R E S E A R C H A R T I C L E
Open Access
A quantitative analysis method for
comitant exotropia using
video-oculography with alternate cover
Nohae Park
1, Byunggun Park
1, Minkyung Oh
2, Sunghyuk Moon
1*and Myungmi Kim
3Abstract
Background:The purpose of this study was to evaluate the efficacy of a quantitative analysis method for comitant exotropia using video-oculography (VOG) with alternate cover.
Methods:Thirty-four subjects with comitant exotropia were included. Two independent ophthalmologists measured the angle of ocular deviation using the alternate prism cover test (APCT). The video files and data of changes in ocular deviation during the alternate cover test were obtained using VOG. To verify the accuracy of VOG, the value obtained using VOG and the angle of a rotating model eye were compared, and a new linear equation was subsequently derived using these data. The calculated values obtained using VOG were compared with those obtained using the APCT.
Results:Rotation of the model eye and the values obtained using VOG demonstrated excellent positive correlation (R= 1.000;p< 0.001). A simple linear regression model was obtained: rotation of the model eye = 0.978 × value obtained using VOG for a model eye–0.549. The 95% limit of agreement for inter-observer variability was ±4.63 prism diopters (PD) for APCT and that for test-retest variability was ±3.56 PD for the VOG test. The results of APCT and calculated VOG test demonstrated a strong positive correlation. Bland-Altman plots revealed no overall tendency for the calculated values obtained from VOG to differ from those obtained using APCT.
Conclusions:VOG with alternate cover is a non-invasive and accurate tool for quantitatively measuring and recording ocular deviation. In particular, it is independent of the proficiency of the examiner and, can therefore, be useful in the absence of skilled personnel.
Trial registration:ClinicalTrial.gov,NCT03119311, Date of registration: 04/17/2017, Date of enrolment of the first participant to the trial: 04/25/2017.
Keywords:Strabismus, Video-oculography, Ocular deviation, Alternate cover
Background
Accurate measurements are important for planning stra-bismus surgery. Methods available for measuring the angle of ocular deviation include the alternate prism cover test (APCT), Hirschberg test, and Krimsky test. In APCT, the subject gazes at the target with both eyes, a prism is placed in front of the uncovered eye, and an al-ternate cover test is performed. The angle is measured by increasing or decreasing the strength of the prism
used until there is no deviation or the deviation is re-versed. However, the prism must be changed several times, especially when there is an accompanying vertical strabismus. Consequently, the duration of the examin-ation will be long in such cases and, as such, it is diffi-cult to perform in a child who does not cooperate or gaze in accordance with instructions. In such situations, the Hirschberg and Krimsky tests are used to determine the angle of deviation. The Hirschberg test measures the distance between the corneal light reflex and the center of the pupil, and then converts it into an angle. Al-though it is a relatively simple method, it may not accur-ately measure the exact ocular deviation. The Krimsky * Correspondence:[email protected]
1Department of Ophthalmology, Busan Paik Hospital, Inje University College
of Medicine, 75 Bokji-ro, Busanjin-gu, Busan 47392, Republic of Korea Full list of author information is available at the end of the article
test measures the angle of ocular deviation using a prism and the corneal light reflex. For this reason, APCT mea-sures the entire deviation, including tropic and phoric components, whereas the Krimsky tests only measure the tropic component. Both the Hirschberg and Krimsky tests require correction of angle kappa, which is largely subjective and, therefore, can lead to intobserver er-rors. When the goal of surgery is to achieve orthotropia, APCT should be used whenever possible [1]. In addition, such tests may have limitations in recording eye move-ments themselves.
On the other hand, a scleral search coil can be used to objectively record and measure ocular deviation. This is an accurate method because it has a spatiotemporal resolution < 1° and < 1 ms. However, it is difficult to wear a scleral search coil for more than 30 min because it is worn on the limbus of the cornea. Therefore, pho-tography and video-oculography (VOG) have been pro-posed as methods to measure eye movements noninvasively and objectively [2–6]. VOG has demon-strated a measurement error < 1° for an eye movement range < 40°, and a high correlation (R2= 0.99) with the scleral search coil method for both horizontal and vertical eye movements below 15° [6, 7]. In particular, several studies have reported measuring ocular deviation in intermittent exotropia using VOG [8–10]. To our knowledge, there has been no attempt to quantitatively measure ocular deviation using VOG with dissociation of both eyes. We believe it is important to measure ocular deviation with dissociation of both eyes, similar to APCT, for surgery. Therefore, we attempted a method of using VOG with alternate cover for non-invasive and reliable measurement of the angle of ocular deviation. Additionally, we evaluated VOG as an alternative method to standard tests to determine whether it can obviate these limitations.
Methods
This prospective study was performed at the Depart-ment of Ophthalmology, Inje University Busan Paik Hospital. All aspects of the research protocol complied with the tenets of the Declarations of Helsinki and were approved by the Institutional Review Board of Inje Uni-versity Busan Paik Hospital (Busan, Korea). Written in-formed consent was obtained from all parents or legal guardians; children and adolescent assent forms were also provided for children 7 years of age and older.
Calibration of VOG using a model eye
A model eye with a pupil diameter of 5.5 mm and globe diameter of 26 mm was used to verify the accuracy of VOG. A protractor was attached to the center of the eyeball to verify the amount of rotation of the eyeball. Each of the two experiments was repeated four times,
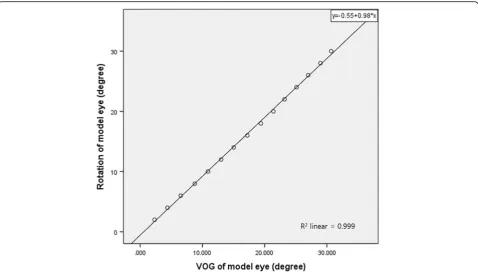
and a total of eight experiments were performed. The eyeball was rotated from 0° to 30° at intervals of 2°. The video taken of the model eye stopped for > 5 s every 2°. The degree of rotation of the eyeball and the values ob-tained using VOG were compared. Based on the results of the analysis, a linear regression equation for the de-gree of eyeball rotation was derived. In the reliability analysis of eight repeated VOG tests for a model eye, the intra-class correlation coefficient was 1.000 (95% confi-dence interval [CI] 1.000 to 1.000; p< 0.001). The intra-class correlation coefficient between the first measure-ment of two independent examiners was 1.000 (95% CI 0.999 to 1.000;p< 0.001). The VOG demonstrated excel-lent agreement among all eight repeated examinations. The linear regression equation was derived from the mean value of the eight VOGs and the rotated angle of the model eye using linear regression analysis (Fig.1).
Rotation angle of the model eye degreesð Þ ¼0:978 angle obtained using VOG degreesð Þ–0:549
Calculated VOG value prism dioptersð Þ ¼ tan rotation angle of the model eye degrees½
ð Þ 100
Participants
Thirty-four subjects with comitant exotropia who could be observed > 3 times, with a difference between distant and near deviation angle < 3 prism diopters (PD), were enrolled. All subjects underwent APCT to measure the angle of ocular deviation. On the same day, VOG (SLMED, Seoul, Korea) was performed and APCT was performed 30 min later. Subjects with incomitant stra-bismus, horizontal deviation > 50 PD in APCT, ocular comorbidity other than strabismus or with systemic dis-ease, refractive errors > 6.00 diopters, those not willing to undergo VOG, children < 4 years of age, and subjects wearing spectacles during measurements were excluded.
Comparison of APCT and VOG
Two independent ophthalmologists performed APCT using a plastic prism set (Luneau SAS, Prunay LeGillon, France). The subjects were asked to fixate on a black-on-white optotype at 3 m, which subtended a visual angle of 50 min of arc (MOA), equating to a Snellen optotype of 20/200.
The VOG equipment used in the present study had a tilted semi-transparent glass through which the subject could gaze at the target with a red light with a visual angle of 50 MOA in the monitor situated at 1 m. The subject wearing the VOG goggles was instructed to look at the red light, between the two eyes, with head pos-ition kept straight so that during the examination the
eyes were in primary position. During the first 10 s, ini-tial binocular alignment was verified with both eyes open. Subsequently, each eye was allowed 5 s of covered time and 5 s of uncovered time, and the alternate cover test was repeated 5 times, with each eye being covered for 5 s. A 120 Hz camera was used for VOG, and the eyeball was observed to deviate during the alternate cover test; the magnitude of deviation was subsequently obtained (Fig.2). The obtained values were expressed in
degrees (°), and were substituted into the linear regres-sion equation derived earlier using the model eye. The new angle values thus obtained were converted to PD to compare with the values obtained using APCT.
Main outcome measure
The inter-observer variability of APCT performed by two independent examiners and the inter-visit variability of four examinations by one examiner were measured.
Fig. 2Interface of the video-oculography device. This image reveals the degree of movement of the eyeball in the form of a graph. The red line refers to the movement of the right eye, and the amount of change in the two points (in the circle) is represented by an angle in the square
Fig. 1The rotation of the model eye and the value obtained using video-oculography demonstrated excellent positive correlation (R= 1.000;
The VOG recorded the distance moved by the eye dur-ing re-fixation after its deviation in the alternate cover; three repeated test values were obtained and a reliability analysis was performed. The first value among the re-sults obtained using VOG was used in the linear regres-sion equation and subsequently compared with the value obtained using APCT.
Statistical analysis
SPSS version 18.0 (SPSS, Inc., Chicago, Illinois, USA) was used for statistical analysis. The Pearson correlation coefficient was used to determine the linear relationship between VOG and the model eye, and the linear regres-sion equation was derived using linear regresregres-sion ana-lysis. The reliabilities of APCT and VOG were evaluated using intra-class correlation coefficient, and consistent variability between APCT and VOG was represented using a Bland-Altman plot. Correlation between the two tests was calculated using the Pearson correlation coefficient.
Results Participants
Thirty-four subjects with comitant exotropia, of whom 22 (64.7%) were female, were included in the present study. The mean age was 13.7 ± 11.2 years (range, 5– 51 years). Thirty-one of 34 subjects had uncorrected vis-ual acuity better than 20/30 in both eyes; uncorrected visual acuity in either eye of the other three subjects was not worse than 20/70. APCT and VOG were performed in all subjects (Table1).
Comparison of APCT and VOG
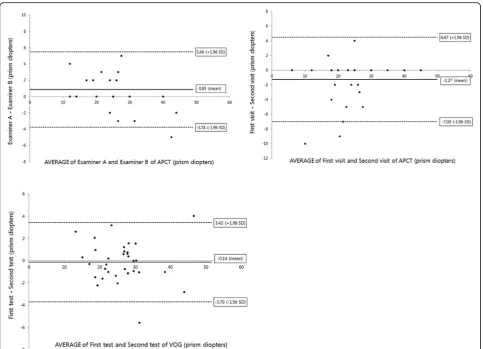
The inter-observer variability for APCT was determined using the results from two independent examiners. The Bland-Altman plot demonstrated consistent variability, ex-cept for one subject with deviation > 40 PD. The half-width of the 95% limit of agreement was ±4.63 PD (Fig.3 [top left]). On reliability analysis, the inter-observer correlation coefficient was 0.974 (95% CI 0.947 to 0.987;p< 0.001).
The inter-visit reliability of the APCT was determined for 24 of 34 subjects who had been examined by one examiner > 4 times in three months; the inter-visit correl-ation coefficient was 0.968 (95% CI 0.941 to 0.985;p< 0. 001). The Bland-Altman plot between the first and second APCT demonstrated consistent variability, except for two
subjects, the half-width of the 95% limit of agreement be-ing ±5.74 PD (Fig.3[top right]).
Thirty-four subjects were included in the VOG test. Reliability analysis of the three VOG readings demon-strated high agreement (0.990 [95% CI 0.983 to 0.995];p < 0.001), and the half-width of the 95% limit of agree-ment on Bland-Altman plot was ±3.56 PD (Fig. 3
[bottom]).
Of the 34 subjects, 28 (82.4%) exhibited a difference in ocular deviation of < 3 PD between VOG and APCT, and 32 (94.1%) demonstrated a difference of < 5 PD (Table2).
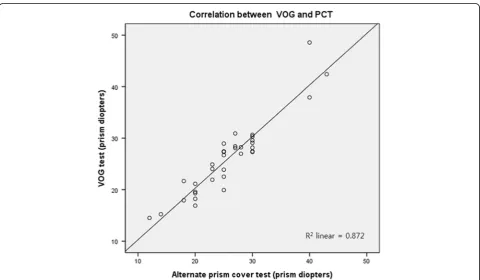
The Bland-Altman plot of VOG and APCT demon-strated consistent variability, except for two subjects, the half-width of the 95% limit of agreement being ±5.05 PD (Fig. 4). Furthermore, there was also a strong positive linear relationship between the two tests (R= 0.934; p< 0.001) (Fig.5).
Discussion
The purpose of our study was to measure the objective angle of ocular deviation using VOG with alternate cover in subjects with exotropia. The principle of the VOG device used in our study was that light was trans-mitted through the tilted semi-transparent glass and the subject could look at the target. As the light was being reflected, the two cameras could record the movement of the eyes without blocking the visual axes. The pupil was detected in real time, and the deviation of the eye-ball was assessed by measuring the change in the refer-ence point of the center of the pupil.
Although APCT may represent a typical test for meas-uring angles of deviation, the results can differ because of differences in measurements using prisms made by individual examiners. Therefore, error involved in the measurements are dependent on the skill of the exam-iner and the cooperation of the subject [11–13]. In par-ticular, the Pediatric Eye Disease Investigator group [11] suggested that two skilled observers may have an error≥ 12 PD in the measurement of esotropia exceeding 20 PD, and an error≥6 PD in the measurement of 10 to 20 PD esotropia. The angle of ocular deviation measured by one observer demonstrated that the 95% limit of agree-ment on a measureagree-ment was ±7.3 PD for esotropia ex-ceeding 20 PD, and ± 4.1 PD for 10–20 PD esotropia at distance. In addition, APCT could not record eye
Table 1Mean angle of exotropia measured using alternate prism cover test and video-oculography
Value Alternate prism cover test (n= 34) Video-oculography (n= 34)
Examiner 1 Examiner 2 Average value of three test-retests Calculated value from linear equation
Degrees 14.32 ± 3.66 (6.84–23.27) 13.84 ± 4.14 (5.71–24.23) 15.47 ± 3.91 (8.50–26.58) 14.58 ± 3.83 (7.77–25.44)
Prism diopters 25.65 ± 6.88 (12–43) 24.79 ± 7.81 (10–45) 27.81 ± 7.52 (14.95–50.02) 26.13 ± 7.28 (13.64–47.57)
Data presented as mean ± SD (range)
movement itself; therefore, it depends on the record of the examiner. For this reason, methods using photog-raphy were used for measurements that are more object-ive. Among them, Yang et al. [2] took pictures at a distance of 1 m, and the corneal light reflex points and limbus locations were extracted from two-dimensional photographs and analyzed using a three-dimensional strabismus photo analyzer (R & DB Foundation, Seoul, Republic of Korea). The results demonstrated high cor-relation with the Krimsky test. This is useful to examine
cases of manifest strabismus. However, because this test did not dissociate the two eyes, the angle of ocular devi-ation would be variable according fusion of both eyes in intermittent exotropia, or changeable depending on dominant eye in incomitant strabismus. Therefore, there are restrictions to its use in intermittent exotropia and incomitant strabismus. Additionally, there are limitations in measuring the angle of ocular deviation for retinop-athy of prematurity with macular dragging because the angle kappa cannot be considered. In another improve-ment study, the use of an infrared ray filter and an infra-red camera with this method was proposed to observe the deviation angle in patients with latent strabismus [3]. An alternative for objectively measuring eye move-ments is to use a VOG device equipped with a camera at a sample rate of 200 to 250 Hz. In previous studies, it was reported to have high correlation with the scleral search coil in the fixation position [6, 7]. The VOG de-vice used in our study had a frequency of 150 Hz; hence,
Fig. 3Bland-Altman plots revealing interobserver variability and inter-visit variability for the alternate prism cover test (APCT) and test-retest variability for video-oculography with alternate cover. Upper and lower dotted lines represent the 95% limits of agreement. The half-width of the 95% limit of agreement measured of the interobserver variability (top left), inter-visit variability (top right) for APCT and test-retest variability (bottom) for video-oculography were 4.63 prism diopters (PD), 5.74 PD and 3.56 PD, respectively
Table 2Differences between alternate prism cover test and video-oculography
Prism diopters Subjects, n (%)
< 3 28 (82.4)
3–5 4 (11.7)
> 5 2 (5.9)
it was less accurate than the scleral search coil used to assess rapid eye movements. However, because our study was intended to measure the distance moved during an eyeball deviation, the results were not greatly influenced by camera frequency. In our study, we needed a device verification step to accurately measure the amount of
eyeball rotation. The results obtained using VOG and the amount of eyeball rotation showed statistically high correlation (linear correlation coefficient = 1.000; p< 0. 001), and a linear regression equation of the eyeball rota-tion angle with the angle obtained using VOG was de-rived. Using this equation, the degree of ocular change
Fig. 4Bland-Altman plot comparing the values obtained using the alternate prism cover test (APCT) and video-oculography (VOG) test. The Bland-Altman plot demonstrated consistent variability. The half-width of the 95% limit of agreement was ±5.05 prism diopters. There was no overall tendency for the values obtained using VOG to differ from those obtained using APCT
Fig. 5Scatter plot and Pearson correlation between values calculated using video-oculography (VOG) and the values obtained using the alternate prism cover test (APCT). The values calculated from VOG demonstrated a strong correlation with the values obtained using APCT
(R= 0.934;p< 0.001)
in the subject group measured using VOG was verted to actual eyeball rotation angle values. These con-verted values were compared with the angles of ocular deviation obtained using APCT. The Bland-Altman plot between the APCT values and the calculated VOG values showed consistent variability, except for two sub-jects. As for the outliers, one subject exhibited ocular deviation values of 20, 20, and 25 PD from the three APCTs, and 19.92 PD from VOG testing. In our study setting, ocular deviation was analyzed based on the last visit, and was judged to be located outside the 95% limits of agreement. The other subject had exotropia with inferior oblique overaction in both eyes. It was V-pattern exotropia with 55 PD in the upward gaze, 40 PD in the primary position, and 35 PD in the downward gaze. We presume that the upward gaze may have been the cause of the positive difference despite maintenance of head position.
The advantage of using VOG is that all eye move-ments can be recorded as video recordings, and the eye tracking system can record both eye movements and the angle of ocular deviation. Another advantage is the dis-sociation of the two eyes using alternate covering, and measurement of the distance moved by the eye by re-cording a video. Hence, VOG is not influenced by the angle kappa. Several studies reporting the objective measurement of strabismus were influenced by the angle kappa because their assessments were based on corneal light reflex points. In addition, the measurement of the manifest strabismus alone was performed without dis-sociating the two eyes [2, 5, 14–16]. In contrast, in a study measuring the angle of ocular deviation by dissoci-ating the two eyes, Yang et al. [3] used an infrared trans-mission filter for dissociation and measured the ocular deviation using photographs. However, because photo-graphs―unlike video recordings―do not reflect the continuity of time, it is different from the method used in our study in that it does not record eye movement in real time. Therefore, if we analyze the angle of ocular deviation by the method used in our study with the aid of VOG, we can analyze deviation patterns in dissociated strabismus cases and use it for screening in intermittent exotropia with good convergence. Second, it is also use-ful for measuring the maximum angle of ocular devi-ation, which is significant in intermittent exotropia. Third, it can measure the ocular deviation in a short time. It took approximately 2 min during the VOG test (1 min for wearing goggles, 1 min for performing VOG with alternate cover). Finally, because VOG can quanti-tatively record and compare eye movements in both eyes separately, it is possible to accurately analyze the differ-ence between secondary and primary deviations in inco-mitant strabismus. This may be useful for follow-up observations. The purpose of our study was to evaluate
the accuracy of VOG and to include the inter-visit vari-ability of a single examiner in the process of comparing and analyzing the degree of variability of APCT mea-surements. However, paralysis, a type of incomitant stra-bismus, was excluded from our study because there can be changes in ocular deviation during recovery. In the future, we will perform a comparative analysis of both eyes in cases of incomitant strabismus such as paralysis.
Conclusion
VOG with alternate cover can be used to quantitatively and non-invasively measure the angle of ocular devi-ation, and more reliably. Moreover, the corrected values demonstrate high agreement with APCT values. Because this test is not significantly influenced by the skill of the examiner, it can accurately measure the angle of ocular deviation, even in the absence of an expert and record of ocular deviation itself. In particular, it is highly valuable as a screening test that can detect strabismus in many patient populations.
Abbreviations
APCT:Alternate prism cover test; MOA: Min of arc; PD: Prism diopters; VOG: Video-oculography
Acknowledgments None.
Funding
This study was supported by 2016 Inje University Busan Paik Hospital research grant.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Authors’contributions
SHM and NHP designed study, collected data, interpreted statistical analysis and drafted paper. BGP contributed to the analysis and interpretation of data at revision process. MMK aided in study design, acquisition of resources and review of the manuscript. MKO interpreted statistical analysis. All authors read and approved the final manuscript.
Ethics approval and consent to participate
All aspects of the research protocol complied with the tenets of the
Declarations of Helsinki and were approved by the Institutional Review Board of Inje University Busan Paik Hospital (Busan, Korea). Written informed consent was obtained from all parents or legal guardians; children and adolescent assent forms were also provided for children 7 years of age and older.
Consent for publication Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author details
1Department of Ophthalmology, Busan Paik Hospital, Inje University College
of Medicine, 75 Bokji-ro, Busanjin-gu, Busan 47392, Republic of Korea.
2Department of Pharmacology, Busan Paik Hospital, Inje University College of
medicine, Busan, Republic of Korea.3Department of Ophthalmology, Yeungnam University College of Medicine, Daegu, Republic of Korea.
Received: 18 July 2017 Accepted: 16 March 2018
References
1. Choi RY, Kushner BJ. The accuracy of experienced strabismologists using the Hirschberg and Krimsky tests. Ophthalmology. 1998;105:1301–6.
2. Yang HK, Han SB, Hwang JM, Kim YJ, Jeong CB, Kim KG. Assessment of binocular alignment using the three-dimensional strabismus photo analyzer. Br J Ophthalmol. 2012;96:78–82.
3. Yang HK, Seo JM, Hwang JM, Kim KG. Automated analysis of binocular alignment using an infrared camera and selective wavelength filter. Invest Ophthalmol Vis Sci. 2013;54:2733–7.
4. von Noorden GK. Binocular vision and ocular motility: Theory and Management of Strabismus, 6. St. Louis: Mosby; 2002.
5. Quick MW, Boothe RG. A photographic technique for measuring horizontal and vertical eye alignment throughout the field of gaze. Invest Ophthalmol Vis Sci. 1992;33:234–46.
6. Houben MM, Goumans J, van der Steen J. Recording three-dimensional eye movements: scleral search coils versus video oculography. Invest Ophthalmol Vis Sci. 2006;47:179–87.
7. van der Geest JN, Frens MA. Recording eye movements with video-oculography and scleral search coils: a direct comparison of two methods. J Neurosci Methods. 2002;114:185–95.
8. Laria C, Pinero DP. Evaluation of binocular vision therapy efficacy by 3d video-oculography measurement of binocular alignment and motility. Binocul Vis Strabolog Q Simms Romano. 2013;28:136–45.
9. Hirota M, Kanda H, Endo T, Lohmann TK, Miyoshi T, Morimoto T, Fujikado T. Relationship between reading performance and saccadic disconjugacy in patients with convergence insufficiency type intermittent exotropia. Jpn J Ophthalmol. 2016;60:326–32.
10. Economides JR, Adams DL, Horton JC. Variability of ocular deviation in strabismus. JAMA Ophthalmol. 2016;134:63–9.
11. Pediatric Eye Disease Investigator Group. Interobserver reliability of the prism and alternate cover test in children with esotropia. Arch Ophthalmol. 2009;127:59–65.
12. Holmes JM, Leske DA, Hohberger GG. Defining real change in prism-cover test measurements. Am J Ophthalmol. 2008;145:381–5.
13. Hrynchak PK, Herriot C, Irving EL. Comparison of alternate cover test reliability at near in non-strabismus between experienced and novice examiners. Ophthalmic Physiol Opt. 2010;30:304–9.
14. Brodie SE. Photographic calibration of the Hirschberg test. Invest Ophthalmol Vis Sci. 1987;28:736–42.
15. Miller JM, Mellinger M, Greivenkemp J, Simons K. Videographic Hirschberg measurement of simulated strabismic deviations. Invest Ophthalmol Vis Sci. 1993;34:3220–9.
16. Hasebe S, Ohtsuki H, Tadokoro Y, Okano M, Furuse T. The reliability of a video-enhanced Hirschberg test under clinical conditions. Invest Ophthalmol Vis Sci. 1995;36:2678–85.
17. Yang HK, Hwang JM. The effect of target size and accommodation on the distant angle of deviation in intermittent exotropia. Am J Ophthalmol. 2011; 151:907–13. e901
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript at www.biomedcentral.com/submit