Reading
Disability
With
Motor
Problems
May
Be an Inherited
Subtype
Sonya
M. Regehr,
MSc,
and
Bonnie
J. Kaplan,
PhD
From the Departments of Pediatrics and Psychology, University of Calgary, and Alberta Children ‘a Hospital Research Centre, Calgary, Alberta, Canada
ABSTRACT. There is evidence from a number of studies that various forms of reading disability are inherited. The familial patterns of one specific type of reading disability that occurs together with impaired coordination and
bal-ance were evaluated. Ten reading-disabled children with
these motor problems, ten children with only reading
problems, and ten control children without reading dis-abilities were examined along with their siblings and
parents. The control children were matched to the
read-ing-disabled children for age, sex, and family
socioeco-nomic status. A high prevalence of reading and motor
problems was found in the relatives of the children with
reading disability and motor problems, whereas a high
prevalence of only reading problems was found in the
relatives of the children with only reading disability.
There were no differences among the three groups of
children or their siblings on number of pregnancy and
birth complications or prevalence of attention deficit
disorder. It was concluded that reading disability with
motor problems may be an inherited type of reading
disability, distinct from reading disabifity without motor problems, which is also inherited. Pediatrics 1988; 82:204-210; reading disability, motor deficit, genetias.
There is evidence that reading disability in
gen-eral is inherited. The concordance rate for the
disorder is 70% for monozygotic twin pairs and only
31% for dizygotic twin pairs.’ Furthermore, in
nu-merous studies evidence of strong familial patterns
of the disorder has been found. For instance,
Hallgren2 tested 90 families in which one of the
parents was reading disabled and found that 45.7%
of their offspring were also. None of the studies on
reading disability in general, however, has been able
to establish the mode of genetic transmission. For
instance, Lewitter et al3 performed segregation
Received for publication Sept 1, 1987; accepted Nov 23, 1987. Reprint requests to (B.J.K.) Alberta Children’s Hospital Re-search Centre, 1820 Richmond Ed, SW, Calgary, Alberta, Can-ada T2T 5C7.
PEDIATRICS (ISSN 0031 4005). Copyright © 1988 by the American Academy of Pediatrics.
analysis for 133 family pedigrees and found no
evidence of a single dominant or recessive gene
responsible for the disorder. They concluded that
reading disability is heterogeneous and that any
further attempts at genetic analysis would require
prior classification of the reading-disabled families
into subtypes.
Investigators have conducted research on the
in-heritance of subtypes of reading disability.4 Two
major subtypes have been studied: reading
disabil-ity associated with verbal/language problems and
reading disability associated with visual/spatial
problems. Several types of research indicate that
the verbal/language subtype of reading disability is
inherited. It tends to occur frequently within only
certain families, making a relative of a
reading-disabled individual of this subtype not only more
likely to be reading disabled but also more likely to
be of this particular subtype.’ One group of
re-searchers found evidence that a gene on chromo-some 15 may be responsible for the transmission of
this subtype of reading disability.5 Investigators
have also found evidence of familial patterns for
the visual/spatial type of reading disability,6’7 but
no one has yet isolated a gene that may be
respon-sible for this subtype.
These two subtypes of reading disability are by
no means the only ones that have been postulated8;
they are, however, the only ones that have been
examined for genetic cause. Another subtype of
reading disability which has been hypothesized,9
but not yet analyzed for genetic involvement, is
reading disability characterized by the cooccurrence of impaired balance and coordination. Researchers
have noted that many individuals with reading
disability have motor as well as reading problems:
they have been found to perform abnormally on
tests of balance, coordination, posture, body
equi-librium, spatial visualization, oculomotor control,
sug-gested that these motor problems are indicative of
cerebellovestibular dysfunction’5 and that the
rea-son these children have trouble reading is because
of impaired ocular fixation and scanning abilities,
as well as limited cerebellar capacity to regulate the
order and speed of sensory input to the cortex.’2”5
The aim of the current study was to examine the
inheritance ofthis subtype of reading disability that
is associated with signs of cerebellovestibular
dys-function. Ten reading disabled children with motor
problems (group RDMP), ten children with only
reading disability (group RDO), and ten control
children with no problems in either area (group
NC), plus the siblings and parents of each type,
were compared on a variety of motor and reading
tests to determine whether (1) the relatives of one
type of child were more likely to be of that type as
well and (2) children in group RDMP appeared to
be a genetically separate disorder from those in
group RDO.
METHODS
Subjects
Ten children from each of the three groups were
selected from referrals to the local children’s
hos-pita! and from the public and private school sys-tems. A total of 74 suitable families were contacted
before 30 willing participants could be found. The
most typical reasons for families declining to
par-ticipate were that the parents were embarrassed
about their own reading disability, that families
were too busy, or that the parents thought that
their child had been overtested already.
The control children were matched as closely as
possible to the children in group RDMP for gender,
age, and family socioeconomic status, using the
socioeconomic index for occupations in Canada.’6
Most families consisted of the child initially re-ferred to the study (the proband), a biologic sibling
of that child, and the children’s biologic parents. In
three cases, however, the father was unwilling to be
tested, and so only the proband, a sibling, and the
mother participated. When more than one sibling
was available for the study, the one closest in age
to the proband was chosen. All children were
be-tween the ages of 7 and 14 years, and each child
from the reading disability groups had a full-scale
IQ score of at least 85 and a performance or verbal scale score of at least 90 as assessed by the Wechsler
Intelligence Scale for Children-Revised
(WISC-R).’7 There were no significant differences between
the three groups or the siblings for age, sex, or
socioeconomic status, according to analysis of
var-iance.
Procedure
Each family member was tested individually for
30 to 60 minutes by one of the authors (S.R.).
Subjects were first given the balance, bilateral
co-ordination, and upper limb coordination subtests
of the Bruininks-Oseretsky Motor Proficiency
Test,’8 the motor accuracy and design copy subtests
of the Southern California Sensory Integration
Test,’9 and a test of fast successive and alternating
finger, hand, and foot movements.20’2’ Next, the
reading recognition, reading comprehension, and
spelling subtests of the Peabody Individual
Achievement Test (PIAT)22 were administered.
The parents were also given a self-report
question-naire concerning their reading history and their
own perception of their current reading ability. In
addition, the mothers were given a questionnaire
concerning pregnancy and birth complications24
and the Conners’ Abbreviated Symptom
Question-naire for attention deficit disorder for both of
their children in the study.
The examiner who tested all of the children was
aware of the experimental hypotheses and the
re-ferral status of the children. Final assignment of
children to one of the three groups, however, was
not determined until after all assessments were
finished. In addition, the objective nature of the
standardized tests was thought to minimize
sub-stantially any potential experimenter bias. All of
the reading and motor tests used in this study had
objective, quantifiable formats (primarily multiple
choice), in contrast to interpretive, qualitative
eval-uations such as those found in ,informal reading
inventories or the typical neurologic examination.
Group Assignment
When probands were initially referred to the
study, they were temporarily assigned to one of the
three groups based on available records. Final group
assignment was determined by performance on the
measures. For classification as only reading dis-abled or reading disabled with motor problems, a child had to have a reading quotient of less than
0.90, calculated as observed age divided by expected
age, where observed age was defined as the mean
score of three PIAT subtests (reading recognition,
reading comprehension, and spelling) and expected
age was defmed as the mean of the child’s
chrono-logic age, mental age, and age for grade. Other
reading quotient scores of our Canadian sample are
inflated by the PIAT, which overestimates reading
ability. For instance, our control children were
re-ported by their parents to be average readers in school, yet their average percentile scores were high
relative to the American norms: 78.20 on reading
recognition, 81.20 on reading comprehension, and
74.40 on spelling. Furthermore, plotting the reading
quotient scores revealed a bimodal and
nonoverlap-ping distribution with all children referred to the
study as reading disabled scoring below 0.90 and all
children referred to the study as normal readers
scoring above 1.00.
To be classified as having motor problems, a child
had to score at least 1 SD below the test mean in
two of the following areas: balance, bilateral
coor-dination, upper limb coordination, and fme motor
coordination. As with the reading tests, some of the
balance and coordination tests appeared to
over-estimate the children’s ability relative to their
peers, and therefore these somewhat liberal
diag-nostic criteria were adopted. It is important to note
that even with these somewhat liberal diagnostic
criteria, none of the control children referred to the
study were found to have motor problems.
RESULTS
To confirm that the proband groups did differ
from each other on the reading and motor variables
as intended, a multivariate analysis of variance was
done with proband diagnosis as the grouping
van-able and balance, bilateral coordination, and upper
limb coordination (as assessed by the
Bruininks-Oseretsky test), fine motor coordination (as
as-sessed by the design copy, motor accuracy, and foot
and hand movement tests), and reading
recogni-tion, reading comprehension, and speffing (as
as-sessed by the PIAT) as the dependent variables.
Overall, the three groups differed significantly from
each other (F (24, 32) = 12.14, P < .0001), and so
the univariate tests were examined. Significant
dif-ferences were found on each of the seven variables
(P < .0001). Newman-Keuls multiple comparisons
(a 0.05) confirmed that the probands in group
RDMP were impaired on the motor tests relative
to the other two groups, which did not differ from
each other, and the children in the RDO and RDMP
groups were impaired on the reading tests relative
to the control group but did not differ from each
other. Furthermore, there were no significant
dif-ferences among the three groups of probands or
their siblings on reports of pregnancy and birth
complications, attention deficit disorder, age, sex,
or socioeconomic status. The IQ data for probands
in groups RDO and RDMP were also examined,
and it was found that although the probands in the
RDO group had much higher performance (mean
110.0) than verbal (mean 101.9) scale scores (t (9)
= 2.35, P < .05), the probands in the RDMP group
had relatively similar verbal (mean 101.2) and
per-formance (mean 102.1) scores.
A multivariate analysis of variance test was then
performed on the sibling data, with proband
diag-nosis as the between-group variable and the seven
reading and motor tests as the dependent variables.
Overall, the three groups of siblings differed
signif-icantly from each other (F (16, 40) = 3.63, P <
.0005) and specifically on bilateral coordination (F
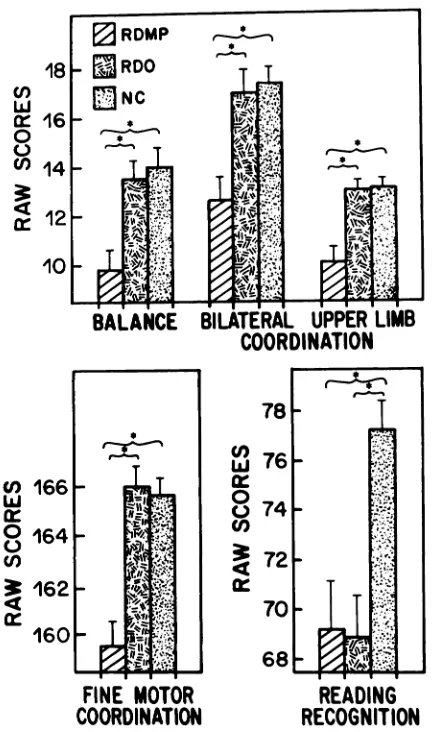
(2, 27) = 15.75, P < .0001), upper limb coordination (F (2, 27) = 6.95, P < .005), fine motor coordination (F (2, 27) = 8.62, P < .001), reading comprehension (F (2, 27) = 7.07, P < .005), and reading recognition (F (2, 27) = 5.84, P < .008). Newman-Keuls
com-parisons revealed that siblings of children in the
RDMP group were impaired on bilateral and upper
limb coordination relative to siblings of those in
the other two groups, who did not differ from each
other, and siblings of children in the RDMP and
RDO groups were impaired on fine motor
coordi-nation relative to siblings of control children but
did not differ from each other. Finally, siblings of
children in the RDMP and RDO groups were
im-paired relative to siblings of control children but
did not differ from each other, on reading
recogni-tion and reading comprehension (Fig 1).
Similar analyses of parent data resulted in
com-parable separation of groups. Overall, there were
significant differences between the parent groups
(F (18, 32) = 4.38, P < .001), and specifically there
were differences on balance (F (2, 24) = 8.41, P <
.005), bilateral coordination (F (2, 24) = 7.50, P <
.005), upper limb coordination (F (2, 24) = 17.42,
P < .0001), fine motor coordination (F (2, 24) =
17.24, P < .0001), and reading recognition (F (2,
24) = 5.98, P < .01). Newman-Keuls comparisons
revealed that parents of children in group RDMP
were impaired relative to the parents of the other
two groups of children on balance, bilateral
coor-dination, upper limb coordination, and fine motor
coordination and that parents of children in groups
RDO and RDMP were impaired relative to parents
of control children on reading recognition (Fig 2).
For the purposes of drawing up pedigrees of the
30 families (Fig 3), criteria were established for
diagnosing reading disability and motor problems.
For siblings, an average reading and spelling score
below the 50th percentile was required for a
diag-nosis of reading disability. Scores more than 0.5 SD
below test means in two of the four motor areas
were required for a diagnosis of motor problems.
U)
z
5z
LLfl-cU)
Lu
Za::
U)
18
U)
Lu
c 16
0 C-)
U)
14
4
c 12
10
RDMP
‘:i-’
.RDO T
T
_Fc
‘-.-..---‘ IF.4,
.
,. *
F ::.,
-
.- L’ .;:;,:
BALANCE
BILATERAL
UPPER LIMB
COORDINATION
COORDINATION
READING
READING
RECOGNITION
cOMPREHENSION
FINE MOTOR
COORDINATION
Ld0 0
Li
-I pa:
zO
L&jL
0
a:
Lu
Fig 1. Means and standard errors of three groups of
siblings on motor and reading tests. Only variables for
which univariate analyses revealed significant group
dif-ferences are displayed. An asterisk indicates that two
groups marked by brackets differ from each other at P <
.05 by Newman-Keuls post hoc test. Abbreviations:
RDMP, reading disability and motor problems; RDO,
reading disability only; NC, control.
because (1) evidence discussed earlier indicated that
the children’s scores were being inflated by both
the reading and motor tests, and (2) it has been
argued that, in a genetic study, to diagnose mild
reading disability in family members as the absence
of a reading disability would be misleading.27
Clas-sifying parents required using the control adults in
this study as reference, because many of the tests
used did not provide norms for adults. Reading
disability was diagnosed in parents if they had an
average reading and spelling score at least two grade
levels below the average score for the control par-ents. For a diagnosis of motor problems, a parent
had to score more than 1.5 SD below the control
means in two of the four motor areas.
None of the 20 control parents or ten siblings of
control children met the diagnostic criteria for read-ing disability, but one control father met the criteria
78
76
fl
w
7472
70-68____
READING
RECOGNITION
Fig 2. Means and standard errors of three groups of
parents on motor and reading tests. Only variables for
which univariate analyses revealed significant group
dif-ferences are displayed. An asterisk indicates that two
groups marked by brackets differ from each other at P <
.05 by Newman-Keuls post hoc test. Abbreviations:
RDMP, reading disability and motor problems; RDO,
reading disability only; NC, control.
for motor problems. Two families with only reading
disability had more than one child aged 7 to 14
years, and these additional children were tested for
inclusion in the pedigrees, although their data were
not included in the statistical analyses. The
evi-dence of the pedigrees supports the findings of the
statistical analyses. Two distinct familial patterns
emerged, with reading disabilities often occurring
alone among the relatives of the probands with
reading disability only but rarely occurring without
motor problems among the relatives of the
pro-bands from the RDMP group. It is likely that these
familial patterns were genetic, because the two
reading disability groups did not differ from the
control groups on socioeconomic status or on
re-ports of pregnancy and birth complications. Also,
parents of the probands from the reading disability
pro-____
j:
#{149}RDMP
0
MPQ
RDO0
Normal j Not TestedFig
3.
A, Pedigrees of families with a proband withreading disability and motor problem (RDMP). B, Pedi-grees of families with a proband with only reading
disa-bility (RDO). Asterisk indicates an RDO family which is
probably more appropriately characterized as RDMP.
Child referred to study happened to be RDO, however,
and so their data were analyzed with IWO group. Arrows
point to probands in each family.
bands on their responses to the question “How
often do (did) you read to your children?”,
suggest-ing that there was no difference in environmental
variables which might facilitate reading.
To determine whether the reading and motor
problems were associated in families with reading
disabilities and motor problems, a
x2
analysis wasperformed on the sibling data. There was a
signifi-cant association between the two
(x2
= 6.24, P =0.035), suggesting that reading and motor problems
in this group were not of separate origins but were
related, possibly sharing one common genetic cause.
DISCUSSION
It had been predicted that the relatives of the
children with reading disability without motor
problems would be more likely to have the same
difficulty as well and that the relatives of the
chil-dren with reading disability and motor problems
would be more likely to be reading disabled and
have motor problems. This prediction was
con-firmed by the results of the study: the siblings and
parents of the children in group RDMP performed
worse than the relatives of the children in the other
two groups on the tests of motor ability, and the
siblings and parents of children in both
reading-disabled groups were impaired relative to the
rela-tives of the control children on reading. The
differ-ences between the groups on reading and spelling
ability, however, were not as striking as the
differ-ences on motor ability. Perhaps this was because
our society places more emphasis on remediating
reading difficulties than on correcting coordination
and balance. Thus, a strong environmental effect
could have diminished the expected familial
pat-terns on reading and have little effect on the
pat-terns of motor ability. In general, the siblings and
parents of the probands who were reading disabled
only were more likely to be reading disabled only
as well, and the siblings and parents ofthe probands
with motor problems and reading disability were
more likely to be reading disabled and have motor
problems.
The data also supported the idea that reading
disability with motor problems is a separate
disor-der from reading disability only: the siblings of the
probands with reading disability and motor
prob-lems had deficits on bilateral coordination and
up-per limb coordination relative to the control
sib-lings, but the relatives of the probands with only
reading disability did not. Similarly, the parents of
the probands with reading disability and motor
problems had deficits on balance, bilateral
coordi-nation, upper limb coordination, and motor
accu-racy relative to the control group, whereas the
parents ofthe probands with reading disability only
did not. Thus, among the siblings and parents,
motor problems were primarily confined to the
relatives of the probands with motor problems.
Examination of the family pedigrees (Fig 3)
con-firms this idea: there were certain families with a
history of both reading and motor problems and
others with a history of only reading problems.
One finding, however, did contradict the
hypoth-esis that motor problems were unique to the
rela-tives of probands with both reading and motor
problems. The siblings ofthe probands with reading
disability only, although scoring significantly better
than the siblings of the RDMP probands with both
reading and motor problems, scored significantly
worse than the control siblings on fine motor
co-ordination. This could mean that, although balance
and gross motor coordination problems are specific
motor problems, deficits in fine motor coordination
can occur in the children of families with a history
of reading disability only. It should be noted,
how-ever, that the tests of fine motor coordination often
resembled academic tests, requiring children to
draw or trace using a pen or pencil. The tests of
gross motor coordination and balance involved
tasks such as walking on a balance beam or
throw-ing a ball, which are less like academic tests than
tasks involving drawing and tracing. Perhaps, then,
the children with only reading disability, who had
already experienced a considerable amount of
fail-ure on traditional academic tasks, became more
nervous and unsure on the tests of fine motor
coordination than on the other motor tests, and as
a result performed more poorly.
Efforts were made in this study to control for a
number of the nongenetic factors that can affect
familial patterns of reading ability. For instance, it
was found that the groups of reading-disabled
chil-dren did not differ from the group of control
chil-dren on socioeconomic status or reports of
preg-nancy and birth complications. Also, the parents of
the reading-disabled probands did not differ from
the parents of the control probands on their
re-sponses to the question “How often do (did) you
read to your children?” Indeed, the parents of the
reading-disabled children placed great emphasis on
the importance of being able to read well, and many
were paying considerable tuition to have their
chil-dren educated in special schools for the learning
disabled. Thus, it appears relatively unlikely that
the observed familial patterns of reading disability
were due to nongenetic factors such as family
so-cioeconomic status or negative attitudes toward
reading shared in certain families.
The sample may have been biased in that biologic
families willing to volunteer a considerable amount of time for research were required. Many families
who were called about the study refused to
partici-pate, partly because of the time commitment
in-volved and partly because many parents were
em-barrassed about their inability to read and did not
want to be tested. Embarrassment about a reading
disability was particularly common among the
fa-thers: 44 of 74 families who were called regarding
the study declined to participate, and of these 44
families who declined, 15 did so because the father
was unwilling to be tested. Eventually, some
fami-lies were tested without the father to keep the
sample from becoming too biased. Even so, the final
sample of families with reading-disabled members
was middle to upper class, which is probably not
typical of all families with reading-disabled
chil-dren. In this case, the bias of the sample probably
served to weaken the results. One would expect that
inclusion of the more severely impaired parents
would result in even stronger evidence of familial
patterns.
The size of the sample in this study (n = 10 for
each proband group) was small, but power analyses
performed before the study began indicated that
reducing the heterogeneity among the
reading-dis-abled children by considering subgroups yielded
sufficient power to detect differences among the
groups. Indeed, because conservative a levels were
used to ensure that we did not make any type I errors (reporting the existence of an effect which was due to chance alone), the significant differences
among the groups that emerged are especially
corn-pelling.
The physiologic basis of the coordination and
balance problems in children with reading disability
and motor problems is not known, although the
type of dysfunction seen suggests cerebellovestibu-lar involvement. It is also not known whether the
children’s motor problems are related to their
read-ing problems, but it seems feasible that their
cere-bellovestibular dysfunction could result in an
ina-bility to precisely control eye-hand movements in
the gathering of sensory information and then to
accurately relay this information from the retina to
the cortex. This could, in turn, result in reading
difficulties.
Several studies have reported abnormal and
er-ratic eye movements in reading-disabled
chil-dren.#{176} Furthermore, in one of these studies,#{176}the
eye movements of children with gross and fine
motor deficits similar to those of the children with
motor problems in this study, were examined,
in-cluding three children who were actually part of the
sample of children with both motor and reading
problems in the present study. These researchers
found that their reading-disabled subjects with
mo-tor problems had significantly worse fixational
con-trol when viewing a simple stationary stimulus than
did a group of normal control children.
Further-more, the degree of fixational instability exhibited
by these children has been shown to substantially
degrade visual resolution,3’ and so it might be
pre-dicted that their oculomotor problems would
di-rectly affect their visual processing ability when reading. It has also been reported that patients with
a neurologic disorder and acquired fixational
con-trol problems have great difficulty reading because
the words and letters appear to “jump about.”32
Thus, oculomotor control could be a mechanism
whereby the motor problems of the
reading-dis-abled children in the present study could affect
reading ability. That these children may have had
such visual/motor problems was indicated by the
disa-bility only, like many reading-disabled children,
had much higher verbal than performance IQ
scores, the children with motor problems had
sim-ilar verbal and performance scores. One could argue
that the children with reading disability only had a
primary verbal/language problem, which affected
their verbal but not performance IQ scores.
Con-versely, the children with both reading and motor
problems may have had a primary visual/motor
problem affecting their performance score and a
verbal/language problem secondary to their visual
deficits. Specifically, the visual/motor problem
might have resulted in an inability to read and
therefore to develop the vocabulary that affects
verbal IQ scores. There is some evidence to suggest
that the children with reading disability and motor
problems in this study had motor deficits which
may have included oculomotor problems resulting
in a visually based reading deficit. More research is
needed, however, regarding this controversial issue
of oculomotor dysfunction in children with reading
disabilities.
SUMMARY
In conclusion, this study has shown that two
types of reading disability do show strong familial
patterns, with some families having a history of one
type or the other. Furthermore, in the families with
a history of reading disability and motor problems,
it appears that the reading and motor problems are
related, perhaps as part of one genetic disorder
characterized by underlying cerebellovestibular
dysfunction. More research is now needed to
repli-cate these findings and also to use segregation
analysis to investigate the possible mode of
inher-itance.
ACKNOWLEDGMENT
This research was funded by the Alberta Heritage
Foundation for Medical Research.
REFERENCES
1. Pennington BF, Smith SD: Genetic influences on learning disabilities and speech and language disorders. Child Dev 1983;54:369-387
2. Hallgren M: Specific dyslexia (“congenital word blindness”):
A clinical and genetic study. Acta Psychiatr Neural Scand (suppl) 1950, p 65
3. Lewitter F!, DeFries JC, Elston RC: Genetic models of reading disability. Behau Genet 1980;10:9-30
4. Regehr 5: The genetic aspects of developmental dyslexia. Can J Behav Sci 1987;19:240-253
5. Smith SD, Kimberling WJ, Pennington BF, et a!: Specific reading disability: Identification of an inherited form through linkage analysis. Science 1983;219:1345-1347
6. Childs B, Finucci JM: The genetics of learning disabilities. Ciba Found Symp 1979;66:359-376
7. Omenn GS, Weber BA: Dyslexia: Search for phenotypic and genetic heterogeneity. Am J Med Genet 1978;1:333-342
8. Rourke BP: Overview of learning disability subtypes, in Rourke BP (ed): Neuropsychology of Learning Disabilities: Essentials of Subtype Analysis. New York, Guilford Press,
1985, pp 3-14
9. Doehring, DG: Reading disability subtypes: Interaction of reading and nonreading deficits, in Rourke BP (ed): Neu-rOpSyChO1y of Learning Disabilities: Essentials of Subtype Analysis New York, Guilford Press, 1985, pp 133-146
10. Ayres AJ: Deficits in sensory integration in educationally handicapped children. J Learning Disabil 1969;2:160-168
11. De Quiros JB: Diagnosis ofvestibular disorders in the
learn-ing disabled. J Learning Disabil 1976;9:50-58
12. Ottenbacher K: Excessive postrotary nystagmus duration in learning disabled children. Am J Occup Ther 1980;34:40-44
13. Steinberg MA, Rendle-Short J: Neuro-sensori-motor dys-function in young children with educational and behavioural problems and controls. Except Child 1980;27:107-114
14. Younes RP, Rosner B, Webb G: Neuroimmaturity of learn-ing-disabled children: A controlled study. Dev Med Child
Neurol 1983;25:574-579
15. Levinson HN: A Solution to the Riddle Dyslexia. New York, Springer-Verlag, 1980
16. Blishen BR, McRoberts HA: A revised socioeconomic index for occupations in Canada. Can Rev Social Anthropol 1976;13:71-79
17. Wechsler D: Manual for the Wechsler Intelligence Scale for Children-Revised. New York, Psychological Corporation,
1974
18. Bruininks RH: Bruininks-Oseretsky Test of Motor
Profi-ciency. Circle Pines, MN, American Guidance Services, 1978
19. Ayres AJ: Southern California Sensory Integration Test
Bat-teiy. Los Angeles, Western Psychological Services, 1972 20. Denckla MB: Development of speed in repetitive and
suc-cessive finger-movements in normal children. Dev Med
Child Neurol 1973;15:635-645
21. Denckla MB: Development of motor co-ordination in
nor-mel children. Dev Med Child Neurol 1974;16:729-741
22. Dunn L, Markwardt F: Peabody Individual Achievement Test. Circle Pines, MN, American Guidance Services, 1970
23. Finucci JM, Whitehouse CC, Isaacs SD, et al: Derivation and validation ofa quantitative definition ofspecific reading disability for adults. Dev Med Child Neurol 1984;26:143-153
24. Levine MD: The Anaer System Parent Questionnaire, Form
2P. Cambridge, MA, Educators Publishing Service mc, 1980
25. Goyette CH, Conners CK, Ulrich RF: Normative data on revised Conners parent and teacher rating scales. JAbnorm
Child Psychol 1978;6:221-236
26. Finucci JM, Isaacs SD, Whitehouse CC, et al: Empirical validation of reading and spelling quotients. Dev Med Child Neurol 1982;24:733-744
27. Pennrngton BF: Issues in the diagnosis and phenotypic analysis of dyslexia: Implications for family studies, in Smith SD (ed): The GenetiCs of Learning Disabilities: Gene-typic Studies. San Diego, College Hill Press, 1986, pp 69-96
28. Zangwill OL, Blakemore C: Dyslexia: Reversal of
eye-move-ments during reading. Neuropsychologia 1972;10:371-373
29. Pavlidis GTh: Do eye movements hold the key to dyslexia? Neuropsychologia 1981;19:57-64
30. Raymond J, Ogden N, Fagan J, et al: Fixational instability and saccadic eye movements ofdyslexic children with subtle cerebellar dysfunction. Am J Optom Physiol Opt 1988;65: 174-181
31. Murphy BJ: Pattern threshold for moving and stationary gratings during smooth eye movement. Vision Res 1978; 18:521-530
32. Natheson M, Bergman PS, Bender MB: Reading disturb-ances in the presence of oculomotor disorders. Eur Neurol