Effect on changes of blood coagulation function, cytokines and immune
function in patients undergoing laparoscopic radical gastrectomy for
gastric cancer
Jia-Qi Liu
1, Shao-Jun Yang
2, Jie-Qing Chen
1, Ru-Kui Su
1, Zhong Huang
1, Yin-Zhuo Qi
11Department of General Surgery, Beihai People's Hospital of Guangxi Province, Beihai 536000, China
2The Spleen and Stomach Diseases, Beihai People's Hospital of Guangxi Province, Beihai 536000, China
Journal of Hainan Medical University
http://www.hnykdxxb.com
ARTICLE INFO ABSTRACT
Article history:
Received 7 Jul 2016
Received in revised form 17 Jul 2016 Accepted 12 Jul 2016
Available online 24 Jul 2016
Keywords:
Laparoscopic radical gastrectomy for gastric cancer
Coagulation function Cytokine
Immune function Perioperative period
Corresponding author: Yin-Zhuo Qi, Department of General Surgery, Beihai
People's Hospital of Guangxi Province, Beihai 536000, China.
Fund project: Research Project of Beihai Municipal Science and Technology Bureau (No.: 201602026).
1. Introduction
Gastric cancer is the highest incidence of malignant tumors of the digestive tract[1], and laparoscopic radical gastrectomy for
gastric cancer is a common method in the treatment of gastric cancer, with advantages of less trauma, faster recovery time and less complications[2], but because of the characteristics of the surgery itself will cause a certain degree of damage to the patient, for example, ischemic reperfusion, increased oxidative stress, inflammatory response, as well as the complement system activation and changes in immune function, which can affect the treatment of cancer and surgery rehabilitation[3]. This study examined the
changes of blood coagulation function related index, cytokines and T lymphocyte levels in gastric cancer patients with laparoscopic radical gastrectomy for gastric cancer before and after at different periods, and to explore the clinical significance of related index changes on the treatment of cancer and surgical rehabilitation.
2. Materials and methods
2.1. General data
Collection of 40 cases of laparoscopic radical gastrectomy for gastric cancer (laparoscopic group) and 40 cases of radical gastrectomy (open group) was done in our hospital from May 2014 to May. The laparoscopic group 40 cases, male 28 cases,
female 12 cases, aged 40 to 79 years old, weight 45–79 kg, average (64.13±8.61) kg, the average operation time was (130.17±18.46) min, (175.38±22.48) mL average amount of bleeding during
operation; Among them, the 13 cases of cardiac carcinoma, 12 cases of gastric body and gastric carcinoma in 15 cases; According to the TNM staging of II grade 15 cases, III grade 25 cases; the radical distal gastrectomy in 23 cases, proximal gastrectomy in 5 cases, 12 cases of total gastrectomy. The laparoscopic group 40
cases, male 26 cases, female 14 cases, aged 40–79 years old, weight 45–79 kg, average (63.83±8.55) kg, the average operation time was (138.24±21.33) min, (184.62±25.67) mL average amount of
bleeding during operation; The cardiac carcinoma in 12 cases, 12 cases of gastric body and 16 cases of gastric cancer; According to the TNM staging of II grade 16 cases, III grade 24 cases; the radical distal gastrectomy in 22 cases, proximal gastrectomy in 6 cases, 12 cases of total gastrectomy. There were no statistical differences in age, sex, and physical condition between the two groups of patients with gastric cancer (P>0.05).
2.2.
Inclusion and exclusion criteria
All patients were diagnosed by the relevant inspection in 2011 the Ministry of health "standard" in the treatment of gastric cancer; All patients were consistent with the standard treatment of laparoscopic radical gastrectomy and open surgery; With the immune disease, heart disease, respiratory system disease, endocrine disease and dysfunction of liver and kidney diseases; Exclude tumor metastasis or recurrence and received chemotherapy treatment, infectious diseases and surgery patients; All the patients can actively cooperate with the treatment and treatment of related drug allergy; Patients before treatment are detailed information. This study was approved by the ethics committee of our hospital, and the patients signed the informed consent to carry out.
2.3. Blood sample collection
5 mL fasting peripheral blood of laparoscopic gastric cancer patients with radical correction was collected before surgery (T0), 1 d (T1) after surgery, 3 d (T3) after surgery and 5 d (T5) after surgery, to detect the relevant indicators by laboratory tests.
2.4. Cytokine detection
CRP (C reactive protein), IL-6 (IL-6) and TNF-alpha (Tumor necrosis factor-alpha) were determined by enzyme-linked immunosorbent assay kit from Wuhan Huamei Biological Engineering Co. Ltd., Nanjing Kingsy Biological Technology Co., Ltd. and Hangzhou point state biotechnology limited company. Infinite 200 (Eliasa Company: TECAN, Switzerland) was used in the determination of the OD value of 450 nm, and the corresponding concentration by standard curve calculation, operation process was done in strict accordance with the instructions.
2.5. T lymphocyte detection
FACSCalibur/Calibur flow cytometry (BD, USA) was used to detect CD4+, CD8+ and CD4+/CD8+ levels in patients undergoing laparoscopic radical gastrectomy for gastric cancer. The experiment was conducted in strict accordance with the specification.
2.6. Coagulation function test
CA-500 automatic blood coagulation analyzer (Sysmex, Japan) was used to detect the laparoscopic radical gastrectomy for gastric cancer patients during peri APTT (activated partial thromboplastin time), fibrinogen (FIB), platelet (PLT), and experimental operation was done in strict accordance with the instructions.
2.7. Statistical analysis
Statistics and analysis of relevant data was performed by statistical software SPSS19.0, coagulation function, cytokines and T lymphocyte are represented by the mean and standard deviation and subjected to comparison analysis of variance; the difference was statistically significant when P<0.05.
3. Results
3.1. Comparison of blood coagulation function in two patients
with gastric cancer after radical operation
levels was significantly lower than that before surgery in two group patients and laparotomy patients index decreased more significantly (P<0.05); 3 d after surgery, APTT and PLT in two group patients was significantly lower than that of T1 and FIB were significantly higher than that of T1 (P<0.05), but the laparotomy group patients were significantly lower than the laparoscopic group (P<0.05). 5 d after surgery, the APTT, FIB and PLT levels in the two groups were significantly higher than that of the T3 (P<0.05), and the patients in the open group were significantly lower than that in the laparoscopic group (P<0.05) (Table 1).
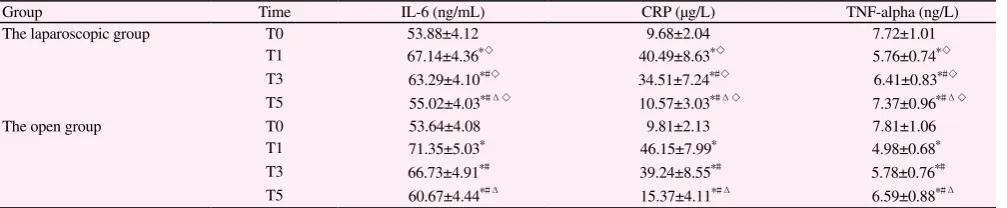
3.2. Comparison of cytokines in two patients with gastric
cancer during perioperative period
Detection analysis of cytokines IL-6, CRP and TNF-alpha in patients with radical operation of laparoscopic gastric cancer in perioperative before operation by ELISA found that the cytokine IL-6, CRP and TNF-alpha levels in two groups of patients did not change significantly (P>0.05); 1 d after the operation, the IL-6 and CRP levels in two groups of patients were significantly higher than that before operation (P<0.05), while TNF-alpha was lower than that before surgery, compared with the laparoscopic group (P<0.05), and the index change in open group patients wasmore obvious; 3 d after operation, IL-6 and CRP level in two group patients was significantly lower than at the T1 (P<0.05), while TNF-alpha level was significantly higher than that of T1 (P<0.05). The IL-6 and CRP in open surgery group was significantly higher than that in the laparoscopic group (P<0.05), and TNF-alpha was significantly lower than that in the laparoscopic group (P<0.05); 5 d after operation,
IL-6 and CRP levels in two patients were significantly lower than that of T3 (P<0.05), TNF-alpha level was significantly higher than that of T3 (P<0.05). IL-6 and CRP were significantly higher in the open group than in the laparoscopic group (P<0.05), TNF-alpha was significantly lower than the laparoscopic group (P<0.05) (Table 2).
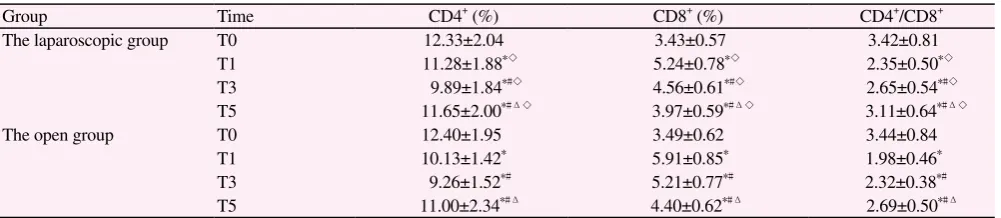
3.3. Comparison of T lymphocytes in two group patients with
gastric cancer undergoing radical operation in perioperative
period
Detection analysis of T lymphocytes CD4+, CD8+ and CD4+/CD8+ in patients with laparoscopic gastric cancer of radical resection of perioperative period by flow cytometry analysis found that the T lymphocyte CD4+, CD8+ and CD4+/CD8+ levels in two groups before treatment did not change significantly (P>0.05); 1 d after surgery, CD4+ and CD4+/CD8+ in two group patients were significantly lower than that before surgery (P<0.05), while CD8+ was higher than that before surgery, compared with the laparoscopic group, and the change index of patients in open group was more obvious; 3 d after surgery, the CD4+ and CD8+ levels in two patients was significantly lower than that of T1 (P<0.05) and CD4+/CD8+ were significantly higher than that of T1 (P<0.05). The CD4+ and CD4+/CD8+ levels in the open group patients were significantly lower than the laparoscopic group (P<0.05), while CD8+ was significantly higher than that in the laparoscopic group (P<0.05); 5 d after surgery, CD8+ level in the two groups patients was significantly lower than that of T3 (P<0.05), while CD4+ and CD4+/CD8+ were significantly higher than that of T3 (P<0.05). CD8+ was significantly higher than that in the laparoscopic group (P<0.05), while CD4+ and CD4+/CD8+ levels
Table 1
Comparison of blood coagulation function in two patients with gastric cancer after radical operation (x依s).
Group Time APTT (s) FIB (g/L) PLT (×109/L)
The laparoscopic group T0 35.24±4.11 4.66±1.26 244.39±12.13
T1 32.48±3.89*◇ 3.52±1.18*◇ 233.88±13.01*◇
T3 30.18±3.76*#◇ 4.53±1.14*#◇ 206.58±10.64*#◇
T5 31.88±3.91*#Δ◇ 5.87±1.35*#Δ◇
261.11±13.25*#Δ◇
The open group T0 35.40±4.06 4.72±1.35 245.03±13.19
T1 30.01±3.67* 2.91±1.00* 219.68±12.49*
T3 27.33±3.50*# 3.87±1.21*# 190.91±10.22*#
T5 29.44±4.03*#Δ 4.69±1.26*#Δ 244.36±11.84*#Δ
Compared with T0, *P<0.05; compared with T1, #P<0.05; compared with T3, ΔP<0.05; compared with the open group, ◇P<0.05.
Table 2
Comparison of cytokines in two patients with gastric cancer during perioperative period (x依s).
Group Time IL-6 (ng/mL) CRP (μg/L) TNF-alpha (ng/L)
The laparoscopic group T0 53.88±4.12 9.68±2.04 7.72±1.01
T1 67.14±4.36*◇ 40.49±8.63*◇ 5.76±0.74*◇
T3 63.29±4.10*#◇ 34.51±7.24*#◇ 6.41±0.83*#◇
T5 55.02±4.03*#Δ◇ 10.57±3.03*#Δ◇ 7.37±0.96*#Δ◇
The open group T0 53.64±4.08 9.81±2.13 7.81±1.06
T1 71.35±5.03* 46.15±7.99* 4.98±0.68*
T3 66.73±4.91*# 39.24±8.55*# 5.78±0.76*#
T5 60.67±4.44*#Δ 15.37±4.11*#Δ 6.59±0.88*#Δ
were significantly lower than the laparoscopic group, the data had significant difference (P<0.05) (Table 3).
4. Discussion
With the improvement of people's living standard and the change of diet structure, the incidence of gastric cancer is gradually increasing, and gastric cancer has become one of the highest incidence of malignant tumors in our country and the treatment of gastric cancer has become highly essential[4,5]. Surgery, chemotherapy and radiotherapy are three common methods of cancer treatment, because of the special nature cancer, the current treatment of cancer is still mainly based on surgery[6]. Laparoscopic surgery has the advantages of rapid recovery, less trauma and less complications, has been recognized and used by more and more medical workers, and has been praised by the majority of patients[7]. However, due to its own characteristics, it will cause some damage to the patients[8]. A variety of laparoscopic gastric cancer surgeries in invasive operation and abdominal incision will cause varying degrees of damage to the patients, such as ischemic reperfusion, increased oxidative stress, inflammatory response, as well as the complement system activation and immune function changes[9], which brought difficulties to the postoperative recovery of the patients and the cure of cancer[10]. Study of the coagulation function, cytokines and T lymphocyte changes of laparoscopic radical gastrectomy for gastric cancer patients during the perioperative period help to understand the effect of operation on the patient's physical function and how to improve the side effects, which is of great significance to the treatment of gastric cancer patients.
The study found that APTT and PLT levels of the two group gastric patients after radical resection decreased gradually, and the open group changes more obvious. 5 d postoperative, APTT and PLT levels increased, but the open group was lower than the laparoscopic group; 1 d after gastric cancer radical surgery, FIB levels of two groups of patients decreased, and then began to restore. Laparoscopic surgery is a minimally invasive surgery, which can reduce tissue exposure and damage degree, so as to effectively reduce the related factors such as ROS stress generated after the
operation, while the probability of the formation of a complex of clotting factor decreased[11]. FIB levels recovered rapidly, reducing the risk of thrombosis in patients after surgery. The rapid recovery of PT, APTT and PLT promotes blood coagulation function to achieve a normal state, which is conducive to the rapid arrival of the relevant therapeutic drugs to the lesion area, and promote the treatment of cancer and postoperative rehabilitation. The immune suppression caused by surgical trauma often cause the surgical infection and the metastasis of tumor cells. To explore the changes of immune function in patients with gastric cancer before and after laparoscopic radical gastrectomy is helpful to understand the clinical value of the treatment of cancer[12,13]. This study found that 3 d after the radical operation of gastric cancer, CD8+ and CD4+/CD8+ levels began to recover, and CD4+ level of the patients with gastric cancer began to recover postoperative 5 d. CD4+ T lymphocytes release IL-2, INF-alpha and other cellular immune response, CD8+ T lymphocytes release IL-4, IL-5 and others to participate in the humoral immune response, and the balance of CD4+/CD8+ directly reflect the body's immune response[14,15]. Fast recovery of T lymphocytes can effectively inhibit the recurrence and metastasis of gastric cancer and killing residual tumor cells, and can reduce the risk of infection, and speed up the rehabilitation of the operation and postoperative treatment of gastric cancer. Laparoscopic radical resection of gastric cancer caused damage to the body, leading to the occurrence of inflammatory reaction and the change of digestive function, which affected the rehabilitation of surgery and the treatment of cancer. This study found that 1 d after the radical operation of gastric cancer, IL-6 and CRP levels of two group patients were significantly elevated, then gradually decreased; TNF-alpha levels of the two group of patients significantly decreased, then gradually increased. TNF-alpha is an important inflammatory factor, which has an important anti-tumor effect[16], and the recovery of TNF-alpha after operation has achieved the goal of killing tumor cells to a certain extent. IL-6 and CRP are important inflammatory factors, their levels reflects the severity of trauma, and the raise of which can increases the incidence of complications and promote the transfer of cell[17,18]. Elevated levels of IL-6 and CRP after laparoscopic radical gastrectomy for gastric cancer can reduce the incidence of inflammatory reactions, reduce the incidence of complications and
Table 3
Comparison of T lymphocytes in two group patients with gastric cancer undergoing radical operation in perioperative period (x依s).
Group Time CD4+ (%) CD8+ (%) CD4+/CD8+
The laparoscopic group T0 12.33±2.04 3.43±0.57 3.42±0.81
T1 11.28±1.88*◇ 5.24±0.78*◇ 2.35±0.50*◇
T3 9.89±1.84*#◇ 4.56±0.61*#◇ 2.65±0.54*#◇
T5 11.65±2.00*#Δ◇ 3.97±0.59*#Δ◇ 3.11±0.64*#Δ◇
The open group T0 12.40±1.95 3.49±0.62 3.44±0.84
T1 10.13±1.42* 5.91±0.85* 1.98±0.46*
T3 9.26±1.52*# 5.21±0.77*# 2.32±0.38*#
T5 11.00±2.34*#Δ 4.40±0.62*#Δ 2.69±0.50*#Δ
prevent the further increase of cancer[19,20].
In summary, this study examined changes of the coagulation related indicators (PT, APTT, FIB and PLT), cytokines (IL-6, CRP, TNF-alpha) and T lymphocytes (CD4+, CD8+ and CD4+/ CD8+ ) levels of patients with gastric cancer of laparoscopic radical gastrectomy in different periods before and after operation, and to explore the clinical significance of related index changes to the treatment of cancer surgery and rehabilitation, and can provide important help for the implementation of laparoscopic radical gastrectomy of gastric cancer patients.
References
[1] Akre K, Ekström AM, Signorello LB, et al. Aspirin and risk for gastric cancer: a population-based case-control study in Sweden. Brit J Cancer 2015; 84(7): 965-968.
[2] Takahashi T, Nakajima K, Miyazaki Y, et al. Surgical strategy for the gastric gastrointestinal stromal tumors (GISTs) larger than 5 cm: laparoscopic surgery is feasible, safe, and oncologically acceptable. Surg
Laparo Endo Per 2015; 25(2): 875-878.
[3] Fernándezhevia M, Delgado S, Castells A, et al. Transanal total mesorectal excision in rectal cancer: short-term outcomes in comparison with laparoscopic surgery. Ann Thorac Surg 2015; 261(2): 221-227. [4] Chen XX. The nursing experience of the treatment of gastric cancer with
bone metastasis pain by the combination of zoledronic acid. Guizhou Med 2015; 39(5): 472-473.
[5] Zhuo QX, Huang JM, Sun JY. Analysis of diagnosis and treatment of elderly patients with gastric cancer over 80 years old. Pract Geriatr Med 2016; 30(2): 173-174.
[6] Ni Q, Ji A, Yin J, et al. Effects of two common polymorphisms rs2910164 in miR-146a and rs11614913 in miR-196a2 on gastric cancer susceptibility. Gastroent Res Pract 2015; 2015(6): 1-10.
[7] Park EJ, Cho MS, Baek SJ, et al. Long-term oncologic outcomes of robotic low anterior resection for rectal cancer: a comparative study with laparoscopic surgery. Ann Thorac Surg 2015; 261(1): 129-137.
[8] Boni L, David G, Mangano A, et al. Clinical applications of indocyanine green (ICG) enhanced fluorescence in laparoscopic surgery. Surg Endosc 2015; 29(7): 2046-2055.
[9] Singh RK, Saini AM, Goel N, et al. Major laparoscopic surgery under regional anesthesia: a prospective feasibility study. Med J Armed Forces
India 2015; 71(2): 126-131.
[10] Mike M, Kano N. Laparoscopic surgery for colon cancer: a review of the fascial composition of the abdominal cavity. SurgToday 2015; 45(2): 129-139.
[11] Zhao ZL, Fang Q, Wang YL. Effects of dexmedetomidine on the dosage of sevoflurane and serological indexes in laparoscopic surgery for gastric cancer. J Hainan Med Univ 2015; 21(3): 390-392.
[12] Liu B. The control study of preoperative arterial interventional chemotherapy and radical gastrectomy for the treatment of advanced gastric cancer. J Hainan Med Univ 2016; 22(2): 182-185.
[13] Mike M, Kano N. Laparoscopic surgery for colon cancer: a review of the fascial composition of the abdominal cavity. Surg Today 2015; 45(2): 129-139.
[14] Garrido MC, Riveiro-Falkenbach E, Ruano Y, et al. Primary cutaneous small/medium CD4+ T-cell lymphoma occurring during treatment with
vemurafenib for advanced melanoma. Am J Dermatopath 2015; 37(6): 440-443.
[15] Hoff C, Grau C, Overgaard J. Influence of lifelong cumulative HIV viremia on long-term recovery of CD4+ cell count and CD4+/CD8+ ratio
among patients on combination antiretroviral therapy. Aids 2015; 29(5): 595-607.
[16] Adachi T, Arito M, Suematsu N, et al. Roles of layilin in TNF-α-induced epithelial-mesenchymal transformation of renal tubular epithelial cells.
Biochem Bioph Res Co 2015; 467(1): 63-69.
[17] Taylor PR, Roy S, Leal SM, et al. Erratum: activation of neutrophils by autocrine IL-17A-IL-17RC interactions during fungal infection is regulated by IL-6, IL-23, RORγt and dectin-2. Nat Immunol 2015;
16(2): 214-214.
[18] Fong SW, Ling LF, Wei CST, et al. Systemic and coronary levels of CRP, MPO, sCD40L and PlGF in patients with coronary artery disease.
BMC Res Notes 2015; 8(1): 1-7.
[19] Gatehouse HS, Gatehouse LN, Malone LA, et al. Amylase activity in honey bee hypopharyngeal glands reduced by RNA interference. J
Apicult Res 2015; 43(1): 9-13.