ARTICLE
Atopic Dermatitis in Children in the United States,
1997–2004: Visit Trends, Patient and Provider
Characteristics, and Prescribing Patterns
Kimberly A. Horii, MDa, Stephen D. Simon, PhDb, Deede Y. Liu, MDc, Vidya Sharma, MBBS, MPHa
aSection of Dermatology andbOffice of Medical Research, Children’s Mercy Hospitals and Clinics, Kansas City, Missouri;cDepartment of Internal Medicine, University of
Kansas School of Medicine, Kansas City, Kansas
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.Atopic dermatitis is the most common chronic inflammatory skin disease of childhood and is increasing in prevalence throughout the world. Morbidity and resource use for atopic dermatitis are comparable to other chronic diseases. Topical corticosteroids are first-line therapeutic agents for atopic dermatitis; topical cal-cineurin inhibitors are considered second-line agents for patients who are older than 2 years. The aims of this study were to examine trends in visits for atopic dermatitis in children in the United States between 1997 and 2004, identify factors that were associated with a pediatric visit for atopic dermatitis, and assess changes in the treatment of atopic dermatitis over time.
METHODS.Visits for atopic dermatitis by children (0 –18 years) to office-based phy-sicians and hospital outpatient departments using 1997–2004 National Ambula-tory Medical Care Survey and National Hospital AmbulaAmbula-tory Care Survey data-bases were analyzed. Medication prescribing rates during 2 time periods (1997– 2000 and 2001–2004) were also analyzed.
RESULTS.There were an estimated 7.4 million visits for atopic dermatitis. Statistically significant differences in patients with atopic dermatitis included age 2 to 5 years, black race, Asian race, and specialist or hospital outpatient clinic evaluation. The increase in atopic dermatitis visits per year was statistically significant. No statis-tical differences in prescribing rates were identified between the 2 time periods. Between 1997 and 2000, topical corticosteroids were prescribed in 34% of visits, decreasing to 25% between 2001 and 2004. Between 2001 and 2004, topical calcineurin inhibitors were prescribed in 23% of visits. In the same period, topical corticosteroids were prescribed in 24% of visits by children who were younger than 2 years; topical calcineurin inhibitors were prescribed in 22% of visits.
CONCLUSIONS.Visits for atopic dermatitis in children are increasing. A recommended first-line treatment was prescribed in a minority of the visits.
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-0289
doi:10.1542/peds.2007-0289
Key Words
atopic dermatitis, topical corticosteroids, topical calcineurin inhibitors, NAMCS, NHAMCS
Abbreviations
AD—atopic dermatitis
NAMCS—National Ambulatory Medical Care Survey
NHAMCS—National Hospital Ambulatory Medical Care Survey
NCHS—National Center for Health Statistics
ICD-9-CM—International Classification of Diseases, Ninth Revision, Clinical Modification
ED— emergency department CI— confidence interval OR— odds ratio
FDA—Food and Drug Administration
Accepted for publication Mar 7, 2007
Address correspondence to Kimberly A. Horii, MD, Section of Dermatology, Children’s Mercy Hospitals and Clinics, 2401 Gillham Rd, Kansas City, MO 64108. E-mail: [email protected]
A
TOPIC DERMATITIS (AD)is the most common chronic inflammatory skin condition seen in the pediatric population. Studies have documented an increase in theprevalence of AD throughout the world.1–3 Although
similar increases have been found within the United States, these studies have been limited to small
geo-graphic areas.4 Morbidity and resource use, similar to
many other chronic illnesses, have been reported in both children and adults with AD.5–12In addition, families of children with moderate to severe AD have been found to have a higher impact on their quality of life than families
of children with insulin-dependent diabetes.5Compared
with looking after a child with chronic asthma, caring for a child with moderate to severe AD has been associated with greater parental sleep disturbances, anxiety levels, and increased maternal depression.11Costs to third-party payers to care for patients who were younger than 65 years and had AD in the United States were estimated to be between 0.9 billion to 3.8 billion dollars per year in 1997–1998.12
Patients with AD characteristically present with xero-sis, pruritus, and relapsing eczematous skin lesions dis-tributed in age-specific patterns.13–15Frequently, there is a family history of atopy, and the diagnosis of AD often precedes the development of either asthma or allergic rhinitis.16 There is currently no cure for AD; therapy is mainly directed at alleviating the symptoms of the dis-ease.15,17,18 Topical corticosteroids have been the main-stay of treatment for AD for many years. Only recently has a new class of medications, the topical calcineurin inhibitors, been introduced. Topical calcineurin inhibi-tors have expanded the viable options for treatment of AD. Although estimates have been made regarding the initial use of these newer medications, factors related to their use and changes in treatment use for AD have not
yet been measured.19 The aims of this study were to
describe the trends in visits for AD in children (0 –18 years) in the United States between 1997 and 2004, examine factors that were associated with the diagnosis of AD, and assess changes in the treatment of AD over time.
METHODS
A retrospective, cross-sectional study of outpatient en-counters compiled from the National Ambulatory Med-ical Care Survey (NAMCS) and the National Hospital Ambulatory Medical Care Survey (NHAMCS) databases from 1997 through 2004 was performed. The NAMCS and the NHAMCS are administered by the Ambulatory Care Statistics Branch of the Centers for Disease Control and Prevention National Center for Health Statistics
(NCHS).20–22The NAMCS collects information on patient
visits to non–federally funded, community, office-based physician practices throughout the United States. The NHAMCS collects information on patient visits to hospi-tal outpatient departments (general medicine, surgery,
pediatrics, obstetrics and gynecology, and a combined category of other clinics) and to hospital emergency departments (EDs). The data from both databases repre-sent a proportion of visits, not a proportion of patients, because these surveys do not track individual patients.
The surveys have multistage probability designs. The NAMCS has a 3-stage sampling design, with sampling based on geographic location, physician practices within a geographic location (stratified by physician specialty), and visits within individual physician practices. The NHAMCS has a 4-stage sampling design, with sampling based on geographic area, hospitals within a geographic area, clinics or EDs within hospitals, and patient visits within clinics or EDs. Visit weights accounting for selec-tion probability, adjustment for no response, and other adjustments to reflect the universe of ambulatory visits in the United States allow extrapolation to national es-timates for all aspects of the surveys.23,24
Demographics such as age, gender, race, and insur-ance status are included. Physician and hospital infor-mation includes self-identified specialty (in the NAMCS only), clinic type (in the NHAMCS only) such as hospital outpatient department or ED, geographic region, and whether the practice is in a rural area. Clinical
charac-teristics include up to 3 diagnoses (coded using the
In-ternational Classification of Diseases, Ninth Revision, Clinical
Modification [ICD-9-CM]), up to 8 medications, and the
correspondingNational Drug Code Directoryclass number
for each medicine.25
Study Population
All visits by children who were aged newborn to 18 years and had a diagnosis of AD (ICD-9-CM code of 691.8) in any of the primary or secondary diagnoses fields in the NAMCS and hospital outpatient depart-ments (excluding hospital EDs) of the NHAMCS were included. A total of 510 sample records for AD met inclusion criteria. An additional category was created for analysis of medication use for patients who were younger than 2 years at the time of their visit. There were 238 sample records in this category.
Data Analysis
Topical corticosteroids were identified using theNational
Drug Code Directoryclass prefix 1268, oral corticosteroids
by the prefix 1032, antihistamines by the prefix 1944, and topical calcineurin inhibitors by the drug mention code 01087 for topical tacrolimus (Protopic; Astellas Pharma US, Inc, Deerfield, IL) and code 02031 for top-ical pimecrolimus (Elidel; Novartis Pharmaceuttop-icals Corp, East Hanover, NJ). Only prescription medications were included in the data analysis. No over-the-counter medications, such as topical 1% hydrocortisone or mois-turizers/emollients, were included. It was possible for
and in 52 (22%) of those cases, ⱖ2 of the drugs were prescribed. Cases with multiple prescriptions were in-cluded in all individual drug analyses.
Race/ethnicity variables in the NHAMCS and NAMCS were combined into single variables with the following values: white not of Hispanic origin, Hispanic, black not of Hispanic origin, Asian not of Hispanic origin, and other/unknown. When the value of Hispanic was blank, the variables were treated as though they were not of Hispanic origin. The pay type variable was combined into 4 categories: commercial insurance (private insur-ance and workers’ compensation), government (Medi-care, Medicaid), self-pay, and other/unknown (blank,
no charge, other and unknown). Age categories were⬍1
year, 1 year, 2 to 5 years, 6 to 10 years, and 11 to 18 years. Any patient who was older than 18 years was excluded from the analysis. We defined specialist as allergy, allergy and immunology, dermatology, and pe-diatric allergy. All other physicians were considered gen-eralists.
Statistical Analysis
SEs were calculated using Stata software (Stata Corp, College Station, TX) as recommended by the NCHS, which accounts for the complex sampling design of the
NAMCS/NHAMCS.23,24,26 All statistical tests were based
on estimates that had a ⬍30% relative SE (ie, the SE
divided by the estimate expressed as a percentage of the
estimate) and were based on ⱖ30 cases in the sample
data. According to the NCHS, estimates with a ⬎30%
relative SE or based on⬍30 sample cases may be
unre-liable.
Ninety-five percent confidence intervals (CIs) for all counts and proportions were estimated. We used the svy:logistic procedure in Stata to compare various demo-graphic categories and to evaluate interactions among these variables. Trends over time were tracked using year of visit as a continuous predictor variable. For events in which the sample size was small (ie, medica-tion use in children younger than 2 years), the time variable was dichotomized into two 4-year intervals (1997–2000 and 2001–2004).
All analyses were performed with Stata 9 for Win-dows. All tests were conducted using a 2-sided␣level of .01.
RESULTS
Demographic Characteristics of All Pediatric Visits
There were an estimated 1.5 billion (95% CI: 1.4 –1.7) visits by patients who were agedⱕ18 years in the United States during the time interval 1997 to 2004. Of those visits, 51% were by boys and 69% were by white pa-tients (Table 1). For these visits, 65% were by children with commercial insurance coverage. Only 14% of the visits were in a nonurban setting. Most children were
seen in a physician’s office (88%) rather than in a hos-pital outpatient clinic (12%), and 69% of the visits were to a generalist. Of the pediatric outpatient visits, 16% were by children who were younger than 1 year, 10% by children who were 1 year of age, 22% by children who were aged 2 to 5 years, 20% by children who were aged 6 to 10 years, and 33% by children who were aged 11 to 18 years.
Factors Associated With AD Visits and Visit Rates
There were an estimated 7.4 million (95% CI: 5.9 – 8.8) visits in the United States by children who were aged newborn to 18 years and had AD to offices of pediatri-cians, other primary care physipediatri-cians, specialists, and hos-pital outpatient clinics between 1997 and 2004. Of the pediatric AD visits, the demographic characteristics were similar to all pediatric visits with the exception of race (only 51% white), specialty (only 43% generalists), and
age (only 21% 11–18 years, but⬎31% between 2 and 5
TABLE 1 Demographics of the Patient Population Variable AD Visits (Millions),
n(%)
All Pediatric Visits (Millions),
n(%)
Gender
Female 3.6 (49)a 760 (49)b
Male 3.8 (51) 800 (51)
Age, y
0 1.1 (15) 250 (16)
1 0.9 (12) 150 (10)
2–5 2.3 (31) 340 (22)
6–10 1.5 (21) 310 (20)
11–18 1.5 (21) 510 (33)
Race
Hispanic 1.5 (20) 220 (14)
Black 1.4 (19) 180 (12)
Asian 0.6 (11) 60 (4)
White 3.8 (51) 1070 (69)
Other 0.1 (1) 20 (1)
Insurance
Government 1.8 (25) 370 (24)
Self-pay 0.6 (8) 70 (5)
Other 0.5 (6) 100 (7)
Commercial 4.5 (61) 1010 (65)
Region
Midwest 1.5 (21) 360 (23)
South 2.7 (36) 510 (33)
West 1.5 (20) 340 (22)
Northeast 1.7 (23) 350 (23)
Setting
Urban 6.8 (92) 1330 (86)
Nonurban 0.6 (8) 220 (14)
Practice
Physician office 6.4 (87) 1370 (88)
HOP 1.0 (13) 180 (12)
Provider
Specialist 3.3 (44) 70 (4)
HOP 1.0 (13) 180 (12)
Generalist 3.1 (43) 1300 (69)
HOP indicates hospital outpatient.
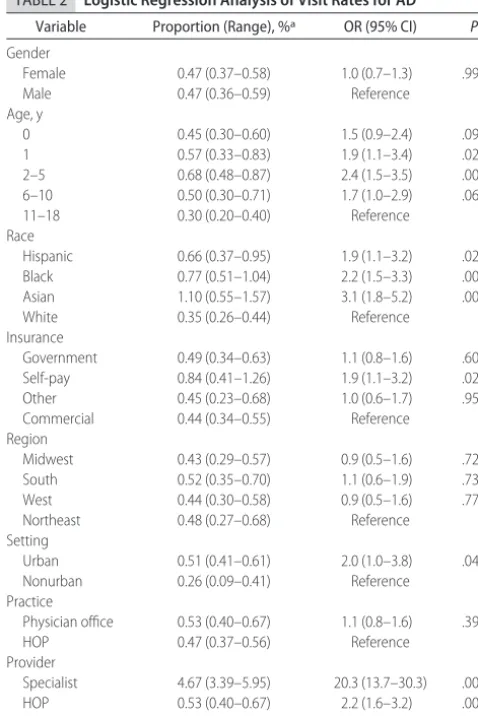
years; Table 1). These trends were tested with a logistic regression model. All of the disparities mentioned were statistically significant at an␣level of .01 (Table 2).
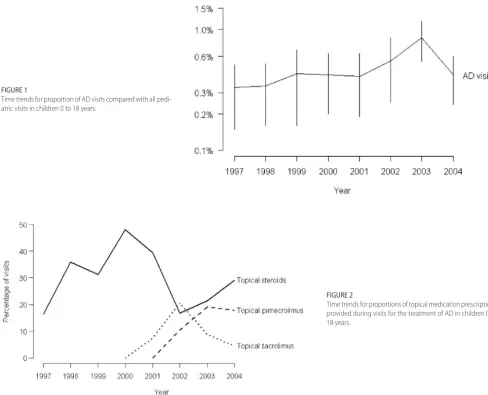
Annual AD visits started in 1997 at 620 000 and increased to a peak of 1.7 million visits in 2003. In 2004, however, the number of visits declined to 850 000. Dur-ing this period, the total number of pediatric visits was very stable. The increase in AD visits per year was sta-tistically significant (odds ratio [OR]: 1.10; 95% CI: 1.02–1.18) as shown in Fig 1.
We examined interactions between time periods (1997–2000 vs 2001–2004) and all of the specified de-mographic groups to determine whether the increasing rate of AD was preferentially associated with these groups. No interactions were significant at a .01 level, indicating that the increase was more or less uniform across these groups.
Medication Prescribing
During 1997 to 2000, there were 2.8 million AD visits, and 0.9 million (34%) involved the prescription of
top-ical corticosteroids. From 2001 to 2004, there were 4.6 million AD visits, and 1.1 million (25%) involved the prescription of topical corticosteroids. This decline was not statistically significant (OR: 0.6; 95% CI: 0.3–1.2). A total of 400 000 (14%) of the AD visits in 1997 to 2000 and 1.0 million (21%) in 2001 to 2004 involved the prescription of antihistamines. This increase was also not statistically significant (OR: 1.6; 95% CI: 0.5– 4.8).
Topical tacrolimus (Protopic) was prescribed in 0.5 million (10%) and topical pimecrolimus (Elidel) was prescribed in 0.6 million (13%) of the 4.6 million AD visits in 2001 to 2004. Figure 2 shows the trends in proportions of prescriptions for these drugs over time.
Among children who were younger than 2 years, there were 0.7 million AD visits in 1997 to 2000 and 1.3 million in 2001 to 2004. Of these visits, 150 000 (21%) and 310 000 (24%), respectively, involved the prescrip-tion of topical corticosteroids. This trend was not statis-tically significant (OR: 1.2; 95% CI: 0.4 –3.9). For chil-dren who were younger than 2 years in 1997–2000, antihistamines were prescribed in 50 000 (7%) visits for AD and in 220 000 (18%) of the visits in 2001–2004. For children who were younger than 2 years in 2001–2004, topical tacrolimus was prescribed in 97 000 (8%) visits for AD, whereas topical pimecrolimus was prescribed in 180 000 (14%) visits.
Between 1997 and 2004, oral corticosteroids were prescribed in 1.1 million (17%) of the 6.7 million AD visits (asthma cases were excluded from this analysis). There was no significant time trend in the prescription of oral corticosteroids in this group (OR: 1.3; 95% CI: 0.6 – 3.1). There were 130 000 (6%) prescriptions for oral corticosteroids among the 2.0 million AD visits in chil-dren who were younger than 2 years and did not have asthma between 1997 and 2004.
DISCUSSION
The estimated number of pediatric visits for AD has been increasing annually in the United States. The increase in AD visits per year in our cohort was statistically signifi-cant. This finding is consistent with the increasing prev-alence of AD seen throughout the world, although it must be noted that our data represent a proportion of visits, not a proportion of children.1–3 Therefore, visit trends can serve only as a surrogate measure of the prevalence of AD in children over time throughout the United States.
Reasons for this national increase in the number of visits for AD are unknown. Experts have developed nu-merous hypotheses to account for the reported world-wide increased prevalence of atopic diseases; however, consensus agreement on 1 specific cause remains elu-sive.16,27,28 Possible explanations for this increase over time include the “hygiene hypothesis,” exposure to en-vironmental risk factors, lifestyle changes, and western-ization.29–32 Another possibility is that physicians may
TABLE 2 Logistic Regression Analysis of Visit Rates for AD Variable Proportion (Range), %a OR (95% CI) P
Gender
Female 0.47 (0.37–0.58) 1.0 (0.7–1.3) .99
Male 0.47 (0.36–0.59) Reference
Age, y
0 0.45 (0.30–0.60) 1.5 (0.9–2.4) .09
1 0.57 (0.33–0.83) 1.9 (1.1–3.4) .02
2–5 0.68 (0.48–0.87) 2.4 (1.5–3.5) .001
6–10 0.50 (0.30–0.71) 1.7 (1.0–2.9) .06
11–18 0.30 (0.20–0.40) Reference
Race
Hispanic 0.66 (0.37–0.95) 1.9 (1.1–3.2) .02
Black 0.77 (0.51–1.04) 2.2 (1.5–3.3) .001
Asian 1.10 (0.55–1.57) 3.1 (1.8–5.2) .001
White 0.35 (0.26–0.44) Reference
Insurance
Government 0.49 (0.34–0.63) 1.1 (0.8–1.6) .60
Self-pay 0.84 (0.41–1.26) 1.9 (1.1–3.2) .02
Other 0.45 (0.23–0.68) 1.0 (0.6–1.7) .95
Commercial 0.44 (0.34–0.55) Reference
Region
Midwest 0.43 (0.29–0.57) 0.9 (0.5–1.6) .72
South 0.52 (0.35–0.70) 1.1 (0.6–1.9) .73
West 0.44 (0.30–0.58) 0.9 (0.5–1.6) .77
Northeast 0.48 (0.27–0.68) Reference
Setting
Urban 0.51 (0.41–0.61) 2.0 (1.0–3.8) .04
Nonurban 0.26 (0.09–0.41) Reference
Practice
Physician office 0.53 (0.40–0.67) 1.1 (0.8–1.6) .39
HOP 0.47 (0.37–0.56) Reference
Provider
Specialist 4.67 (3.39–5.95) 20.3 (13.7–30.3) .001
HOP 0.53 (0.40–0.67) 2.2 (1.6–3.2) .001
Generalist 0.29 (0.21–0.37) Reference
HOP indicates hospital outpatient.
simply be better at diagnosing children with AD than in the past and therefore may be diagnosing more mild cases.3
Although the total number of annual pediatric patient visits remained stable over time, the number of esti-mated annual AD visits peaked at 1.7 million visits in 2003. Although this peak in 2003 may be an anomaly, a potential explanation for this finding may be related to the introduction of the topical calcineurin inhibitors in 2000 and 2001, which were initially marketed to pri-mary care physicians, specialists, and the public.19,33With increased public knowledge of topical calcineurin inhib-itors, parents who had previously not seen a physician for their child’s AD may have potentially sought this
novel treatment.34Media influences on demand for
test-ing and treatment have also been noted to occur in other
medical specialties.35,36 Marketing of the topical
cal-cineurin inhibitors may have also increased primary care physician knowledge about AD, which could have led to an increase in their comfort with diagnosing and treating AD. Future evaluation of visit trends for AD during 2005
and after the January 2006 Food and Drug Administra-tion (FDA) approval of a topical calcineurin inhibitor boxed warning will be important to follow.
The demographic characteristics of the pediatric pa-tients seen with AD were similar to all other pediatric visits that occurred between the same time interval ex-cept for age, race, and physician specialty. Patients who were 2 to 5 years of age were seen more often for a diagnosis of AD. Although AD often develops before 1 year of age, a delay in making the diagnosis of AD or potential parental hesitation to obtain treatment for AD during infancy may explain why children 2 to 5 years of age were more commonly seen for AD than any other pediatric age group.
Black and Asian children were also seen more fre-quently for the diagnosis of AD in our cohort. These results mirror those reported by Janumpally et al,37who found that black and Asian/Pacific Islander individuals were more likely than white individuals to seek medical care for the diagnosis of AD. A British study found that London-born black Caribbean children were at a
poten-FIGURE 1
Time trends for proportion of AD visits compared with all pedi-atric visits in children 0 to 18 years.
FIGURE 2
tially higher risk for developing AD when compared with their white counterparts, suggesting that certain racial groups may be at an increased risk for developing AD.38
Specialists and hospital outpatient clinic physicians were the providers who saw the majority of patients with a diagnosis of AD. These results suggest that chil-dren with AD may require or families may seek subspe-cialty care for the treatment of AD. Therefore, there may be an increased need in the future for more subspecial-ists who are trained to care for AD. Hospital outpatient clinics (staffed by generalists), most commonly located in urban settings, also reported more pediatric visits for AD. Urban patients with AD may not have access to subspe-cialists or private generalist practices and therefore may seek their care for AD from hospital outpatient clinic physicians.
Topical corticosteroids are accepted first-line anti-in-flammatory agents to treat flares of AD.15,17,18When se-lected and used appropriately, topical corticosteroids are usually not associated with significant adverse effects.14 Surprising, fewer than one third of all pediatric visits and fewer than 1 in 4 visits for AD of patients who were younger than 2 years were treated with topical cortico-steroids in our cohort.
It is unclear why topical corticosteroids were not pre-scribed in a majority of the pediatric visits for AD in our cohort. Unfortunately, steroid phobia of the physician or the parent may limit the prescribing and use of this first-line therapy for patients with AD.39 In a question-naire-based study performed in the United Kingdom in 2000, 72.5% of patients reported that they worried about using topical corticosteroids either on their own or on their child’s skin, and 24% were noncompliant with
their treatment regimen because of these concerns.40In
another study that surveyed patients and physicians about pediatric AD, 94% of the physicians had concerns, such as the long-term consequences of topical cortico-steroids, and admitted to taking precautions when
treat-ing children for AD.41Misunderstandings about the use
and adverse effects of topical corticosteroids by all types of medical professionals and conflicting messages to pa-tients/parents about topical corticosteroid safety may also contribute significantly to the undertreatment of pediatric AD.42This limited use of evidence-based ther-apy is not dissimilar to other studies that have shown low usage rates of other effective therapies in children.43 Although it seemed that the introduction of topical calcineurin inhibitors was chronologically coincident with both an increase in the number of visits for AD and a decrease in the number of topical corticosteroid pre-scriptions, there was an insufficient number of records in the database to allow a statistical analysis of this trend.
Oral corticosteroids were prescribed in 1 in 6 visits for AD in this study, although oral corticosteroids are not a recommended first-line therapy for AD because of their
possible adverse effects and the potential for rebound flare of symptoms.14,17,18 Topical calcineurin inhibitors are also not indicated as first-line therapies for the treat-ment of AD but are recommended for patients who are unresponsive to or intolerant of other first-line thera-pies.44,45Topical calcineurin inhibitors are approved for the short-term or intermittent treatment of mild to mod-erate AD (topical pimecrolimus) or modmod-erate to severe AD (topical tacrolimus) in patients who are older than 2 years.33 In this study, we found similar rates of use of topical corticosteroids and topical calcineurin inhibitors in patients who were younger than 2 years (24% vs 22%). It is unknown whether these children who re-ceived off-label-use topical calcineurin inhibitors had previously had topical corticosteroid therapy that failed. The FDA public health advisory, which initially raised the concern of a potential risk for malignancy associated with the use of topical calcineurin inhibitors, and the subsequent FDA-approved boxed warning occurred
after our study period.46–48 Evaluation of prescribing
pattern trends of topical corticosteroids and topical calcineurin inhibitors over the next 5 years will be im-portant to follow, specifically evaluating for any changes that may have occurred after the announcement of the public health advisory and boxed warning.
This is a secondary data analysis; as such, there are limitations associated with its use. We acknowledge that we cannot confirm the accuracy of the diagnosis of AD reported by the participating providers to the national databases. We restricted our study to include the ICD-9-CM code for AD to obtain our data; however, provid-ers were not instructed to follow any defined diagnostic criteria before making a diagnosis of AD. This may have affected our results. We may have overestimated the number of visits and prescribing patterns for AD if the data included other skin conditions that were incorrectly diagnosed and treated as AD.
Because this study looks at proportion of visits, not proportion of patients, we cannot determine whether the results are potentially inflated by individual patients who had severe AD and had multiple visits. Further-more, because the NHAMCS provides data on patient visits only to outpatient hospital departments and hos-pital EDs, hoshos-pital-based subspecialty clinic data are not separately available for analysis in our cohort.
Further-more, because emollients and over-the-counter topical steroids are not prescribed “medications,” we were not able to evaluate whether either were recommended therapeutic options during visits for AD in our cohort. Nevertheless, the NAMCS and NHAMCS are well suited to study practice variations from a public health or policy perspective. The availability of large numbers of patients, detailed clinical information, and sophisticated sampling techniques provides nationally representative data that are unavailable elsewhere.
CONCLUSIONS
We found that the estimated number of visits for the diagnosis of AD in children in the United States has increased over time. Reasons to account for this national increase in the number of visits for AD have yet to be fully elucidated. We also found that black and Asian children were more likely than white children to be seen for the diagnosis of AD and that specialists and hospital outpatient clinic physicians were seeing the majority of pediatric patients with AD in our cohort. We also deter-mined that recommended first-line treatment options for AD in children seem to have been prescribed in a minority of pediatric patient visits for AD. Continued evaluation of visit trends and prescribing patterns for AD in children over the next several years will be important to follow.
REFERENCES
1. Larsen FS, Diepgen T, Svensson A. The occurrence of atopic dermatitis in north Europe: an international questionnaire study.J Am Acad Dermatol.1996;34:760 –764
2. Larsen FS, Holm NV, Henningsen K. Atopic dermatitis a genet-ic-epidemiologic study in a population-based twin sample. J Am Acad Dermatol.1986;15:487– 494
3. Williams HC. Is the prevalence of AD increasing? Clin Exp Dermatol.1992;17:385–391
4. Laughter D, Istvan JA, Tofte SJ, Hanifin JM. The prevalence of atopic dermatitis in Oregon school children.J Am Acad Derma-tol.2000;43:649 – 655
5. Su JC, Kemp AS, Varigos GA, Nolan TM. Atopic eczema: its impact on the family and financial cost.Arch Dis Child.1997; 76:159 –162
6. Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health related quality of life.Int J Dermatol.2002;41:151–158
7. Dahl RE, Bernhisel-Broadbent J, Scanlon-Holdford S, Sampson HA, Lupo M. Sleep disturbances in children with atopic der-matitis.Arch Pediatr Adolesc Med.1995;149:856 – 860
8. Chamlin SL, Frieden IJ, Williams ML, Chren MM. Effects of atopic dermatitis on young American children and their fami-lies.Pediatrics.2004;114:607– 611
9. Chamlin SL, Mattson CL, Frieden IJ, et al. The price of pruritus: sleep disturbances and cosleeping in atopic dermatitis. Arch Pediatr Adolesc Med.2005;159:745–750
10. Emerson RM, Williams HC, Allen BR. What is the cost of atopic dermatitis in preschool children? Br J Dermatol. 2001;143: 514 –522
11. Moore K, David TJ, Murray CS, Child F, Arkwright PD. Effect of childhood eczema and asthma on parental sleep and
well-being: a prospective comparative study. Br J Dermatol.2006; 154:514 –518
12. Ellis CN, Drake LA, Prendergast MM, et al. Cost of atopic dermatitis and eczema in the United States.J Am Acad Dermatol. 2002;46:361–370
13. Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol.1980;92:44 – 47
14. Eichenfield LF, Hanifin JM, Luger TA, Stevens SR, Pride HB. Consensus conference on pediatric atopic dermatitis.J Am Acad Dermatol.2003;49:1088 –1095
15. Darsow U, Lubbe J, Taieb A, et al. Position paper on diagnosis and treatment of atopic dermatitis.J Eur Acad Dermatol Venereol. 2005;19:286 –295
16. Eichenfield LF, Hanifin JM, Beck LA, et al. Atopic dermatitis and asthma: parallels in the evolution of treatment.Pediatrics. 2003;111:608 – 616
17. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines of care for atopic dermatitis.J Am Acad Dermatol.2004;50:391– 404 18. Hoare C, Li WP, Williams H. Systemic review of treatments for
atopic dermatitis.Health Technol Assess.2000;4:1–191. Available at: www.ncchta.org/execsumm/summ437.htm accessed Sep-tember 25, 2006
19. Department of Health and Human Services, Public Health Ser-vice, Food and Drug Administration, Center for Drug Evalua-tion and Research. Available at: www.fda.gov/ohrms/dockets/ ac/05 / briefing/2005-4089b2_01_05_Cleared%20version%20 Elidel-Protopic%20Drug%20Use%20Review%20D040389% 207–2004.pdf. Accessed January 19, 2007
20. Woodwell DA, Cherry DK. National Ambulatory Medical Care Survey: 2002 Summary—Advance Data From Vital and Health Statistics: No. 346. Hyattsville, MD: National Center for Health Statistics; 2004
21. Hing E, Middleton K.National Hospital Ambulatory Medical Care Survey: 2002 Outpatient Department Summary—Advance Data From Vital and Health Statistics: No. 338. Hyattsville, MD: Na-tional Center for Health Statistics; 2004
22. McCaig LF, Burt CW.National Hospital Ambulatory Medical Care Survey: 2002 Emergency Department Summary—Advance Data From Vital and Health Statistics: No. 335. Hyattsville, MD: Na-tional Center for Health Statistics; 2004
23. National Center for Health Statistics.Public Use Microdata File Documentation, National Hospital Ambulatory Medical Care Survey, 2003. Hyattsville, MD: National Technical Information Service; 2005
24. National Center for Health Statistics.Public Use Microdata File Documentation, National Ambulatory Medical Care Survey, 2003. Hyattsville, MD: National Technical Information Service; 2005 25. US Food and Drug Administration.National Drug Code Directory,
1995 Edition. Washington, DC: Public Health Service; 1995 26. Hing E, Gousen S, Shimizu I, Burt C. Guide to using masked
design variables to estimate standard errors in public use files for the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Care Survey. Inquiry. 2003/ 2004;40:416 – 415
27. Simpson EL, Hanifin JM. Atopic dermatitis. Med Clin N Am. 2006;90:149 –167
28. Levy RM, Gelfand JM, Yan AC. The epidemiology of atopic dermatitis.Clin Dermatol.2003;21:109 –115
29. Elston DM. The hygiene hypothesis and atopy: bring back the parasites?J Am Acad Dermatol.2006;54:172–179
30. Strachan DP. Hay fever, hygiene, and household size. BMJ. 1989;299:1259 –1260
31. Flohr C, Pascoe D, Williams HC. Atopic dermatitis and the hygiene hypothesis: too clean to be true?Br J Dermatol.2005; 152:202–216
internation study of asthma and allergies in children.J Allergy Clin Immunol.1999;103:125–138
33. Food and Drug Administration Pediatric Advisory Committee. Briefing Information. Available at: www.fda.gov/ohrms/dockets/ ac/05/briefing/2005-4089b2.htm. Accessed January 19, 2007 34. Qureshi AA, Fischer MA. Topical calcineurin inhibitors for
atopic dermatitis balancing clinical benefit and possible risks. Arch Dermatol.2006;142:633– 637
35. Sharma V, Dowd D, Swanson DS, Slaughter AJ, Simon SD. Influence of the new media on diagnostic testing in the emer-gency department.Arch Pediatr Adolesc Med.2003;157:257–260 36. Braun M, Klotz T, Mathers MJ, et al. “Viagra effect”: influence of the mass media on patient behavior. Urol Int. 2001;66: 145–148
37. Janumpally SR, Feldman SR, Gupta AK, Fleischer AB. In the United States, blacks and Asian/Pacific Islanders are more likely than whites to seek medical care for atopic dermatitis. Arch Dermatol.2002;138:634 – 637
38. Williams HC, Pembroke AC, Forsdyke H, Boodoo G, Hay RJ, Burney PG. London-born black Caribbean children are at in-creased risk of atopic dermatitis.J Am Acad Dermatol.1995;32: 212–217
39. Del Rosso J, Friedlander SF. Corticosteroids: options in the era of steroid-sparing therapy. J Am Acad Dermatol. 2005;53: S50 –58
40. Charman CR, Morris AD, Williams HC. Topical corticosteroid phobia in patients with atopic eczema.Br J Dermatol.2000;142: 931–936
41. Paller AS, McAlister RO, Doyle JJ, Jackson A. Perceptions of
physicians and pediatric patients about atopic dermatitis, its impact, and its treatment.Clin Pediatr (Phila).2002;41:323–332 42. Beattie PE, Lewis-Jones MS. Parental knowledge of topical therapies in the treatment of childhood atopic dermatitis.Clin Exp Dermatol.2003;28:549 –553
43. Marshall BC, Henshaw C, Evans DA, Bleyl K, Alder S, Liou TG. Influenza vaccination coverage level at a cystic fibrosis center. Pediatrics. 2002;109(5). Available at: www.pediatrics.org/cgi/ content/full/109/5/e80
44. Fonacier L, Spergel J, Charlesworth EN, et al. Report of the topical calcineurin inhibitor task force of the American college of allergy, asthma, and immunology and the American acad-emy of allergy, asthma, and immunology.J Allergy Clin Immu-nol.2005;115:1249 –1253
45. Berger TG, Duvic M, Van Voorhees AB, Frieden IJ. The use of topical calcineurin inhibitors in dermatology: safety concerns. J Am Acad Dermatol.2006;54:818 – 823
46. US Food and Drug Administrion, Center for Drug Evaluation and Research. Alert for Healthcare Professionals: Tacrolimus (Marketed as Protopic). Available at: www.fda.gov/cder/drug/ InfoSheets/HCP/ProtopicHCP.htm. Accessed January 19, 2007 47. US Food and Drug Administrion, Center for Drug Evaluation and Research. Alert for Healthcare Professionals: Pimecrolimus (Marketed as Elidel). Available at: www.fda.gov/cder/drug/ InfoSheets/HCP/elidelHCP.htm. Accessed January 19, 2007 48. US Food and Drug Administrion. FDA News: FDA Approves
DOI: 10.1542/peds.2007-0289
2007;120;e527
Pediatrics
Kimberly A. Horii, Stephen D. Simon, Deede Y. Liu and Vidya Sharma
Patient and Provider Characteristics, and Prescribing Patterns
2004: Visit Trends,
−
Atopic Dermatitis in Children in the United States, 1997
Services
Updated Information &
http://pediatrics.aappublications.org/content/120/3/e527
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/120/3/e527#BIBL
This article cites 36 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/dermatology_sub
Dermatology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-0289
2007;120;e527
Pediatrics
Kimberly A. Horii, Stephen D. Simon, Deede Y. Liu and Vidya Sharma
Patient and Provider Characteristics, and Prescribing Patterns
2004: Visit Trends,
−
Atopic Dermatitis in Children in the United States, 1997
http://pediatrics.aappublications.org/content/120/3/e527
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.