This may be the author’s version of a work that was submitted/accepted for publication in the following source:
Tuzovic, Sven& Kuppelwieser, Volker (2016)
Developing a framework of service convenience in health care: An ex-ploratory study for a primary care provider.
Health Marketing Quarterly,33(2), pp. 127-148.
This file was downloaded from: https://eprints.qut.edu.au/95980/
c
Consult author(s) regarding copyright matters
This work is covered by copyright. Unless the document is being made available under a Creative Commons Licence, you must assume that re-use is limited to personal use and that permission from the copyright owner must be obtained for all other uses. If the docu-ment is available under a Creative Commons License (or other specified license) then refer to the Licence for details of permitted re-use. It is a condition of access that users recog-nise and abide by the legal requirements associated with these rights. If you believe that this work infringes copyright please provide details by email to [email protected]
Notice:Please note that this document may not be the Version of Record (i.e. published version) of the work. Author manuscript versions (as Sub-mitted for peer review or as Accepted for publication after peer review) can be identified by an absence of publisher branding and/or typeset appear-ance. If there is any doubt, please refer to the published source.
2 DEVELOPING A FRAMEWORK OF SERVICE CONVENIENCE IN HEALTH
CARE: AN EXPLORATORY STUDY FOR A PRIMARY CARE PROVIDER
ABSTRACT
From retail health clinics and online appointment scheduling to (mobile) kiosks that enable
patient check-in and automate the collection of co-pays and open balances – convenience has
become an important topic in the health care sector over the last few years. While service
convenience has also gained much interest in academia, one common limitation is that authors
have adopted a “goods-centered” perspective focusing primarily on retail settings. Results of
this exploratory study reveal that health care service convenience encompasses seven different
dimensions: decision, access, scheduling, registration & check-in, transaction, care delivery,
and post-consultation convenience. Implications and future research suggestions are
discussed.
INTRODUCTION
Due to technological advances and changing consumer preferences, service convenience has
received growing attention in the last few years. As consumers increasingly desire more
convenience in service exchanges (Seiders, Voss, Godfrey, & Grewal, 2007), service
providers have tried to meet the rising convenience demands by providing new
technology-based self-service delivery options, ranging from check-in kiosks at airports, in-room hotel
checkout, self-scanning technology in supermarkets to Internet shopping (Dabholkar, Bobbitt,
& Eun-Ju, 2003).
In academia, service convenience has also gained much interest recently. Previous
research has identified convenience as a key motive of shopping both offline and online (e.g.,
Christodoulides & Michaelidou, 2011; Rohm & Swaminathan, 2004). Several scholars have
3 link convenience to customer satisfaction (Aagja et al. 2011; Berry et al. 2002; Colwell et al.
2008; Seiders et al. 2007). However, one common limitation is that authors have adopted a
“goods-centered” perspective that is based on the stages of the consumer buying process
focusing only on retail settings.1
People-processing services (Lovelock & Wirtz, 2010) which
are characterized with high levels of credence attributes (e.g., health care) have not found
their way into the service convenience literature so far. Furthermore, the majority of existing
research only has considered convenience within one channel (i.e., the “bricks and mortar”
retail outlet); yet, as consumers are increasingly using the Web and/or Apps to search online
for product information and/or to make purchases, the question arises how convenience is
perceived across multiple channels.
To fill this gap, the purpose of this paper is to investigate service convenience in the
context of credence-based services. Specifically, this paper focuses on health care services,
which are “radically different from ordinary services, e.g. fast moving consumer goods.”
(Lanseng & Andreassen, 2007, p. 395). Over the last few years, convenience has become an
important topic in the health care sector. Zainuddin, Previte, and Russell-Bennett (2011, p.
371) define convenience in their study on value creation in health care as “the facilitation of
the desired behaviour through the implementation of relevant processes and structures” which
includes convenient location of service centers, useful facilities such as parking, and other
helpful services such as courtesy phone call reminders.” With the rise of the Internet,
technology has become a significant driver to increase convenience for patients as well. For
example, many health care organizations have launched e-health services (e.g., Huang &
Chang, 2012) and ‘patient portals’ that allow patients to access their electronic health records.
As more and more consumers become accustomed to using smartphones and other small
1
One noteworthy exception is the qualitative work by Geissler, Rucks, and Edison (2006) who conducted focus
4 portable devices such as tablets, portals now ‘go mobile’ allowing patients to access their
personal health information via special Apps (Shaw, 2011). And as smartphones and iPads are
changing the way consumers connect and communicate, so are electronic medical records
replacing paper in doctor’s offices (Ayot, 2012). More and more patients now are being
greeted with kiosks or ‘health tablets’ as they check-in for appointments.
The results of this study reveal that health care service convenience encompasses
seven different dimensions: decision, access, scheduling, registration & check-in, transaction,
care delivery, and post-consultation convenience. In addition, usefulness, ease of use and
assurance factors of self-service technology are important side factors that have an influence
on its general use, and ultimately on patients’ perceived convenience with the
registration/check-in and transaction encounters.
This study provides important contributions for the domain of convenience research.
First, our study takes an important step toward advancing the understanding of the service
convenience construct as it changes from a “goods-centered” perspective to a “service
encounter-oriented” view. Specifically, we suggest that previous conceptualizations (Berry,
Seiders, & Grewal, 2002; Seiders et al., 2007) are not universally applicable in a health care
context. Credence-based health care services are more complicated due to (1) a high level of
information asymmetry between the buyer (patient) and seller (health care provider), (2) a
high consumer involvement combined with a high level of emotional vulnerability, and (3)
the fact that consumers seek health care services as a means to achieve good health (Dobele &
Lindgreen, 2011). Second, our study integrates service convenience research with the
technology acceptance model (TAM) literature (e.g., Wu, Zhao, Zhu, Tan, & Zheng, 2011).
As providers have increasingly implemented (mobile) self-service technology (SST) during
the service encounter, our findings suggest that the adoption of mobile SST in health care can
5 Since convenience is considered to have an influence on satisfaction and behavioral
intentions (e.g., Aagja, Mammen, & Saraswat, 2011), the results have practical implications
for health care managers as well. That is, the findings allow health care managers to diagnose
gaps in health care convenience and improve the organizational service design. Health care
practitioners can use the results of patients’ convenience perceptions during the consultation
process to evaluate redundancies in the backstage and improve the clinical workflow.
This paper begins by reviewing the existing literature on service convenience. Next,
the authors present the research design and methodology. This is followed by a discussion of
the findings of in-depth interviews with patients and health care experts. The paper concludes
with implications for research and practitioners, limitations and future directions.
LITERATURE REVIEW
The construct of convenience itself is not new to literature. Aagja et al. (2011) point out that
the notion of convenience dates back to an article in the 1920s in the Harvard Business
Review in which Copeland (1923) defines convenience goods as those customarily purchased
at easily accessible stores. More recently, service convenience has been defined as
“consumers’ time and effort perceptions related to buying or using a service” (Berry et al.
2002, p. 4). Consequently, when retailers start to offer ways for convenient shopping to
customers, they are saving the customers’ time or effort in the service encounter and thereby
increase the value of their market offer (Colwell, Aung, Kanetkar, & Holden, 2008).
Several scholars have made attempts to conceptualize the convenience construct (e.g.,
Berry et al., 2002; Brown, 1989, 1990) and develop a measurement scale (Colwell et al.,
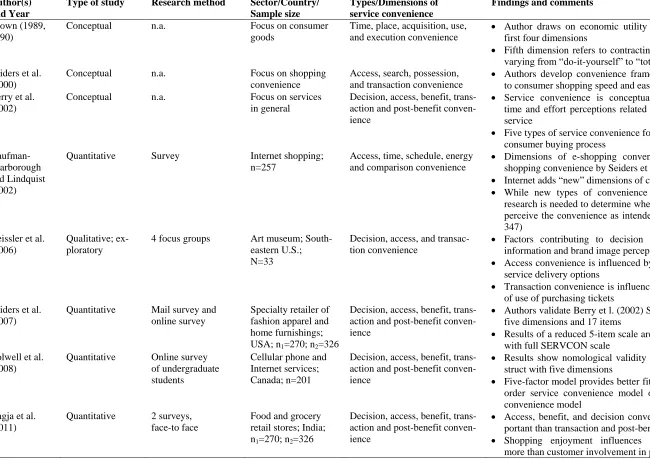
2008; Seiders et al., 2007). Table 1 lists a summary of the existing literature on service
convenience. Recently, Aagja et al. (2011) suggest exploratory research to better understand
the nuances of service convenience as well as other service settings and locations.
6 RESEARCH DESIGN AND METHOD
Research setting
The health care sector has been one of the fastest growing sectors in the service economy
(Andaleeb, 2001; Dagger, Sweeney, & Johnson, 2007), and is considered to be a “fertile field
of service research” (Berry & Bendapudi, 2007). For a number of reasons, health care services
are considered to be “radically different from ordinary services, e.g. fast moving consumer
goods.” (Lanseng & Andreassen, 2007). For example, health care services are characterized
by a high level of information asymmetry between the buyer (patient) and seller (health care
provider). Despite low expertise, a patient has to trust the health professional with his/her life,
which suggests high consumer involvement combined with a high degree of emotional
vulnerability (Dobele & Lindgreen, 2011).
As health organizations respond to higher consumer expectations and tighter budgets,
many are looking to (mobile) self-service technologies (SSTs) as a way to improve efficiency
and satisfaction (Rhoads & Drazen, 2009). SSTs are defined as technological interfaces that
allow customers to produce services independent of direct service employee involvement
(Cunningham, Young, & Gerlach, 2008; Meuter, Ostrom, Roundtree, & Bitner, 2000). In
health care, SSTs can come in three main types (Rhoads & Drazen, 2009): they can be
freestanding kiosks (like those at the airport), countertop and wall-mounted kiosks (like bank
ATMs), or they can be mobile kiosks (tablet PC, also referred to as health tablets). Most of
these kiosks are now being used to enable patient check-in, to collect patients’ demographic,
clinical and billing information (e.g., Phreesia.com), and to automate the collection of co-pays
and open balances. Considering the growing demand for health care services, changing
consumer preferences and increased competition from large retail stores or chain drug stores
(Fox, 2011), health care organizations have to understand the many facets of service
7 Data collection
This paper is guided by an interpretative research approach (Beckmann & Elliott, 2000;
Dobele & Lindgreen, 2011; Zainuddin et al., 2011) and utilizes qualitative methods to explore
patients’ perceptions of convenience (Geissler et al., 2006). A qualitative research approach
was chosen because of the exploratory nature of the study. Currently, there are only a few
empirical studies that have operationalized the construct service convenience; yet none of
those have considered credence-based services. The depth interview methodology was used to
understand how patients perceive convenience when they are in the need of a health care
provider, including the three stages of pre-visit, visit (i.e., physical service encounter) and
post-visit. The depth interview, “a method that has been increasingly used in the theory
development process in other areas of marketing” (Gwinner, Gremler, & Bitner, 1998, p.
103), was expected to be helpful in discovering factors not addressed in previous service
convenience research.
Working together with a local family practice with multiple locations in the Pacific
Northwest, 14 patients were recruited to participate in the research study. Because of strict
privacy guidelines in the health care sector, e.g. HIPAA (Health Insurance Portability and
Accountability Act), the marketing department of the family practice was responsible for
contacting prospective respondents. Purposeful sampling was chosen as the objective was to
(1) have a group of participants that had used the family practice’s Phreesia tablet at least
once during a visit within the last six months (i.e., they had experience with mobile
self-service technology) and (2) maximize diversity with regard to age, gender, and years as
patient. Telephone interviewing was chosen rather than face-to-face interviews. Although
telephone interviewing has been used less often than face-to-face interviews in qualitative
research (Novick, 2008; Opdenakker, 2006), several scholars point out that telephone
8 2001; Musselwhite, Cuff, McGregor, & King, 2007; Sweet, 2002). Although literature has
raised concerns about the quality of data obtained over the telephone and its comparability
with face-to-face interviews (Sykes & Hoinville, 1985), there is little evidence showing
significant differences (Novick, 2008; Smith, 2005). In the present context, telephone
interviews appeared to be more suitable than the alternatives of interviewing patients either at
home or at the time of their doctor’s visit for several reasons. Telephones allow participants to
remain on “their own turf” (McCoyd & Kerson, 2006, p. 399), permit more anonymity
(Sweet, 2002; Tausig & Freeman, 1988) and privacy (Sturges & Hanrahan, 2004), and they
take less time to undertake leading to greater acceptability among interviewees (Smith, 2005).
All interviews took place during one week in spring 2012. The duration of phone
interviews with patients varied from 15 to 20 minutes. Additional information was expected
to be gained from discussion with health care experts due to their long, practical experience in
the field of health care and as a provider of health services (see Hadwich, Georgi, Tuzovic,
Büttner, & Bruhn, 2010). As such, three personal depth interviews were conducted with a
marketing director of a local private, nonprofit health care organization that includes six
hospitals and more than 100 primary-care and specialty-care medical clinics, as well as two
family physicians who are Residence Faculty at a local Army Medical Center. These
interviews lasted 25 to 35 minutes. All interviews were semi-structured, that is, a list of
questions was used as a guide (see Appendix). It has to be noted that the sample is skewed as
85 percent were female. The average age was 43 years, with the youngest person being 26 and
the oldest person being 63 years old. The average time as patient was about six years. Most of
the participants have used the family practice’s tablet twice as a patient.
Data analysis
All interviews were audiotaped and transcribed to further facilitate the analysis, resulting in
9 MAXQDA, a software package designed for coding qualitative data. A content analysis was
then conducted to extract meaning from the text (Weber 1983). The reliability of the results
was enhanced by documenting the empirical research process thoroughly (Hadwich et al.,
2010; Tuzovic, 2009). The coding structure was developed in the context of critical
discussion and reflection with colleagues involved in marketing research. First, all interviews
were read to gain a holistic view of the data. Next, the author compared comments about
convenience to search for common elements and themes. Ward and Ostrom (2006) refer to
this procedure as “intratext cycle” and “intertext cycle”. External validity was enhanced by
drawing analytical conclusions based on the literature review. To enhance construct validity,
the same general structure was used for all interviews.
RESULTS OF THE QUALITATIVE INTERVIEWS WITH PATIENTS
Pre-encounter convenience
The discussion with patients reveals two main themes that explain service convenience in
health care at the pre-encounter stage.
Access convenience: Participants were asked: “What does convenient service in health
care mean?” Patients did not use the term “access” but referred to several components of
physical accessibility, in particular factors such as hours of operation location, parking, and
directions. The Appendix includes examples for the factor physical accessibility. Another
important component of access refers to the availability of access channels offered to patients.
Most patients preferred to have the ability to go online. However, others were satisfied using
the phone (see Appendix):
Scheduling convenience: A second theme that emerged relates to “scheduling
convenience”. According to Gupta and Denton (2008), appointment scheduling systems “lie
at the intersection of efficiency and timely access to health services” and can be a source of
10 as soon as possible, but patients with an appointment expect to be seen at a short notice
(Joustra et al., 2010). Patients in this study commented in particular on the availability of
appointment slots and the timeliness of appointment scheduling (see Appendix). The second
important factor that appears to influence scheduling convenience relates to the pre-encounter
communication between the patient and the health care provider. That is, patients expect that
their phone calls are returned in a timely manner. They consider it as inconvenient if they
speak to someone who cannot help them.
Convenience during the service encounter
Patients were asked to think about (1) the check-in and registration process and (2) the
transaction stage (e.g. making payments), and how health care providers could improve the
perceived convenience for patients. The discussion reveals that convenience of the
check-in/registration and transaction is interrelated with the benefits and usefulness of the provider’s
self-service application, such as a health tablet.
Registration/check-in convenience: Several patients expressed that this stage of the
service encounter should be quick and efficient. Comments include: “I would like my
check-in to be easy and quick” (Patient 2); “And that once I get there I’ll be checked-check-in quickly”
(Patient 3). So while the speed of registration can be considered as one factor, another factor
relates to efficient administration. According to the literature, administrative service elements
facilitate the production of a core service while adding value to a customer’s use of the
service (Dagger et al., 2007; Grönroos, 1990). This includes that the staff coordinates and
organizes medical care efficiently. For example, one patient commented: “I would say a
minimum wait time when you check in of five minutes and efficient enough to where they’re
verifying everything ensuring date of birth and verifying who you are” (Patient 10). Patients
seem to feel inconvenient when having to answer too many questions, in particular if they do
11 Transaction convenience: In a retailing context transaction convenience refers to
consumers’ perceived expenditures of time and energy to complete the purchase transaction.
In the case of health care the transaction stage is different. Patients usually have to make
payments before the actual consultation with the physician and medical staff. In addition,
several issues can increase the complexity for patients when it comes to billing, for example,
different kind of health plans, the difference between co-payments and outstanding balances,
and in-network versus out-of-network expenses. One important sub-theme that appears to
have an influence on transaction convenience is the accuracy of the billing and payment data.
Patients expressed that they need to have accurate information about their obligations.
Convenience in the transaction experience thus can be interpreted as avoiding billing surprises
for patients.
Convenience of SST use: Drawing on the technology acceptance model (TAM)
(Davis, 1989; Davis, Bagozzi, & Warshaw, 1989) and recent amended versions such as
Venkatesh, Morris, Davis, and Davis (2003) Unified Theory of Acceptance and Use of
Technology (UTAUT), a large number of studies has provided empirical support for the
determinant roles of usefulness and ease of use in the adoption and acceptance of
technology/SSTs. Usefulness refers to the benefits customers associate with using the SSTs
(Weijters, Rangarajan, Falk, & Schillewaert, 2007). Futhermore, in the context of
self-services, usefulness of a self-service application can be interpreted as the expected
convenience reflecting the consumers’ interest in reducing time, effort, and money (Lanseng
& Andreassen, 2007).
In the present study, patients referred to various aspects of convenience of using the
provider’s health tablet, including saving time for the check-in process, being more
independent in using the tablet at their pace, or making less errors in filling out the
12 payments with the health tablet, the discussion resulted in additional factors that influence
patients’ use of SSTs. These factors can be summarized under the term assurance and include
the device’s reliability, privacy and confidentiality issues, system integration, and the need for
staff assistance for novice users (see Appendix). This is in line with previous research on the
acceptance of mobile payment systems. For example, Meharia (2012) concludes that security,
privacy, confidentiality, processing integrity and availability are important factors associated
with consumer acceptance of mobile payment services. Experts added an interesting facet that
the patients did not mention, that is, the assurance of cleanliness. In other words, the context
of health care adds more requirements for safety standards to the implementation of SSTs and
patients’ trust beliefs about the provider and the device (i.e., its reliability, safety, etc.) are an
important determinant of SST use.
In this study, respondents viewed the convenience of transactions via health tablet
ambivalent. One the one hand, they perceived it as beneficial and some of the patients
appreciated the ease of use of making payments. On the other hand, the majority did not like
to lose control over their payment modus (see Appendix). This suggests that perceived control
of the payment modus appears to be an important factor for the perception of transaction
convenience.
Care delivery convenience: Previous research has identified benefit convenience as a
dimension of service convenience which is strongly related to the core service provision and
is defined as “consumers’ perceived time and effort expenditures to experience the service’s
core benefits” (Berry et al., 2002, p. 7). In the health care sector, benefit translates into the
clinical care and the quality that a patient receives during the examination and consultation.
Various studies have investigated quality factors in health care (e.g., Carlucci, Renna, &
Schiuma, 2013; Dagger et al., 2007; Wang, Huang, & Howng, 2011). The discussion with
13 relates to the timely delivery of clinical care. Patients expressed that health care should be
provided quickly and efficiently, that is, being able to see the doctor in a reasonable amount
of time. This also includes avoiding redundancies, such as having to answer repetitive
questions during the consultation, or inefficient clinical workflows (see Appendix).
Furthermore, patients expressed unanimously the importance of “psychological care” (Liu,
Amendah, En-Chung, & Lai Kwan, 2006) which encompasses aspects such as the doctor’s
empathy and attentiveness. So while patients do not like wait times, they perceive spending
more time with their doctor as a sign of “good care” (see Appendix).
Post-encounter convenience
Previous research has referred to post-benefit convenience in the context of retailing (Berry et
al., 2002). In this study, participants referred to the follow-up communication, for example,
receiving lab results via email. Convenience thus means to reduce patients’ perceived time
and effort after their visit. This includes receiving follow-up communication in a timely
manner (see Appendix).
RESULTS OF THE QUALITATIVE INTERVIEWS WITH EXPERTS
The purpose of the expert interviews was to gain additional information and to evaluate the
dimensions that resulted from the qualitative analysis of the patient responses. The feedback
of the experts was mostly congruent with the answers of the patients. For example, the experts
agreed with patients that easy scheduling influences perceived convenience (“I think a lot of
times what patients perceive as convenient is that they can get the appointment that they want
at the time that they wanted,” Expert 3). In several cases, the experts communicated factors of
service convenience more holistically than patients resulting in additional sub-themes as well
as one more main theme. First, with regard to the theme of access the practitioners had a more
differentiated view on accessibility. That is, beyond the factors mentioned by patients, easy
14 Regarding access channels, the feedback from the experts was also more
substantiated. For example, one expert suggested that multiple channels should be offered to
patients (“I think it’s making choices available is what helps give that convenience”). That is,
having choices on how to contact the service provider (e.g. email, online, by phone, in person)
provides convenience. Some health care providers also acknowledge that interacting with
health care providers has to become equally convenient as shopping online. While patients
only refer to the “space” dimension of access, the discussion with the experts also generated a
different view, which can be summoned as “time” dimension of access. That is, convenience
means to have flexible access to the service provider. For example, customers may want to
use their iPad in the middle of the night to schedule a physical, check the availability, or make
a payment (see Appendix for exemplary statements of experts).
Interesting insights were gathered from the experts regarding the pre-encounter
communication. As the practitioners point out the communication does not have to be with the
physician as long as someone is acknowledging the patient’s needs, i.e. someone is responsive
to the patient’s inquiry. Besides reactive communication, experts pointed out the importance
of active communication, including courtesy phone call reminders or rescheduling the
appointment quickly (see Appendix).
Decision-making convenience: One new theme emerged during the discussion with
the practitioners. While the literature review suggests that decision convenience is a
dimension of service convenience, the discussion with patients did not generate much insight
in the context of health care services. Only one patient mentioned explicitly the importance of
information, for example, online descriptions about physicians and the facility or ratings that
indicate the level of quality (see Appendix). For example, Gressel (2013, p. 247) argues that
the “difficulty of accessing and understanding relevant health care quality information
15 they will feel an increased level of convenience. However, the discussion with the experts
yielded further insights regarding the theme of decision-making convenience. It appears that
beyond the scope of providing patients with static information, convenience also is related to
providing patients with relevant tools and services for assessing a person’s medical needs.
The health care practitioners mentioned features that would enable patients to assess their
own medical need. This could vary from nurse consultations on the phone to online
consultations via webcam. Other options are e-health services which allow patients to conduct
their own health screening. For example, Huang and Chang (2012) list a number of interactive
tools found on U.S. hospital websites. The result would be a decision tree that tells patients if
they should then contact their health provider for an appointment (see Appendix).
Post-consultation convenience: Finally, practitioners had a more differentiated view on
the post-consultation encounter. It appears that in the situation of health care services one has
to distinguish two stages: (1) immediate medical support services after the consultation with
the physician such as follow-up schedule, prescriptions, lab services, or pharmacy and (2) the
post-encounter stage, referring to follow-up communication, for example, sending patients
their lab results, giving instructions or referrals to another doctor (see Appendix for
exemplary statements from experts).
PROPOSED FRAMEWORK OF HEALTH CARE SERVIVCE CONVENIENCE
A conceptual model of health care service convenience is proposed (see Figure 1). Based on
existing service convenience literature and the findings from the exploratory study, the
proposed model indicates that service convenience in health care is an abstract construct that
can be described by seven dimensions: decision, access, scheduling, registration & check-in,
transaction, care delivery, and post-consultation convenience. In addition, within the service
16 important side factors that have an influence on its general use, and ultimately on patients’
perceived convenience with the registration/check-in and transaction encounters.
Insert Figure 1 about here
DISCUSSION AND IMPLICATIONS
Implications for service convenience theory
Services differ based on their search, experience and credence qualities. This research seeks to
clarify the concept of service convenience in the context of credence services, such as health
care. Applying a service-encounter perspective of the service purchasing process (Lovelock &
Wirtz, 2010; Zeithaml, Bitner, & Gremler, 2013) the study expands the existing knowledge of
service convenience which is mainly focused on goods and retailing and offers new insight
how convenience is perceived by patients during the pre-encounter, service encounter and
post-encounter stages.
The study supports previous work about the dimension of access convenience (e.g.,
Berry et al., 2002; Geissler et al., 2006; Seiders, Berry, & Gresham, 2000). Physical access
appears to be a key factor for convenience, no matter if the setting is retailing or a credence
service. Decision convenience was also identified in the present study as a dimension,
supporting the SERVCON scale. Here service researchers should address the question if the
role of decision convenience might differ for more tangible services versus services with
experience or credence attributes. We posit that due to the lack of search attributes in health
care, tangible cues become even more important in the context of decision convenience. Thus,
health care providers should enhance the information and e-health services to increase
decision convenience for patients. Transaction convenience can be also considered as a
relevant dimension in the case of credence services, supporting the existing SERVCON scale
as well as findings by Geissler et al. (2006) in the context of experience services. Service
17 al.’s (2002) conceptualization assumes that the transaction (i.e. payment) follows the benefit
(i.e. shopping). However, in many service settings the transaction happens before the
consumption of the service. For instance, patients in health care may have to pay a
co-payment before their doctor visit, the actual benefit or consumption of the service. The
question arises if each dimension has a different impact on the overall perceived convenience
depending on which comes first, the service consumption or the payment.
This study also identified new convenience dimensions that have not been captured in
prior research. Most notably, scheduling convenience and registration/check-in convenience
are facets of convenience that may have a strong influence on customer satisfaction. Since
many services rely on reservations and appointment scheduling, service researchers may want
to investigate if there are similarities in other people-processing services (e.g., restaurants,
hotels, physical therapy), or even with possession-processing services such as laundry and dry
cleaning or car repair services.
Finally, the role of self-service technology convenience needs to be further explored.
Even though self-service technology has become increasingly important for businesses,
previous research has ignored its role in the context of convenience. While a separate research
stream on the TAM model has investigated numerous aspects of the adoption of (mobile)
self-service technology in various types of contexts, self-service researchers need to further investigate
how factors such as ease of use, assurance, privacy, trust or external factors influence
self-service technology convenience and its interrelationships with self-service quality and customer
satisfaction. This study is the first that suggests recognizing self-service technology
convenience as a determinant of two convenience dimensions during the service encounter,
hoping to stimulate further research to test these assumptions in a larger quantitative study.
18 This study makes important contributions to health care practitioners and policy makers. First,
the framework facilitates a greater appreciation of the convenience factors that patients seek
during the pre-encounter stage. Access convenience, in particular, is an important area that
needs to be acknowledged by health care practitioners. Recent reports indicate that more and
more Americans are using retail health clinics (RHCs) located in large retail stores (e.g.,
Walmart, Kroger) or chain drug stores (e.g., CVS, Walgreen’s) to take care of minor health
needs (Fox, 2011; Williams, Khanfar, Harrington, & Loudon, 2011). Major hospitals have
been adding clinics in retail areas in order to meet patients where they live and work (Howell,
2012). For example, the Mayo Clinic has opened a location inside Minnesota’s Mall of
America. Thus, health care organizations that want to adapt to people’s changing needs have
to increase access convenience for patients (for example, availability of parking, directions,
and multiple channels to contact the clinic).
Second, health care managers can use the findings for improving the organizational
service design. For example, clinic directors have recognized that patients’ perceptions of
urgency or need are an important factor in determining their overall satisfaction with the
timeliness of access (Gupta & Denton, 2008). Bhandari and Snowdon (2012) argue that
efficient and timely access to health care services has a profound impact on the well-being of
individuals. The authors suggest that from a design perspective it is important to understand
the interaction of channels (i.e. phone, website, walk-in clinics) in health care. Since making
appointments online is considered convenient, health care managers should invest in such
technology. For example, a growing number of hospitals now use InQuicker, an online
waiting service for emergency rooms and urgent care center patients (PRWeb, 2012).
Third, in deciding whether and how to implement SSTs, health care practitioners can
use the framework as a diagnostic tool. As interest in SSTs has been growing rapidly to
19 succeeded, either because of a lack of interest on the part of patients to use it or the SSTs are
not integrated with existing systems diminishing the overall benefit (Rhoads & Drazen, 2009).
Health care practitioners can use the results of patients’ convenience perceptions during the
service encounter stage to evaluate user acceptance at the front stage as well as redundancies
in the backstage and improve the clinical workflow (“Much of that comes back to
documentation – so redundancy of documentation. […] Wouldn’t it be great if you had a way
or system for your medical assistant to when this patient gets asked that question, they just
document it once and now it shows up automatically on your screens so you don’t have to ask
them those questions.” Expert 1).
RESEARCH LIMITATIONS AND FUTURE RESEARCH
As with any study, this research has some limitations that provide directions for future
research. First, due to the nature and design of this study, its findings cannot be generalized to
other health care organizations or other service industries. With regard to other health care
organizations, the conditions can vary by location, size and type of the health service (i.e.
primary care, specialty care, hospital services). While the current study was conducted in
collaboration with a primary care organization, patients of large hospitals or in the need of
specialty care may have different perceptions of health care convenience.
Second, the sample is potentially biased. Since the large majority were females, future
research should consider having a balanced sample with regard to gender. Furthermore, all
respondents had used the family practice’s tablet. Nonusers were not included in the sample.
Thus, an avenue for future research is to compare users versus nonusers along the seven
convenience dimensions.
REFERENCES
20 Andaleeb, Syed Saad. (2001). Service quality perceptions and patient satisfaction: a study of
hospitals in a developing country. Social Science & Medicine, 52(9), 1359-1370. doi: http://dx.doi.org/10.1016/S0277-9536(00)00235-5
Ayot, Herina. (2012, 23 March 2012). Health Tablets in the Waiting Room Revolutionizing
Telemedicine. Retrieved 10 January, 2013, from
http://healthworkscollective.com/herinaayot/30507/health-tablets-waiting-room-revolutionizing-telemedicine
Beckmann, Suzanne C., & Elliott, Richard H. (Eds.). (2000). Interpretive consumer research: Paradigms, methodologies, and applications. Copenhagen: Copenhagen Business School.
Berry, Leonard L., & Bendapudi, Neeli. (2007). A Fertile Field for Service Research. Journal of Service Research, 10(2), 111-122. doi: 10.1177/1094670507306682
Berry, Leonard L., Seiders, Kathleen, & Grewal, Dhruv. (2002). Understanding Service Convenience. Journal of Marketing, 66(3), 1-17.
Bhandari, Gokul, & Snowdon, Anne. (2012). Design of a patient-centric, service-oriented health care navigation system for a local health integration network. Behaviour & Information Technology, 31(3), 275-285. doi: 10.1080/0144929X.2011.563798
Brown, Lew G. (1989). The Strategic and Tactical Implications of Convenience in Consumer Product Marketing. Journal of Consumer Marketing, 6(3), 13.
Brown, Lew G. (1990). Convenience in Services Marketing. Journal of Services Marketing, 4(1), 53.
Carlucci, Daniela, Renna, Paolo, & Schiuma, Giovanni. (2013). Evaluating service quality dimensions as antecedents to outpatient satisfaction using back propagation neural network. Health Care Management Science, 16(1), 37-44. doi: 10.1007/s10729-012-9211-1
Carr, Eloise C. J., & Worth, Allison. (2001). The use of the telephone interview for research. NT Research, 6(1), 511-525.
Christodoulides, George, & Michaelidou, Nina. (2011). Shopping motives as antecedents of e-satisfaction and e-loyalty. Journal of Marketing Management, 27(1/2), 181-197. doi: 10.1080/0267257X.2010.489815
Colwell, Scott R., Aung, May, Kanetkar, Vinay, & Holden, Alison L. (2008). Toward a measure of service convenience: multiple-item scale development and empirical test. Journal of Services Marketing, 22(2), 160-169. doi: 10.1108/08876040810862895 Copeland, Melvin T. (1923). Relation of Consumer's Buying Habits to Marketing Methods.
Harvard Business Review, 1(3), 282-289.
Cunningham, Lawrence F., Young, Clifford E., & Gerlach, James H. (2008). Consumer views of self-service technologies. Service Industries Journal, 28(6), 719-732. doi: 10.1080/02642060801988522
Dabholkar, Pratibha A., Bobbitt, L. Michelle, & Eun-Ju, Lee. (2003). Understanding consumer motivation and behavior related to self-scanning in retailing. International Journal of Service Industry Management, 14(1), 59.
Dagger, Tracey S., Sweeney, Jillian C., & Johnson, Lester W. (2007). A Hierarchical Model of Health Service Quality: Scale Development and Investigation of an Integrated Model. Journal of Service Research, 10(2), 123-142. doi: 10.1177/1094670507309594 Davis, Fred D. (1989). Perceived Usefulness, Perceived Ease of Use, and User Acceptance of
Information Technology. MIS Quarterly, 13(3), 319-340.
Davis, Fred D., Bagozzi, Richard P., & Warshaw, Paul R. (1989). User Acceptance of Computer Technology: A Comparison of two Theoretical Models. Management Science, 35(8), 982-1003.
Dobele, Angela, & Lindgreen, Adam. (2011). Exploring the nature of value in the word-of-mouth referral equation for health care. Journal of Marketing Management, 27(3/4), 269-290. doi: 10.1080/0267257X.2011.545677
Fox, Maggie. (2011, 22 November 2011). Study: Retail Clinics Gaining in Popularity. from http://www.nationaljournal.com/healthcare/study-retail-clinics-gaining-in-popularity-20111122
21 Gressel, Justin W. (2013). Development of a Quality Ranking Model for Home Health Care
Providers. Health Marketing Quarterly, 30(3), 246-262. doi: 10.1080/07359683.2013.814503
Grönroos, Christian. (1990). Service Management and Marketing: Managing the Moments of Truth in Service Competition. Lexington, MA: Lexington Books.
Gupta, Diwakar, & Denton, Brian. (2008). Appointment scheduling in health care: Challenges and opportunities. IIE Transactions, 40(9), 800-819. doi: 10.1080/07408170802165880
Gwinner, Kevin P., Gremler, Dwayne D., & Bitner, Mary Jo. (1998). Relational Benefits in Services Industries: The Customer's Perspective. Journal of the Academy of Marketing Science, 26(2), 101-114.
Hadwich, Karsten, Georgi, Dominik, Tuzovic, Sven, Büttner, Julia, & Bruhn, Manfred. (2010). Perceived quality of health services: A conceptual scale development of e-health service quality based on the C-OAR-SE approach. International Journal of
Pharmaceutical and Healthcare Marketing, 4(2), 112-136. doi:
10.1108/17506121011059740
Howell, Whitney L.J. (2012, 12 April 2012). Retail Health Clinics on the Rise. from http://www.porterresearch.com/Resource_Center/Blog_News/Industry_News/2012/A pril/Retail_Health_Clinics_on_the_Rise
Huang, Edgar, & Chang, Chiu-Chi Angela. (2012). Patient-Oriented Interactive E-health Tools on U.S. Hospital Web Sites. Health Marketing Quarterly, 29(4), 329-345. doi: 10.1080/07359683.2012.732871
Joustra, P. E., de Wit, J., Struben, V. M. D., Overbeek, B. J. H., Fockens, P., & Elkhuizen, S. G. (2010). Reducing access times for an endoscopy department by an iterative combination of computer simulation and Linear Programming. Health Care Management Science, 13(1), 17-26. doi: 10.1007/s10729-009-9105-z
Kaufman-Scarborough, Carol & Lindquist, Jay D. (2002). E-shopping in a multiple channel environment. The Journal of Consumer Marketing, 19(4), 333-350.
Lanseng, Even J., & Andreassen, Tor W. (2007). Electronic healthcare: a study of people's readiness and attitude toward performing self-diagnosis. International Journal of Service Industry Management, 18(4), 394-417. doi: 10.1108/09564230710778155 Liu, Sandra S., Amendah, Eklou, En-Chung, Chang, & Lai Kwan, Pei. (2006). Satisfaction
and Value: A Meta-Analysis in the Healthcare Context. Health Marketing Quarterly, 23(4), 49-73. doi: 10.1080/07359680802131566
Lovelock, C.H., & Wirtz, J. (2010). Services Marketing. People, Technology, Strategy (7th ed.). Upper Saddle River, NJ: Prentice-Hall.
McCoyd, Judith L. M., & Kerson, Toba Schwaber. (2006). Conducting intensive interviews using email: a serendipitous comparative opportunity. Qualitative Social Work, 5(3), 389-406.
Meharia, Priyanka. (2012). Assurance on the Reliability of Mobile Payment System and its Efects on it's Use: An Epirical Examination. Accounting & Management Information Systems / Contabilitate si Informatica de Gestiune, 11(1), 97-111.
Meuter, Matthew L., Ostrom, Amy L., Roundtree, Robert I., & Bitner, Mary Jo. (2000). Self-Service Technologies: Understanding Customer Satisfaction with Technology-Based Service Encounters. Journal of Marketing, 64(3), 50-64.
Musselwhite, Kimberly, Cuff, Laura, McGregor, Lisa, & King, Kathryn M. (2007). The telephone interview is an effective method of data collection in clinical nursing research: A discussion paper. International Journal of Nursing Studies, 44(6), 1064-1070. doi: http://dx.doi.org/10.1016/j.ijnurstu.2006.05.014
Novick, Gina. (2008). Is there a bias against telephone interviews in qualitative research? Research in Nursing & Health, 31(4), 391-398. doi: 10.1002/nur.20259
Opdenakker, Raymond. (2006). Advantages and Disadvantages of Four Interview Techniques in Qualitative Research (Vol. 7).
PRWeb. (2012, 12 September 2012). University Hospitals Emergency Room Visitors Can
Now Wait at Home with InQuicker. from
http://www.prweb.com/releases/2012/9/prweb9886919.htm
22 Rohm, Andrew J., & Swaminathan, Vanitha. (2004). A typology of online shoppers based on
shopping motivations. Journal of Business Research, 57(7), 748. doi: 10.1016/S0148-2963(02)00351-X
Seiders, Kathleen, Berry, Leonard L., & Gresham, Larry G. (2000). Attention, Retailers! How Convenient Is Your Convenience Strategy? Sloan Management Review, 41(3), 79-89. Seiders, Kathleen, Voss, Glenn B., Godfrey, Andrea L., & Grewal, Dhruv. (2007).
SERVCON: development and validation of a multidimensional service convenience scale. Journal of the Academy of Marketing Science, 35(1), 144-156. doi: 10.1007/s11747-006-0001-5
Shaw, Gienna. (2011, 16 March 2011). Patient Portals go Mobile. Retrieved 10 January, 2013, from http://www.healthleadersmedia.com/content/MAG-263728/Patient-Portals-go-Mobile
Smith, Elizabeth M. (2005). Telephone interviewing in healthcare research: a summary of the evidence. Nurse Researcher, 12(3), 32-41.
Sturges, Judith E., & Hanrahan, Kathleen J. (2004). Comparing telephone and face-to-face qualitative interviewing: A research note. Qualitative Research, 4(1), 107-118. doi: 10.1177/1468794104041110
Sweet, Linda. (2002). Telephone interviewing: is it compatible with interpretive phenomenological research? Contemporary Nurse, 12(1), 58-63.
Sykes, Wendy, & Hoinville, Gerald. (1985). Telephone Interviewing on a Survey of Social Attitudes: a Comparison With Face-to-Face Procedures. London: Social and Community Planning Research.
Tausig, Jane E., & Freeman, Ellen W. (1988). The next best thing to being there: conducting the clinical research interview by telephone. The American Journal Of Orthopsychiatry, 58(3), 418-427.
Tuzovic, Sven. (2009). Key determinants of real estate service quality among renters and buyers. Journal of Services Marketing, 23(7), 496-507. doi: 10.1108/08876040910995284
Venkatesh, Viswanath, Morris, Michael G., Davis, Gordon B., & Davis, Fred D. (2003). User Acceptance of Information Technology: Toward a Unified View. MIS Quarterly, 27(3), 425-478.
Wang, Hsiu-Ling, Huang, Jun-Ying, & Howng, Shen-Long. (2011). The effect on patient loyalty of service quality, patient visit experience and perceived switching costs: lessons from one Taiwan university hospital. Health Services Management Research, 24(1), 29-36. doi: 10.1258/hsmr.2010.010011
Ward, James C., & Ostrom, Amy L. (2006). Complaining to the Masses: The Role of Protest Framing in Customer-Created Complaint Web Sites. Journal of Consumer Research, 33(2), 220-230.
Weijters, Bert, Rangarajan, Devarajan, Falk, Tomas, & Schillewaert, Niels. (2007). Determinants and Outcomes of Customer's Use of Self-Service Technology in a Retail Setting. Journal of Service Research, 10(1), 3-21. doi: 10.1177/1094670507302990 Williams, Cheryl-Ann N., Khanfar, Nile M., Harrington, Catherine, & Loudon, David.
(2011). Marketing Retail Health Clinics: Challenges and Controversies Arising From a Health Care Innovation. Health Marketing Quarterly, 28(3), 270-285. doi: 10.1080/07359683.2011.595648
Wu, Kewen, Zhao, Yuxiang, Zhu, Qinghua, Tan, Xiaojie, & Zheng, Hua. (2011). A meta-analysis of the impact of trust on technology acceptance model: Investigation of moderating influence of subject and context type. International Journal of Information Management, 31(6), 572-581. doi: 10.1016/j.ijinfomgt.2011.03.004
Zainuddin, Nadia, Previte, Josephine, & Russell-Bennett, Rebekah. (2011). A social marketing approach to value creation in a well-women's health service. Journal of
Marketing Management, 27(3/4), 361-385. doi: 10.1080/0267257X.2011.547081
Zeithaml, Valarie A., Bitner, Mary Jo, & Gremler, Dwayne D. (2013). Services Marketing: Integrating Customer Focus across the Firm (6th ed.). New York: McGraw-Hill Irwin.
23 Themes and exemplary statements
Themes and sub-themes Exemplary statements Decision-making convenience
Information about facility and physicians
It took us a couple of years when we thought you know, let’s get online and check out [xyz] and it was really neat to be able to get on there actually and see all the doctor’s profiles which is what I’m just not used to doing. (…) Choosing a doctor is, I don’t want to say it’s scary but you want a good doc-tor and someone you might feel comfortable with and sometimes just seeing that person and just feeling that personality or just how they’re talking or -- I don’t know, that was very helpful to me actually. (Patient 7)
Tools and services for assessing one’s own medical needs
I think you have to educate your patients and some of that could potentially be achieved through – if they access the system online for instance, if there was kind of a menu-driven process that leads them through a decision tree to the point of where they needed to access care. (Expert 3)
Access convenience Physcial access (e.g. location, parking, operating hours, directions)
Coming to the clinic just as long as the directions from the office are clear. And also […] parking lot space. It always has really jam tight or just not properly made to which it’s harder to find a good parking spot. (Patient 1) I think that being open later until the evening like 7 or on the weekends till 7
or that type of thing. That would be important. (Patient 14) Availability of multiple
access channels (phone, online)
I call but I have done online too. It’s convenient both ways. (Patient 8) I make my appointments online […] and I really like that because it’s quick
and it’s more convenient for me than maybe having to call and be put on hold. (Patient 10)
Registration/check-in convenience Efficient administration
(e.g. redundancy of ques-tions)
I mean, yeah, it’s good probably for the doctor to know if there was some-thing else bothering you than what you’re there for the visit but to me it was too time consuming and I didn’t like all the questions. (Patient 8)
Timely appointment scheduling
And that I’ll be able to make appointments when necessary within a reasona-ble amount of time. (Patient 3)
Being able to see the doctor quickly. (Patient 9) Patient-provider
pre-encounter communication (both inbound and out-bound communication)
Convenience is having my calls returned in a timely manner or reaching who I want to speak to or need to speak to the same day. I think it’s quite incon-venient to call and leave a message and wait for a return, received a return call that I missed and I start to go through the same process again to call and leave a message on this automated system where I’m not speaking to a per-son. That’s very inconvenient so speaking to someone who can help me when I call. Or that if I’m calling them back, I can get to them. (Patient 14)
Transaction convenience
Accuracy of billing data They’ve looked at my coverage and have determined whether I need to [make] a co-pay or not depending on the nature of my visit and if I didn’t have that human interaction I might be paying that co-pay inappropriately. (Patient 11)
Control of payment modus It would probably not be convenient because I would want clarification as to why I have outstanding balance, I wouldn’t just pay it without questioning it. (Patient 9)
Care delivery convenience
Timely and efficient care Well, most important, like what is important to me, most important is the doctor be prompt, in other words, when I get there I check-in, I’m on time I would like the doctor to be on time too. (Patient 5)
Attentiveness of physician The thing I appreciated the most about my experience over there is the doctor that I see. She takes the time to listen to me, you know, she doesn’t rush me through (…) She takes the time to go over them with me to make sure I un-derstand the information so I don’t go home with a false idea. (Patient 4) Post-consultation convenience
Post-encounter communication
24 Yeah. I would just say making sure that contact with me is with in a timely
manner. (Patient 14)
Post-care support I look forward to the day that you could get home and there’s an email wait-ing for you with a summary, what you did or you lived with that information, maybe some patient teaching tools that are available and accompany that. (Expert 2)
Determinants and moderating factors influencing use of (mobile) kiosks
Self-efficiency That you do it at your own pace and that you know you’re pretty much independ-ent. You can just do the tablet and you don’t really have to wait for someone to be available to ask you the questions. (Patient 9)
Ease of use I think it was very easy; you just follow the instructions and then continue on next button; it’s pretty self-explanatory. (Patient 19)
Reliability I think it would be the reliability and the maintenance associated with keeping them reliable. (Expert 2)
Privacy I was helping that elderly lady fill hers out (…) she asked me to help her and I obviously was hearing the answers to her health questions. So, it wasn’t private at all because I was helping her to fill that out and I could see everything. (Patient 3) Cleanliness I think that is one of the factors that we’ll have to think about is not only keeping
them clean but our customers perceiving that they are clean. Infection control is very important inside a healthcare setting. (Expert 2)
Age When I was there I noticed there’s an elderly couple that was really frustrated with the system. (Patient 3)
25 Table 1: Literature review
Author(s) and Year
Type of study Research method Sector/Country/ Sample size
Types/Dimensions of service convenience
Findings and comments
Brown (1989, 1990)
Conceptual n.a. Focus on consumer
goods
Time, place, acquisition, use, and execution convenience
Author draws on economic utility theory to derive the first four dimensions
Fifth dimension refers to contracting out previous tasks, varying from “do-it-yourself” to “total convenience” Seiders et al.
(2000)
Conceptual n.a. Focus on shopping
convenience
Access, search, possession, and transaction convenience
Authors develop convenience framework that is related to consumer shopping speed and ease
Berry et al. (2002)
Conceptual n.a. Focus on services
in general
Decision, access, benefit, trans-action and post-benefit conven-ience
Service convenience is conceptualized as consumers’ time and effort perceptions related to buying or using a service
Five types of service convenience follow the stages of the consumer buying process
Kaufman-Scarborough and Lindquist (2002)
Quantitative Survey Internet shopping; n=257
Access, time, schedule, energy and comparison convenience
Dimensions of e-shopping convenience are based on shopping convenience by Seiders et al. (2000)
Internet adds “new” dimensions of convenience
While new types of convenience “bear face validity, research is needed to determine whether actual customers perceive the convenience as intended by the retailer” (p. 347)
Geissler et al. (2006)
Qualitative; ex-ploratory
4 focus groups Art museum; South-eastern U.S.; N=33
Decision, access, and transac-tion convenience
Factors contributing to decision convenience include information and brand image perceptions
Access convenience is influenced by physical access and service delivery options
Transaction convenience is influenced by speed and ease of use of purchasing tickets
Seiders et al. (2007)
Quantitative Mail survey and online survey
Specialty retailer of fashion apparel and home furnishings; USA; n1=270; n2=326
Decision, access, benefit, trans-action and post-benefit conven-ience
Authors validate Berry et l. (2002) SERVCON scale with five dimensions and 17 items
Results of a reduced 5-item scale are generally consistent with full SERVCON scale
Colwell et al. (2008)
Quantitative Online survey of undergraduate students
Cellular phone and Internet services; Canada; n=201
Decision, access, benefit, trans-action and post-benefit conven-ience
Results show nomological validity of second-order con-struct with five dimensions
Five-factor model provides better fit to data than second-order service convenience model or one-factor service convenience model
Aagja et al. (2011)
Quantitative 2 surveys, face-to face
Food and grocery retail stores; India; n1=270; n2=326
Decision, access, benefit, trans-action and post-benefit conven-ience
Access, benefit, and decision convenience are more im-portant than transaction and post-benefit convenience Shopping enjoyment influences service convenience
26 Figure 1: Model of health care service convenience
Access convenience Post-consultation convenience Scheduling convenience Decision-making convenience
Information about healthcare provider (i.e., facility, physicians)
Patient-provider pre-encounter communication (reactive/proactive calls)
Tools for self-assessment of medical needs
Physical access (i.e., location, parking, directions, operating hours, support services)
Healthcare SERVCON
Registration & Check-in convenience
Timeliness of check-in process
Accuracy of billing data
Post-encounter communication Psychological care (e.g., attentiveness) Timely and efficient physiological care
Care delivery convenience
Post-care support services
Efficient office administration
Pre-encounter / Pre-care stage
Service encounter stage
Transaction convenience
Post-care / Post-encounter stage
Online accessibility Multi-channel availability P9 P9 P9 P9 P9 P9 P9 P1a P1b P2a P2b P2c P3a P3c P4a P4b P5a P5b P6a P6b P7a P7b P8a P8b (Mobile) Kiosks use Patients’ acceptance of (mobile) kiosks
Perceived benefits/usefulness
Perceived ease of use
Assurance (reliability, security, confidentiality, privacy, staff assistance, system integration)
Moderating patient factors Personality, age, tech skills, medical conditions
Control of payment modus Availability of appointments