechanisms of alloautoimmune and/or autoalloimmune responses.
B
ILIARY ATRESIA (BA)is an infantile liver disease of unknown cause in which the intrahepatic and extrahepatic bile ducts are damaged progressively by an ongoing fibrosing process, even in some patients with good bile drainage. Several factors have been proposed as contributors to the etiopathogenesis of the perinatal form of BA, including occultviral infections, defects in morphogenesis, vascular insults, toxic agents, and aberrant immune responses.1,2In 1988, on the
basis of our HLA-DR immunohistochemical study of the biliary epithelium in patients with BA, we postulated that
immune-mediated insults are involved in the development of BA.3Other reports also suggested that immune-mediated
bile duct injury plays an important role in BA.4–7Suskind et al8demonstrated maternal microchimerism in patients with
BA, which suggests that the etiopathogenesis involves graft-versus-host disease (GvHD) induced by maternal lymphocytes
engrafted through the placenta. Recently, Kobayashi et al9demonstrated maternal microchimerism
immunohistochemi-cally, with maternal anti-HLA antibody, in the hepatocytes and bile duct epithelia in BA. However, maternal microchi-merism itself does not necessarily prove any etiopathogenesis involved in BA, because 2-way maternofetal cell trafficking is a common phenomenon. In an attempt to obtain additional information to clarify the immunologic process that is involved, we characterized phenotypes and located the maternal chimeric cells infiltrating the livers of patients with BA.
METHODS
Patients
All 8 patients in this part of the study were male infants. The patients’ age at the time of surgery, associated anomalies, and types of porta hepatis were reviewed retrospectively. Liver biopsy specimens from these infants with
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-0568
doi:10.1542/peds.2007-0568
Key Words
biliary atresia, graft-versus-host disease, microchimerism, CD8
Abbreviations
BA— biliary atresia
GvHD— graft-versus-host disease BEC— biliary epithelial cell
FISH—fluorescence in situ hybridization
BA were fixed in 10% formaldehyde solution and
em-bedded in paraffin. Serial tissue sections of 2-m
thick-ness were prepared. Control specimens were liver tissues biopsied or resected for liver transplantation, at Kyoto
University Hospital, from 6 male patients⬍6 months of
age with various diseases, including cholestatic disease (tyrosinemia, Crigler-Najjar syndrome, hemangioendo-thelioma, choledochal cyst, and congenital absence of the portal vein).
Immunohistochemical Analyses
Immunohistochemical examinations were performed by using an Envision kit (Dako, Kyoto, Japan). Primary antibodies used in this study were against cytokeratin (diluted 50-fold; Dako), CD4 (prediluted; Nichirei, Tokyo, Japan), CD8 (prediluted; Nichirei), CD34 (di-luted 50-fold; Dako), CD56 (predi(di-luted; Nichirei), and CD79a (prediluted; Dako).
Fluorescence in Situ Hybridization
The existence of the XX chromosome was detected by using the fluorescence in situ hybridization (FISH) method. Probes for X and Y chromosomes (Vysis,
Down-ers Grove, IL) were used, and the 4⬘
,6-diamino-2-phe-nylindole/fluorescein isothiocyanate/Texas red triple-bandpass combination (Nikon, Tokyo, Japan) was applied. The slides were scanned at a magnification of 1000 with a fluorescence microscope (Nikon Eclipse 600) equipped with an epi-illumination system, includ-ing a 100-W mercury lamp with a set of filters. A total of
1000 nonoverlapping cells with nuclei with positive signals for both sex chromosomes (red: Y-positive; green: X-posi-tive) were counted. Cells with truncation of the nuclei from sectioning or with single signals for sex chromosomes were all excluded from the counts. Locations of XX chro-mosome-positive cells were investigated separately on the slides stained with cytokeratin-specific antibody and on the consecutive slides stained with hematoxylin and eosin.
Double-staining for FISH and immunohistochemical analyses was performed for CD8, CD4, CD45 (predi-luted; Nichirei), CD79a, and cytokeratin in all cases, and results were matched to the corresponding fields on the consecutive slides stained with hematoxylin and eosin to characterize phenotypically the XX chromosome-posi-tive cells. Double-staining analysis of CD34 and CD56 with FISH for the XX chromosome was not performed, because such cells had not infiltrated the portal area. The investigation was approved by the institutional review boards at Kobe Children’s Hospital and Kyoto University Graduate School of Medicine, and parental informed consent to participate in this study was obtained.
RESULTS
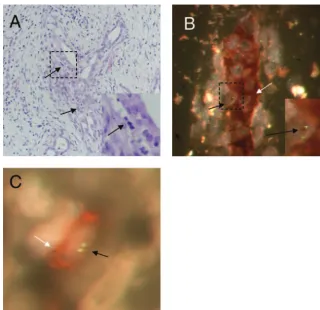
We first examined the histologic results for maternal chimerism and determined a phenotype of the chimeric cells in the liver samples from the patients with BA. In the specimens from all 8 patients with BA, lymphocytes had infiltrated the portal area; some had destroyed bile ducts with inflammatory edema (Fig 1A). The lympho-cytes were immunohistochemically positive for CD8 or FIGURE 1
CD79a, few for CD4, and none for CD34 or CD56. Counts of maternal cells with a set of double X chromo-somes in the specimens, which ranged from 6 to 50 cells per 1000 cells in patients with BA, were significantly higher than counts in samples from patients without BA
(patients with BA: 19.9⫾5.2 cells per 1000 cells; control
patients: 2.2⫾0.3 cells per 1000 cells;P⫽.0007) (Table 1).
In the double-staining analyses, some XX⫹cells were
present in the injured bile duct epithelium stained for
cytokeratin (Fig 1B). Furthermore, the numbers of XX⫹
maternal CD8⫹ cytotoxic T cells in patients with BA
were significantly higher than those in patients without
BA (patients with BA: 2.6 ⫾ 1.0 cells per 1000 cells;
control patients: 0.3⫾0.2 cells per 1000 cells;P⫽.020)
(Fig 1C). In addition, 7 of 8 patients with BA (86%)
showed infiltration of XX⫹CD8⫹T cells, although only 2
(33%) of 6 control patients showed such cells.
Strik-ingly, the proportion of maternal CD8⫹T cells in total
CD8⫹ T cells was 10-fold higher than that in patients
without BA (patients with BA: 27.9 ⫾ 12.4%; control
patients: 1.0⫾0.6%;P⫽.008), whereas the total
num-ber of CD8⫹T cells in patients with BA was lower than
that in control patients (patients with BA: 13.6 ⫾ 3.2
cells per 1000 cells; control patients: 28.5⫾4.2 cells per
1000 cells; P ⫽ .029). Neither XX⫹ CD4⫹ T cells nor
CD79a⫹B cells were remarkable. These findings indicate
that there are maternal CD8⫹ T cell-predominant
im-mune responses proceeding in the liver samples from patients with BA.
DISCUSSION
Our quantitative analysis of maternal XX⫹ cells in the
liver of male patients with BA indicated 1 cell per 102to
103cells counted, with the stringent criterion that a pair
of X signals be clearly included within a nontruncated nucleus. The frequency of these maternal cells in the patients with BA was much higher than levels of nonself
cells found after solid organ transplantation10or normal
pregnancy11 (1 cell per 104 to 105 cells). More
impor-tantly, the frequency of XX⫹ cells was nearly 10-fold
greater than that in patients without BA. However, our investigation was based on a relatively small number of maternal cells in only 8 cases, which could lead to type II statistical errors. We avoided using neonatal hepatitis as a control condition because neonatal hepatitis is itself a disease of unknown cause and could be a mild type of GvHD.
In the phenotypic analysis, the significantly elevated
number of maternal XX⫹CD8⫹cells and the proportion
of XX⫹CD8⫹cells in total CD8⫹T cells were noted. We
found only a few total CD4⫹T cells, including XX⫹cells.
The effector cells predominantly found in BA are
con-troversial, with some reports indicating CD4⫹ T cells5,7
but another indicating CD8⫹T cells.12Above all, the high
chimeric rate of maternal cells of immune origin (XX⫹
CD8⫹ T cells) indicates that patients with BA have a
considerable gross amount of these immunologic mater-nal cells in their tissues, which suggests the possible involvement of these cells in the pathogenesis of BA.
In addition, these XX⫹cells were located in the portal
area, intimately situated with the cytokeratin-positive biliary epithelial cells (BECs), which indicates a close association between microchimeric maternal cells and the BA lesion site. However, our additional phenotypic characterization using CD45 and cytokeratin staining with FISH for XX signals in 4 patients (patients 2, 6, 7,
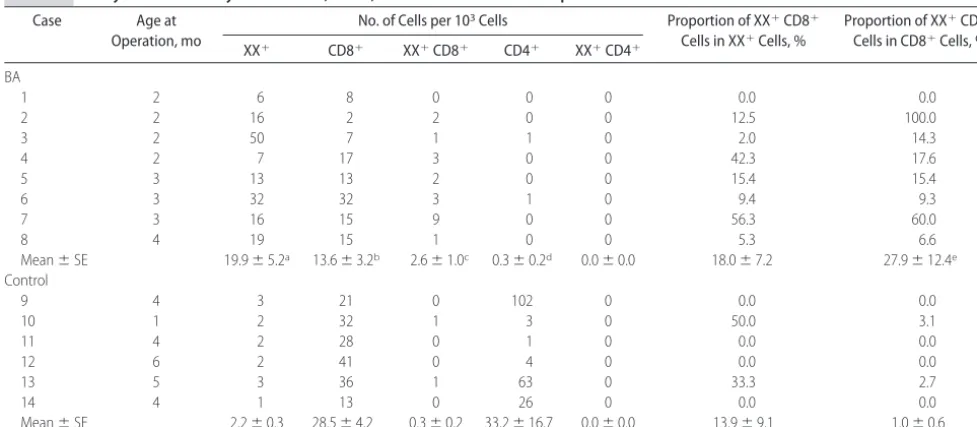
TABLE 1 Analysis of Maternally Derived XXⴙ, CD8ⴙ, and CD4ⴙT Cells in Liver Specimens From Patients With or Without BA
Case Age at
Operation, mo
No. of Cells per 103Cells Proportion of XX⫹CD8⫹
Cells in XX⫹Cells, %
Proportion of XX⫹CD8⫹
Cells in CD8⫹Cells, %
XX⫹ CD8⫹ XX⫹CD8⫹ CD4⫹ XX⫹CD4⫹
BA
1 2 6 8 0 0 0 0.0 0.0
2 2 16 2 2 0 0 12.5 100.0
3 2 50 7 1 1 0 2.0 14.3
4 2 7 17 3 0 0 42.3 17.6
5 3 13 13 2 0 0 15.4 15.4
6 3 32 32 3 1 0 9.4 9.3
7 3 16 15 9 0 0 56.3 60.0
8 4 19 15 1 0 0 5.3 6.6
Mean⫾SE 19.9⫾5.2a 13.6⫾3.2b 2.6⫾1.0c 0.3⫾0.2d 0.0⫾0.0 18.0⫾7.2 27.9⫾12.4e
Control
9 4 3 21 0 102 0 0.0 0.0
10 1 2 32 1 3 0 50.0 3.1
11 4 2 28 0 1 0 0.0 0.0
12 6 2 41 0 4 0 0.0 0.0
13 5 3 36 1 63 0 33.3 2.7
14 4 1 13 0 26 0 0.0 0.0
Mean⫾SE 2.2⫾0.3 28.5⫾4.2 0.3⫾0.2 33.2⫾16.7 0.0⫾0.0 13.9⫾9.1 1.0⫾0.6
Patients with BA received Kasai’s operation and those without BA received orthotopic liver transplantation; liver specimens were obtained at that time. The basic diseases in control cases were as follows: case 9, Crigler-Najjar syndrome; case 10, tyrosinemia; case 11, hemangioendothelioma; case 12, tyrosinemia; case 13, congenital biliary dilation; case 14, congenital absence of portal vein. aP⫽.0007, compared with patients without BA, by Mann-WhitneyUtest.
and 8) revealed that cytokeratin and CD45 were both detectable in 28% of 14 XX signal-positive cells counted. This XX-positive signal in cytokeratin-positive cells sug-gests that maternal cells might give rise to the transdif-ferentiated BECs in the fetus if they are circulating stem
cells13and might work as targets in autoalloimmune (or
host-versus-graft) responses, rather than GvHD. Because microchimeric maternal cells are basically thought to be immunologically tolerant to the fetus, the immunologic environment in patients with BA should be examined carefully. It was reported that immuno-competent maternal microchimeric cells could cause GvHD-like symptoms in patients with severe combined
immunodeficiency.14,15In addition, Landing et al16
char-acterized BA as one of the immunologic deficiency dis-eases of children attributable to the fact that the rapid progressive loss of Hassall’s corpuscles of the thymus
continues for ⬎18 months after birth. On the basis of
these previous observations and the existence of mater-nal microchimerism, we hypothesize that matermater-nal chi-meric cells could be involved in the pathogenesis of BA, acting in a role similar to a graft in a GvHD-like process. We verified this hypothesis with the 3 requirements necessary for graft-versus-host reaction that Billingham
formulated in 1966.17 (1) “The graft must contain
im-munologically competent cells” is satisfied by maternal
CD8⫹ effector cells being located in the biliary
epithe-lium. (2) “The host must be incapable of rejecting the transplanted cells,” and our study clarified that patients with BA have significantly high levels of bidirectional compatibility at HLA class I with their mothers (T.M., N.I., K.T., S.S., and Y.T., manuscript in preparation). Notably, because a HLA-compatible relationship be-tween mothers and fetuses is likely to be a key
determi-nant contributing to maternal microchimerism,18the
re-sults also indicate that patients with BA may have genetically favorable conditions for accepting maternal microchimeric cells. (3) “The host must express tissue antigens that are not present in the transplant donor” is satisfied by the fact that fetal major and minor histocom-patibility antigens are rarely identical to the HLA anti-gens found in the mother (graft) that could thus recog-nize the fetal BECs as a foreign element. Even HLA-identical stem cell transplants can induce GvHD because
of the presence of minor histocompatibility antigens.19
Because it seems to satisfy the 3 criteria described by
Billingham,17 BA can be seen as a phenotype of the
GvHD-like response caused by maternally transferred chimeric T cells.
Studies on human autoimmune diseases, including
juvenile idiopathic inflammatory myopathies,20 type 1
diabetes mellitus,21 and scleroderma,22,23 have clarified
an association with increased fetomaternal or ma-ternofetal microchimerism. Similarly, mama-ternofetal allo-autoimmune or autoalloimmune mechanisms might un-derlie the pathogenesis of BA. This concept of a new disease spectrum called maternofetal immune disease does not contradict the previously proposed etiologic considerations, such as viral infections or the ductal plate
malformation theory.24The viruses responsible may not
necessarily be specific, because common hepatotrophic
viruses would be sufficient to activate the immunologic competency of the BECs to secrete inflammatory cyto-kines, which would make BECs more susceptible to T cell attack.25
ACKNOWLEDGMENTS
This work was supported by research grant C from Kan-sai Medical University.
We thank Kumiko Hayashi, Kyoto Laboratory, Mit-subishi Kagaku, for her contribution to FISH prepara-tion.
REFERENCES
1. Sokol RJ, Mack C. Etiopathogenesis of biliary atresia. Semin Liver Dis.2001;21(4):517–524
2. Perlmutter DH, Shepherd RW. Extrahepatic biliary atresia: a disease or a phenotype?Hepatology.2002;35(6):1297–1304 3. Muraji T, Hashimoto K, Ifuku H, et al. Increased expression of
HLA-DR antigen on biliary epithelium cells in biliary atresia.
J Jpn Soc Pediatr Surg.1988;24(4):793–796
4. Kobayashi H, Puri P, O’Brian S, et al. Hepatic overexpression of MHC class II antigens and macrophage-associated antigens (CD68) in patients with biliary atresia of poor prognosis.J Pe-diatr Surg.1997;32(4):590 –593
5. Davenport M, Gonde C, Redkar R, et al. Immunohistochemis-try of the liver and biliary tree in extrahepatic biliary atresia.
J Pediatr Surg.2001;36(7):1017–1025
6. Schweizer P, Petersen M, Jeszberger N, et al. Immunohisto-chemical and molecular biological investigations regarding the pathogenesis of extrahepatic biliary atresia.Eur J Pediatr Surg.
2003;13(1):7–15
7. Mack CL, Tucker RM, Sokol RJ, et al. Biliary atresia is associ-ated with CD4⫹Th1 cell-mediated portal tract inflammation. Pediatr Res.2004;56(1):79 – 87
8. Suskind DL, Rosenthal P, Heyman MB, et al. Maternal micro-chimerism in the livers of patients with biliary atresia. BMC Gastroenterol.2004;4:14 –18
9. Kobayashi H, Tamatani T, Tamura T, et al. Maternal microchi-merism in biliary atresia.J Pediatr Surg.2007;42(6):987–991 10. Starzl T, Demetris AJ, Murase N, Ildstad S, Ricordi C, Trucco M.
Cell migration, chimerism and graft acceptance.Lancet.1992; 339(8809):1579 –1582
11. Lo DYM, Lo ESF, Watson N, et al. Two-way cell traffic between mother and fetus: biologic and clinical implications. Blood.
1996;88(11):4390 – 4395
12. Shinkai M, Shinkai T, Puri P, Stringer M. Elevated expression of IL2 is associated with increased infiltration of CD8⫹T cells in
biliary atresia.J Pediatr Surg.2006;41(2):300 –305
13. Ko¨rbling M, Katz RL, Khanna A, et al. Hepatocytes and epi-thelial cells of donor origin in recipients of peripheral-blood stem cells.N Engl J Med.2002;346(10):738 –746
14. Grogan TM, Broughton DD, Doyle WF. Graft-versus-host reaction: a case report suggesting GVHR occurred as a result of maternofetal cell transfer.Arch Pathol.1975;99(6):330 –334 15. Mu¨ller SM, Ege M, Pottharst A, Schulz AS, Schwarz K,
Friedrich W. Transplacentally acquired maternal T lympho-cytes in severe combined immunodeficiency: a study of 121 patients.Blood.2001;98(6):1847–1851
16. Landing BH, Yutuc IL, Swanson VL. Clinicopathological corre-lations in immunologic deficiency diseases of children with emphasis on thymic histologic patterns. In:Immunodeficiency: Its Nature and Etiological Significance on Human Diseases: Proceedings
of the International Symposium on Immunodeficiency. Tokyo,
17. Billingham RE. The biology of graft versus host reactions.
Harvey Lect.1966;62:21–78
18. Berry SM, Hassan SS, Russell E, Kukuruga D, Land S, Kaplan J. Association of maternal histocompatibility at class II HLA loci with maternal microchimerism in the fetus.Pediatr Res.2004; 56(1):73–78
19. Goulmy E, Schipper R, Blokland E, Falkenburg F. Mismatches of minor histocompatibility antigens between HLA-identical donors and recipients and the development of graft-versus-host-disease after bone marrow transplantation.N Engl J Med.
1996;334(5):281–285
20. Artlett CM, Ramos R, Jiminez SA, Patterson K, Miller FW, Rider LG. Chimeric cells of maternal origin in juvenile idio-pathic inflammatory myopathies: Childhood Myositis Hetero-geneity Collaborative Group. Lancet. 2000;356(9248): 2155–2156
21. Nelson JL, Gillespie KM, Lambert NC, et al. Maternal micro-chimerism in peripheral blood in type 1 diabetes and pancre-atic isletcell microchimerism.Proc Natl Acad Sci USA.2007; 104(5):1637–1642
22. Nelson JL, Furst DE, Maloney S, et al. Microchimerism and HLA-compatible relationship of pregnancy in scleroderma.
Lancet.1998;351(9102):559 –562
23. Johnson KL, Nelson JL, Furst DE, et al. Fetal cell microchimer-ism in tissue from multiple sites in women with systemic sclerosis.Arthritis Rheum.2001;44(8):1848 –1854
24. Tan CEL, Driver M, Howard ER, Moscoso GJ. Extrahepatic biliary atresia: a first-trimester event? Clues from light micros-copy and immunohistochemistry. J Pediatr Surg.1994;29(6): 808 – 814
25. Reynoso-Paz S, Coppel RL, Mackay RL, et al. The immunology of bile and biliary epithelium.Hepatology.1999;30(2):351–357
RATING YOUR DOCTOR, FAIRLY
“The drive to give consumers more information about the quality of their doctors has gotten an important shove forward by New York’s attorney general, Andrew Cuomo. That could be good for patients in dozens of states across the country that are served by some of the major health insurance companies. An investigation by Mr. Cuomo’s office found that various doc-tor-rating systems currently used or planned by insurers are based primarily on the cost of care, not its quality. Doctors may be awarded a grade or stars much like a restaurant or movie review, if they routinely treat sick patients for less than their competitors do. With that information, employers are able to steer their workers to lower-cost doctors by reducing deductibles or co-payments for those who patronize them. Unfortunately, insurers seldom make clear just how they come up with their ratings, and there is no guarantee that the cheapest doctors are necessarily the best choice. Now the attorney general’s office has negotiated agreements with several major health insurers, including Aetna, Cigna, UnitedHealthcare, and Empire Blue Cross/ Blue Shield, that should make the ratings systems more useful to consumers and fairer to doctors. Under the agreements, if insurers rate doctors, they cannot rely solely on cost but must also include quality as measured by national standards and guidelines. They have to make public what factors are included in their ratings and reveal how much weight they gave to cost in any composite score. An independent monitoring organization, approved by the attorney general, must oversee the process.”
DOI: 10.1542/peds.2007-0568
2008;121;517
Pediatrics
Tanaka, Yasutsugu Takada, Seisuke Sakamoto, Hironori Haga and Susumu Ikehara
Toshihiro Muraji, Naoki Hosaka, Naoki Irie, Makiko Yoshida, Yukihiro Imai, Kohichi
Quantification and Phenotypes of Maternal Cells in the Liver
Maternal Microchimerism in Underlying Pathogenesis of Biliary Atresia:
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/3/517
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/3/517#BIBL
This article cites 24 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/hepatology_sub
Hepatology
http://www.aappublications.org/cgi/collection/gastroenterology_sub
Gastroenterology
http://www.aappublications.org/cgi/collection/neonatology_sub
Neonatology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-0568
2008;121;517
Pediatrics
Tanaka, Yasutsugu Takada, Seisuke Sakamoto, Hironori Haga and Susumu Ikehara
Toshihiro Muraji, Naoki Hosaka, Naoki Irie, Makiko Yoshida, Yukihiro Imai, Kohichi
Quantification and Phenotypes of Maternal Cells in the Liver
Maternal Microchimerism in Underlying Pathogenesis of Biliary Atresia:
http://pediatrics.aappublications.org/content/121/3/517
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.