Bartłomiej Szynglarewicz
1, Rafał Matkowski
1, 2, Agnieszka Hałoń
3,
Iwona Gisterek
2, Józef Forgacz
1, Marek Pudełko
1, Jan Kornafel
2Initial Series of Low Anterior Resection
with an Autonomic Nerve-Preserving Technique
for Rectal Cancer Using an Ultrasound Scalpel*
Niska resekcja przednia raka odbytnicy
z zaoszczędzeniem nerwów autonomicznych
z użyciem noża ultradźwiękowego
– wstępne obserwacje wyników czynnościowych
1 2nd Department of Surgical Oncology, Lower Silesian Oncology Center, Wrocław, Poland 2 Department of Oncology, Wroclaw Medical University, Poland
3 Department of Pathomorphology, Wroclaw Medical University, Poland
Abstract
Background. Achieving effective local control and obtaining optimal functional outcomes are now both needed in the surgical management for rectal cancer.
Objectives. The aim of this study was to assess early functional results after low anterior resection performed with an ultrasound scalpel.
Material and Methods. Nineteen consecutive rectal cancer patients surgically treated during the years 2004–2008 with low anterior resection with sharp total mesorectal excision were studied. Dissection was performed with an ultrasound scalpel instead of electrocautery. The frequency of axial vibration and the extension of longitudinal vibration were 55.5 kHz and 75 µm, respectively. Special effort was made to identify and preserve autonomic nerves. Postoperative complications and functional results were analyzed.
Results. Surgery was completed with no intraoperative complications. The mean operating time was 150.20 ± 27.09 min. In each case, resection and anastomosis (straight, double-stapled) were done with ease. There was no post-operative mortality. Blood transfusion was not required. Neither anastomotic leakage nor abdominal infectious complications were noticed. Delayed wound healing and prolonged bowel paralysis occurred in two patients (13%) with diabetes and chronic obturative pulmonary disease, respectively. Urinary bladder disturbance developed in one female patient (7%) as stress incontinence. This dysfunction was transient, with symptoms being significantly reduced during the six postoperative months.
Conclusions. Based on this initial series, rectal dissection with an ultrasonic knife appears safe and seems to facili-tate autonomic nerve preservation, probably due to minimized thermal damage to tissue. Further investigations and cost-effectiveness analysis are needed to assess its usefulness for the routine surgical practice (Adv Clin Exp Med 2010, 19, 1, 113–119).
Key words: rectal cancer, low anterior resection, total mesorectal excision, autonomic nerves preservation, ultra-sound scalpel.
Streszczenie
Wprowadzenie. Obecnie w operacyjnym leczeniu raka odbytnicy istotne znaczenie ma zarówno uzyskanie sku-tecznej kontroli miejscowej nowotworu, jak i osiągnięcie optymalnych wyników czynnościowych.
Cel pracy. Ocena wczesnych wyników czynnościowych u pacjentów chorych na raka odbytnicy po niskiej resekcji przedniej wykonanej z użyciem noża ultradźwiękowego.
Materiał i metody. Analizą objęto dziewiętnastu kolejnych pacjentów operowanych z intencją radykalności
tech-Adv Clin Exp Med 2010, 19, 1, 113–119 ISSN 1230-025X
ORIGINAL PAPERS
© Copyright by Wroclaw Medical University
Anterior resection is nowadays the preferred option for the surgical management of most rectal cancers without sphincter infiltration. Since the introduction of total mesorectal excision (TME) by Heald et al.[1], adequate local control of rectal cancer and improved patient survival have been achieved compared with traditional resection. The value of a therapeutic procedure is also defined by side effects and functional results. The formation of a colon J-pouch or a transverse coloplasty pouch improves anorectal function after low anterior resec-tion [2, 3]. Autonomic nerve preservaresec-tion results in decreased risk of urogenital complications [4]. For all of these techniques, electrocautery remains the most often used surgical tool for mesorectal dissec-tion. However, the possible advantages of more pre-cise devices are currently being investigated [5].
The aim of this study was to assess the useful-ness of an ultrasonic knife for sphincter-preserv-ing total mesorectal excision.
Material and Methods
Patients
At the 2nd Department of Surgical Oncology of the Lower Silesian Oncology Center, fifteen patients with histologically confirmed UICC stage I–III rectal cancer underwent TME resection per-formed with an ultrasonic knife from January 2004 to December 2007. Eleven of them entered the study by fulfilling the inclusion criteria, i.e. prima-ry tumor located maximally 12 cm from the anal verge, absence of distant metastases, anterior resec-tion with sphincter preservaresec-tion, lack of intraop-erative bowel perforation, absence of macroscopic
infiltration of adjacent organs, and distal and radial margins microscopically free of cancer infiltration (R0 resection). Four patients were excluded from the analysis because of intraoperative perforation in one case and the kind of surgical management in the other patients (abdomino-sacral excision in two cases and Hartmann’s procedure in one). The data were collected in a prospective manner. The data are given in Table 1.
Surgical Treatment
All patients underwent elective surgery with preoperative bowel preparation by means of 4 l of polyethylene glycol solution one day before sur-gery. Prophylactic antibiotics were administered at anesthesia induction. Resection of the rectum was performed strictly according to the TME prin-ciples with sharp dissection under direct vision of the plane between the parietal and visceral pelvic fascia to the levator level (Figs. 1–4). Dissection was made with an ultrasonic knife. The rectum was mobilized to the pelvic floor and the lateral ligaments were divided as laterally as possible. Special effort was made to identify and preserve the hypogastric plexuses and the pelvic nerves. An end-to-end anastomosis was constructed using the double-stapling technique with a Proximate TLH transverse and a Proximate ILS circular intralu-minal device (Ethicon Endo-Surgery Europe, Norderstedt, Germany). Bowel washout was per-formed using a 2% povidone iodine solution.
Ultrasonic Knife
The ultrasonic knife (Ultracision, Ethicon Endo-Surgery Europe, Norderstedt, Germany)
niką całkowitego wycięcia mezorektum w latach 2004–2008, u których niską przednią resekcję wykonano całkowi-cie nożem ultradźwiękowym. Parametry pracy urządzenia wynosiły: osiowa częstotliwość drgań 55,5 kHz, zasięg wibracji pionowej 75 µm. W każdym przypadku podczas preparowania mezorektum szczególny nacisk kładziono na dokładną identyfikację i zaoszczędzenie nerwów autonomicznych miednicy. Prospektywnej ocenie poddano wczesne wyniki czynnościowe oraz częstość i rodzaj powikłań pooperacyjnych.
Wyniki. Powikłań śródoperacyjnych nie zaobserwowano. Średni czas zabiegu wynosił 150,20 ± 27,09 min. U żad-nego pacjenta nie zaistniały techniczne trudności w wykonaniu resekcji i zespolenia (koniec do końca metodą dwu-staplerową). Nie wystąpiła śmiertelność pooperacyjna. W żadnym przypadku nie zaistniała potrzeba transfuzji pre-paratów krwiopochodnych. Nie stwierdzono nieszczelności zespolenia ani innych powikłań infekcyjnych w obrębie jamy brzusznej. Wydłużone gojenie rany i przedłużona pooperacyjna atonia jelit wystąpiły u dwóch pacjentów (13%) chorych na cukrzycę i przewlekłą obturacyjną chorobę płuc. Zaburzenia czynności pęcherza moczowego roz-winęły się u jednej pacjentki (7%) jako wysiłkowe nietrzymanie moczu. Dysfunkcja ta miała charakter przejściowy, ze znaczącym złagodzeniem objawów w ciągu 6 miesięcy po zabiegu.
Wnioski. Uzyskane wyniki wstępne wskazują, że całkowite wycięcie mezorektum nożem ultradźwiękowym jest zabiegiem bezpiecznym, który może ograniczyć ryzyko śródoperacyjnego uszkodzenia nerwów autonomicznych, prawdopodobnie dzięki niewielkiemu urazowi termicznemu preparowanych tkanek. Aby jednak ocenić przydat-ność tej techniki w rutynowej praktyce chirurgicznej, są potrzebne wyniki dalszych badań, z analizą wskaźnika koszt–efektywność włącznie (Adv Clin Exp Med 2010, 19, 1, 113–119).
Table 1. Patient characteristics and tumor pathology
Tabela 1. Dane kliniczne i histopatologiczne
No.
(Nr) Age (Wiek) Gender (Płeć) UICC stage (Stadium zaawansowania) Grade (Stopień dojrzałości histologicznej) Mucinous histology (Śluzowe utkanie raka) 1
2 3 4 5 6 7 8 9 10 11 12 13 14 15
52 67 46 77 73 75 51 49 78 68 72 65 73 58 77
female female male male female female male male male female male male female female male
I II II II I II III III II I I II III I II
I III II II I II III II II I II I III II II
absent absent present absent absent absent absent absent absent absent absent absent absent absent present
Fig. 1. Total excision of the mesorectum
Ryc. 1. Przednie wycięcie odbytnicy techniką całkowitego wycięcia mezorektum (TME)
Fig. 2. Sharp dissection under the direct vision
Ryc. 2. Preparowanie „na ostro” pod kontrolą wzroku
Fig. 3. Avascular plane between parietal and visceral lamina of the pelvic fascia
Ryc. 3. Beznaczyniowa przestrzeń między blaszką trzewną i ścienną powięzi miednicy
Fig. 4. Resected specimen (rectum with mesorectum)
includes a generator delivering electrical energy to a hand-piece, where it is transformed via piezo-electric crystals into mechanical energy in the form of vibration. The active blade of the instru-ment vibrates axially with a constant frequency of 55.5 kHz and the energy, liberated as a longi-tudinal ultrasound wave, is applied directly to the tissue. The longitudinal extension of the vibration can be varied between 50 and 100 µm in five steps (75, level 3, in the present study).
Adjuvant Therapy
Four patients with UICC stage I tumor did not receive neoadjuvant therapy. Five patients with stage II and III tumors received preoperative short-term scheduled radiation in five fractions of 5 Gy each to a total dose 25 Gy. One patient with stage II tumor did not undergo radiation due to misevaluation of the direct spread in the preop-erative staging. For one patient with metastases in one lymph node detected in postoperative patho-logical assessment, neoadjuvant radiotherapy was not given because of the lack of enlarged and sus-picious lymph nodes in the mesorectum in preop-erative endorectal ultrasound. Adjuvant therapy, tumor site, and anastomosis location are shown in Table 2.
Follow-Up
Follow-up was scheduled every three months during the first postoperative year and every six months thereafter. Physical examination, blood
tests, serum markers, barium enema, endoscopy, chest radiograph, and abdominal ultrasound were done. With every suspicion of a postoperative complication, a careful investigation using addi-tional clinical examination, blood tests, abdomi-nal ultrasound, endoscopy, gynecological exami-nation, colposcopy, endorectal sonography, or CT scanning was performed. Anastomotic leak was considered to be present if any of the following features were noted: the presence of peritonitis caused by anastomotic dehiscence, the presence of feculent substances and gas from the pelvic drain, or the presence of pelvic abscess with the demonstration of leakage by transrectal examina-tion, endoscopy, or imaging tests. Anastomosis stricture was deemed present when dilatation was needed. Anorectal physiology was evaluated clinically and dysfunction was defined by a fre-quency of bowel movements of more than 3 per 24 hours, urgency (lack of ability to defer defeca-tion for more than 15 minutes), incontinence (of gas, liquids, and solids), and inability to defecate and empty the neorectum in one attempt. Bladder disturbances were stated to be present when dysu-ria, nyctudysu-ria, stress, or complete incontinence was present. Patients were specifically asked about the use of soiling pads.
Results
Surgery was completed with no intraoperative complications. The mean operating time was 158 min. In each case, resection and anastomosis were
Table 2. Neoadjuvant therapy and tumor site data
Tabela 2. Leczenie przedoperacyjne, umiejscowienie guza i zespolenia jelitowego
No.
(Nr) Preoperative treatment (Terapia przedoperacyjna) Tumor site – cm* (Umiejscowienie guza) Anastomosis site – cm* (Umiejscowienie zespolenia) 1
2 3 4 5 6 7 8 9 10 11 12 13 14 15
not given radiotherapy radiotherapy radiotherapy not given radiotherapy not given not given radiotherapy not given not given radiotherapy radiotherapy not given not given
8 5 7 8 6 6 12 12 7 9 7 7 8 6 11
6 4 5 6 5 5 7 7 5 7 6 5 6 5 7 * from the anal verge.
done with ease. There was no postoperative mor-tality. Blood transfusion was not required. Neither anastomotic leakage nor abdominal infectious complications were noticed. Postoperative mor-bidity was found in three patients (27%) and was not severe. Delayed wound healing and prolonged bowel paralysis occurred in two patients (18%) with diabetes and chronic obturative pulmonary disease, respectively. Urinary bladder disturbance developed in one female patient (9%) as stress incontinence. Catheterization was not required. This dysfunction was transient, with symptoms being significantly reduced during the six postop-erative months. The results are presented in detail in Table 3.
Discussion
No anastomotic leak or anorectal disturbances were observed in this preliminary series. In con-trast, in a previous study, anorectal dysfunction
was found in 55% and anastomotic leakage in 5% of women after anterior resection with electro-cautery due to T4 rectal cancer [6]. In each series, approximately half of the patients underwent radiotherapy, but extended en bloc resection was performed for T4 tumors. Therefore it is hard to conclude that this difference can be caused by the surgical tool. The extent of tumor and the small group of patients in the present report are most likely to be the reason. Delayed wound healing caused by infection occurred in an elderly patient with diabetes, obesity, and steroid therapy. These features and comorbidity are the well-known risk factors of postoperative healing disorders after colorectal surgery, regardless of the dissection technique [7, 8].
Major and minor urogenital disturbances are common in up to 60% of patients following low anterior resection [9]. Damage to the sacral splanchnic nerves leads to detrusor denervation and decreased sensitivity of the bladder. Associated symptoms are difficulty with bladder emptying,
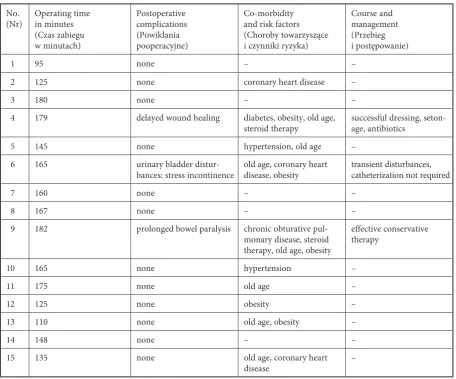
Table 3. Postoperative complications
Tabela 3. Powikłania pooperacyjne
No.
(Nr) Operating time in minutes (Czas zabiegu w minutach)
Postoperative complications (Powikłania pooperacyjne)
Co-morbidity and risk factors (Choroby towarzyszące i czynniki ryzyka)
Course and management (Przebieg i postępowanie)
1 95 none – –
2 125 none coronary heart disease –
3 180 none – –
4 179 delayed wound healing diabetes, obesity, old age,
steroid therapy successful dressing, seton-age, antibiotics
5 145 none hypertension, old age –
6 165 urinary bladder
distur-bances: stress incontinence old age, coronary heart disease, obesity transient disturbances, catheterization not required
7 160 none – –
8 167 none – –
9 182 prolonged bowel paralysis chronic obturative
pul-monary disease, steroid therapy, old age, obesity
effective conservative therapy
10 165 none hypertension –
11 175 none old age –
12 125 none obesity –
13 110 none old age, obesity –
14 148 none – –
15 135 none old age, coronary heart
overflow incontinence, and loss of sensation of fullness of the bladder. Loss of sympathetic inner-vation due to damage to the hypogastric nerves results in urgency and stress incontinence [10, 11]. The reported rates of bladder disturbances and sexual dysfunction are 6–25% and 13–30%, respectively [12–14]. Similarly to the present find-ing, most of these disorders (90%) are believed to be transient, with significant or complete reduc-tion within six months [15]. The risk of these com-plication can be significantly decreased by sharp dissection under direct vision with special effort to identify and preserve pelvic nerves and the hypogastric plexus [4, 9]. In a recent report by the present authors, the incidence of urogenital com-plications was decreased by a factor or more than five compared with a previous T4 tumor study [6]. Urological problems may occur in almost all cases of extended resections; lesions of neural struc-tures may be inevitable because of the extent of the tumor [16].
However, it may be also influenced by the surgical device used for dissection. The harmonic scalpel, which is known since 1979 [17], coagulates bleeding vessels, which are coapted by tamponad-ing and sealed with a denatured protein coagulum [18]. However, in contrast to electrocautery, the ultrasound scalpel can do this without desicca-tion (temperature above 100°C). The limited heat generation minimizes the zone of thermal injury [19]. The cutting mechanisms are also different from that observed with electrocautery, which increases the temperature of the cells, causing the water to vaporize, expand, and explode the cells. The harmonic scalpel can rupture cells because of vaporizing cellular water at a low temperature, which results in tissue separation and very precise cavitational cutting. Moreover, the vibrating blade
edge cuts tissue by stretching it beyond its elastic limit, especially in areas of high protein density. Therefore, the harmonic scalpel produces four times less lateral tissue damage than electrocau-tery [20]. No histological indications of thermal damage at a distance of more than 2 mm were reported [21]. This can be important for precise mesorectum dissection and the identification autonomic nerves and avoiding their injury. Less thermal damage to tissue was observed in ani-mal model studies [22]. In humans, the harmonic scalpel was first used in laparoscopic surgery [23]. Nowadays it has been adapted for colorectal sur-gery. Its usefulness for minimally invasive proce-dures, such as laparoscopic bowel resections [24, 25], transanal endoscopic microsurgery [26], and laparoscopic liver metastases excisions [27], has been reported. For an open approach, optimistic results from a series of abdominoperineal exci-sions and extended en bloc resections have been published [28, 29]. Reports on the use of the ultra-sonic knife for dissection of the mesorectum are rare [30]. In a series of Balogh and colleagues, the ultrasonic scalpel permitted atraumatic, blood-less, and oncologically correct dissection in low or ultra-low anterior resection patients with low morbidity and good functional results [30]. The present initial findings suggest that it may be a valuable tool for this surgical maneuver by minimizing tissue damage and facilitating auto-nomic nerve preservation.
Based on this initial series, rectal dissection with the ultrasonic knife appears safe and seems to facilitate autonomic nerve preservation, prob-ably due to minimized thermal damage to tis-sue. Further investigations and cost-effectiveness analysis are needed to assess its usefulness for the routine surgical practice.
References
Heald RJ, Ryall RD:[1] Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986, 1, 1479–1482.
Seow-Choen F:
[2] Colonic pouches in the treatment of low rectal cancer. Br J Surg 1996, 83, 881–882.
Z’graggen K, Maurer CA, Birrer S, Giachino D, Kern B, Buchler MW:
[3] A new surgical concept for rectal
replace-ment after low anterior resection. Ann Surg 2001, 234, 780–787.
Junginger T, Kneist W, Heintz A:
[4] Influence of identification and preservation of pelvic autonomic nerves in rectal cancer surgery on bladder dysfunction after total mesorectal excision. Dis Colon Rectum 2003, 46, 621–628.
Kockerling F, Yildirim C, Rose J, Scheidbach H, Geers P:
[5] Total mesorectal excision with the water-jet-dissection. Technique and results. Tech Coloproctol 2004, 8, Suppl 1, 217–225.
Matkowski R, Szynglarewicz B, Gisterek I, Lacko A, Kasprzak P, Sydor D, Forgacz J, Pudelko M, Kornafel J: [6]
Pre and postoperative radiochemotherapy and complication risk following en block total mesorectal and female genitalia excision for T4 rectal cancer. Colorectal Dis 2007, 9, Suppl 3, P209.
Barie PS, Eachempati SR:
[7] Surgical site infections. Surg Clin N Am 2005, 85, 1115–1135.
Raymond DP, Pelletier SJ, Crabtree TD, Schulman AM, Pruett TL, Sawyer RG:
[8] Surgical infection and the ageing
population. Am Surg 2001, 67, 827–832.
Pocard M, Zinzindohoue F, Haab F, Caplin S, Parc R, Tiret E:
[9] A prospective study of sexual and urinary
Fletcher TF, Bradley WE:
[10] Neuroanatomy of the bladder-urethra. J Urol 1978, 119, 153–160.
Daniels IR, Woodward S, Taylor FGM, Raja A, Toomey P:
[11] Female urogenital dysfunction following total mesorectal excision for rectal cancer. World J Surg Oncol 2006, 4, 6.
Maurer CA, Z’Graggen K, Renzulli P, Schilling MK, Netzer P, Buchler MW:
[12] Total mesorectal excision preserves
male genital function compared with conventional rectal cancer surgery. Br J Surg 2001, 88, 1501–1505.
Saha S, Booth MI, Dehn TC:
[13] The results of total mesorectal excision for rectal carcinoma in a district general hospital before the era of surgical specialization. Colorectal Dis 2002, 4, 36–40.
Shah EF, Huddy SP:
[14] A prospective study of genito-urinary dysfunction after surgery for colorectal cancer. Colorectal Dis 2001, 3, 122–125.
Sterk P, Shekarriz B, Gunter S, Nolde J, Keller R, Bruch HP, Shekarriz H:
[15] Voiding and sexual dysfunction after
deep rectal resection and total mesorectal excision: prospective study on 52 patients. Int J Colorectal Dis 2005, 20, 423–427.
Aleksic M, Hennes N, Ulrich B:
[16] Surgical treatment of locally advanced rectal cancer. Options and strategies. Dig Surg 1998, 15, 342–346.
Hodgson WJ:
[17] The ultrasonic scalpel. Bull N Y Acad Med 1979, 55, 908–915.
Foschi D, Cellerino P, Corsi F, Taidelli T, Morandi E, Rizzi A, Trabucchi E:
[18] The mechanisms of blood vessel
closure in humans by the application of ultrasonic energy. Surg Endosc 2002, 16, 814–819.
McCarus SD:
[19] Physiologic mechanism of the ultrasonically activated scalpel. J Am Assoc Gynecol Laparosc 1996, 3, 601–608.
Amaral JF:
[20] Ultrasonic dissection. Endosc Surg Allied Technol 1994, 2, 181–185.
Koch C, Friedrich T, Metternich F, Tannapfel A, Reimann HP, Eichfeld U:
[21] Determination of temperature
eleva-tion in tissue during the applicaeleva-tion of the harmonic scalpel. Ultrasound Med Biol 2003, 29, 301–309.
Tulikangas PK, Smith T, Falcone T, Boparai N, Walters MD:
[22] Gross and histologic characteristics of
laparo-scopic injuries with four different energy sources. Fertil Steril 2001, 75, 806–810.
Amaral JF:
[23] Laparoscopic application of a ultrasonically activated scalpel. Gastrointest Endosc Clin N Am 1993, 3, 381–391.
Targarona EM, Balague C, Marin J, Neto RB, Martinez C, Garriga J, Trias M:
[24] Energy sources for laparoscopic
colectomy: a prospective randomized comparison of conventional electrosurgery, bipolar computer-controlled electrosurgery and ultrasonic dissection. Operative outcome and costs analysis. Surg Innov 2005, 12, 339–344.
Msika S, Deroide G, Kianmanesh R, Iannelli A, Hay JM, Fingerhut A, Flamant Y:
[25] Harmonic scalpel in
laparo-scopic colorectal surgery. Dis Colon Rectum 2001, 44, 432–436.
Langer C, Markus P, Liersch T, Fuzesi L, Becker H:
[26] UltraCision or high-frequency knife in transanal endoscopic microsurgery (TEM)? Advantages of a new procedure. Surg Endosc 2001, 15, 513–517.
Shah SR, Sirivatanauksorn Y, Spalding DR, Davidson BR:
[27] Laparoscopic resection of liver metastasis using a har-monic scalpel. Indian J Gastroenterol 2001, 20, 72–73.
Maruta F, Sugiyama A, Matsushita K, Ishida K, Ikeno T, Shimizu F, Murakami M, Kawasaki S:
[28] Use of the
Harmonic Scalpel in open abdominoperineal surgery for rectal carcinoma. Dis Colon Rectum 1999, 42, 540–542.
Ike H, Shimada H, Fujii S, Kamimukai N, Ohshima T, Imada T:
[29] Extended abdominoperineal resection with
partial prostatectomy for T3 rectal cancer. Hepatogastroenterology 2003, 50, 377–379.
Balogh A, Zollei I, Varga L, Tiszlavicz L, Lazar G Jr, Bagi R, Palko A, Nagy F:
[30] Total mesorectal excision with
ultrasonic coagulation knife (“UltraCision”) in surgery of rectal cancer. Orv Hetil 2000, 141, 379–383.
Address for correspondence:
Rafał Matkowski
Wroclaw Medical University Department of Oncology Lower Silesian Oncology Center Plac Hirszfelda 12
53-413 Wrocław Poland
Phone: +48 71 368 93 91
E-mail [email protected], [email protected] Conflict of interest: None declared