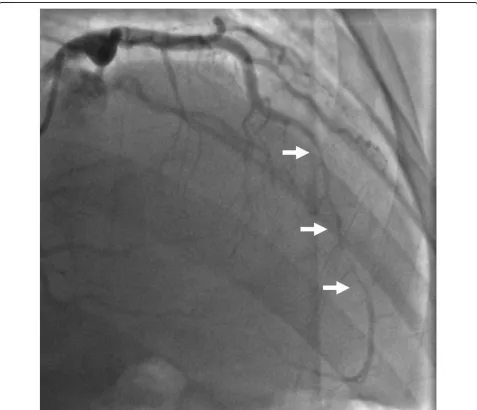
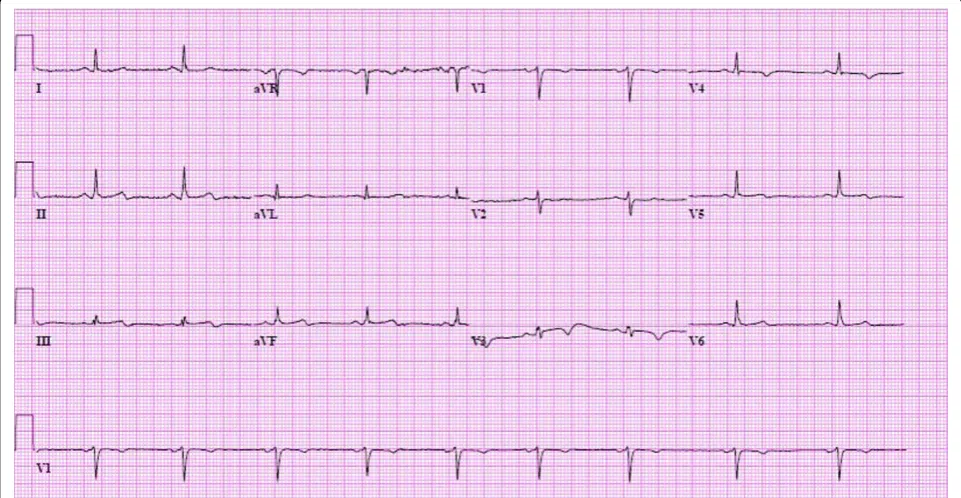
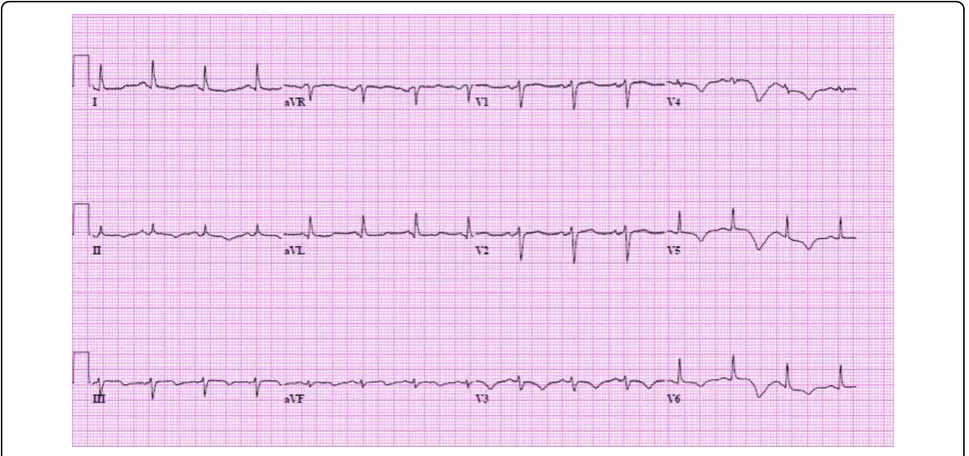
Recurrent post-partum coronary artery dissection
Full text
Figure
Related documents
The identified models which can be used to forecast values for arrival and service level of tractor drawn carts are developed for subsequent hours at harvest
The resistances could be seen as a direct response to a government policy that disavows or has failed to identify the conflict- generating potential in a strategy geared
The wavy surface is selected to increase the heat transfer rate and thermal efficiency in the heat exchanger square channel.. The insertion method in the middle
employers are equally important. This comment proposes that the arbitrary and capricious standard should apply to all plan interpretation practices to promote plan creation, and as
In this manuscript, numerical solutions of both the fractional diffusion and fractional diffusion-wave equations have been obtained by a Petrov-Galerkin finite element method
Density-Based Algorithm (DBSCAN) is a data clustering algorithm proposed by Ester in 1996. It is a method of quick logical division by grouping a set of points in a space that
