Abstract
The GlaxoSmithKline RTS,S vaccine has been undergoing Phase III trials to evaluate efficacy for protection from malaria, a disease infecting between 300-600 million people every year. As RTS,S is a transmission blocking vaccine, transmission intensity may be important in vaccine efficacy. Therefore, all trial sites conducted a concordant Malaria Transmission Intensity (MTI) study, from 2011-2013, to look at the prevalence of malaria by microscopy within the trial site. Malaria parasitemia prevalence is often used as a surrogate of transmission intensity. Unfortunately, it is known that microscopy can miss many, if not most, of malaria parasitemia in a population. Nucleic acid detection methods are more sensitive than microscopy, often
detecting parasitemia counts below the detection limit of microscopy (called “submicroscopic” parasitemia). We use a real-time Polymerase Chain Reaction (RT-PCR) assay for pfldh on dried blood spots from 800 patient blood samples collected during the 2013 MTI study in Lilongwe, Malawi to determine the difference in prevalence of parasitemia between testing methods. We found that the addition of RT-PCR nearly tripled the number of participants with malaria
Introduction
Malaria is a highly symptomatic, highly infectious, highly deadly disease-- it infects hundreds of millions of individuals every year and kills roughly 600,000 people [1]. It is caused by parasites of the Plasmodium sp. and is transmitted by means of a vector, the Anopheles mosquito. In this process, a mosquito infected with the Plasmodium parasite can spread the parasite to humans through a bite, and, subsequently, an uninfected mosquito can pick up the parasite through the blood of an infected human [2]. Thus, transmission intensity, often imputed from the overall prevalence of the parasite within a human population, can significantly impact the rate of human infections [3]. However, malaria infections are completely preventable and treatable through the avoidance of the Anopheles mosquito and through a combination of early detection and sufficient treatment [4]. Unfortunately, the endemic populations affected by the Plasmodium parasite are often those of lower resource countries, more specifically in
Sub-Saharan Africa. These countries often lack the means for efficient detection and treatment. Countries with intensive endemic malaria have economies 33% in size when compared to those without [5]. Thus, malaria is a disease of poverty and remains the most clinically important vector-borne parasitic infection around the world. Unfortunately, currently used control
measures, such as antimalarial drugs, insecticide treated bed nets, and indoor residual spraying, are unlikely to completely control malaria. Thus, the search for a vaccine for malaria has become of great importance to the medical community [6].
Over the past several decades, GlaxoSmithKline has worked to develop a vaccine for the Plasmodium falciparum parasite [7]. Plasmodium falciparum is one of five species of the
Plasmodium genus that can cause symptoms in humans and is the most prevalent and deadly of
in Sub-Saharan Africa, 90% of those killed by Plasmodium falciparum are children under the age of 5 [8]. Thus, targeting this species of malaria for vaccine development could have the greatest impact on limiting infection and potentially malaria mortality. The vaccine, known as RTS,S, targets the Plasmodium falciparum parasite between its first and second stage of its life cycle, the period during which the sporozoite migrates and infects the liver [7]. Falciparum malaria parasites then mature in the liver for 7-14 days before emerging and proceeding to the erythrocyte life cycle stage, the stage at which clinical malaria occurs [7]. Therefore, targeting this portion of the parasite life cycle has great potential to prevent any infection into the liver and, therefore, progression through the life cycle to the stages associated with clinical disease [7].
The vaccine appears to work by inducing antibodies in the human to circumsporozoite protein (CS), the dominant protein expressed on the surface of the sporozoite and which is minimally expressed on the surface of infected liver hepatocytes [7]. Phase II clinical trials were promising, indicating that the vaccine could reduce malaria infections by upwards of 50% in children and 25% in young infants [7]. Subsequently, GlaxoSmithKline began Phase III human trials at 11 different sites in 7 countries across Sub-Saharan Africa, one of which was the
University of North Carolina research center in Lilongwe, Malawi. Despite promising Phase II results, Phase III trials indicated that the vaccine was not as effective in humans as expected, generating a 46% efficacy in study populations [9, 21], and research has now begun to identify the causes of vaccine ineffectiveness in order to better prepare for future vaccine designs.
(MTI) study was conducted at all trial sites for three years in order to monitor localized
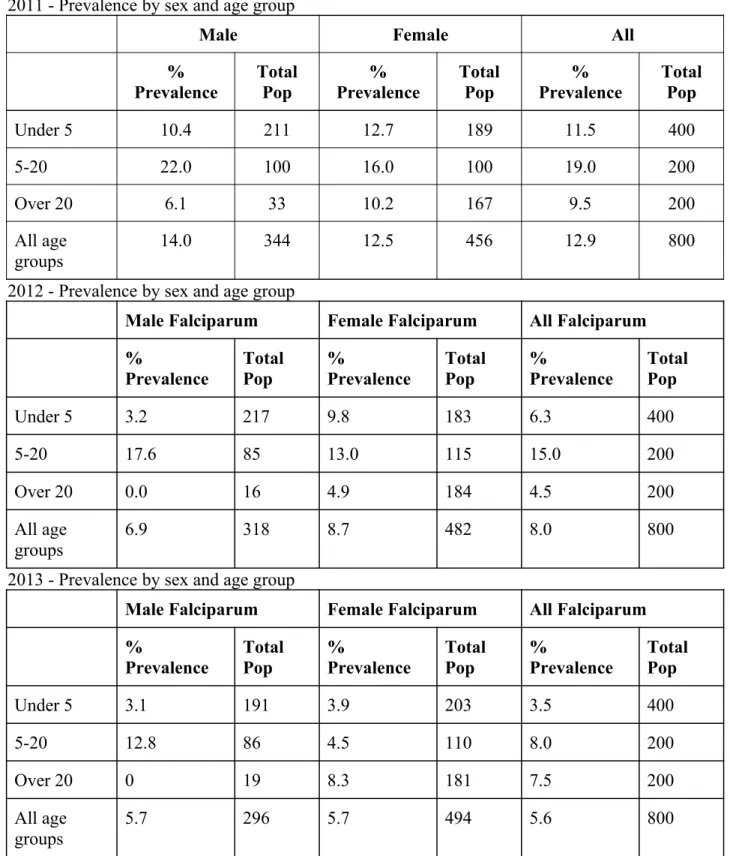
transmission intensities at each study site over the course of the vaccine trial. At the UNC site, this involved identifying a cohort of 800 individuals each year and conducting a cross-sectional survey of malaria parasitemia prevalence, a commonly used surrogate of transmission intensity. Malaria diagnoses for these patients were made using the current “gold standards” for malaria testing in the developing world-- rapid diagnostic testing (RDT) and microscopy [10-13]. These tests have been used throughout low resource countries because of their ease of use and cost accessibility; however, it has been shown that these tests are insensitive and often can miss diagnoses for individuals with low parasite count [10-13]. Additionally, it has been shown that a significant portion of the Plasmodium population exists in a submicroscopic state, at risk of feigning detection through the gold standards of testing [14]. Therefore, the sole use of these tests can cause an underestimation of transmission intensity of Plasmodium falciparum within endemic countries, which could have serious implications in understanding vaccine efficacy.
rates using real time PCR (RT-PCR) than using microscopy, supporting the clinically important presence of submicroscopic parasitemia within endemic populations [10-13]. We hypothesized that the MTI study methods would fail to detect all present parasitemia within the population, and thus produce an under representation of the parasite prevalence and thus underestimate transmission intensity. In this study, we tested dried blood spot samples collected concurrently with microscopy slides by RT-PCR to detect any potential submicroscopic parasitemia within the Lilongwe population in order to determine if the underestimation of transmission intensity would be significant in regards to the vaccine trials.
Research also has been conducted to identify risk factors associated with contracting microscopic and symptomatic malaria [16-18]; identifying and mitigating these risk factors for contracting the disease have become important tactics in preventative efforts to decrease malaria mortality around the world. Such risk factors that have been identified are age, education level, lack of knowledge of malaria, lack of bed nets, a household location in rural areas, household infrastructure, crowded households with individuals sharing rooms, and number of windows in the household [16-18]. However, significantly less research has been conducted on
submicroscopic malaria, and, more specifically, if these risk factors vary between microscopic and submicroscopic parasites. We therefore used this study to assess for factors that were associated with submicroscopic parasitemia from those collected during the study.
Materials and Methods
Patient samples and data: During the original RTS,S human trials, the MTI study enrolled a
filter paper. These spots were dried, labeled with study identifiers and packaged individually with desicant. Of the 800 patients each year, 400 were children under 5, 200 were between ages 5 and 20, and 200 were over the age of 20. Samples from all years were tested for malaria using the two “gold standards”—an HRP2 rapid diagnostic test (RDT) and microscopy. Microscopy slides were read by two independent readers, and discordant results were reviewed by a third reader.
DNA was extracted from 792 dried blood spot samples from a 2013 survey using Invitrogen PureLink Pro96 Genomic DNA extraction kits (Invitrogen, Carlsbad, CA) per the manufacturer protocol. Samples for 8 participants were not able to be found. The extracted DNA was then tested for the presence of malaria using a RT-PCR that targeted the Plasmodium
falciparum lactate dehydrogenase (LDH) gene (pfldh) using a previously described assay [24].
LDH is encoded by a single copy gene in the genome and is specific for P. falciparum. Thus, this assay can be used to estimate parasitemia level within the patient. Samples were considered positive if the fluorescent indicator exceeded a specific intensity cut-off as determined by the cycle threshold. All samples were run with corresponding negative and positive controls to ensure the accuracy of measurements.
Data Analysis: The presence of malaria within the study population was calculated as a
percentage and was compared between the assays to identify individuals housing malaria in submicroscopic parasitemia form. Individuals who tested negative using microscopy and positive using RT-PCR were considered to have submicroscopic parasitemia, as the parasites found within their blood could not be identified using microscopy.
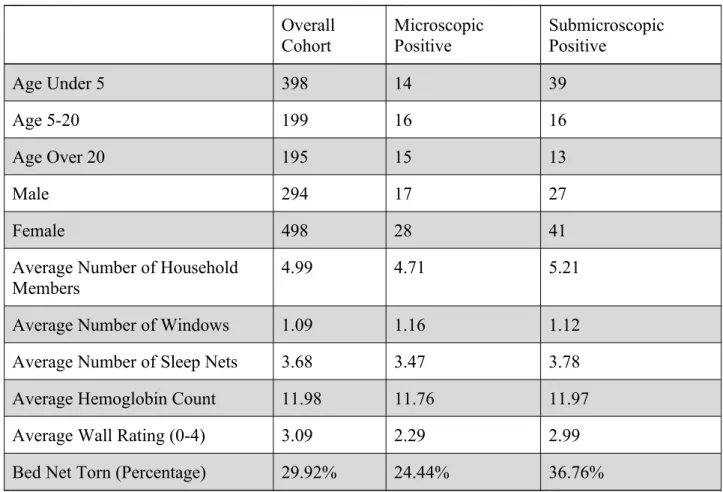
factors associated with the presence of malaria in submicroscopic parasite form. Information regarding patient demographics, which were collected during the initial human trials, were gathered and were compared using categorical counts within the group of submicroscopic positive patients and the group of microscopic positive patients. The variables studied were age, gender, number of household members, number of windows, number of sleep nets, hemoglobin count, household wall rating, and presence of torn bed nets [Table 1, Table 2, Figure 1]. A majority of these variables were determined through household patient interviews, and wall rating was projected onto a scale from 1-4, based on a predetermined scale: 1=no windows that close, no screens/walls not intact, 2=walls and closed windows intact, but no screens, 3=walls and windows with screens, but some holes in screens that could allow mosquito entrance, 4=walls and windows with screens that are completely intact. Additionally, statistical Chi Squared tests for significance were performed for each variable, comparing the differences in counts between microscopic positive patients and submicroscopic positive patients to determine if the differences in counts were significant enough to identify a possible relationship. Any variable with a P value less than 0.05 was identified as statistically significant.
Results
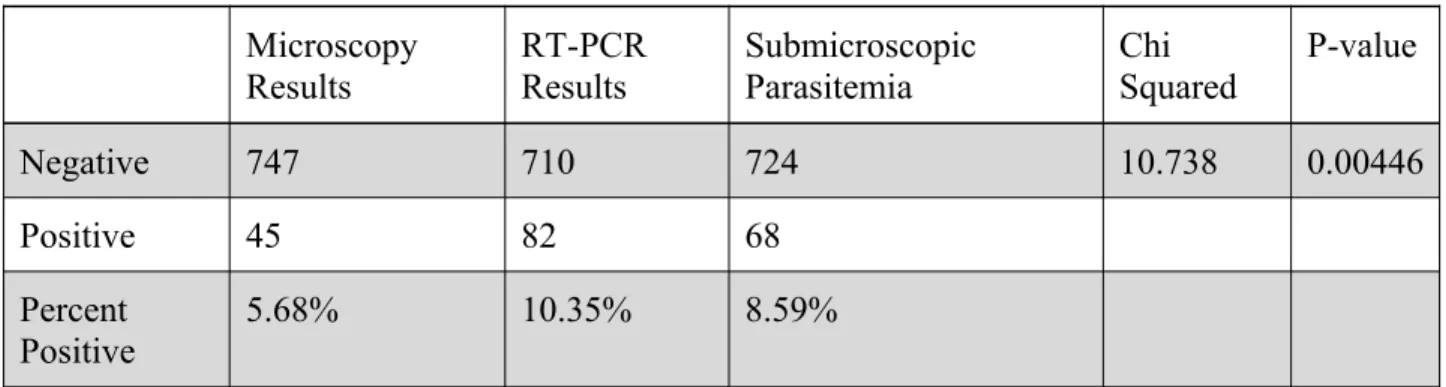
Of the 800 patients who were part of the RTS,S vaccine study, only 792 blood spots were available to be tested using RT-PCR, and, therefore, the 8 remaining patients and their related microscopy results were not used for analysis. This represents 1% of all samples and is unlikely to impart significant bias. Of the 792 patients analyzed, 45, or 5.68%, were found positive for Plasmodium falciparum using microscopy for diagnosis; likewise, of the 792 patients analyzed,
[Table 3, Figure 2]. The Chi Squared value of 10.738 (p-value=0.0446) between testing methods indicates that the difference in positive count using these methods is significant. These results indicate the presence of a statistically and likely clinically significant level of
submicroscopic parasitemia within the blood of patients in the study cohort.
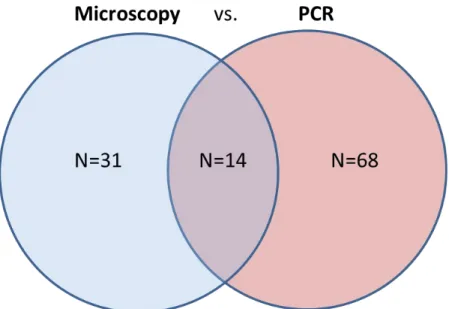
In total, 68 patients, or 8.59% of the study population, met the predefined criteria for submicroscopic infection [Table 3, Figure 3]. Interestingly, of the 45 microscopy positive patients, only 14 tested positive by RT-PCR. This indicates that 31 of the microscopy positive patients were not identified as positive using RT-PCR [10-13], and these results should be taken into account when drawing conclusions from the data. The 45 microscopy positive and the 68 submicroscopic positive patients thus indicate that the overall composite malaria prevalence within the Lilongwe population is 113 of the 792 individuals, or 14.3% [Figure 2, Figure 3]. These individuals then were grouped into individual cohorts for additional epidemiological analysis.
difference in its relationship between the variables. This also identified characteristics with trends that differed between the pool of microscopic individuals and submicroscopic individuals, and this statistical difference identified these characteristics as potential risk factors for
contracting submicroscopic malaria as opposed to microscopic malaria. Only one of the
potential risk factors studied had a Chi Squared value that indicated significance in trend [Table 1, Figure 1, Figures 4-5]. The age of the individuals was identified as showing trends that differed significantly between submicroscopic and microscopic patients (p-value=0.02271) [Table 2, Figure 4]. The age distribution for microscopic malaria was relatively consistent between ages under 5, 5-20, and over 20, with counts of 14, 16, and 15 respectively [Table 2, Figure 1]. However, the age distribution for submicroscopic malaria shifted significantly, with 39, or over 50% of positive patients, being under the age of 5, and with the other two age groups having 16 and 13 [Table 2, Figure 4]. This indicates that a majority of patients testing positive for submicroscopic parasitemia are under the age of 5, which differs from the expected results found in the microscopy positive patients. Therefore, young age can be identified as a potential risk factor for submicroscopic, asymptomatic malaria in this cohort.
Discussion
microscopy, identifying the presence of submicroscopic parasites within their blood [Table 3, Figure 2, and Figure 3]. Because 8.59% of the study population tested positive for
submicroscopic malaria, which indicated a significant difference in relationships [Figure 2 and Figure 3], it can be concluded that submicroscopic malaria is an extremely common condition in the population of Lilongwe, Malawi. However, as stated in the results, a significant number of microscopy positive patients also were identified as PCR negative [Table 3]. Because RT-PCR has been shown to be more sensitive and accurate than microscopy for malaria diagnostics [10-13], all microscopy positive patients should also be found to be RT-PCR positive. However, previous research has shown that RT-PCR assays can often miss diagnose microscopy positive blood samples as well [20]. Studies on diagnostic sensitivity between the two assays have shown that, although RT-PCR assays have a 96% sensitivity in high parasite density blood, their
sensitivity may drop to 20% in blood with parasite density less than 100/microliter [20].
Therefore, although these results should be noted, they are not unexpected, and they should not decrease the validity of the conclusion that the Plasmodium falciparum population in Lilongwe, Malawi has a significant presence of endemic submicroscopic parasitemia within its human reservoirs.
fail to detect parasitemia if there is variation in the parasite genome where the primers bind. Lastly, as the assay and protocol design only detect Plasmodium falciparum, it could be possible that individuals have been infected with a different species of the parasite that was detected in microscopy but that could not be detected in a falciparum specific RT-PCR assay. As
Plasmodium vivax and ovale are also known to be endemic to Malawi [22], these patients could
have been infected with one of these species instead, which would potentially cause microscopy positive results and RT-PCR negative results. However, in order to determine the source of the discrepancy, these discordant samples will need to be retested using an assay that can detect different malaria species. Another possibility to resolve these discordant results would be to use an even more sensitive RT-PCR. Pfldh is a single copy gene in the genome. Use of a multi-copy gene in detection assays can increase their sensitivity. One potential test that could be used is a detection assay that targets 18s ribosomal targets that have more than one gene copy per genome [23].
Several clinical and public health implications could be associated with the identification of submicroscopic parasitemia in Lilongwe. Currently, microscopy and rapid diagnostic testing are the gold standard methods for diagnosis of malaria in the developing world [10-13].
unexpected transmission between humans by allowing the persistence of asymptomatic infection in the population that acts as a reservoir for transmission by mosquitos. However, as microscopy will likely remain the standard of care in most locations due to the financial barriers of more sensitive and expensive tests, such as RT-PCR, in resource poor countries [5]. Thus, hospitals and control programs currently using microscopy for the diagnosis of malaria should take these limitations into account.
These findings also have implications associated with RTS,S vaccine trials. The results of the Phase III trial showed an efficacy lower than expected from initial Phase II trials. In part, this lower efficacy could be due to the underestimation of transmission intensity. None of the other trial sites evaluated intensity of transmission with nucleic acid detection. The vaccine is designed to block the establishment on infection prior to the liver stage. In low transmission intensity settings, where an individual may only be bit a few times a year by infected mosquitos, a modest efficacy of 95% would essentially stop infection in most people, and, therefore, reduce clinical cases. However, in areas of Africa, children can be bitten several hundred times a month by infected mosquitos. Thus, even if a vaccine were 99% effective at blocking infection of the liver, most children would still develop an infection every month.
submicroscopic Plasmodium falciparum infection. In addition, other demographic factors, those that correlated with the above mentioned microscopy malaria risk factors, were selected for study in order to better analyze statistical differences between the microscopic and submicroscopic groups. Possible factors selected for analysis were gender, number of household members, number of household windows, number of household bed nets, household wall rating, and the presence of torn bed nets in the household [Table 1]. As malaria is spread through interpersonal contact and through interaction with the Anopheles mosquito, each of these factors could have a strong impact on malaria transmission and could be compared between microscopic and
submicroscopic parasites in order to better understand the potential need for further researching submicroscopic parasitemia and their effect on the RTS,S vaccine [2].
These results also suggest a potential risk factor for contracting submicroscopic malaria-- age [Figure 4]. As stated above, the difference in age group distribution between microscopic malaria patients and submicroscopic malaria patients was statistically significant (p=0.02271) [Figure 4]. This value indicates that the high proportion-- 50.2% [Table 2]-- of submicroscopic positive patients who are under the age of 5 and the almost equal distribution between age groups of microscopic positive patients represent contrasting relationships [Figure 4]. And these results suggest that age may impact an individual’s susceptibility to developing asymptomatic,
undetectable malaria versus detectable malaria. Therefore, future studies should continue to develop this relationship and continue to examine the validity of age as a risk factor for submicroscopic parasitemia. As RTS,S is likely to be targeted to children under 5, the
may have a larger impact on transmission intensity. However, this study would be difficult and intensive, as each child would have to be followed actively for disease by testing the blood at frequent intervals, since patients with submicroscopic parasitemia are asymptomatic.
This risk factor could have implications for clinical diagnosis and treatment of the disease in addition to impacting our understanding of RTS,S Phase III trial results. If children under 5 have a significantly greater risk of contracting submicroscopic parasitemia, they also are at a greater risk of contributing to transmission between humans even when asymptomatic.
Additionally, the trials performed by GlaxoSmithKline on the RTS,S vaccine used infants and children as its patients [7]. Therefore, a high proportion of children under 5 containing the Plasmodium Falciparum parasite in their blood in a form that could not be detected by
microscopy during initial Phase III trials could significantly impact the results produced by GlaxoSmithKline. Thus, in the future, GlaxoSmithKline should look to determine if the RTS,S vaccine can reduce submicroscopic parasitemia in addition to its effect on clinical disease. As the goal of the RTS,S malaria vaccine is to reduce and, eventually, to eliminate clinical mortality around the world, these questions will be important to address as vaccine development continues.
five—those already most significantly burdened with malaria—the greatest. Eliminating death from malaria in the future, therefore, will certainly involve the understanding and control of this relationship.
Acknowledgements
So many people from so many organizations across multiple countries have worked together to make this thesis possible for me, and each deserves my sincerest thanks. More specifically, I would like to thank the staff at The UNC Project in Malawi at the Kamuzu Central Hospital for working and cooperating with me during my two summers in Malawi, the UNC Summer Undergraduate Research Fellowship program for funding one of those research
summers, every member of the Juliano and Meshnick laboratories in the UNC Gillings School of Public Health for allowing me to join their malaria genomics staff, Karin Pfennig in the
References
1. "Factsheet on the World Malaria Report 2014." WHO. World Health Organization, n.d. Web. 18 Mar. 2015.
2. "Biology." Malaria. Centers for Disease Control and Prevention, n.d. Web. 18 Mar. 2015. 3. Duke-Sylvester, Scott et al. "The Effect of Intermittent Preventive Treatment on Anti-malarial Drug Resistance Spread in Areas with Population Movement." Malaria Journal 13.428 (2014): n. pag. Web. 18 Mar. 2015.
4. "Malaria Fact Sheet." Malaria. World Health Organization, n.d. Web. 02 Mar. 2015.
5. Gallup JL, Sachs JD. The Economic Burden of Malaria. In: Breman JG, Egan A, Keusch GT, editors. The Intolerable Burden of Malaria: A New Look at the Numbers: Supplement to Volume 64(1) of the American Journal of Tropical Medicine and Hygiene. Northbrook (IL): American Society of Tropical Medicine and Hygiene; 2001 Jan.
6. Group, N.M.W., NIAID Research Agenda for Malaria. 2008.
7. "Malaria Kills: Fact Sheet." The RTS,S Malaria Vaccine Candidate (n.d.): n. pag.MVI PATH. Malaria Vaccine Initiative. Web. 18 Mar. 2015.
8. Barrell, Bart et al. "Genome Sequence of the Human Malaria Parasite Plasmodium
Falciparum." Nature 419, 498-511 (3 October 2002). Nature Publishing Group, n.d. Web. 18 Mar. 2015.
9. Agnandji S. T., Lell B., Soulanoudjingar S. S., Fernandes J. F., Abossolo B. P., Conzelmann C., et al. (2011b). First results of phase 3 trial of RTS,S/AS01 malaria vaccine in African children. N. Engl. J. Med. 365 1863–1875 10.1056/NEJMoa1102287
10. Mayor, Alfredo et al. “Sub-Microscopic Infections and Long-Term Recrudescence of
Plasmodium Falciparum in Mozambican Pregnant Women.”Malaria Journal 8 (2009): 9. PMC. Web. 18 Mar. 2015.
11. Saute, F. , Menendez, C. , Mayor, A. , Aponte, J. , Gomez-Olive, X. , Dgedge, M. and Alonso, P. (2002), Malaria in pregnancy in rural Mozambique: the role of parity, submicroscopic and multiplePlasmodium falciparum infections. Tropical Medicine & International Health, 7: 19–28.
13.Harris, Ivor et al. “A Large Proportion of Asymptomatic Plasmodium infections with Low and Sub-Microscopic Parasite Densities in the Low Transmission Setting of Temotu Province, Solomon Islands: Challenges for Malaria Diagnostics in an Elimination Setting.” Malaria Journal 9 (2010): 254. PMC. Web. 18 Mar. 2015.
14. Lin, Jessica T., David L. Saunders, and Steven R. Meshnick. "The Role of Submicroscopic Parasitemia in Malaria Transmission: What Is the Evidence?" Trends in Parasitology 30.4 (2014): 183-90. Web.
15. Drakeley, Christopher et al. “Asymptomatic malaria infections: detectability, transmissibility and public health relevance.” Nature Reviews Microbiology (2014) Dec;12(12): 833–840.
16. Tedros A. Ghebreyesus, Mitiku Haile, Karen H. Witten, Asefaw Getachew,Mekonnen Yohannes, Steven W. Lindsay, and Peter Byass. Household risk factors for malaria among children in the Ethiopian highlands. Trans R Soc Trop Med Hyg (January-February 2000) 94 (1): 17-21.
17. K.A. Koram, S. Bennett, J.H. Adiamah, and B.M. Greenwood. Socio-economic risk factors for malaria in a peri-urban area of The Gambia. Trans R Soc Trop Med Hyg (March-April 1995) 89 (2): 146-150.
18. W. van der Hoek, F. Konradsen, D.S. Dijkstra, P.H. Amerasinghe, and F.P. Amerasinghe. Risk factors for malaria: a microepidemiological study in a village in Sri Lanka. Trans R Soc Trop Med Hyg (May-June) 92 (3): 265-269.
19. Golassa L, Enweji N, Erko B, Aseffa A, Swedberg G: Detection of a substantial number of Sub-microscopic Plasmodium falciparum infections by polymerase chain reaction: a potential threat to malaria control and diagnosis in Ethiopia. Malaria Journal 2013, 12:352.
20. Coleman, Russell E et al. “Comparison of PCR and Microscopy for the Detection of
Asymptomatic Malaria in a Plasmodium Falciparum/vivax endemic Area in Thailand.” Malaria Journal 5 (2006): 121. PMC. Web. 20 Mar. 2015.
21. The RTS,S Clinical Trials Partnership (2014). “Efficacy and Safety of the RTS,S/AS01 Malaria Vaccine during 18 Months after Vaccination: A Phase 3 Randomized, Controlled Trial in Children and Young Infants at 11 African Sites.” Ed. Sanjeev Krishna. PLoS Medicine 11.7 (2014): e1001685. PMC. Web. 25 Mar. 2015.
22. Berger, Stephen. Infectious Diseases of Malawi. Infectious Diseases of Malawi. N.p.: GIDEON Informatics, 2014. 194. Print.
23. Hoffman, Natalie et al. "Ultra-Sensitive Detection of Plasmodium Falciparum by
Characteristics Mean SD Age: Gender: Male Female 10.05 N=296 N=494 11.26
Number of Household Members
Number of Windows Number of Sleep Nets Hemoglobin
Wall Rating Torn Bed Nets
Parasitemia (parasites per microliter) 4.99 1.09 3.68 11.98 3.09 0.381 2224.27 1.64 0.3939 2.198 1.66 4.96 .486 31301.79
Overall Cohort
Microscopic Positive
Submicroscopic Positive
Age Under 5 398 14 39
Age 5-20 199 16 16
Age Over 20 195 15 13
Male 294 17 27
Female 498 28 41
Average Number of Household Members
4.99 4.71 5.21
Average Number of Windows 1.09 1.16 1.12
Average Number of Sleep Nets 3.68 3.47 3.78
Average Hemoglobin Count 11.98 11.76 11.97
Average Wall Rating (0-4) 3.09 2.29 2.99
Bed Net Torn (Percentage) 29.92% 24.44% 36.76%
Microscopy Results
RT-PCR Results
Submicroscopic Parasitemia
Chi Squared
P-value
Negative 747 710 724 10.738 0.00446
Positive 45 82 68
Percent Positive
5.68% 10.35% 8.59%
2011 - Prevalence by sex and age group
Male Female All
% Prevalence Total Pop % Prevalence Total Pop % Prevalence Total Pop
Under 5 10.4 211 12.7 189 11.5 400
5-20 22.0 100 16.0 100 19.0 200
Over 20 6.1 33 10.2 167 9.5 200
All age groups
14.0 344 12.5 456 12.9 800
2012 - Prevalence by sex and age group
Male Falciparum Female Falciparum All Falciparum
%
Prevalence Total Pop % Prevalence Total Pop % Prevalence Total Pop
Under 5 3.2 217 9.8 183 6.3 400
5-20 17.6 85 13.0 115 15.0 200
Over 20 0.0 16 4.9 184 4.5 200
All age
groups 6.9 318 8.7 482 8.0 800
2013 - Prevalence by sex and age group
Male Falciparum Female Falciparum All Falciparum
% Prevalence Total Pop % Prevalence Total Pop % Prevalence Total Pop
Under 5 3.1 191 3.9 203 3.5 400
5-20 12.8 86 4.5 110 8.0 200
Over 20 0 19 8.3 181 7.5 200
All age groups
5.7 296 5.7 494 5.6 800