BRIEF REPORT
Vitamin D Repletion in Patients with Primary
Hyperparathyroidism and Coexistent Vitamin D
Insufficiency
Andrew Grey, Jenny Lucas, Anne Horne, Greg Gamble, James S. Davidson, and Ian R. Reid Department of Medicine (A.G., J.L., A.H., G.G., I.R.R.), University of Auckland, 92019 Auckland, New Zealand; and Department of Chemical Pathology (J.S.D.), Labplus, Auckland City Hospital, Auckland, New Zealand
Vitamin D insufficiency is common in patients with primary hyperparathyroidism (PHPT) and may be associated with more severe and progressive disease. Uncertainty exists, how-ever, as to whether repletion of vitamin D should be under-taken in patients with PHPT. Here we report the effects of vitamin D repletion on biochemical outcomes over 1 yr in a group of 21 patients with mild PHPT [serum calcium <12 mg/dl (3 mmol/liter)] and coexistent vitamin D insufficiency [serum 25 hydroxyvitamin D [25(OH)D] <20 g/liter (50 nmol/liter)].
In response to vitamin D repletion to a serum 25(OH)D level greater than 20g/liter (50 nmol/liter), mean levels of serum calcium and phosphate did not change, and serum calcium did not exceed 12 mg/dl (3 mmol/liter) in any patient. Levels of intact PTH fell by 24% at 6 months (P<0.01) and 26% at 12
months (P<0.01). There was an inverse relationship between the change in serum 25(OH)D and that in intact PTH (rⴝ ⴚ0.43,Pⴝ0.056). At 12 months, total serum alkaline phospha-tase was significantly lower, and urineN-telopeptides tended to be lower than baseline values (Pⴝ0.02 and 0.13, respec-tively). In two patients, 24-h urinary calcium excretion rose to exceed 400 mg/d, but the group mean 24-h urinary calcium excretion did not change.
These preliminary data suggest that vitamin D repletion in patients with PHPT does not exacerbate hypercalcemia and may decrease levels of PTH and bone turnover. Some patients with PHPT may experience an increase in urinary calcium excretion after vitamin D repletion. (J Clin Endocrinol Metab 90: 2122–2126, 2005)
P
RIMARY HYPERPARATHYROIDISM (PHPT) is a com-mon endocrine condition, particularly in postmeno-pausal women (1). Frequently PHPT is asymptomatic, and there is uncertainty as to the optimal management of this form of the disease. A considerable body of evidence, how-ever, suggests a low incidence of disease progression and/or disease complications in patients managed by observation alone (2–9).Vitamin D deficiency [serum 25 hydroxyvitamin D [25(OH)D]⬍20g/liter (50 nmol/liter)] is increasingly com-mon worldwide, principally as a consequence of sunlight deprivation consequent on both increased public awareness of the risk of skin malignancies associated with exposure to UV radiation and increasing numbers of frail elderly people (10, 11). Patients with PHPT may be at higher risk than eucalcemic individuals of vitamin D deficiency because of accelerated catabolism of 25(OH)D induced by the increased levels of 1,25 dihydroxyvitamin D3 [1,25(OH)2D] that are characteristic of the disorder (12, 13). In eucalcemic subjects, treatment of vitamin D deficiency is recommended to correct
secondary hyperparathyroidism, normalize bone turnover, and reduce the risks of fractures and falls (14, 15). Epidemi-ological studies suggest that vitamin D-deficient patients with PHPT have higher levels of PTH and markers of bone turnover, larger parathyroid adenomas, and more frequent fractures than vitamin D-replete patients (16 –19). These studies suggest that vitamin D deficiency may exacerbate the biochemical phenotype of PHPT by promoting more marked parathyroid cell proliferation and imply that maintenance or restoration of vitamin D sufficiency might prevent or reverse this phenomenon. However, only very limited published data are available that address the effects of correction of vitamin D deficiency in PHPT (20 –22), in part because of concerns that such therapy might exacerbate the hyper-calcemia and/or hypercalciuria that are features of PHPT (18, 23).
In our unit, it has been standard practice to maintain vitamin D sufficiency in patients with PHPT. In this paper, we report the results of a prospective audit of the effects of vitamin D repletion [to a serum level of 25(OH)D⬎20
g/liter (50 nmol/liter)] on biochemical indices of calcium metabolism in a cohort of patients with mild PHPT and vitamin D insufficiency. Our results suggest that repletion of vitamin D in patients with PHPT modestly reduces levels of PTH and markers of bone turnover, without exacerbating hypercalcemia. Although the mean level of urinary calcium excretion did not change within the First Published Online January 11, 2005
Abbreviations: ALP, Alkaline phosphatase; 1,25(OH)2D, 1,25 dihy-droxyvitamin D3; 25(OH)D, 25 hydroxyvitamin D; PHPT, primary hyperparathyroidism.
JCEM is published monthly by The Endocrine Society (http://www. endo-society.org), the foremost professional society serving the en-docrine community.
doi: 10.1210/jc.2004-1772
group, two patients experienced an increase in urinary calcium excretion.
Patients and Methods Patients
Twenty-five hypercalcemic patients (23 women, two men) referred to the Endocrinology Department at Auckland City Hospital were found to have PHPT and coexistent vitamin D insufficiency [25(OH)D⬍20 g/liter (50 nmol/liter)]. All patients had serum calcium less than 12 mg/dl (3 mmol/liter) and were considered by their attending physician to be suitable for conservative (nonoperative) management. Four of the female patients were taking antiresorptive agents before commencing vitamin D replacement (three estrogen, one estrogen and etidronate). No alteration was made to these treatments during the 12 months of observation.
Vitamin D replacement
Vitamin D repletion was undertaken using cholecalciferol 1.25 mg (50,000 IU) tablets (PSM Healthcare, Auckland, New Zealand). Patients were prescribed one tablet per week for 1 month and thereafter one tablet per month for 12 months. Calcium supplements were not prescribed.
Measurements
All measurements were performed on samples collected after over-night fasting. Serum calcium was measured 1 wk after the initial dose of cholecalciferol and monthly thereafter for the duration of the obser-vation period. Serum 25(OH)D was measured monthly. Intact PTH, total alkaline phosphatase (ALP), urinary excretion ofN-telopeptides, and 24-h urinary calcium excretion were measured at baseline and after 6 and 12 months of vitamin D supplementation. Serum 1,25(OH)2D was mea-sured at baseline and after 6 months of vitamin D supplementation in 10 patients.
Total serum calcium, phosphate, albumin, and creatinine were mea-sured using a modular autoanalyzer (Roche, Stockholm, Sweden). An albumin-adjusted serum calcium was calculated using the formula sCaadj⫽total sCa⫺0.02 (sAlbumin [grams per liter]⫺ 40). Serum 25(OH)D was measured by a competitive RIA (Diasorin, Stillwater, MN); serum 1,25(OH)2D by RIA (IDS, Boldon, UK); intact PTH by either an electrochemiluminescence immunoassay [E170, Roche, normal range 19 – 81 pg/ml (1.7–7.3 pmol/liter)] or a two-site immunoradiometric assay [Nichols Institute Diagnostics, San Clemente, CA; normal range 11–55 pg/ml (1–5 pmol/liter)]. In each subject, all the PTH measure-ments were performed using the same assay. UrineN-telopeptides of type 1 collagen were measured by an enzyme-linked immunoassay (Ostex International Inc., Seattle, WA).
Bone densities of the lumbar spine (L1–L4) and femoral neck were measured in 13 and 12 patients, respectively, at baseline and after 12 months of vitamin D therapy, using a DPX-L densitometer (Lunar, Madison, WI).
Statistical analysis
All analyses were performed using the procedures of SAS (version 9.1; SAS Institute, Cary, NC). The Student’sttest for paired samples was used to test whether biochemical or bone density variables changed over 6 and 12 months. These comparisons were prespecified, so a difference was considered statistically significant ifP⬍0.05 for a two-tailed test. Confirmatory analyses using a standard mixed-models approach to repeated measures produced the same conclusions. Relationships be-tween biochemical variables, and their changes over time, were assessed using Pearson’s correlation coefficient.
The current report represents an audit of an established clinical prac-tice in our unit, for which our institutional ethics committee does not require that written informed consent be obtained. Patients consented to the treatment and investigations described as part of their normal med-ical care.
Results
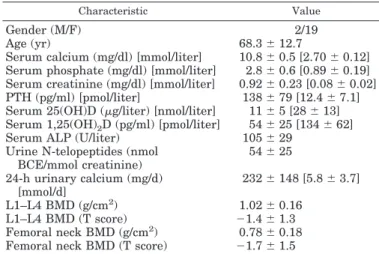
Table 1 shows the baseline demographic and biochemical characteristics of the patients. There was the expected pre-dominance of women, and the biochemical measurements were typical of patients with mild PHPT. All patients had baseline serum calcium less than 12 mg/dl (3 mmol/liter). The mean baseline serum 25(OH)D level was 11g/liter (28 nmol/liter, range 3.2–21). Of the 25 subjects who commenced vitamin D replacement, evaluable data were available for 21. Three women discontinued the vitamin D supplement within the first month. Of these, one developed nonspecific arthralgia, one felt generally unwell, and one did not wish to continue taking a monthly tablet. A fourth patient under-went parathyroid surgery at her request after 3 months of vitamin D repletion. During that time, her serum 25(OH)D level increased from 4.4 g/liter (11 nmol/liter) to 33g/ liter (83 nmol/liter) and serum calcium declined from 11.4 mg/dl (2.86 mmol/liter) to 10.9 mg/dl (2.73 mmol/liter). Two other women underwent parathyroid surgery during the year of observation; one during an admission for chole-cystectomy, the other electively. For each of these patients, biochemical data after 6 months of vitamin D supplemen-tation were available, and they were included in the analysis. After initiation of cholecalciferol therapy, the serum 25(OH)D increased such that the level in each individual patient exceeded 20 g/liter (50 nmol/liter) (Fig. 1). The mean (range) increment in serum 25(OH)D at 6 months was 19 (6 –37)g/liter [47 (16 –92) nmol/liter]; the mean (⫾sd) levels of serum 25(OH)D at 6 and 12 months after commenc-ing vitamin D replacement were 30 ⫾7 g/liter (76 ⫾17 nmol/liter) and 31 ⫾ 6 g/liter (77 ⫾ 14 nmol/liter), re-spectively (P⫽ns for comparison of 6- and 12-month values). Thus, there was no evidence of a progressive increase in serum 25(OH)D levels over time. Levels of 1,25(OH)2D did not change significantly after either 6 months [change from baseline, 12⫾33 pg/ml (30⫾83 pmol/liter),P⫽0.28, n⫽ 10] or 12 months [change from baseline, 24⫾32 pg/ml (60⫾ 81 pmol/liter),P⫽0.13, n⫽6] of vitamin D repletion.
Serum calcium did not change after vitamin D repletion (Fig. 2A). The mean changes in serum calcium after 6 and 12
TABLE 1. Baseline characteristics of patients with primary hyperparathyroidism
Characteristic Value
Gender (M/F) 2/19
Age (yr) 68.3⫾12.7
Serum calcium (mg/dl) [mmol/liter] 10.8⫾0.5 [2.70⫾0.12] Serum phosphate (mg/dl) [mmol/liter] 2.8⫾0.6 [0.89⫾0.19] Serum creatinine (mg/dl) [mmol/liter] 0.92⫾0.23 [0.08⫾0.02]
PTH (pg/ml) [pmol/liter] 138⫾79 [12.4⫾7.1]
Serum 25(OH)D (g/liter) [nmol/liter] 11⫾5 [28⫾13] Serum 1,25(OH)2D (pg/ml) [pmol/liter] 54⫾25 [134⫾62]
Serum ALP (U/liter) 105⫾29
Urine N-telopeptides (nmol BCE/mmol creatinine) 54⫾25 24-h urinary calcium (mg/d) [mmol/d] 232⫾148 [5.8⫾3.7] L1–L4 BMD (g/cm2) 1.02⫾0.16 L1–L4 BMD (T score) ⫺1.4⫾1.3 Femoral neck BMD (g/cm2) 0.78⫾0.18
Femoral neck BMD (T score) ⫺1.7⫾1.5
months of vitamin D repletion were 0.005 ⫾ 0.03 mg/dl (0.02⫾0.12 mmol/liter) (P⫽0.51) and⫺0.008⫾0.02 mg/dl (⫺0.03⫾0.09 mmol/liter) (P⫽0.12), respectively. No patient experienced a rise in serum calcium to greater than 12 mg/dl (3 mmol/liter). Ionized calcium did not change over 12 months of vitamin D repletion [change from baseline, 0.04⫾ 0.36 mg/dl (0.01⫾0.09 mmol/liter), n⫽11,P⫽0.61]. In one patient, the serum calcium ostensibly rose by 1.4 mg/dl (0.35 mmol/liter), from 10.5 to 11.9 mg/dl (2.62 to 2.97 mmol/ liter) between the baseline and 6-month assessments (Fig. 2A). She did not develop symptoms of hypercalcemia, and a review of her monthly serum calcium data revealed that the level of 11.9 mg/dl (2.97 mmol/liter) was clearly an outlying value [mean (range) of four other measurements 10.9 (10.6 – 11.4) mg/dl [2.72 (2.64 –2.84) mmol/liter]. She underwent elective parathyroid surgery 7 months after commencing vitamin D replacement during an admission to the hospital for cholecystectomy.
Levels of intact PTH declined by 25% during vitamin D repletion (Fig. 2B). The average change in PTH was similar in magnitude at 6 and 12 months [change at 6 months,⫺33⫾ 49 pg/ml (⫺3.0⫾4.4 pmol/liter),P⫽0.007; change at 12 months,⫺36⫾44 pg/ml (⫺3.2⫾4.0 pmol/liter),P⫽0.004] (Fig. 2B). The change in the serum 25(OH)D level was in-versely correlated with the change in the level of PTH at 6 months (r ⫽ ⫺0.43, P ⫽ 0.056), consistent with a causal relationship between the two variables. There was no cor-relation between change in serum 1,25(OH)2D and change in PTH after 6 months of vitamin D repletion (r⫽ ⫺0.02,P⫽ 0.96).
The decline in PTH levels was accompanied by a signif-icant fall in total ALP (Fig. 3). One patient with a serum
␥-glutamyltransferase greater than 100 U/liter was excluded from this analysis. Total ALP fell by 13.6⫾28 U/liter from baseline to 6 months (n⫽14,P⫽0.10) and 18.9⫾26 U/liter from baseline to 12 months (n ⫽ 14, P ⫽ 0.02). Urine
N-telopeptide excretion tended to decline at 12 months (change from baseline values,⫺14.5⫾33 nmol bone collagen equiv-alent per millimole creatinine, n⫽14,P⫽0.13).
Overall, 24-h urinary excretion of calcium did not change during the 12-month observation period. There was a small, nonsignificant increase observed at 6 months [60⫾112 mg/d (1.5⫾2.8 mmol/d);P⫽0.08], but by 12 months the mean urine calcium excretion was comparable with that at baseline [change from baseline,⫺0.4⫾116 mg/d (⫺0.01⫾2.9 mmol/ d), P ⫽ 0.99]. In three patients the 24-h urinary calcium excretion rose to exceed 400 mg/d (10 mmol/d) after 6 months of vitamin D replacement. In one of these, urinary calcium excretion fell subsequently, such that the 12-month value was below that recorded at baseline. No patient de-veloped symptomatic urolithiasis during the observation period.
There was no change in bone mineral density at either the lumbar spine (change from baseline, 0.00⫾0.05 g/cm2,P⫽ 0.98, n⫽13) or femoral neck (change from baseline, 0.01⫾
FIG. 1. Levels of serum 25(OH)D in patients with PHPT and vitamin D insufficiency treated with cholecalciferol for 1 yr. Values for indi-vidual patients are connected by thesolid lines. Thedotted line rep-resents the level of serum 25(OH)D above which the World Health Organization defines vitamin D sufficiency. To convert serum 25(OH)D values to nanomoles per liter, multiply by 2.5.
FIG. 2. Serum calcium (A) and PTH (B) values in patients with PHPT and vitamin D insufficiency treated with cholecalciferol for 1 yr. Each data point represents the change from baseline value in an individual patient at the indicated time point. Thehorizontal barsrepresent group mean⫾SD. **,P⬍0.01vs.baseline. To convert serum calcium values to millimoles per liter, divide by 4. To convert PTH values to picomoles per liter, divide by 11.1
0.07 g/cm2,P⫽0.71, n⫽12) after 12 months of vitamin D repletion.
Reanalysis of the data set after excluding the patients who were receiving antiresorptive therapy or the male patients did not alter the results.
Discussion
Our findings suggest that vitamin D repletion in patients with mild PHPT does not promote an increase in serum calcium and may modestly decrease levels of PTH and bone turnover. There may be a small early (⬍6 month) increase in urinary calcium excretion, the clinical significance of which is uncertain. These data are consistent with the suggestion from epidemiological studies that hypovitaminosis D in PHPT is associated with a more severe biochemical pheno-type (17, 18, 24) and suggest that maintenance of vitamin D sufficiency may restrain the progression of PHPT.
Vitamin D insufficiency [serum 25(OH)D⬍20g/liter (50 nmol/liter)] is a common finding in eucalcemic populations (10). Vitamin D deficiency may be more common in patients with PHPT than in eucalcemic patients because of acceler-ated catabolism of 25(OH)D induced by the elevacceler-ated levels of 1,25(OH)2D that are characteristic of the disorder (12, 13, 25). Silverberg et al. (18) reported that 53% of a cohort of patients with PHPT manifested vitamin D insufficiency, and Carnevaleet al.(26) found serum 25(OH) levels less than 12
g/liter (30 nmol/liter) in 27% of their cohort. Some author-ities advocate surgical intervention for patients with PHPT and hypovitaminosis D (18, 23), and others caution against vitamin D supplementation (27) because of concerns that repletion of vitamin D might exacerbate hypercalcemia and hypercalciuria, but there are virtually no published data that address the biochemical effects of vitamin D repletion in PHPT. Kantorovichet al.(22) described three patients with PHPT and vitamin D insufficiency, in two of whom PTH fell, and serum calcium remained stable, after vitamin D reple-tion. Our data provide evidence that vitamin D repletion in patients with PHPT may be reasonable and safe and argue against the need to refer patients with PHPT and vitamin D insufficiency for parathyroid surgery in the absence of other indications.
The mechanism by which vitamin D repletion leads to a decline in PTH levels in PHPT is unclear. Our finding that the magnitude of the increment in 25(OH)D level was correlated with the degree of decline in PTH is suggestive of a vitamin D-dependent mechanism. An attractive hypothesis is that, in the presence of a PTH-induced increase in 1␣-hydroxylase activity (28), vitamin D repletion in PHPT might lead to increased levels of circulating 1,25(OH)2D, which is a known inhibitor of PTH gene transcription, PTH protein production and parathyroid gland proliferation (29, 30). The limited data available from our study do not support this notion because there was no association between change in 1,25(OH)2D and change in PTH. Furthermore, administration of active vita-min D metabolites to patients with PHPT does not decrease PTH levels (31), and levels of 1,25(OH)2D are not related to those of 25(OH)D in cross-sectional studies of PHPT (16, 18). It is possible, however, that parathyroid-derived 1,25(OH)2D (32, 33) might act in an intracrine fashion to reduce PTH levels, independent of the circulating 1,25(OH)2D level. Al-ternative explanations include non-1,25(OH)2D-mediated ef-fects of 25(OH)D or other vitamin D metabolites on PTH production or stimulation by vitamin D repletion of expres-sion in parathyroid tissue of the vitamin D receptor, dimi-nution of which in parathyroid adenomas (34, 35) may pro-mote tumor growth and greater PTH production.
The reductions we observed in markers of bone turnover presumably reflect the lowering of PTH levels. Although the reduction in the bone resorption marker urineN-telopeptide was not statistically significant, this is likely the result of the small sample size and the large biological variation in the mea-surement of this variable. Our findings are consistent with those of a cross-sectional study that reported inverse associations between serum 25(OH)D and both PTH and ALP in 124 pa-tients with PHPT (18). Chronic PTH excess stimulates bone turnover and promotes bone loss, at least at skeletal sites en-riched for cortical bone (36, 37); conversely, surgical correction of PHPT decreases markers of bone turnover and increases bone mineral density (37, 38). Limited observational data sug-gest that hypovitaminosis D and the degree of PTH elevation are independently associated with fracture risk in PHPT (19). Thus, the reduction in PTH levels and bone turnover that ac-company vitamin D repletion in patients with PHPT might be predicted to lead to increased BMD and reduced fracture risk. That our data did not demonstrate any effect of vitamin D repletion on bone mineral density might reflect the short fol-low-up and/or the small sample size.
The significance of the increase in urinary calcium excretion that we observed in two of our patients after vitamin D reple-tion is uncertain. Although relative hypercalciuria is a feature of PHPT and urolithiasis occurs in 10–20% of patients with PHPT (39), urinary calcium excretion is a poor predictor of stone formation, such that regular monitoring of urinary calcium excretion is no longer recommended in patients with PHPT (40). A previous episode of urolithiasis is the most powerful pre-dictor of subsequent stone formation in PHPT, and long-term follow-up of patients who have not had renal tract stones sug-gests that the risk of a first event is low (9). Nonetheless, until more safety data are available, it is important to monitor urine calcium excretion in patients with PHPT after vitamin D repletion.
FIG. 3. Plot of changes in total ALP (dark bars) and urineN -telopep-tides of type 1 collagen (open bars) in patients with PHPT and vitamin D insufficiency treated with cholecalciferol for 1 yr. *,P⬍0.05vs.
In summary, the current data provide preliminary evi-dence that judicious replacement of vitamin D, to a serum value of 25(OH)D above the level regarded by the World Health Organization as sufficient for skeletal health in eu-calcemic individuals, may be safe in patients with PHPT and coexistent vitamin D insufficiency. The observation that vi-tamin D repletion reduces levels of PTH and bone turnover in PHPT suggests that maintenance of vitamin D sufficiency in patients with PHPT may restrain disease progression and severity. Larger studies of vitamin D repletion in PHPT, with longer follow-up, are both justified and necessary to assess the safety and efficacy of this treatment.
Acknowledgments
Received September 7, 2004. Accepted January 5, 2005.
Address all correspondence and requests for reprints to: Associate Professor Andrew Grey, Department of Medicine, University of Auck-land, Private Bag 92019, AuckAuck-land, New Zealand. E-mail: a.grey@ auckland.ac.nz; or James S. Davidson, Department of Chemical Pathol-ogy, Labplus, Auckland City Hospital, Private Bag 92-024, Auckland, New Zealand.
This work was supported by the Health Research Council of New Zealand.
References
1. Adami S, Marcocci C, Gatti D2002 Epidemiology of primary hyperparathy-roidism in Europe. J Bone Miner Res 17:N18 –N23
2. Rubinoff H, McCarthy N, Hiatt RA1983 Hypercalcemia: long-term follow-up with matched controls. J Chronic Dis 36:859 – 868
3. Posen S, Clifton-Bligh P, Reeve TS, Wagstaffe C, Wilkinson M1985 Is parathyroidectomy of benefit in primary hyperparathyroidism? Q J Med 54: 241–251
4. Rao DS, Wilson RJ, Kleerekoper M, Parfitt AM1988 Lack of biochemical progression or continuation of accelerated bone loss in mild asymptomatic primary hyperparathyroidism: evidence for biphasic disease course. J Clin Endocrinol Metab 67:1294 –1298
5. Sampson MJ, van’t Hoff W, Bicknell EJ1987 The conservative management of primary hyperparathyroidism. Q J Med 65:1009 –1014
6. Wermers RA, Khosla S, Atkinson EJ, Hodgson SF, O’Fallon WM, Melton 3rd LJ1997 The rise and fall of primary hyperparathyroidism: a population-based study in Rochester, Minnesota, 1965–1992. Ann Intern Med 126:433– 440 7. Davies M, Fraser WD, Hosking DJ2002 The management of primary
hy-perparathyroidism. Clin Endocrinol (Oxf) 57:145–155
8. Miedlich S, Krohn K, Paschke R2003 Update on genetic and clinical aspects of primary hyperparathyroidism. Clin Endocrinol (Oxf) 59:539 –554 9. Silverberg SJ, Shane E, Jacobs TP, Siris E, Bilezikian JP1999 A 10-year
prospective study of primary hyperparathyroidism with or without parathy-roid surgery. N Engl J Med [Erratum (2000) 342:144] 341:1249 –1255 10. Lips P, Duong T, Oleksik A, Black D, Cummings S, Cox D, Nickelsen T2001
A global study of vitamin D status and parathyroid function in postmeno-pausal women with osteoporosis: baseline data from the multiple outcomes of raloxifene evaluation clinical trial. J Clin Endocrinol Metab 86:1212–1221 11. Holick MF2001 Sunlight “D”ilemma: risk of skin cancer or bone disease and
muscle weakness. Lancet 357:4 – 6
12. Clements MR, Davies M, Hayes ME, Hickey CD, Lumb GA, Mawer EB, Adams PH1992 The role of 1,25-dihydroxyvitamin D in the mechanism of acquired vitamin D deficiency. Clin Endocrinol (Oxf) 37:17–27
13. Clements MR, Davies M, Fraser DR, Lumb GA, Mawer EB, Adams PH1987 Metabolic inactivation of vitamin D is enhanced in primary hyperparathy-roidism. Clin Sci 73:659 – 664
14. Chapuy MC, Arlot ME, Delmas PD, Meunier PJ1994 Effect of calcium and cholecalciferol treatment for three years on hip fractures in elderly women. BMJ 308:1081–1082
15. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB, Baze-more MG, Zee RY, Wong JB2004 Effect of vitamin D on falls: a meta-analysis. JAMA 291:1999 –2006
16. Rao DS, Honasoge M, Divine GW, Phillips ER, Lee MW, Ansari MR, Talpos GB, Parfitt AM2000 Effect of vitamin D nutrition on parathyroid adenoma
weight: pathogenetic and clinical implications. J Clin Endocrinol Metab 85: 1054 –1058
17. Rao DS, Agarwal G, Talpos GB, Phillips ER, Bandeira F, Mishra SK, Mithal A2002 Role of vitamin D and calcium nutrition in disease expression and parathyroid tumor growth in primary hyperparathyroidism: a global perspec-tive. J Bone Miner Res 17:N75–N80
18. Silverberg SJ, Shane E, Dempster DW, Bilezikian JP1999 The effects of vitamin D insufficiency in patients with primary hyperparathyroidism. Am J Med 107:561–567
19. Nordenstrom E, Westerdahl J, Lindergard B, Lindblom P, Bergenfelz A2002 Multifactorial risk profile for bone fractures in primary hyperparathyroidism. World J Surg 26:1463–1467
20. Lumb GA, Stanbury SW1974 Parathyroid function in human vitamin D deficiency and vitamin D deficiency in primary hyperparathyroidism. Am J Med 56:833– 839
21. Woodhouse NJ, Tun Chot S, Bordier P, Sigurdsson G, Joplin GF1973 Vitamin D administration in primary hyperparathyroidism. Clin Sci 44:3P (passim) 22. Kantorovich V, Gacad MA, Seeger LL, Adams JS2000 Bone mineral density
increases with vitamin D repletion in patients with coexistent vitamin D insufficiency and primary hyperparathyroidism. J Clin Endocrinol Metab 85: 3541–3543
23. Bilezikian JP2000 Primary hyperparathyroidism. When to observe and when to operate. Endocrinol Metab Clin North Am 29:465– 478
24. Bandeira F, Caldas G, Freese E, Griz L, Faria M, Bandeira C2002 Relationship between serum vitamin D status and clinical manifestations of primary hy-perparathyroidism. Endocr Pract 8:266 –270
25. Davies M, Heys SE, Selby PL, Berry JL, Mawer EB1997 Increased catabolism of 25-hydroxyvitamin D in patients with partial gastrectomy and elevated 1,25-dihydroxyvitamin D levels. Implications for metabolic bone disease. J Clin Endocrinol Metab 82:209 –212
26. Carnevale V, Manfredi G, Romagnoli E, De Geronimo S, Paglia F, Pepe J, Scillitani A, D’Erasmo E, Minisola S2004 Vitamin D status in female patients with primary hyperparathyroidism: does it play a role in skeletal damage? Clin Endocrinol (Oxf) 0:81– 86
27. al Zahrani A, Levine MA1997 Primary hyperparathyroidism. Lancet 349: 1233–1238
28. Feldman D1999 Vitamin D, parathyroid hormone, and calcium: a complex regulatory network. Am J Med 107:637– 639
29. Miura R, Furukawa Y, Yumita S, Sohn HE, Mizunashi K, Yoshinaga K1987 25-Hydroxyvitamin D3 loading test in primary hyperparathyroidism, hypo-parathyroidism and pseudohypohypo-parathyroidism. Endocrinol Jpn 34:97–104 30. Beckerman P, Silver J1999 Vitamin D and the parathyroid. Am J Med Sci
317:363–369
31. Lind L, Wengle B, Sorensen OH, Wide L, Akerstrom G, Ljunghall S1989 Treatment with active vitamin D (alphacalcidol) in patients with mild primary hyperparathyroidism. Acta Endocrinol 120:250 –256
32. Correa P, Segersten U, Hellman P, Akerstrom G, Westin G2002 Increased 25-hydroxyvitamin D3 1␣-hydroxylase and reduced 25-hydroxyvitamin D3 24-hydroxylase expression in parathyroid tumors—new prospects for treat-ment of hyperparathyroidism with vitamin D. J Clin Endocrinol Metab 87: 5826 –5829
33. Segersten U, Correa P, Hewison M, Hellman P, Dralle H, Carling T, Aker-strom G, Westin G2002 25-Hydroxyvitamin D(3)-1␣-hydroxylase expression in normal and pathological parathyroid glands. J Clin Endocrinol Metab 87: 2967–2972
34. Carling T, Rastad J, Szabo E, Westin G, Akerstrom G2000 Reduced para-thyroid vitamin D receptor messenger ribonucleic acid levels in primary and secondary hyperparathyroidism. J Clin Endocrinol Metab 85:2000 –2003 35. Sudhaker Rao D, Han ZH, Phillips ER, Palnitkar S, Parfitt AM2000 Reduced
vitamin D receptor expression in parathyroid adenomas: implications for pathogenesis. Clin Endocrinol (Oxf) 53:373–381
36. Grey AB, Stapleton JP, Evans MC, Reid IR1996 Accelerated bone loss in post-menopausal women with mild primary hyperparathyroidism. Clin En-docrinol (Oxf) 44:697–702
37. Guo CY, Thomas WE, al-Dehaimi AW, Assiri AM, Eastell R1996 Longitudinal changes in bone mineral density and bone turnover in postmenopausal women with primary hyperparathyroidism. J Clin Endocrinol Metab 81:3487–3491 38. Silverberg SJ, Gartenberg F, Jacobs TP, Shane E, Siris E, Staron RB, McMahon
DJ, Bilezikian JP1995 Increased bone mineral density after parathyroidectomy in primary hyperparathyroidism. J Clin Endocrinol Metab 80:729–734 39. Silverberg SJ2000 Natural history of primary hyperparathyroidism.
Endo-crinol Metab Clin North Am 29:451– 464
40. Bilezikian JP, Potts Jr JT, Fuleihan Gel H, Kleerekoper M, Neer R, Peacock M, Rastad J, Silverberg SJ, Udelsman R, Wells SA2002 Summary statement from a workshop on asymptomatic primary hyperparathyroidism: a perspec-tive for the 21st century. J Clin Endocrinol Metab 87:5353–5361
JCEM is published monthly by The Endocrine Society (http://www.endo-society.org), the foremost professional society serving the endocrine community.