and Situation-Specific Drinking
in Women Substance Abusers
Sherry H. Stewart, PhD
Patricia J. Conrod, PhD
Sarah Barton Samoluk, PhD
Robert O. Pihl, PhD
Maurice Dongier, MD
ABSTRACT. Posttraumatic stress disorder (PTSD) and alcohol use disorders are frequently co-morbid conditions (Stewart, 1996). Alcohol use may serve a ‘‘negatively-reinforcing’’ function among traumatized individuals with PTSD (Stewart, 1996; Stewart, Conrod, Pihl, & Dongier, 1999a; Stewart, Pihl, Conrod, & Dongier, 1998). As such, the heavy drinking behavior of those with PTSD should be relatively situation-specific (i.e., more frequent in ‘‘negative’’ discriminative contexts than in other types of contexts). To test this ‘‘situational-specificity’’
hypoth-Sherry H. Stewart is affiliated with the Department of Psychology, Dalhousie University, Halifax, NS, Canada. Patricia J. Conrod is affiliated with the Department of Psychology, State University of New York at Stony Brook, Stony Brook, NY. Sarah Barton Samoluk is affiliated with the Department of Psychology, Queen Eliza-beth II Health Sciences Centre, Halifax, NS, Canada. Robert O. Pihl is affiliated with the Department of Psychology, McGill University, Montreal, PQ, Canada. Maurice Dongier is affiliated with the Department of Psychiatry, Douglas Hospital, Verdun, PQ, Canada.
Address correspondence to: Dr. Sherry H. Stewart, Department of Psychology, Dalhousie University, Life Sciences Centre, 1355 Oxford Street, Halifax, Nova Scotia, Canada, B3H 4J1 (E-mail: [email protected]).
The authors wish to acknowledge the research assistance of Sylvana Côté, Vero-nique Fontaine, Heather Lee Loughlin, and Heidi Mason.
This research was supported by a grant from the National Health Research Devel-opment Program (NHRDP), Health Canada, and was conducted through the McGill University--Douglas Hospital Alcohol Research Program, Verdun, Quebec, Canada.
Alcoholism Treatment Quarterly, Vol. 18(3) 2000
esis, a lifetime measure of trauma exposure (Everstine & Everstine, 1993), the PTSD Symptom Self-Report Scale (Foa, Riggs, Dancu, & Rothbaum, 1993), and the 42-item Inventory of Drinking Situations (Annis, Graham, & Davis, 1987) were administered to a community-re-cruited sample of 294 adult women substance abusers. PTSD symp-toms were significantly positively correlated with frequency of heavy drinking in negative situations, but unrelated to frequency of heavy drinking in positive and temptation situations. At the level of specific drinking situations, PTSD symptoms were significantly positively cor-related with frequency of heavy drinking in the negative situations of Unpleasant Emotions, Physical Discomfort, and Conflict with Others. PTSD symptoms were unrelated to frequency of heavy drinking in the positive situations of Pleasant Times with Others and Social Pressure to Drink, or in the temptation situations of Testing Personal Control and Urges and Temptations. Additionally, PTSD symptoms were signifi-cantly negatively correlated with frequency of heavy drinking in posi-tive situations involving Pleasant Emotions. Anxiety sensitivity (fear of anxiety-related sensations; Peterson & Reiss, 1992), but not Neuroti-cism (tendency to experience negative affect; Costa & McCrae, 1992), mediated the observed associations between PTSD symptoms and situ-ation-specific heavy drinking in negative contexts in general, and Con-flict with Others and Physical Discomfort situations in particular. Im-plications for designing potentially more effective interventions for women with co-morbid PTSD-alcohol use disorders are discussed.
[Article copies available for a fee from The Haworth Document Delivery Service: 1-800-342-9678. E-mail address: <[email protected]> Website: <http://www.HaworthPress.com>]
Posttraumatic stress disorder (PTSD) is an anxiety disorder that can devel-op following exposure to a ‘‘trauma’’--a situation involving threatened or actual serious injury or death, or a threat to the physical integrity of the self or others, where the individual’s response involves extreme fear, helplessness, or horror (DSM-IV Criterion A; APA, 1994). DSM-IV PTSD symptoms include intrusions (Criterion B; e.g., nightmares), avoidance/numbing (Crite-rion C; e.g., avoiding trauma reminders), and arousal (Crite(Crite-rion D; e.g., increased startle).
Research across a variety of trauma (e.g., sexual and physical victimiza-tion; combat; disaster) and populations (e.g., clinical and community; men and women) indicates a high co-morbidity between PTSD and alcohol use disorders (Stewart, 1996). Some have suggested that, from an operant condi-tioning perspective (Skinner, 1938), alcohol use may serve a ‘‘negatively-re-inforcing’’ function among traumatized individuals with PTSD. That is, their heavy drinking may represent a learned behavior maintained by its short-term anxiety- or arousal-reducing consequences (Stewart, 1996; Stewart, Conrod, Pihl, & Dongier, 1999a; Stewart, Pihl, Conrod, & Dongier, 1998). For
exam-ple, a woman dealing with rape-related PTSD may learn to misuse alcohol in an attempt to escape or avoid the anxiety-related symptoms that have emerged since her sexual victimization. In fact, PTSD tends to precede the emergence of problem drinking in co-morbid cases (Stewart, 1996) and sig-nificantly increases the risk for a first onset alcohol use disorder (Stewart et al., 1998). Moreover, degree of alcohol dependence has been shown to be positively associated with PTSD arousal symptoms in women (Stewart et al., 1999a).
Co-morbid PTSD-alcohol disordered individuals display episodic heavy drinking or ‘‘bingeing’’ (Stewart, 1996). If heavy drinking does serve a negatively-reinforcing function among such co-morbid cases, the presence of PTSD symptoms should be related to a pattern of heavy drinking episodes which are limited to contexts that reliably signal that negative reinforcement is available by drinking. In operant conditioning terms, such ‘‘discriminative contextual stimuli’’ (Skinner, 1938) for individuals with co-morbid PTSD-al-cohol disorders could include any contexts involving anxious emotions or physical arousal symptoms. However, few studies have examined the specif-ic contexts involved in the heavy drinking behavior of co-morbid PTSD-al-cohol disordered individuals.
The Inventory of Drinking Situations (IDS; Annis, Graham, & Davis, 1987) measures alcoholics’ typical heavy drinking situations, based on Mar-latt and Gordon’s (1985) eight-category taxonomy. The IDS and its short form (i.e., the IDS-42) contain eight subscales tapping relative frequency of heavy alcohol use in eight distinct types of drinking situations (e.g., Physical Discomfort). The short-form IDS-42 appears to be a useful instrument for assessing the situational-specificity hypothesis with respect to the drinking behavior of traumatized individuals with significant PTSD symptoms. It contains three scales which have been determined via factor analysis (e.g., Stewart, Samoluk, Conrod, Pihl, & Dongier, in press) to tap heavy drinking in ‘‘negative’’ situations (i.e., contexts signaling that negative reinforcement is available from drinking--Unpleasant Emotions, Conflict with Others, and Physical Discomfort scales). It also contains five additional scales which have been determined to tap heavy drinking in other types of situations--spe-cifically, ‘‘positive’’ situations (i.e., Pleasant Emotions, Pleasant Times with Others, Social Pressure scales) and ‘‘temptation’’ situations (i.e., Urges and Temptations, Testing Personal Control scales).
Certain personality factors are related to a pattern of situation-specific heavy drinking. Among a sample of alcoholics and cocaine addicts, Cannon, Rubin, Keefe, Black, Leeka, and Phillips (1992) showed that negative tem-perament or ‘‘Neuroticism’’ (N; a tendency to experience a variety of nega-tive emotions; Costa & McCrae, 1992) was posinega-tively correlated with fre-quency of heavy drinking on a negative drinking situations factor of the IDS
(i.e., items from the Unpleasant Emotions and Conflict with Others sub-scales). Anxiety sensitivity (AS; fear of anxiety-related bodily sensations; Peterson & Reiss, 1992) is another personality factor that has been explored with respect to the situational-specificity hypothesis. Samoluk and Stewart (1998) found that, among university student drinkers, AS levels were signifi-cantly positively correlated with drinking frequency on a higher-order IDS-42 factor of negative situations, but not significantly correlated with drinking frequency on higher-order IDS-42 factors of positive or temptation situations. Whether the situation-specificity hypothesis regarding the rela-tions between AS levels and drinking situarela-tions would also be supported in substance abusers remains to be determined.
These same personality variables of N and/or AS may be involved in the high co-morbidity of PTSD and alcohol use disorders (Stewart, 1996). High levels of N have been reported in clinical samples of alcoholics (e.g., Martin & Sher, 1994), and N is an established risk factor for the development of PTSD following trauma exposure (e.g., McFarlane, 1989). AS levels are also ele-vated among those with alcoholism (Stewart, Samoluk, & MacDonald, 1999b) and those with PTSD (e.g., Taylor, Koch, & McNally, 1992). More-over, AS levels are higher in PTSD than in all other anxiety disorders save panic disorder (Taylor et al., 1992). It has been suggested that AS may represent a pre-morbid vulnerability factor for the development of PTSD following exposure to a traumatic event since people with high AS should be more likely to develop conditioned fear reactions (e.g., flashbacks) to trauma cues. In turn, the experience of anxiety-related PTSD symptoms may in-crease AS (Taylor et al., 1992).
Revisions of the traditional operant conditioning (i.e., tension-reduction) theory of alcoholism involving anxiety-related personality risk variables sug-gest that certain types of individuals may be more motivated than others to learn to drink to escape or avoid anxiety (Stewart et al., 1999b). For example, high N individuals might be more prone than others to learn to drink to escape/avoid anxiety. But the personality variable of AS may be a more powerful motivating factor for the use of alcohol to escape/avoid anxiety than N. Individuals who are highly fearful of the occurrence of anxiety symptoms should be theoretically more likely than others to engage in behaviors aimed at escaping/avoiding anxiety, such as heavy drinking (Stewart et al., 1999b). According to such personality risk models, AS and/or N may serve as ‘‘me-diating’’ or intervening variables (Baron & Kenny, 1986) in explaining the hypothesized relation between PTSD and situation-specific heavy drinking in negative contexts. Those alcohol abusers with PTSD may more often drink heavily in negative situations (e.g., when experiencing Unpleasant Emotions) at least partly because they are more prone to experiencing negative affect
and/or because they are highly fearful of the experience of anxiety symptoms (cf. Stewart et al., 1999b).
The first purpose of the present study was to evaluate the situational-speci-ficity hypothesis. We hypothesized that a greater frequency of PTSD symp-toms would be significantly associated with a greater frequency of heavy drinking in negative contexts in general, and with a greater frequency of heavy drinking in specific contexts involving Unpleasant Emotions, Physical Discomfort, and Conflict with Others. We further predicted that PTSD symp-tom frequency would be unrelated to frequency of heavy drinking in positive and temptation situations. The second purpose was to evaluate the potential mediating roles of N and/or AS in explaining the hypothesized relations between PTSD symptoms and situation-specific drinking in negative con-texts. We expected that both AS and N would be related to a greater frequen-cy of heavy drinking in negative contexts (cf. Cannon et al., 1992; Samoluk & Stewart, 1998). However, we hypothesized that the personality variable of AS would prove to be a stronger mediator than N in explaining relations between PTSD symptoms and heavy drinking in negative contexts.
METHOD
Participants.In total, 294 women were recruited through advertisements placed in English and French newspapers circulated in the Greater Montreal area as part of a larger project on alcohol and prescription drug abuse/depen-dence in women. Individuals who responded to the advertisement were con-tacted by telephone for a screening interview in which information on their substance use, psychiatric, and medical histories was obtained. Inclusion criteria were female gender, 30 to 50 years of age (i.e., the age range at which distributions for the abuse of alcohol and prescription drugs overlap for women), and abusing or dependent on alcohol and/or a prescription depres-sant drug (anxiolytic/analgesic). Screening for alcohol and prescription drug abuse involved use of the Brief Michigan Alcoholism Screening Test (Brief MAST; Pokorny, Miller, & Kaplan, 1972), and two versions of the Drug Abuse Screening Test (DAST; Skinner, 1982) for anxiolytic and analgesic medication use, respectively. Cutoffs for inclusion were 10 and/or 12 on the Brief MAST and DAST, respectively. Alcohol and/or prescription drug de-pendence were coded if a participant acknowledged at least 3 of the 7 DSM-IV (APA, 1994) criteria for substance dependence within the previous 12 months, for any of the three substances of interest (alcohol, anxiolytics, analgesics). Women abusing/dependent on substances other than alcohol or prescription drugs were not excluded.
This recruitment procedure resulted in a heterogeneous sample of sub-stance abusing women. The Computerized-Diagnostic Interview Schedule
(C-DIS Management Group, 1991) revealed rates of lifetime substance de-pendence disorders as follows: 83% alcohol-, 31% cocaine-, 25% anxiolytic-, 18% cannabis-, 10% opioid analgesic-, and 4% heroin-dependent. About 49% of the sample met lifetime criteria for two or more dependence diag-noses. The mean screening score on the Brief MAST in the total sample was 10.0 (SD= 7.7). The mean screening DAST score for anxiolytics was 3.3 (SD= 6.2) and for analgesics was 0.6 (SD= 2.4). Sixty-two percent of the sample were primarily French-speakers; the others were primarily English-speakers. The average age was 38.7 (SD = 5.9) years. Fifty-four percent were never married, 25% divorced, and 21% married/cohabiting. Forty-one percent had no children, 36% were unemployed, and 28% were homemakers. Thirty-seven percent had completed high school, and 18% had completed under-graduate university. Average education was 12.9 (SD= 3.8) years of school-ing. Mean yearly personal income was about 13,000 Canadian dollars (SD= $12,000).
Measures.French or English versions of all measures were administered to each participant depending on her first language. French translations of English study measures were performed by employees of our research team who were experienced in English to French translation. To verify the transla-tions, each measure was back-translated by a separate employee and modifi-cations to the original translations were made when necessary.
Trauma Exposure Checklist (TEC). The self-report TEC (Everstine & Everstine, 1993) was used to identify all traumatic events to which each participant had been exposed in her lifetime. Sample events on this scale included DSM-IV (APA, 1994) Criterion A events such as physical assault (e.g., being beaten, being mugged) and sexual assault (e.g., rape in adulthood, childhood sexual abuse), as well as other extremely stressful events that might be arguably less traumatic such as threat of loss (e.g., disappearance of family member) or physical loss (e.g., abortion). Sub-threshold events were included given evidence that stressors of lower magnitude than those defined by Criterion A are at times capable of eliciting PTSD symptoms (March, 1993). Respondents were asked to specify which, if any, of all the traumatic experiences to which they had ever been exposed was of most concern to them presently. If the respondent indicated that a particular traumatic experi-ence was of current concern, then she rated the nature and frequency of her associated symptoms on the PTSD self-report measure described below.
PTSD Symptoms Scale-Self Report (PSS-SR). The PSS-SR (Foa, Riggs, Dancu, & Rothbaum, 1993) consists of the 17 symptoms from the DSM-IV (APA, 1994) description of PTSD. Respondents are asked to complete PSS-SR items by rating the frequency of each symptom over the last two weeks on a scale from 0 (not at all) to 3 (almost always). The PSS-SR Total score has excellent psychometric properties (Foa et al., 1993).
Short Form Inventory of Drinking Situations (IDS-42).The IDS-42 (Annis et al., 1987) is a 42-item self-report questionnaire designed to assess relative frequency of heavy drinking across specific situations. The IDS-42 contains eight drinking situation subscales (e.g., Pleasant Times with Others) as de-scribed earlier. Respondents rate their frequency of heavy drinking in each situation on a scale from 1 (never drank heavily in that situation) to 4 (always drank heavily in that situation). The IDS-42 possesses good psychometric properties (Annis et al., 1987).
Anxiety Sensitivity Index (ASI). The ASI (Peterson & Reiss, 1992) is a 16-item self-report questionnaire that assesses an individual’s level of fear of anxiety-related symptoms (e.g., rapid heartbeat; dizziness). Respondents rate the degree to which they agree or disagree with each item on a 5-point scale with anchors of 0 (very little) and 4 (very much). The ASI has sound psycho-metric properties (Peterson & Reiss, 1992).
NEO Five Factor Inventory (NEO-FFI). The NEO-FFI is a self-report measure of personality traits designed to operationalize the Five-Factor Mod-el of personality (Costa & McCrae, 1992). It consists of 60 specific items regarding feelings, preferences, and social behavior, organized across five broad personality domains (i.e., Neuroticism, Extraversion, Openness, Agree-ableness, and Conscientiousness) of 12 items each. Each item is rated on a five point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The NEO-FFI-N domain score, used in the present study, possesses excellent psychometric properties (Costa & McCrae, 1992).
Procedure.After informed consent was obtained, participants completed a number of self-report measures including those described above. Each partic-ipant was provided with $35 (Canadian) as compensation for her time.
RESULTS Sample Means
TEC. Consistent with previous research with substance abusing women (cf., Covington, 1983; Fullilove et al., 1993; Miller, Downs, & Testa, 1993), self-reported rates of trauma exposure on the TEC were high for several events. For example, 42% of the sample reported lifetime histories of physi-cal assault, and 47% reported lifetime histories of sexual assault. Many women reported exposures to multiple events: 68% endorsed six or more experiences on the TEC. About 70% of the sample reported having been exposed to at least one experience in her lifetime that would meet the DSM-IV Criterion A (APA, 1994) definition of a traumatic event.
the sample indicated that there was no listed traumatic experience on the TEC that was currently of concern. These women were not asked to complete the PSS-SR as it would not have been relevant to them, and were automatically assigned scores of zero on PSS-SR items. The average PSS-SR Total score for the entire sample (Table 1) was somewhat lower than that reported for female assault victims assessed three months after their assaults (i.e., M= 24.2;SD = 12.5; Foa, Riggs, & Gershuny, 1995). Most symptoms received moderate endorsement rates. Using Foa et al.’s (1993) cutoffs for the PSS-SR, 63% of the total sample met Criteria B, C, and D for a DSM-IV PTSD diagnosis. When the nature of the events reported on the TEC were
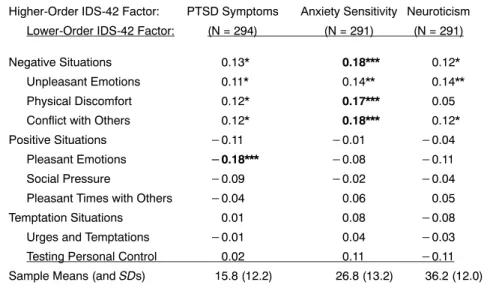
consid-TABLE 1. Bivariate Correlations Between IDS-42 Higher- and Lower-Order Factor Scores, and Scores on the Measures of PTSD Symptoms, Anxiety Sensitivity, and Neuroticism
Anxiety-Related Variables
Higher-Order IDS-42 Factor: PTSD Symptoms Anxiety Sensitivity Neuroticism Lower-Order IDS-42 Factor: (N = 294) (N = 291) (N = 291)
Negative Situations 0.13* 0.18*** 0.12*
Unpleasant Emotions 0.11* 0.14** 0.14**
Physical Discomfort 0.12* 0.17*** 0.05
Conflict with Others 0.12* 0.18*** 0.12*
Positive Situations 0.11 0.01 0.04
Pleasant Emotions 0.18*** 0.08 0.11
Social Pressure 0.09 0.02 0.04
Pleasant Times with Others 0.04 0.06 0.05
Temptation Situations 0.01 0.08 0.08
Urges and Temptations 0.01 0.04 0.03
Testing Personal Control 0.02 0.11 0.11
Sample Means (andSDs) 15.8 (12.2) 26.8 (13.2) 36.2 (12.0)
Notes:N’s vary across columns because three participants failed to fully complete the anxiety-related personality measures. IDS-42 factor scores were calculated via the regression method on the basis of lower- and higher-order confirmatory factor analyses of participants’ IDS-42 item responses (Stewart et al., in press). Asterisks (*) indicate significant correlations: *p< 0.05; **p< 0.01; ***p< 0.005. Correlations between anxiety-related measures and all negative IDS-42 factors were evaluated with one-tailed tests given that directional effects were hypothesized a priori; all other correlations were evaluated using two-tailed tests. Correlations in bold represent those relationships that remained statistically significant after controlling for the influences of the other two anxiety-related measures (i.e., final steps of mediator analyses). PTSD symptoms were assessed with the PSS-SR (Foa et al., 1993), Anxiety Sensitivity with the ASI (Peterson & Reiss, 1992), Neuroticism with the NEO-FFI-N scale (Costa & McCrae, 1992), and Drinking Situations with the IDS-42 (Annis et al., 1987).
ered, 46% met Criteria A-D for a DSM-IV PTSD diagnosis. The sample mean on the ASI (Table 1) was about oneSDabove the female norm (Peter-son & Reiss, 1992). The sample mean on the NEO-FFI-N (Table 1) was also about oneSDabove the female norm (Costa & McCrae, 1992).
Purpose #1: Evaluation of the Situational Specificity Hypothesis. The IDS-42 was scored according to eight lower-order drinking situation factors (corresponding to the eight IDS-42 subscales) and three higher-order factors (i.e., negative, positive, and temptation situations) as determined by confir-matory factor analyses of the IDS-42 item responses of the present sample (Stewart et al., in press). Factor scores were calculated using the regression method (cf. Samoluk & Stewart, 1998). Correlations were then computed between PSS-SR Total scores and each of the IDS-42 factor scores (see Table 1). Correlations between PSS-SR scores and all ‘‘negative’’ IDS-42 factors were evaluated with one-tailed tests given that directional effects were hy-pothesized a priori; all other correlations were evaluated using two-tailed tests. Consistent with hypothesis, PSS-SR scores were significantly positive-ly correlated with heavy drinking in negative situations, but unrelated to heavy drinking in positive or temptation situations. At the level of specific drinking situations, PSS-SR scores were significantly positively correlated with heavy drinking in the negative situations of Unpleasant Emotions, Physical Discomfort, and Conflict with Others. PSS-SR scores were unre-lated to heavy drinking in the positive situations of Pleasant Times with Others and Social Pressure, or in the temptation situations of Testing Personal Control and Urges and Temptations. Unexpectedly, PSS-SR scores were significantly negatively correlated with heavy drinking in positive situations involving Pleasant Emotions.
Purpose #2: Evaluation of Personality Factors as Mediators Hypothesis.
Correlations were computed between scores on the anxiety-related personali-ty measures (i.e., ASI and NEO-FFI-N) and scores on each of the IDS-42 factor scores (see Table 1). Again, correlations between anxiety measures and all ‘‘negative’’ IDS-42 factors were evaluated with one-tailed tests given that directional effects were hypothesized a priori. Consistent with hypothesis, both AS and N were positively correlated with heavy drinking in negative situations, but unrelated to heavy drinking in positive or temptation situa-tions. At the level of specific drinking situations, both AS and N scores were positively correlated with heavy drinking in the negative situations of Un-pleasant Emotions and Conflict with Others. Both AS and N were unrelated to heavy drinking in the positive situations of Pleasant Times with Others, Pleasant Emotions, and Social Pressure, or in the temptation situations of Testing Personal Control, and Urges and Temptations. AS (but not N) was also positively correlated with heavy drinking in Physical Discomfort con-texts.
Scores on the anxiety-related measures were significantly inter-correlated with one another. AS and N were positively inter-correlated (r = 0.31,p< .001, one-tailed test). PSS-SR scores were positively correlated both with AS scores (r= 0.39,p< .001, one-tailed test) and with N scores (r= 0.26, p< .001, one-tailed test).
Tests of the potential mediating roles of the anxiety-related personality variables (AS and N) in accounting for the five significant associations be-tween PTSD symptoms and drinking situations (see Table 1) were performed using mediator regression analyses (Baron & Kenny, 1986). AS and N scores were first separately regressed on PSS-SR scores. PSS-SR scores predicted increased AS (F(1, 288) = 52.71,p< .0001) and increased N (F(1, 288) = 20.69, p < .0001) levels, suggesting that either personality variable could potentially serve as a mediator.
To test the potential mediating roles of AS and N in accounting for the association between PTSD symptoms and heavy drinking in negative con-texts in general, higher-order negative drinking situation factor scores were regressed on PSS-SR scores. As expected, PSS-SR scores predicted in-creased heavy drinking in negative situations (F(1, 292) = 4.79,p < .05). Then, higher-order negative drinking situation factor scores were regressed on AS, N, and PSS-SR scores simultaneously (F(3, 286) = 4.02,p< .01). Univariate effects indicated that AS scores predicted increased heavy drink-ing in negative contexts (partial r = .12,p < .05) whereas N scores were unrelated to heavy drinking in negative contexts (partialr= .06,n.s.). PSS-SR scores no longer predicted increased heavy drinking in negative contexts (partialr= .06,n.s.) after accounting for the influences of AS and N.
To test the potential mediating roles of AS and N in accounting for the association between PTSD symptoms and heavy drinking in Conflict with Others situations, lower-order Conflict with Others drinking situation factor scores were regressed on PSS-SR scores. PSS-SR scores predicted increased heavy drinking in situations involving Conflict with Others (F (1, 292) = 4.44, p < .05). Then, lower-order Conflict with Others drinking situation factor scores were regressed on AS, N, and PSS-SR scores simultaneously (F
(3, 286) = 4.08,p< .01). Univariate effects indicated that AS scores predicted increased heavy drinking in Conflict with Others situations (partialr= .13,
p< .05) whereas N scores were unrelated to heavy drinking in Conflict with Others situations (partial r = .06,n.s.). PSS-SR scores no longer predicted increased heavy drinking in Conflict with Others situations (partialr= .06,
n.s.) after accounting for AS and N. To test the potential mediating roles of AS and N in accounting for the association between PTSD symptoms and heavy drinking in Physical Discomfort situations, lower-order Physical Dis-comfort drinking situation factor scores were regressed on PSS-SR scores. PSS-SR scores predicted increased heavy drinking in Physical Discomfort
contexts (F(1, 292) = 4.13,p< .05). Then, lower-order Physical Discomfort drinking situation factor scores were regressed on AS, N, and PSS-SR scores simultaneously (F(3, 286) = 3.41,p< .05). Univariate effects indicated that AS scores predicted increased heavy drinking in Physical Discomfort con-texts (partial r = .14, p < .05) whereas N scores were unrelated to heavy drinking in Physical Discomfort contexts (partial r =.02, n.s.). PSS-SR
scores no longer predicted increased heavy drinking in Physical Discomfort contexts (partial r = .07, n.s.) after accounting for AS and N. To test the potential mediating roles of AS and N in accounting for the association between PTSD symptoms and heavy drinking in Unpleasant Emotions situa-tions, lower-order Unpleasant Emotions drinking situation factor scores were regressed on PSS-SR scores. PSS-SR scores predicted increased heavy drink-ing in Unpleasant Emotions situations (F (1, 292) = 3.72, p< .05). Then, lower-order Unpleasant Emotions drinking situation factor scores were re-gressed on AS, N, and PSS-SR scores simultaneously (F(3, 286) = 3.34,p< .05). Univariate effects showed that PSS-SR scores no longer predicted in-creased heavy drinking in Unpleasant Emotions contexts (partialr= .05,n.s.) after accounting for AS and N. However, in contrast to findings reported above for the other negative drinking contexts, N (partialr= .09,n.s.) and AS (partialr= .08,n.s.) no longer predicted heavy drinking in Unpleasant Emo-tions situaEmo-tions.
To test the potential mediating roles of AS and N in accounting for the association between PTSD symptoms and lesser heavy drinking in Pleasant Emotions situations, lower-order Pleasant Emotions drinking situation factor scores were regressed on PSS-SR scores. PSS-SR scores predicteddecreased
heavy drinking in Pleasant Emotions contexts (F(1, 292) = 9.77,p< .005). Then, lower-order Pleasant Emotions drinking situation factor scores were regressed on AS, N, and PSS-SR scores simultaneously (F(3, 286) = 3.67,p
< .05). Univariate effects indicated that both AS scores (partialr= .01,n.s.) and N scores were unrelated to heavy drinking in Pleasant Emotions contexts (partialr=.07,n.s.). PSS-SR scores continued to predict less heavy
drink-ing in Pleasant Emotions contexts (partial r = .15, p < .01) even after
accounting for AS and N levels.
DISCUSSION
Evidence for the ‘‘situational-specificity’’ hypothesis was obtained among our sample of substance abusing women: More frequent PTSD symptoms were significantly associated with a greater frequency of heavy drinking in negative situations in general, and with a greater frequency of heavy drinking in situations involving Physical Discomfort, Unpleasant Emotions, and Con-flict with Others in particular. Also consistent with the hypothesis, frequency
of PTSD symptoms was unrelated to heavy drinking in positive or temptation situations in general, and was unrelated to heavy drinking in situations in-volving Pleasant Times with Others, Social Pressure, Urges and Temptations, or Testing Personal Control in particular. Thus, traumatized female substance abusers with significant PTSD symptoms appear particularly likely to drink heavily in discriminative contexts that signal negative reinforcement (i.e., anxiety- or arousal-reduction) from drinking.
This pattern of situation-specific drinking in negative contexts may begin to explain why co-morbid PTSD-alcohol disorders are more difficult to treat successfully than alcohol disorders alone (e.g., Ouimette, Finney, & Moos, 1999). In the general population and in problem drinkers, a tendency to drink in negative contexts is correlated with increasing levels of alcohol depen-dence, whereas drinking in positive contexts is correlated with less risky social drinking (Cunningham, Sobell, Sobell, Gavin, & Annis, 1995). In fact, PTSD symptoms were only significantly positively correlated with drinking in situations that do not necessitate the presence of others (i.e., when experi-encing negative emotions or physical discomfort, or following interpersonal conflict) suggesting that traumatized female substance abusers with signifi-cant PTSD symptoms are likely to be relatively solitary drinkers. Solitary drinking may be ‘‘riskier’’ than drinking in social contexts because no drink-ing companions are present in solitary contexts against which a drinker can compare and regulate her own drinking level (Samoluk, Stewart, Sweet, & MacDonald, 1999).
Unexpectedly, frequency of PTSD symptoms was also significantly nega-tively correlated with frequency of heavy drinking in Pleasant Emotions situations. Thus, traumatized female substance abusers with significant PTSD symptoms appear less likely than others to drink in response to Pleas-ant Emotions. Whether this finding might be explained by the emotional numbing (e.g., difficulties experiencing pleasurable emotions) characteristic of PTSD (DSM-IV; APA, 1994) represents an interesting question for future research.
Consistent with previous findings that certain anxiety-related personality factors (N and AS) are elevated among those with PTSD (cf. McFarlane, 1989; Taylor et al., 1992), PSS-SR Total scores were correlated with both AS and N levels in the present sample of women substance abusers. AS and N were themselves significantly inter-correlated, sharing about 10% overlap-ping variance (cf. Lilienfeld, 1999). Also, AS and N were both associated with more frequent heavy drinking in negative contexts in general, and with more frequent heavy drinking in situations involving Unpleasant Emotions and Conflict with Others in particular (cf. Cannon et al., 1992; Samoluk & Stewart, 1998). AS (but not N) was also significantly associated with more frequent heavy drinking in Physical Discomfort situations (cf. Samoluk &
Stewart, 1998). This is not surprising given that AS involves a fear of anxi-ety-related physical sensations including some of the sensations on the IDS-42 Physical Discomfort scale.
As predicted, we found evidence for the ‘‘mediating’’ role of the personal-ity variable of AS in explaining the association between PTSD symptoms and situation-specific drinking in negative contexts. Regression analyses showed that AS (but not N) mediated the observed associations between PTSD symp-toms and situation-specific heavy drinking in negative contexts in general, and Conflict with Others and Physical Discomfort situations in particular. In other words, those female substance abusers with more frequent PTSD symp-toms drink heavily in certain negative situations (i.e., contexts involving Conflict with Others and Physical Discomfort) at least partly because they are highly fearful of anxiety symptoms (Stewart et al., 1999b). Unexpectedly, neither AS nor N significantly mediated the observed association between PTSD symptoms and situation-specific drinking in Unpleasant Emotions contexts. However, IDS-42 Unpleasant Emotions items tap negative affect drinking contexts in general, as opposed to anxious affect contexts in particu-lar. Theoretically, AS should motivate heavy drinking in situations involving anxious emotions, as opposed to those involving dysphoric or angry emo-tions.
Several potential limitations of the present study should be acknowledged. Our correlational design precludes drawing any firm conclusions regarding direction of causation, or even causation, per se. Moreover, to the extent that
recentPTSD symptoms (as assessed with the PSS-SR) are effectively damp-ened by current alcohol use (Stewart, 1996), true relations between PTSD symptoms and frequency of heavy drinking across various contexts may be underestimated in the current study. Additionally, the present study did not address the degree to which the situational-specificity hypothesis applies to the relation between PTSD and the misuse of substances other than alcohol. However, a recent study by Sharkansky, Brief, Peirce, Meehan, and Mannix (1999) with a largely (98%) male, clinical sample of 86 substance abusers suggests a relation between PTSD diagnoses and situation-specific drug-tak-ing in negative situations similar to the results reported here for heavy drink-ing. The present methods also relied on retrospective memory, which can be subject to distortions and error; future studies should supplement retrospec-tive self-report methods with alternaretrospec-tive methodologies. For example, the prospective daily diary method (cf. Swendson, Tennen, Carney, Affleck, Willard, & Hromi, in press), in which co-morbid PTSD-alcohol abusing patients monitor their PTSD symptoms and their drinking behavior in specif-ic situations, could be used to better establish true functional relations be-tween PTSD symptoms and situation-specific drinking in negative contexts. The present findings also do not establish whether the situation-specific
drinking pattern of substance abusing women with significant PTSD symp-toms is actually learned due to the negatively-reinforcing consequences of drinking in these situations. Lab-based alcohol challenge studies (e.g., Stew-art & Pihl, 1994) could be used to examine the effects of alcohol administra-tion in individuals with PTSD vs. controls, to determine whether PTSD patients are particularly sensitive to short-term alcohol-induced anxiety symptom-reduction effects, for example. Finally, alcohol self-administration methods (e.g., Samoluk et al., 1999) could be used to determine if exposure to relevant discriminative contextual stimuli (e.g., anxiety induction) in-creases drinking among PTSD patients in the lab.
Although statistically significant, the magnitudes of the relations between PSS-SR scores and frequency of drinking in negative contexts were relatively weak. Several factors may account for these relatively weak associations. First, the relation between PTSD symptoms and situation-specific heavy drinking in negative contexts may be stronger in clinic- vs. community-re-cruited samples (i.e., an illness severity issue; Stewart, 1996). Second, the PSS-SR (Foa et al., 1993) reflects overall frequency of DSM-IV (APA, 1994) PTSD symptoms but does not assess their severity. Falsetti, Resnick, Resick, and Kilpatrick’s (1993) PTSD symptom measure, which assesses severity of PTSD symptoms, could be used in future to determine whether stronger relations would be observed between PTSD symptomseverityand situation-specific heavy drinking in negative contexts. Third, although the present study focused on heavy drinking behavior, the sample consisted of a hetero-geneous group of substance abusers (i.e., alcohol and/or prescription drug abusing/dependent women, many of whom were also abusing other sub-stances). Relations between PTSD symptoms and situation-specific heavy drinking thus could have been minimized by the inclusion of women who may have been using substances other than alcohol for similar purposes. Fourth, reference events for our assessment of PTSD symptoms varied wide-ly in severity, from classic Criterion A events (e.g., sexual and physical assault) to stressors of lower magnitude (e.g., abortion). Some individuals may experience PTSD symptoms in response to ‘‘sub-threshold’’ traumatic events (March, 1993). Nonetheless, the relatively liberal definition of trauma used in the present study may have led to an underestimation of the true relation between PTSD symptoms and degree of situation-specific drinking in negative contexts, for those women exposed to clear DSM-IV (APA, 1994) Criterion A events. Finally, the IDS-42 content was developed with respect to the typical heavy drinking situations reported by male alcoholics in general (Annis et al., 1987; Marlatt & Gordon, 1985). As such, the IDS-42 negative drinking context items may not most aptly reflect the heavy drinking situa-tions most typical of women with co-morbid PTSD-alcohol use disorders (e.g., sexual encounters for women with sexual trauma histories; experience
of startle, sleep difficulties, traumatic nightmares, or flashbacks). Assessment of relations between PTSD symptoms and frequency of heavy drinking in these more ‘‘PTSD-specific’’ drinking situations might provide stronger sup-port for the situational-specificity hypothesis.
Several therapy implications emerge from the present findings. Long-term treatment outcome is poorer among co-morbid PTSD-substance disordered patients than among patients with substance disorders alone (Ouimette et al., 1999), and substance abuse relapse occurs more quickly following treatment among substance abusers with PTSD (Brown, Stout, & Mueller, 1996). Since the present results suggest that the heavy drinking behavior of substance abusing women with significant PTSD symptoms is relatively situation-spe-cific, relapse-prevention approaches (Marlatt & Gordon, 1985) targeting their tendency toward increased heavy drinking in situations signaling potential negative reinforcement may be particularly beneficial for co-morbid PTSD-alcoholic women. Specifically, therapy should attend to training these women in healthier methods of dealing with negative affect, interpersonal conflict, and physical discomfort experiences. Moreover, the present study provided strong support for AS as a mediating or intervening personality variable in explaining the ‘‘risky’’ situation-specific heavy drinking pattern of trauma-tized female substance abusers with significant PTSD symptoms. Thus, the efficacy of interventions for this type of substance abuser may be enhanced by the inclusion of established therapy strategies that focus on AS-reduction (Otto & Reilly-Harrington, 1999). Future research could address whether the addition of such AS-reduction strategies improves therapy outcome for co-morbid PTSD-alcohol abusing women relative to standard alcoholism inter-ventions alone.
REFERENCES
American Psychiatric Association (1994).Diagnostic and statistical manual of men-tal disorders, Fourth Edition (DSM-IV). Washington, DC: American Psychiatric Press.
Annis, H. M., Graham, J. M., & Davis, C. S. (1987).Inventory of Drinking Situations (IDS) User’s Guide. Toronto, Canada: Addiction Research Foundation.
Baron, R. M., & Kenny, D. A. (1986). The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical consider-ations.Journal of Personality and Social Psychology,51, 1173-1182.
Brown, P. J., Stout, R. L., & Mueller, T. (1996). Posttraumatic stress disorder and substance use relapse among women: A pilot study. Psychology of Addictive Behaviors,10, 124-128.
Cannon, D. S., Rubin, A., Keefe, C. K., Black, J. L., Leeka, J. K., & Phillips, L. A. (1992). Affective correlates of alcohol and cocaine use.Addictive Behaviors,17, 517-524.
C-DIS Management Group (1991). Computerized Diagnostic Interview Schedule (Revised) for DSM-III-R. Ottawa, Canada: Author.
Costa, P. T., Jr., & McCrae, R. R. (1992).NEO-PI-R: Professional manual. Odessa, FL: Psychological Assessment Resources.
Covington, S. S. (1983). Sexual experience, dysfunction and abuse: A descriptive study of alcoholic and nonalcoholic women [Summary].Dissertation Abstracts International,44, 287B.
Cunningham, J. A., Sobell, M. B., Sobell, L. S., Gavin, D. R., & Annis, H. (1995). Heavy drinking and negative affect situations in a general population and treat-ment sample: Alternative explanations. Psychology of Addictive Behaviors, 9, 123-127.
Everstine, D. S., & Everstine, L. (1993).The trauma response: Treatment for emo-tional injury. New York: W. W. Norton.
Falsetti, S. A., Resnick, H. S., Resick, P. A., & Kilpatrick, D. G. (1993). The Modi-fied PTSD Symptom Scale: A brief self-report measure of posttraumatic stress disorder.Behavior Therapist,16, 161-162.
Foa, E. B., Riggs, D. S., Dancu, C. B., & Rothbaum, B. O. (1993). Reliability and validity of a brief instrument for assessing posttraumatic stress disorder.Journal of Traumatic Stress,6, 459-473.
Foa, E. B., Riggs, D. S., & Gershuny, B. S. (1995). Arousal, numbing and intrusion: Symptom structure of PTSD following assault.American Journal of Psychiatry, 152, 116-120.
Fullilove, M. T., Fullilove, R. E. III, Smith, M., Winkler, K., Michael, C., Panzer, P. G., & Wallace, R. (1993). Violence, trauma, and posttraumatic stress disorder among women drug users.Journal of Traumatic Stress,6, 533-543.
Lilienfeld, S. O. (1999). Anxiety sensitivity and the structure of personality. In S. Taylor (Ed.),Anxiety sensitivity: Theory, research, and treatment of the fear of anxiety(pp. 149-180). Mahwah, NJ: Erlbaum.
March, J. S. (1993). What constitutes a stressor? The ‘‘Criterion A’’ issue. In J. R. T. Davidson & E. B. Foa (Eds.),Posttraumatic stress disorder: DSM-IV and beyond (pp. 37-54). Washington, DC: American Psychiatric Press.
Marlatt, G. A., & Gordon, J. R. (1985). Relapse prevention. New York: Guilford Press.
Martin, E. D., & Sher, K. J. (1994). Family history of alcoholism, alcohol use disorders, and the five-factor model of personality.Journal of Studies on Alcohol, 55, 81-90.
Miller, B. A., Downs, W. R., & Testa, M. (1993). Inter-relationships between victim-ization experiences and women’s alcohol use. Journal of Studies on Alcohol, Suppl. 11, 109-117.
McFarlane, A. C. (1989). The aetiology of post traumatic morbidity: Predisposing, precipitating and perpetuating factors. British Journal of Psychiatry, 154, 221-228.
Otto, M. W., & Reilly-Harrington, N. A. (1999). The impact of treatment on anxiety sensitivity. In S. Taylor (Ed.),Anxiety sensitivity: Theory, research, and treatment of the fear of anxiety(pp. 321-336). Mahwah, NJ: Erlbaum.
functioning and coping of substance abuse patients with posttraumatic stress disorder.Psychology of Addictive Behaviors,13(2), 105-114.
Peterson, R. A., & Reiss, S. (1992).Anxiety Sensitivity Index Manual (2nd edition). Worthington, OH: International Diagnostic Systems.
Pokorny, A. D., Miller, B. A., & Kaplan, H. B. (1972). The Brief MAST: A shortened version of the Michigan Alcoholism Screening Test.American Journal of Psy-chiatry,129, 342-345.
Samoluk, S. B., & Stewart, S. H. (1998). Anxiety sensitivity and situation-specific drinking.Journal of Anxiety Disorders,12, 407-419.
Samoluk, S. B., Stewart, S. H., Sweet, S. D., & MacDonald, A. B. (1999). Anxiety sensitivity and social affiliation as determinants of alcohol consumption. Behav-ior Therapy,30, 285-303.
Sharkansky, E. J., Brief, D. J., Peirce, J. M., Meehan, J. C., & Mannix, L. M. (1999). Substance abuse patients with posttraumatic stress disorder (PTSD): Identifying specific triggers of substance abuse and their associations with PTSD symptoms. Psychology of Addictive Behavior,13(2), 89-97.
Skinner, B. F. (1938).Behavior of organisms. New York: Appleton-Century-Crofts. Skinner, H. A. (1982). The Drug Abuse Screening Test. Addictive Behaviors, 7,
363-371.
Stewart, S. H. (1996). Alcohol abuse in individuals exposed to trauma: A critical review.Psychological Bulletin,120, 83-112.
Stewart, S. H., Conrod, P. J., Pihl, R. O., & Dongier, M. (1999a). Relations between posttraumatic stress symptom dimensions and substance dependence in a commu-nity-recruited sample of substance abusing women.Psychology of Addictive Be-haviors,13(2), 78-88.
Stewart, S. H., & Pihl, R. O. (1994). The effects of alcohol administration on psycho-physiological and subjective-emotional responses to aversive stimulation in anxi-ety sensitive women.Psychology of Addictive Behaviors,8, 14-17.
Stewart, S. H., Pihl, R. O., Conrod, P. J., & Dongier, M. (1998). Functional associa-tions among trauma, PTSD, and substance-related disorders.Addictive Behaviors, 23, 797-812.
Stewart, S. H., Samoluk, S. B., Conrod, P. J., Pihl, R. O., & Dongier, M. (in press). Psychometric evaluation of the short form Inventory of Drinking Situations (IDS-42) in a community-recruited sample of women substance abusers.Journal of Substance Abuse.
Stewart, S. H., Samoluk, S. B., & MacDonald, A. B. (1999b). Anxiety sensitivity and substance use and abuse. In S. Taylor (Ed.),Anxiety sensitivity: Theory, research, and treatment of the fear of anxiety(pp. 287-319). Mahwah, NJ: Erlbaum. Swendson, J., Tennen, H., Carney, M. A., Affleck, G., Willard, A., & Hromi, A. (in
press). Mood and alcohol consumption: An experience sampling test of the self-medication hypothesis.Journal of Abnormal Psychology.
Taylor, S., Koch, W. J., & McNally, R. J. (1992). How does anxiety sensitivity vary across the anxiety disorders?Journal of Anxiety Disorders,6, 249-259.