ON LEVELS OF PHYSICAL PERFORMANCE,
MOBILITY AND FALLS EFFICACY AMONG
ELDERLY IN POONGUDIL OLD
AGE HOME, AT POOVANTHI
Reg No: 3016118552
A DISSERTATION SUBMITTED TO THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY, CHENNAI, IN PARTIAL FULFILMENT
OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE IN NURSING
ON LEVELS OF PHYSICAL PERFORMANCE,
MOBILITY AND FALLS EFFICACY AMONG
ELDERLY IN POONGUDIL OLD
AGE HOME, AT POOVANTHI
Reg No: 3016118552
Signature of the Signature of the
This is to certify that the dissertation entitled “EFFECTIVENESS OF TAILORED EXERCISE PROGRAM ON LEVELS OF PHYSICAL PERFORMANCE, MOBILITY AND FALLS EFFICACY AMONG ELDERLY IN POONGUDIL OLD AGE HOME, AT POOVANTHI” is submitted to the faculty of Nursing, The Tamilnadu Dr. M. G. R. Medical
University, Chennai, by Mrs.Jothimalar M.Sc (N) II Year in partial fulfilment of the requirement for the degree of Master of Science in Nursing. It is the bonafide
work done by her and the conclusions are her own. It is further certified that this
dissertation (or) any past thereof has not formed the basis for award of any degree,
diploma (or) any title.
Prof. H. Ummul Hapipa, M.Sc(N)., Principal,
LEVELS OF PHYSICAL PERFORMANCE, MOBILITY AND
FALLS EFFICACY AMONG ELDERLY IN POONGUDIL OLD
AGE HOME, AT POOVANTHI.
APPROVED BY THE DISSERTATION COMMITTEE ON SEPTEMBER 2017
RESEARCH GUIDE :
Prof.H. Ummul Hapipa, M. Sc (N), Principal,
RASS Academy College of Nursing, Poovanthi, Sivagangai Dist-630611.
CLINICAL SPECIALITY EXPERT :
Mrs.M. Kavitha, M.sc. (N), Associate Professor
Medical Surgical Nursing,
RASS Academy College of Nursing, Poovathi, Sivagangai Dist-630611.
MEDICAL EXPERT :
Dr.S. Karthikeyan, M.D.,
Accident Emergency, MHM, FICM IRCU Consultant, Meenakshi Mission Hospital & Research Centre
Madurai
A DISSERTATION SUBMITTED TO THE TAMILNADU DR.M.G.R. MEDICAL UNIVERSITY, CHENNAI, IN PARTIAL FULFILMENT
OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE IN NURSING
First I thank from the deepest of my heart to my Lord and give all glory and honour for his never failing love and grace and blessing that enabled me to complete this study successfully.
I would like to extend my sincere thanks to Mr.C.Ravisankar, Chairman, RASS Academy College of Nursing, Poovanthi for his support and for providing required facilities for successful completion of this study.
I extend my heartfelt and sincere thanks to my research Prof. H. Ummul Hapipa, M.sc(N), Principal, RASS Academy college of Nursing, Poovanthi for a deniable work, interest, cheerful approach, always with never ending willingness to provide expert and suggestion to would this study to the present form.
I wish to express my sincere gratitude to the Dr.S. Karthikeyan, M.D., IRCU Consultant, Meenakshi Mission Hospital & Research Centre, Madurai for giving permission to conduct study and her guidance, and encouragement in making this study a success.
I express my special thanks and humble regard to guide Associate Prof. M. Kavitha, M. Sc (N), Dept. Of Medical surgical Nursing, RASS Academy
College of Nursing, Poovanthi for her guidance, support, motivation, interest and valuable suggestions and untiring help to would this study in successful way.
My deep sense of gratitude to Associate Prof. Mrs.Karthiga, M.Sc (N).,HOD Community Health Nursing, Associate Prof. Visalachi, M.Sc.(N)., HOD of Medical Surgical Nursing , Associate Prof. Mrs. Sudha, M.Sc.(N) ., HOD of Obstetrics and Gynaecological Nursing, Associate Prof.Miss. Nancy Flamina, M.Sc (N)., HOD of Mental health Nursing , Associate Prof. Mrs. Selvalakshmi, M.Sc (N)., HOD of child health nursing, Lect. Mrs. Murugeswari, M.Sc (N)., Department of mental health
nursing, lect. Mrs. Cithradevi, M.Sc (N)., Department of child health nursing Lect. Mrs. Selvi, M.Sc. (N)., Department of mental health nursing, RASS Academy
the statistical analysis of the data which is core of the study.
I extend my special thanks to class co-ordinator Associate Prof. Miss. Nancy flamina, M.Sc(N)., HOD of mental health nursing, RASS Academy college of nursing, poovanthi for their encouragement and support all through mu ups and downs during my study
My profound thanks to staff, Poongudil old age home, for their help and support. I am thankful to Mrs. Jothimani, Librarian, RASS Academy College of Nursing, for her continuous help in finishing this work successfully.
My sincere thanks to all the faculties of Nursing Department and Administrative Department, RASS Academy College of Nursing for their help throughout the study.
I would like to acknowledge the immense help and moral support extended to me by all my friends, classmates and to all of them whomsoever prayed for my successful completion of project.
CHAPTER TITLE PAGE NO ABSTRACT
I INTRODUCTION 1
Background of the study 1
Need for the study 3
Statement of the problem 7
Objectives of the study 7
Hypothesis 8
Operational definitions 8
Assumption
Delimitations 9
Projected outcomes 9
Conceptual framework 9
II REVIEW OF LITERATURE 13
III METHODOLOGY 23
Research Approach 23
Research Design 23
Variables under the study 24
Setting of the study 24
Study Population 24
Sample Size 24
Sampling Technique 24
Criteria for Sample Selection 24
Development and Description of the tool 25
Pilot Study 29
Procedure for Data Collection 29
Plan for Data Analysis 29
Protection of Human Rights 30
IV ANALYSIS AND INTERPRETATION
OF DATA
31
V DISCUSSION, SUMMARY,
CONCLUSION, IMPLICATIONS, LIMITATIONS &
RECOMMENDATIONS
52
REFERENCES 60
TABLES TITLE PAGE NO
1 Research Design 23
2 Distribution of the samples according to their demographic profile
32
3
Distribution of samples based on the pre and post test level of physical performance, mobility and falls efficacy
38
4
Comparison of pre and post test mean level of physical performance, mobility and falls
efficacy.
42
5
Association between pre test level of physical performance and the selected demographic variables.
46
6 Association between pre test level of elderly mobility and the selected demographic variables.
48
7 Association between pre test level of falls efficacy and the selected demographic variables.
FIGURE TITLE PAGE NO 1 Conceptual framework Based on Ernestine widenbach-
helping art clinical nursing theory
12
2 Distribution of the Samples according to their age 34
3 Distribution of the Samples according to their sex 34
4 Distribution of the Samples according to their history of co-morbid illness
35
5 Distribution of the Samples according to their history of previous fall
35
6 Distribution of the Samples according to their frequency of previous fall
36
7 Distribution of the Samples according to their time of previous fall
36
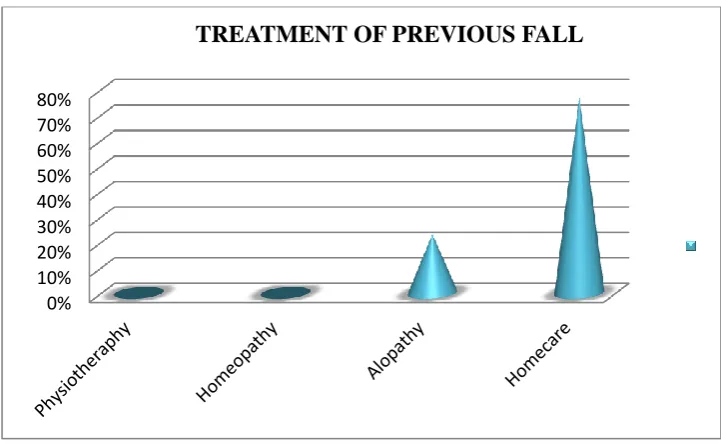
8 Distribution of the samples according to their treatment of previous fall
37
9 comparison between pre and post test level of physical performance
40
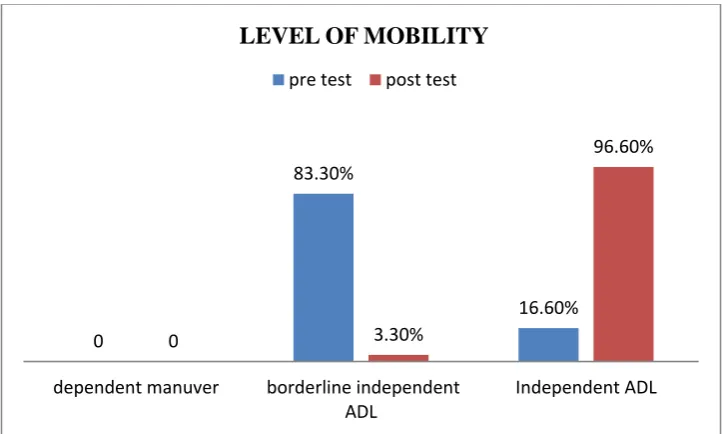
10 comparison between pre and post test level of mobility 40
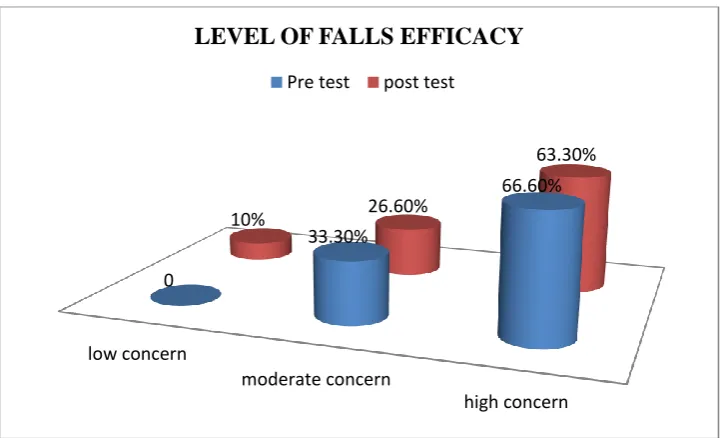
11 comparison between the pre and post test level of falls efficacy
41
12 comparison between the pre and post test mean level of physical performance
44
13 comparison between the pre and post test mean level of mobility
44
14 comparison between the pre and post test mean level of falls efficacy
APPENDIX TITLE PAGE NO
I Tool 64
Section A-Demographic Data of the Subjects.
Section B -Falls efficacy scale 65
Section C-Modified Physical performance Scale 66
Section D -Elderly mobility Scale 68
II
Tailored Exercise program(Flexibility, Balance and Strengthening exercise
70
III Copy of Certification of Ethical committee 87
IV Permission Letter to conduct the study 89
V List of Experts consulted for content validity 90
Effectiveness of tailored exercise program on levels of physical performance , mobility and falls efficacy among elderly in a old age home, Poovanthi was undertaken by Reg.No :301611852 during the year 2017-2018 in partial fulfilment of the requirement for the degree of Master of Science in Nursing at RASS Academy college of Nursing, Poovanthi. Which is affiliated to The Tamilnadu Dr.M.G.R. Medical University ,Chennai.
CHAPTER - I
INTRODUCTION
“Aging is not lost youth but a new stage of opportunity and strength.”
(Betty friedan) Background of the study
“Human Being" has a definition of a man, woman, or child of the
species Homo sapiens, distinguished from other animals by superior mental
development, power of articulate speech, and upright stance. This is what a human
being is (Prateek Surya Prakash, 2015)
The human life span can be split into a number of stages: infancy, childhood,
adolescence, young adulthood, adulthood, and old age. The lengths of these stages,
however, have varied across cultures and time periods. (Wilson, E.O, 2002)
Aging is defined as “the chronological process of growing physically older. However, there is also a social dimension in which chronology is less important than the meaning attached to the process. Different cultural values and social expectations apply according to gender and age group and therefore there are socially structured variations in the personal experience of aging” (Jarry ,1995)
"Getting old is not for sissies." No matter who we are — man, woman, rich
or poor — we all grow old. But the pace and precise way it happens varies from
person to person, depending on genetic and environmental factors. While someone’s
genetic makeup plays a huge part in determining his life expectancy, the quality of
health care received and a healthy lifestyle are significant contributors to longevity.
Nonetheless, dealing with the aging process is a challenge, and when it begins, the
impact is felt throughout the body — in the respiratory, cardiovascular, nervous,
musculoskeletal, and immune systems. And while an individual can age and remain
healthy, some ailments are directly linked to age-related change. Those conditions
include: Vision changes/cataracts, Hearing loss, Arthritis, Sleep changes/disorders,
Physiological changes in elderly refers to the physical changes an Individual experiences because of the decline in the normal functioning of the body resulting in poor mobility, vision, hearing, inability to eat and digest food properly, a decline in memory, the inability to control certain physiological functions and various chronic health problems.
Unstable gait and falls are serious issues in elderly since they lead to injury, restricted activities, increased indoor admissions and even deaths. Risk factors for the repeated falls in elderly are poor muscle strength, cerebellum/basal ganglia involvement, hypoglycemia in diabetes and postural hypotension (mostly drug induced or autonomic) in hypertension and peripheral neuropathies. Preventive strategies for falls need comprehensive medical, rehabilitative and environmental interventions.
Falls, defined as an unintended event that results in change of the starting position of the individual to the same level or lower, are an important cause of mortality, morbidity, disability, and hospitalizations in the elderly population. A situation was observed within this population: women are the ones who fall the most; 30% fall at least once a year and, out of these, 50% fall very often. (Gianluca, Isabela, Marcos,2017).
Fear of falling is a defined geriatric syndrome that may contribute to further functional decline in an already frail patient. When people experience something unpleasant, their natural response is an aversion to that experience. People may begin to limit their activities after a fall or as they become weaker and less agile with increasing age. This leads to a more sedentary lifestyle and physical atrophy, which further predisposes them to falls. (Aimee ,Kuo-wei,Peter Khang, 2013)
Fall-related injuries are more common among older persons and are a major cause of pain, disability, loss of independence and premature death. Injuries are the sixth leading cause of death in adults of 65 years of age or more and falls are the leading cause of such injuries. (Waleed Al-Faisal,2006)
environment and/or of the activity being undertaken. Targeted exercise aimed at improving the physical ability of the individual, such as balance and strength training, is crucial for promoting functional independence and mobility and reducing the risk of falling in older age. Exercise programs that provide a high challenge to balance, have a high dose, include progression of intensity over time and are ongoing are most effective for preventing falls.
Iindividually-tailored exercise programs that target known intrinsic risk factor also appear to be most effective for frail older adults who are advanced in age (> 80 years) and at high risk for falls (i.e., injury-related fall within past six months, presence of two or more risk factors associated with falls, including co-morbid conditions that are less medically stable). A health-care professional who can tailor the type of exercise to the specific needs and abilities of the individual generally supervises these types of programs. The initial focus in these types of exercise programs should be on strengthening all major muscle groups in a seated or supported standing position until sufficient strength permits the inclusion of unsupported standing exercises that emphasize dynamic balance and mobility. In addition to the improvements in physical capacity gained, these programs also positively impact the individual’s perceived quality of life. For older adults at high risk for falls, physical activity serves a tertiary role by raising their physical capacity to a level that will allow for greater independence in the performance of essential activities of daily living (i.e., dressing, bathing, transfers) and require less assistance with more advanced activities of daily living (e.g., shopping, walking in the community, assorted household chores). (Debra J. Rose,2002).
This study provided guidance to older people regarding the safe and effective provision of programs aimed at improving strength and balance and preventing falls in older age.
Need for the study
420 million in 2000 to 974 million in 2030. At present nearly 60%of older adults reside in the developing countries. In India, there has been a sharp increase in the number of elderly (60 years and older):6.4% of total population of 1.21 billion (2011 census). According to 2011 census, elderly (65 years and above ) constitute 5.3% of total population (male 29,364,920 and Female 3,291,030). The likely number of elderly by 2016 will be around 113 million (10-112%of entire population), and it is projected that by the year 2050, the number of elderly would be about 324million.Falls are one of the major problems in the elderly and are considered one of the “Geriatric Giants”. Recurrent falls are an important cause of morbidity and mortality in the elderly and are a marker of poor physical and cognitive status. .(Lewis, 2015).
Older people frequently fall. From 30 to 40 percent of community-dwelling adults older than 65 years fall each year. Rates are higher in nursing home resident and hospitalized patients. The incidence of falls rises steadily from middle age and peaks in persons older than 80 years. Between 20 and 30 percent of older adults who fall suffer serious injuries such as hip fractures and head trauma. The most prevalent fall-related injuries among older adults are fractures of the hip; spine; upper arm; forearm; and bones of the pelvis, hand, and ankle. Of these, the most serious injury is hip fracture, a leading cause of morbidity and excess mortality among older adults. During 1988-1996, the estimated number of hospital admissions for hip fracture increased from 230,000 to 340,000. In 1996, 80% of the admissions for hip fracture occurred among women (3). From 1988 to 1996, hip fracture hospitalization rates for women aged >65 years increased 23% Recovery from falls often is complicated by poor quality of life caused by restricted mobility, functional decline, and increased risk for nursing home.( Waleed Al-Faisal,2006)
are associated with falls in persons above 70 years of age and is associated with greater mortality.
In a Multi-centric Community Study, evaluating Health Problems in the Elderly (Year 2010), in 10 states across India, covering a total population of 10,200 elderly with equal rural and urban distribution, the incidence of falls (History of a single fall in the last 6 months) was found to be 14% (Data to be published).Among the 35 states and union territories in India, Kerala has registered the highest proportion of elderly. The aged in Kerala constitute 11% of the population. Between 30 years, there has been 160% increase in the population of older adults, the majority of them being women. Their population, which was 9% , is expected to increase to 37% by 2051.The Kerala Aging Survey (KAS), conducted among more than 5,000 elderly (2,271 men and 2,722 women) in 14 districts of Kerala, was the keystone of the study. The results of the survey have shown that the age of participants ranged 5 from 60 to over 100 years of age with 54% being women. The results of the study show that falls and fractures are a significant issue among older adults. (Usha.G , Krishnaswamy.B 2011)
Muscle weakness is a common impairment in older adults, it therefore is not surprising that these conditions frequently co-exist in the elderly. Skeletal muscles produce all voluntary human movement. Changes in properties and performance of muscles can profound affect an older person’s ability to walk and function independently. Loss of muscle strength might be particularly problematic for an older person with who has pain, stiffness and mechanical changes to their joint that complicate their ability to mobility and make them particularly vulnerable to small changes in their physical status. Strength training has been the focus of a great deal of recent clinical research in many populations, including older adults. While the benefits of strength training have been well explored in reviews focused on both populations, there has been little attention paid to the benefits and risks of strength training when undertaken by old people. There is also evidence that strength training improves mobility (i.e. increased gait speed), simple functional tasks (i.e. standing up from a chair) and self- rating daily function in older adults.
As the population ages, the problems related to falls and fractures are expected to grow. Meeting these challenges requires a clear understanding of the prevalence and nature of falls, innovative planning to develop prevention programmes, systems and structures which will support falls prevention initiatives, and substantial reforms and policies at the local and national levels. In many developing countries including India, Fall events resulting in fractures is not recognised as a preventable risk factor. Responding to the caution of world experts and addressing the issue will avert the burden of fall related fractures. Several promising strategies such as exercise programmes, environmental modification, and other educational opportunities for preventing falls and fractures exist.
risk-factor modification and multi-factorial interventions, and have found that both can prevent falls in older patients . (Waleed Al-Faisal,2006)
Physical activities that stimulate the multiple dimensions of balance should be the foundation of any structured exercise program aimed at reducing fall risk. Activities designed to improve the older adults’ ability to process and integrate sensory information, anticipate and/or react quickly and efficiently to changes in task demands and/or the environment, allocate attention appropriately, and perform multi-directional and segmental coordination activities in a controlled manner will be particularly important components of such a program25, 26. Including whole body functional activities that focus on improving muscular endurance, strength, and power, particularly in the muscle groups that contribute to postural alignment and stability during gait (e.g., ankle, knee, hip, and trunk) are also important for maintaining a high level of physical function. (Debra J. Rose, 2002).
Investigator has observed several patient verbalize their fear of falls, and inability in physical performance and mobility level in her personal experience. Hence, the nvestigator felt the need for Exercise program for Elderly people. As the investigator inspired by review of several studies, she was motivated to conduct the study on effectiveness of tailored exercise program on improvement in the level of physical performance, mobility and reduce the level of falls efficacy among elderly people.
Statement of the problem
Effectiveness of tailored exercise program on levels of physical performance, mobility and falls efficacy among elderly in poongudil old age home, Poovanthi.
Objectives:
To assess the level of physical performance, mobility and falls efficacy before tailored exercise program among elderly.
To evaluate the effectiveness of tailored exercise program on the level of physical performance, mobility and falls efficacy among elderly.
Hypothesis
H1: There is a significant difference in levels of physical performance, mobility and falls efficacy before and after tailored exercise program.
H2: There is a significant association between pre test level of physical performance, mobility and falls efficacy and the selected demographic variables.
Operational definitions: Effectiveness:
The significant difference in the levels of physical performance, mobility and falls efficacy before and after tailored exercise program.
Tailored Exercise Program:
Individually tailored exercise is define as home based, strength and balance retaining programme, where resistance to lower limb muscles was provided via ankle cuff weights and the programme was carried out at leastthree times per week in 30 minutes.
Flexibility exercise:
Flexibility is the range of motion in the joints and the ability of joints to move freely.
Balance exercise:
Balance exercises can help to maintain the balance and confidence of important to prevent falls and maintain the independence.
Strengthening exercise:
Physical performance:
It refers to the ability to perform a physical task in day today activities assessed before and after the intervention measured by Brown’s Modified Physical Performance Scale.
Mobility:
It refers to the capability to move in ones environment with ease and without restriction and walking aids which is measured by Smith’s Elderly Mobility Scale.
Falls efficacy:
It refers to the beneficial change of elderly about their possibility of preventing fall as measured by Tinette’s falls efficacy scale.
Elderly:
It refers to the persons who are aged 60 and above.
Old age home:
It refers to the place where elderly people are assisted care and supervised.
Delimitation:
The study is limited to Elderly who are,
Aged 60 and above
Residing at Poongudil old age home Projected outcomes:
The study will reveal the importance of given tailored exercises on the level of physical performance, mobility and falls efficacy .
Conceptual Framework
objectives of the study. Based on the theory, it’s schematic representation of the steps, activities and outcome of the study.
The conceptual framework of this study was based on Wiedenbach’s helping art of clinical nursing theory. Ernestine wiedenbach’s views this theory as a set of interrelated concepts that gives systematic view of a phenomenon that is explanatory and predictive in nature. The present study was aimed to help the tailored exercise programme. According to the theorists the practice of nursing comprises a wide variety of services each directed towards the attainment of one of its components.
STEP 1-IDENTIFYING THE NEED FOR HELP:
In identifying the need, the nurse perceives the patient as consistent or inconsistent, collect the information and identifying the need for help. There are two components in identifying the need for help.
a) General information
This comprises of collecting the information to identify the need. In this study the investigator assessed the general information which includes the demographic variables, level of physical performance, level of mobility, and level of falls efficacy among elderly living in old age home.
b) The central purpose
It refers to what the investigator wants to accomplish. Here the central purpose are to improve the level of physical performance, level of mobility and reduce the level of falls efficacy among elderly.
STEP 2- MINISTERING THE NEED FOR HELP.
Realities : It refers to physical, physiological, emotional and spiritual factors that come in play with situation involving the nursing action. Wiedenbach’s defines the five realistic which include:
a) Agent:
b) Recipient:
The recipient is the one who receives nursing action. In the present study the recipients are the elderly residing in old age homes.
c) Goal:
The goal is the nurse’s desired outcome it is similar to the central purpose which is to improve the level of physical performance, mobililty and reduce the level of falls efficacy.
d) Means:
They are the activities through which the investigator aims the goal. It includes skill, techniques, procedures and devices that may be used to facilitate nursing practice. Here it refers to the exercise that is done by the elderly in the presence of the researcher.
e) Framework:
It refers to the facilities in which is practice. The frame work in this study has been considered as old age home, Poovanthi in which the study has been conducted.
Reassessment - If there was no improvement in the level of physical performance, mobility and reduce the level of falls efficacy the investigator recommended the reassessment.
Enhancement - If there was improvement in the level of physical performance, mobility and reduce the level of falls efficacy, enhancement of the intervention will be carried out.
STEP 3-VALIDATING THE NEED HELP WAS MET.
CHAPTER – II
REVIEW OF LITERATURE
The extensive review was made to strengthen the prevent study in order to lay down the foundation which help us to reveal the prevailing situation of the similar studies in different areas. The related literature of this study was presented in the following sessions.
1. Literature related to the level of physical performance among elderly. 2. Literature related to the level of mobility among elderly.
3. Literature related to the level of fall efficacy among elderly.
4. Literature related to other therapeutic exercises to improve the physical performance, mobility and falls efficacy among elderly.
5. Literature related to tailored exercise programme on the level of physical performance, mobility and falls efficacy among the elderly.
Literature related to the level of physical performance among elder
Nicola Veronese et. al., (2016) conducted study to assess the comparison of objective physical performance tests and future mortality in the elderly people. Among 3,099 odler community-dwelling participants included in the progetto Veneto anziani study,2,096 were followed for a mean of 4.4years. physical performance tests measured were short physical performance battery(SPPB),4-meter gait speed, chair stands time, leg extension and flexion, handgrip strength, and 6- minutes walking (6MWT), outcome was mortality assessed with death certificates. Participants who died during the follow-up (n=327) scored significantly worse in all physical performance tests measured at baseline than those who survived (n=1,769). Using a Harrell’s C-index, the highest C-index was observed for 6MWT in men (C-index=0.735;95%confidence interval :0.701-0.770, p< .0001) and SPPB in women (C-index =0.781;95% CI:0.740-0.822, p=.0009).
measured 6- min walk test, grip –strength, 30-sec chair stand test, 8 foot Up-and Go, back scratch, chair sit and reach, unipedal stance, BMI and the frailty with questionnaire. The collected data were analyzed by descriptive statistics, frequencies, correlation analysis, ANOVA, and simple liner regression using the IBM 21. SPSS program. In results, statistic tests showed that there were significant differences between frailty and 6-min walk test, 30-sec arm curl test , 30-sec chair stand test, grip-strength, back scratch, and BMI.
Rob C. Van Lummel et. al., (2015) conducted study to assess the associating between physical performance and physical activity in older adult: associated but separate domains of physical function in old age. In 49 older participants (83+7years; M+SD), performance based tests were conducted and physical activity was measured for one week. Activity monitor data were reduced in terms of duration, periods, and mean duration of periods of lying, sitting, standing and locomotion. The relation between and within physical performance scores and physical activity outcomes were analysed using rank order correlation and factor analysis. Factor structure after varimax rotation revealed two orthogonal factors explaining 78%of the variance in their data; one comprising all physical activity variables and one comprising all physical performance variables. Physical performance scores correlated moderately with physical activity in daily life.
Literature related to level of mobility among the elderly:
screening questions stratified this population to three meaningful mobility limitation levels. Higher levels of mobility limitations were strongly associated with negative health outcomes. Mobility-enhancing interventions could promote successful aging.
Ashari Asmidawati, et. al., (2014) conducted study to improve turning and mobility performance among community dwelling older adults. Study participants will be aged 50 years and above, living in the community and have been identified as
having impaired turning ability [outside of age and gender normal limits on the Step
Quick Turn (180 degree turn) task on the Neurocom® Balance Master with long
plate]. After a comprehensive baseline assessment, those classified as having balance
impairment while turning will be randomized to intervention or control group. The
intervention group will receive a 16 week individualized balance and strength home
exercise program, based on the Otago Exercise Program with additional exercises
focused on improving turning ability. Intervention group will attend four visit to the
assessment centre over 16 weeks period, for provision, monitoring, modification of
the exercise and encourage ongoing participation. Participants in the control group
will continue with their usual activities. All participants will be re-assessed on
completion of the 16 week program. Primary outcome measures will be the Step
Quick Turn Test and Timed-Up and Go test. Secondary outcomes will include other
clinical measures of balance, psychological aspects of falls, incidence of falls and
falls risk factors.Results of this study will provide useful information for clinicians
on the types of exercises to improve turning ability in older people with increased
falls risk and the effectiveness of these exercises in improving outcomes.
in nursing homes ( p < 0.05). However, no statistically significant difference could be found between the BI and RMI values (p > 0.05). A statistically significant relationship was found between the NHP and TUG, RMI BIand the use of assistive devices in daily life activities (p < 0.05).
Literature related to level of falls efficacy among elderly:
Kim Delbaere, et. al., (2010) conducted study to identify the determinants of disparitites between perceived and physiological risk of falling among elderly people Classification tree analysis was used to split the sample into four groups (vigorous, anxious, stoic, and aware)based on the disparity between physiological fall risk in the vigorous (144(29%)) and aware (202(40%))group. The anxious group (54(11%)) had a low physiological risk but high perceived fall risk, which was related to depressive symptoms(p =0.029), neurotic personality traits (p = 0.026, and decreased executive functioning (p =0.010). the stoic group (100(20%)) had a high physiological risk but low perceived fall risk, which was protective for falling and mediated through a positive outlook of life(p =0.001)and maintained physical activity and community participation(p= 0.048).
Aniket sirohi (2017) conducted study to determine the prevalence of falls among elderly persons in a rural area and to study the association of falls with socio demographic variables and selected health conditions among 456 elderly persons in a rural area of Haryana falls, information regarding socio demographic details, selected health conditions, and history of falls in the past 12 months was recorded. Univariate analysis followed by stepwise multivariate logistic regression analysis was carried out. The effect of socio demographic and various health conditions on falls was analyzed using logistic regression analysis. Among the 456 study participants, the prevalence of falls in the past 12 months was 36.6% (95% confidence interval [CI] =32.1–40.0). The prevalence among women was 40.6% (95% CI = 34.5–46.7) and among men was 31.5% (95% CI = 25.0–37.9). Low socioeconomic status, urgency of micturition, knee pain, visual impairment, hearing impairment, functional disability, and depression were significantly associated with falls.
adults.458 community-dwelling adults aged ≥ 60 years underwent a comprehensive
geriatric assessment. Mean and variability of reaction time (RT), commission errors
and omission errors were recorded during a fixed version of the Sustained Attention
to Response Task (SART). RT variability was decomposed using the Fast Fourier
Transform (FFT) procedure, to help characterise variability associated with the
arousal and vigilance aspects of sustained attention. The number of self-reported
falls in the previous twelve months, and falls efficacy (Modified Falls Efficacy
Scale) were also recorded. Significant increases in the mean and variability of
reaction time on the SART were significantly associated with both falls (p < 0.01)
and reduced falls efficacy (p < 0.05) in older adults. An increase in omission errors
was also associated with falls (p < 0.01) and reduced falls efficacy (p < 0.05). Upon
controlling for age and gender affects, logistic regression modelling revealed that
increasing variability associated with the vigilance (top-down) aspect of sustained
attention was a retrospective predictor of falling (p < 0.01, OR = 1.14, 95% CI: 1.03
- 1.26) in the previous year and was weakly correlated with reduced falls efficacy in
non-fallers (p = 0.07).
Literature related to other therapeutic exercise among elderly:
Shuhei Yamamoto et. al., (2016) conducted study to assess the effects of resistance training on muscle strength , exercise capacity, and mobility in middle – aged and elderly patients with coronary artery disease: A meta-analysis. Twenty – two trials totalling 1095 participants were analyzed. Performed random-effects meta- analysis. In middle –aged participants, RT increased lower extremity muscle strength (standardized mean difference (SMD): 0.65, 95%confidence interval (CI):0.35to 0.95), upper extremity muscle strength (SMD: 0.73,95%CI:0.48 to 0.99) and peak oxygen consumption(VO2)(weight mean difference (WMD):0.92Ml/kg /min, 95%CI:0.12 to 1.72), but did not improve mobility compared with the control. In elderly participants, RT increased lower extremity muscle strength (SMD: 0.63, 95%CI: 0.56 to 1.80), and improved mobility (SMD: 0,61, 95% CI: 0.21 to 1.01) compared with the control.
people is characterized by a reduction of energy reserves and also by a decreased of resistance to stressors, resulting in an increase of vulnerability. Thirty-two pre-frail community –dwelling women participated in this study. Potential participants with cognitive impairment (MEEM), over extremities orthopaedic surgery, fractures, inability to walk unaided, neurological disease, acute inflammatory diseases, tumour growth, regular physical activity and current use of immune modulators were excluded. All participants were evaluated by a blinded assessor using: timed up and go (TUG),10-meter walk test (10MWT)and knee extensor muscle strength .the intervention consisted of strengthening exercise of the lower extremities at 70% of 1RM, three times/week for ten weeks. The statistical analysis was performed using the ANOVA and spearman tests. After the intervention, it was observed statistical significance on the work at 180/s (F=12.71, p =0.02), on the power at 180/s (F= 15.40, P=0.02) and on the functional capacity (TUG, F=9.54,p=0.01:TC10, F=3.80, p=0,01). There was a good negative anf statistically significant correlation between the TUG and work at 60/s, such as the TUG and work at 180/s (r=0.65, p=0.01;r=0.72,p=0.01) .
Hee Lee.sang-young et. al., (2014) conducted study to investigate whether lower limb strengthening exercise leads to improved lower limb strength and balance function for the elderly. Aging is associated with a progressive decline in overall muscle strength. Loss of lower limb strength leads to an increased risk of falls and a sedentary lifestyle. The purpose of this study was to investigate whether lower limb strengthening exercise leads to improved lower limb strength and balance function for the elderly. From a total of 74 respondents, 50 subjects were randomly assigned to either a training group (n = 30) or a control group (n = 20). The subjects ranged in age from 65 to 82 years. A randomized controlled trial compared the effects of strengthening exercise and balance function. Leg extension and lower curl exercises were performed during the 12-week study. After training, the lower limb strength and balance of the individuals in the training group had significantly improved compared to the baseline limb strength may lead to balance enhancement in neurologically intact older persons.
Minoru Yamada et. al., (2011) conducted study to assess the resistance
care physician within the previous 3 years, score of ≥8 by Rapid Dementia Screening
Test , able to walk independently, willing to participate in group exercise classes for
at least 6 months, We designed the effect size of the current study to be 0.4. With a
significance level of 0.05, a power of 80%, and a moderate effect size (0.4), a
minimum of 100 participants were needed in both the intervention and control
groups. Accounting for a potential 20% attrition rate, a total of 240 participants were
recruited for this study, which was deemed large enough to detect statistically
significant differences. We analysed the effects of resistance training on all outcome
measures using a mixed 2 (group: robust and frail groups) × 2 (time:
pre-intervention, post-intervention) ANOVA. A 0.05 type 1 error rate was chosen a
priori to indicate statistical significance. A post hoc paired t-test for within-group
comparisons was performed to compare each dependent variable. The Bonferroni
procedure was used to adjust the type 1 error rate of each analysis to 0.025 (0.05/2)
as an indication of statistical significance to guarantee an overall type 1 error rate of
0.05. Data were entered and analysed using the Statistical Package for Social
Science (Windows version 18.0). We screened 412 elderly and enrolled 337 (81.8%)
who met the inclusion criteria for the trial and agreed to participate (Figure 1A). Most of the elderly who did not meet the inclusion criteria (n = 66) were excluded
because they had exercised regularly for 6 months prior to the screening. Nine
people who might have been eligible for the study declined after telephone
screening. Of the 337 individuals who were enrolled in this study, 307 (91.1%)
completed the 12-month intervention along with the second interview and the tests at
the end of the study. Among them 148 in the robust group (93%) and 159 in the frail
group (89%) completed the study.
Literature related to tailored exercise programme on the level of physical performance, mobility and falls efficacy among the elderly:
performed the exercises on their own over a six-month period and recorded each exercise type, frequency, and number of repetitions .Physical therapists regularly assessed the patients’ reports and evaluated their muscle weakness via manual
muscle testing (MMT). They also monitored patient fatigue each month during a face-to-face interview and readjusted the exercise program anytime there was a marked increase in fatigue or a decline in muscle strength. The study also included data from 84 patients with ALS (matching the characteristics of the Home-Ex patients) who underwent supervised exercise with a physical therapist for six months. These were the controls. Researchers assessed patients’ Home-Ex outcomes using the ALS Functional Rating Scale-Revised (ALSFRS-R), which ranges from a score of 0 to 48. Higher scores indicate better function. A total of 15 patients out of 21 completed the six-month study period of home-based exercises. The results showed that patients in the Home-EX group had significant improvements in the total score of ALSFRS-R compared to controls – 38.1 vs. 33.1, respectively. The improvements were significant for the sub-parameter related to respiratory function, with Home-Ex patients scoring 11.8, compared to 10.5 in the control group.
Angelin Persis et. al., (2017) conducted study effectiveness of tailored exercise program on level of physical performance, mobility, falls efficacy among
elderly. A pre experimental study with one group pre and tailored exercise program
on level of physical performance, mobility and post test design using purposive
sampling technique was adopted to select 30 elderly old age home, Vellore. Brown’s
physical performance scale, Smith’s elderly mobility scale and tinette’s falls efficacy
scale were used. Tailored exercise (balance, strengthening and flexibility) were
given thrice a week for a period of 5weeks. The paired “t” value of physical
performance (3.3) was greater than the table value (2.76) which was statistically
significant at p <0.01 level. The paired “t” value of mobility (5.3) was greater than
the table value (3.66) which was statistically significant at p <0.001 level. The paired
“t” vale of falls efficacy (12.7) was greater than the table value (3.66) which was
statistically significant at p <0.001 level proving effectiveness of tailored exercise
program on physical performance, mobility and falls efficacy. The ‘Chi’ square
value of demographic variable of physical performance (history of falls, elderly
mobility (history of falls, period of falls) falls efficacy (BMI, education, co-morbid
Deepti Wadhwa, et. al., (2016) conducted study effectiveness of otago exercise program on reducing the fall in elderly: single case report. To find out the
effectiveness of Otago exercise on reducing the fall risk in elderly Single case study Out Patient Department and at home A single individual with fall risk participated in this study Interventions used in this study included Otago Exercise Program which included strengthening exercise, balance re-training and walking. The interventions were given for 8 weeks. The outcome measures were 30 Second Chair Stand Test, Four-Stage Balance Test, Timed Up and Go test and Berg Balance Scale. The outcome measures were taken on first day, last day of 4th week and 8th week. The scores of 30 Second Chair Stand Test, Four-Stage Balance Test, Timed Up and Go test and Berg Balance Scale were improved.
CHAPTER-III
[image:34.595.86.535.552.628.2]RESEARCH METHODOLOGY
This chapter explains the research methodology adapted by the researcher to study the effectiveness of tailored exercise program on the level of physical performance, mobility and falls efficacy among elderly in a selected old age home, Poovanthi. It includes research approach, research design, setting, population, sample, sampling technique, description of the the tool, pilot study, description of intervention, data collection procedure and plan for data analysis also dealt subsequently.
Research approach:
An quantitative approach was adopted by the investigator to find the effectiveness of tailored exercise program on levels of physical performance, mobility and falls efficacy.
Research design:
The investigator adopted pre experimental research design, one group pre test and post test design for this study. The diagrammatic representative of design is represented below.
Table 1
PRE TEST EXPERIMENT POST TEST
O1 X O2
O1 - pre test assessment of physical performance, mobility & falls efficacy.
O2 - Post test assessment of physical performance, mobility & falls efficacy.
Variables under the study:
In this study tailored exercise program was the independent Variable and the physical performance, mobility and falls efficacy was Dependent variable.
Setting of the study:
The study was conducted in a poongudil old age home, Poovanthi, which was located with in 2 kilo meters away from RASS Academy College of Nursing, Poovanthi, Sivagangai (Dt). Total population of this oldage home 72 persons, 18 bed ritterns, 4 under age of 60 years.
Study Population:
The study population comprised of elderly those who are residing in Poongudil old age home, Poovanthi, Sivagangai (Dt).
Sample
Elderly who fulfil the inclusion criteria was considered as a sample.
Sample size
Sample size was comprised of 30 elderly. Sampling techniques:
The investigator adopted non probability purposive sampling technique was used to select samples for the study.
Criteria for the study: Inclusive criteria: Elderly who are,
Aged 60 years and above
Available during the period of data collection
Willing to participate
Scoring more than 10/20 in mobility scale, 17/36 in physical performance scale and 20/64 in falls efficacy scale.
Exclusive criteria: Elderly who
Have musculo skeletal disorder
Have neurological disorder
Have total blindness
Have total deafness
Have gait and balance disorder
Use assistive device for activities of daily living
Affecting postural stability and movement disorder
Had injury or fracture within last 5 years. Description of the tool:
The tool contain Patient demography profile, physical performance scale, elderly mobility scale and falls efficacy scale.
Section A:
Section: B
Falls Efficacy scale:
Score interpretation:
16 – 19 - low concern about falls
20 – 27 - moderate concern about falls 28 – 64 - high concern about falls S.
No Subject
Not At All Concerned 1 Somewhat Concerned 2 Fairly Concerned 3 Very Concerned 4
1 Cleaning the house (e.g. sweep, vacuum or dust)
2 Getting dressed or undressed 3 Preparing simple meals
4 Taking bath or shower 5 Going shopping
6 Getting in and out of chair 7 Going up or downstairs 8 Walking around in the
neighbourhood
9 Reaching for something above your head or on the ground 10 Going to answer the telephone
before it stops ringing
11 Walking on a slippery surface [for example, wet or icy]
12 Visiting a friend or relative 13 Walking in a place with crowds 14 Walking on an uneven surface[for
example rocky ground, poorly maintained pavement]
15 Walking up or down a slope 16 Going out to a social event[for
Section: C
Physical Performance Test:
Score interpretation:
32/36 –36/ 36 - Indicates not frail 25/36 – 31/36 - Indicates mildly frail 17/36 – 24/36 - Indicates moderate frail
<17/36 – unlikely to be able to function in the community
1. Standing static Balance Feet together
(sec) Semi tandem (sec) Tandem (sec) Score (sec) 10s 10s 10s 10s __0-9s 10s 10s 10s __0-9s Unable __10s __3-9.9s __0-2.9s Unable Unable
__ 4 __ 3 __ 2 __ 1 __ 0
Time Scoring values Score
2. Chair rise <11 sec - 4
11.1 - 14sec - 3 14.1 - 17sec - 2 >17sec - 1 Unable - 0
3. Lift a book and put it on a
shelf
< 2sec - 4
2.1 - 4sec - 3 4.1-6sec - 2 >6sec - 1 Unable - 0
4. Put on and remove a
jacket
<10sec - 4
10.1-15sec - 3 15.1 - 20sec - 2 >20 sec - 1 Unable - 0
5. pick up a penny from
floor
< 2sec - 4
2.1 - 4sec - 3 4.1-6sec - 2 >6sec - 1 Unable - 0
6. Turn 360 degree Discontinuous steps - 0
Continuous steps - 2
Unsteady (grabs, staggers) - 0 Steady - 1
7. 50-foot walk test < 15sec - 4
15.1 - 20sec - 3 20.1 - 25sec - 2 >25sec - 1 Unable - 0
8. Climb one flight of stairs < 5sec - 4
5.1 - 10sec - 3 10.1 - 15sec - 2 >15sec - 1 Unable - 0
9 Climb stairs Number of flights of stairs up and down
(maximum 4)
Section: D
Elderly mobility scale:
TASK Date
Lying to Sitting
2 Independent
1 Needs help of 1 person 0 Needs help of 2+ people Sitting to
Lying
2 Independent
1 Needs help of 1 person 0 Needs help of 2+ people Sitting to
Standin
3 Independent in under 3 seconds 2 Independent in over 3 seconds
1 Needs help of 1 person 0 Needs help of 2+ people
Standing
3 Stands without support and able to reach
2 Stands without support but needs support to reach
1 Stands but needs support
0 Stands only with physical support of another person
Gait 3 Independent (+ / - stick) 2 Independent with frame
1 Mobile with walking aid but erratic unsafe
0 Needs physical help to walk or constant supervision
Timed Walk (6 metres)
3 Under 15 seconds 2 16 – 30 seconds 1 Over 30 seconds
0 Unable to cover 6 metres Recorded time in seconds
Functional
Reach
4 Over 20 cm. 2 10 - 20 cm. 0 Under 10 cm.
Actual reach
/20 /20 /20 Score interpretation:
14 – 20 - Independent in activity of daily living
10 – 13 - Borderline independent in activity of daily living
Pilot study:
In order to test the feasibility, relevance and practicability of the study. A pilot study was conducted among 6 patients who are 60 years and above 60 years old in the same manner of the original study in ANGEL old age home in karuppaurani. Data were analyzed to find out the reliability, it was 0.75.
Data collection procedure:
The investigator met the head of the old age home in order to establish support and co-operation to conduct the study successfully. The formal permission was taken from the higher authority of the old age home, for the main study. The investigator introduced her to the people in old age home and established rapport with them. Pre- experimental one group pre-test post-test design was used for the study. A total number of 30 elderly were selected through non probability purposive sampling technique. Appropriate orientation had given to the samples about the aim of the study, nature of questionnaire and adequate care was taken for confidentially and identity. First day pre test was conducted (It include demographic data, physical performance test, elderly mobility scale and falls efficacy scale)for 30 samples and Tailored exercise was given for 30 min/day on each Monday, Wednesday, and Friday for 5 weeks. The post test of the study was carried out 5 weeks later, using the same tool as same as pre – test. Collected data was then tabulated and analyzed.
Plan for data analysis:
The data analysis was done according to the objectives of study. Both descriptive and inferential statistics were used.
Descriptive statics:
Frequency, percentage and mean were used for analysis pre and post test assessment.
Inferential statistics:
was used to determine the association between the pretest level of physical performance, mobility and falls efficacy with their selected demographic variables.
Protection of human rights:
CHAPTER – IV
ANALYSIS AND INTERPRETATION OF DATA
This chapter deals with the analysis and interpretation of data collected from selected group of sample who have received physical performance, mobility and falls efficacy. The data collected were tabulated analyzed and presented based on objectives and hypothesis
It consists of the following sessions:
Section I – Distribution of samples according to their demographic variables Section II – Distribution of samples according to their physical performance, mobility and falls efficacy.
Section III - Comparison of mean pre and post test level of physical performance, mobility and falls efficacy scale.
Section IV – Association between pre test level of physical performance with their selected demographic variables.
Section V - Association between pre test level of elderly mobility and their selected demographic variables
Section VI - Association between pre test level of falls efficacy scale and their selected demographic variables.
SECTION I
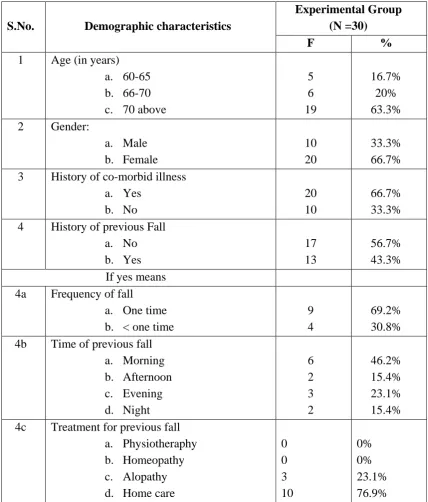
[image:43.595.101.530.224.727.2]Distribution of the samples according to their demographic variables Table 2
Distribution of the samples according to their demographic variables (N=30)
S.No. Demographic characteristics
Experimental Group (N =30)
F %
1 Age (in years) a. 60-65 b. 66-70 c. 70 above
5 6 19 16.7% 20% 63.3% 2 Gender:
a. Male b. Female 10 20 33.3% 66.7% 3 History of co-morbid illness
a. Yes b. No 20 10 66.7% 33.3% 4 History of previous Fall
a. No b. Yes 17 13 56.7% 43.3% If yes means
4a Frequency of fall
a. One time b. < one time
9 4
69.2% 30.8% 4b Time of previous fall
a. Morning b. Afternoon c. Evening d. Night 6 2 3 2 46.2% 15.4% 23.1% 15.4% 4c Treatment for previous fall
a. Physiotheraphy b. Homeopathy c. Alopathy d. Home care
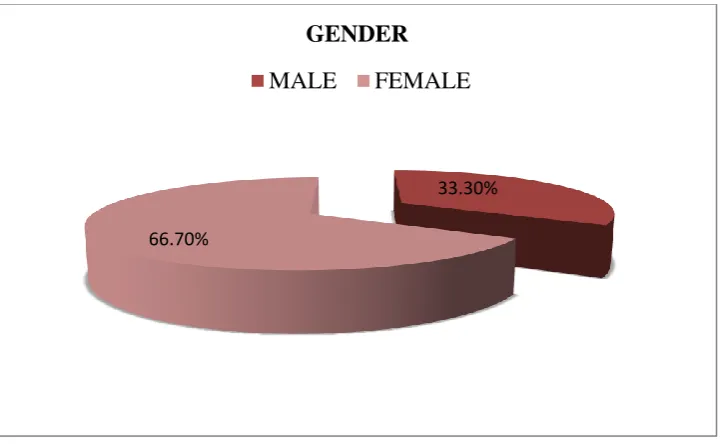
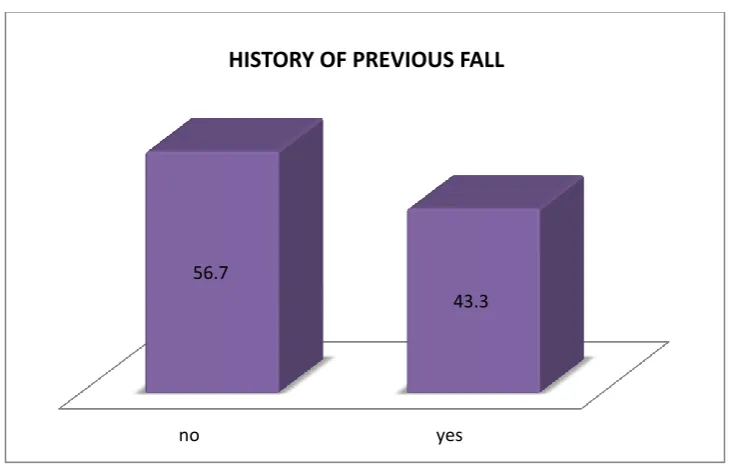
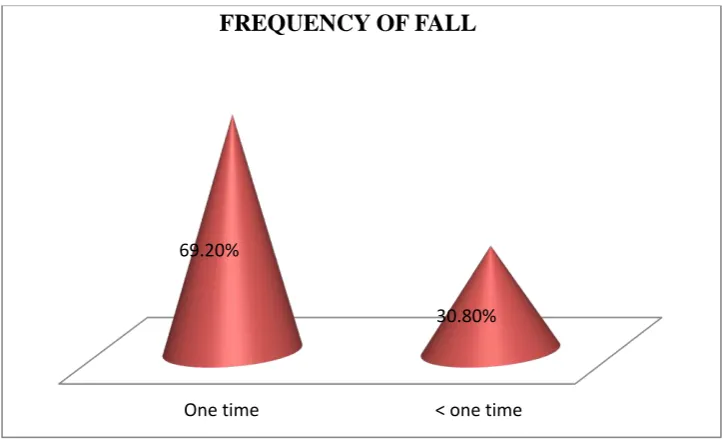
Table 2 summarizes the majority of samples 19 out of 30( 63.3%) in the age group were between 71 years above,6 out of 30 (20%) in the age group between 66 – 70 years and 5 out of 30(16.7%) in the age group between 60-65 years. With regard gender, the most of samples 20 out of 30(66.7%) were in females and10 out of 30 (33.3%) were in male. With regards of co- morbid illness 20 out of 30 (66.7%) were in yes and 10 out of 30 (33.3%)were in no. According to history of fall 17 out of 30 (56.7%) were in no fall and 13 out of 30 (43.3%) were in history of fall.
Figure 2: Distribution of samples according to their age.
Figure 3: Distribution of samples according to their gender
17%
20%
63%
AGE
61-65 years 66-70 years 70 years above
33.30%
66.70%
GENDER
[image:45.595.143.504.403.625.2]Figure 4: Distribution of samples according to their history of co-morbid illness
Figure 5: Distribution of samples according to their history of previous fall
Yes No
66.70%
33.30%
HISTORY OF CO MORBID ILLNESS
no yes
56.7
43.3
[image:46.595.139.504.430.662.2]Figure 6: Distribution of samples according to their frequency of fall
Figure 7: Distribution of samples according to their time of previous of fall
One time < one time 69.20%
30.80%
FREQUENCY OF FALL
Morning
Afternoon Evening
Night 46.20%
15.40% 23.10%
15.40%
Figure 8: Distribution of samples according to their treatment of previous fall
0% 10% 20% 30% 40% 50% 60% 70% 80%
SECTION II
Distribution of samples according to their physical performance, mobility and falls efficacy.
Table 3
Distribution of samples according to their physical performance, mobility and falls efficacy.
Name of the scale
Pre test Post test
F % F %
Level of physical performance
> 17 - unable to function 17 -24 – moderate frailty 25-31 – mild frailty 32-36 – not frail
- 22 8 - - 73.3% 26.6% - - - 29 1 - - 96.6% 3.3% Level of mobility
>10 - dependent manuver
10 -13 – borderline independent ADL <14 - Independent ADL
- 25 5 - 83.3% 16.6% - 1 29 - 3.3 96.6% Levels of fall efficacy
16-19 – low concern 20- 27 – moderate concern 28-64 – high concern
Table 3 shows, regarding the level of physical performance in pre test none of them in unable to function, 22 out of 30 (73.3%)samples having moderate fralilty ,and 8 out of 30 (26.6%) sample having mild frailty level, and none of them in not frail. In post test level of physical performance none of them were below 17, none of there in between 32-36 (not frailty).
In the level of mobility in pre test,none of them in >10 (dependent manuver), 25 out of 30 (83.3%)in between 10 -13(borderline independent in daily living activity), 5 out of 30 (16.6%) in above 14 (independent in daily living activity) and post test none of them in >10 (dependent manuver),25 out of 30 (33%) in between 10-13 (borderline independent in daily living activity)29 out of 30(96.6%) in above 14 (independent in daily living activity).
In the level of fall efficacy in pre test, none of them in 16-19 (low concern ) 20-27 (moderate concern)10 out of 30 (33.3%) in 28-64 (high concern) 20 out of 30 (66.6%) and post test 16-19 (low concern) 3 out of 30 (10%) 20-27 (moderate concern) 8 out of 30 (26.6%) in 28-64 (high concern) 19 out of 30 (63.3%).
Figure 9: comparison between pre and post test level of physical performance
Figure 10: comparison between pre and post test level of mobility
unable to function
moderate frailty
mild frailty not frail 0
73.30%
26.60%
0 0
96.60%
3.30%
LEVEL OF PHYSICAL PERFORMANCE pre test post test
0
83.30%
16.60%
0 3.30%
96.60%
dependent manuver borderline independent ADL
Independent ADL
LEVEL OF MOBILITY
[image:51.595.132.496.403.620.2]Figure 11: comparison between the pre and post test level of falls efficacy
low concern
moderate concern
high concern 0
33.30%
66.60%
10% 26.60%
63.30%
LEVEL OF FALLS EFFICACY
SECTION III
[image:53.595.100.534.233.529.2]Comparison of mean pre and post test level of physical performance, mobility and falls efficacy scale.
Table 4
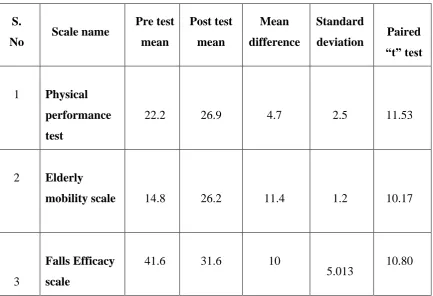
Comparison of mean pre and post test level of physical performance, mobility and falls efficacy scale.
S.
No Scale name
Pre test mean
Post test mean
Mean difference
Standard
deviation Paired “t” test
1 Physical performance test
22.2 26.9 4.7 2.5 11.53
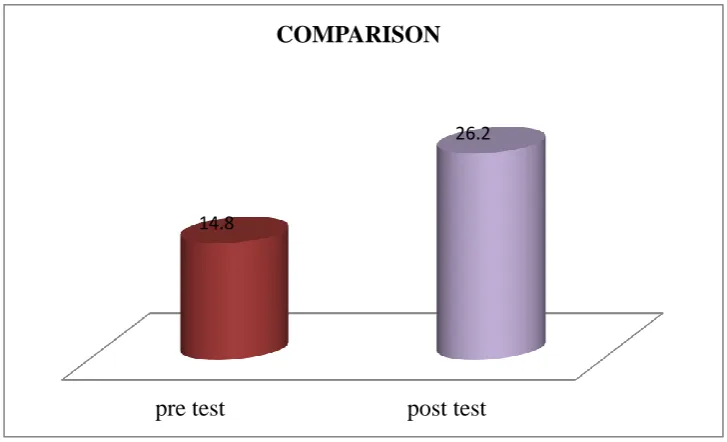
2 Elderly
mobility scale 14.8 26.2 11.4 1.2 10.17
3
Falls Efficacy scale
41.6 31.6 10
5.013 10.80
(** =Significant at 0.05 level)
Table 5 shows regarding the level of physical performance in pre test mean value 22.2, post test mean value 26.9 , pre and post test mean difference 4.7 standard deviation value 2.5, paired “t” test value 11.53 was greater than table value at 0.05 level of significant, which shows that there is significant difference between the pre test and post test level of physical performance. Hence, the formulated research hypothesis H1 was accepted.
In elderly mobility pre test mean value 14.8, post test mean value 26.2 , pre and post test mean difference11.4, standard deviation 1.2 and paired “t” test value 10.17 was greater than table value at 0.05 level of significant, which shows that there is significant difference between the pre test and post test level of mobility. Hence, the formulated research hypothesis H1 was accepted.
Figure 13: comparison between the pre and post test mean level of physical performance test
Figure 14: comparison between the pre and post test mean level of mobility test
pre test post test
14.8
26.2
COMPARISON
pre test post test
22.2
26.9
[image:55.595.133.497.436.657.2]Figure 15: comparison between the pre and post mean level of falls efficacy scale
Pre test post test
41.6
31.6
SECTION IV
[image:57.595.76.559.184.760.2]Association between pre test level of physical performance with their selected demographic variables.
Table 5
Association between pre test level of physical performance with their selected demographic variables.
(N=30)
Demographic Variables Sample (n)Physical Performance Chi
Square
2 value P<0.05 32-36 25-31 17-24 <17
No % No % No % No % No % 1.Age
a. 60 – 65 b. 66 – 70 c. < 70
2.Gender a. Male b. Female 3.Co-morbid illness a. Yes b. No
4.History of previous fall
a. No b. Yes
If yes, means 5.Frequency of fall
a. One time b. < one time
6.Time of fall a. morning
b. Afternoon c. Evening d. Night
7.Treatment of fall a. Physiotheraphy b. Homeopathy c. Alopathy d. Home care
5 6 19 10 20 20 10 17 13 9 4 6 2 3 2 0 0 3 10 16.7 20 63.3 33.3 66.7 66.7 33.3 56.6 43.3 69.2 30.8 46.2 15.4 23.1 15.4 0 0 23.1 76.9 - - - - - - - - - - - - - - - - - - - - - - - - 1 - 11 2 6 4 3 5 13 9 4 6 2 3 2 - - 3 1 0 20 - - 20 30 20 30 29.4 100 100 100 100 100 100 100 - - 100 100 4 6 8 8 14 16 7 12 - - - - - - - - - - - 80 - 100 80 70 80 70 70.6 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 1.203 DF-2 NS 0.052 DF-1 NS 1.65 DF-1 NS 5.417 DF-2 ** 4.76 DF-1 ** 0.978 DF-3 NS 0.6 DF- 3 NS - - - - - - - - - - - - - -