GSJ: Volume 7, Issue 4
,
April
2019, Online: ISSN 2320-9186
www.globalscientificjournal.com
L
YMPHOMA
P
RESENTING
A
S
M
ULTINODULAR
G
OITRE
Sharanjeet Singh1, Norhafiza Mat Lazim2 , Zaleha Kamaludin3, Faezahtul Arbaeyah Hussain4
ORL-HNS Department, Department of Pathology, School of Medical Sciences, Universiti Sains Malaysia
1. Introduction
Head and neck are the second most common site for extra-nodal lymphoma. It can involve virtually any region, including the orbit, paranasal sinuses, Waldeyer's ring, salivary glands, or thyroid but the commonest is the cervical lymph nodes. The diagnosis of lymphoma is based on the histopathology examination of tissue biopsy taken from the enlarged lesion or lymph nodes. The purpose of this report is to make the otolaryngologist aware of this entity as a cause of an anterior neck mass.
Lymphomas are cancers of lymphatic system which composed of lymph nodes in the neck, armpits, groin, chest, and abdomen. It divided into two categories: Hodgkin lymphoma and non-Hodgkin lymphoma. Non-Hodgkin lymphomas (NHL) represent a group of neoplasm that commonly involve extra-nodal structures. NHL of the head and neck arises from lymph nodes in 65% of cases and, 25% to 30% in extra-nodal cases 2.
Twenty four percent of all non-Hodgkin lymphomas originate in extra-nodal sites, with thirty four percent of these involves head and neck structures.7. Primary malignant lymphoma of the thyroid gland is uncommon, and represents less than 5% of all thyroid malignancies 1 .NHL of the thyroid gland generally presents in the sixth or seventh decades of life4,5 .
Keywords : neck tumor,lymphoma,thyroid mass,chronic lymphocytic leukemia
Corresponding Author: Dr Sharanjeet Singh
Department of Otolaryngology - Head and Neck Surgery (ORL-HNS), School of Medical Sciences,
Universiti Sains Malaysia,
Kubang Kerian 16150, Kelantan, Malaysia
Department of Otolaryngology - Head and Neck Surgery (ORL-HNS), School of Medical Sciences,
Universiti Sains Malaysia,
Kubang Kerian 16150, Kelantan, Malaysia Tel: +60174127390
Dr Faezahtul Arbaeyah Hussain
Senior Medical Lecturer and Anatomic Pathologist MMC no:44984 NSR no: 133133
School of Medical Sciences, Universiti Sains Malaysia,
Kubang Kerian 16150, Kelantan, Malaysia
Dr Zaleha Bt Kamaludin Department Of Pathology School of Medical Sciences, Universiti Sains Malaysia,
Kubang Kerian 16150, Kelantan, Malaysia
2. Case Report
A 55-year-old gentleman presented to our otorhinolaryngology clinic with a one-year history of painless swelling in the anterior region of the neck. The swelling had been gradually increasing in size but not associated with dysphagia, hoarseness or dyspnea. There were no constitutional symptoms present in the patient and no symptoms of hypothyroidism or hyperthyroidism. In addition, patient denied any history of trauma or insect bite related to the neck.
Upon examination patient was comfortable and no stridor. Physical examination revealed a firm, non-tender, fixed anterior neck mass along the midline measuring about 8x8 cm. The surface of the mass is smooth, with no overlying skin changes and does not move with deglutition.
Routine hematological biochemical investigations were normal Thyroid function tests were also normal. Ultrasound neck shows multinodular goiter bilaterally and subsequently fine needle aspiration cytology which revealed features suggestive of lymphoma.
We then proceeded with computer tomography of brain, neck, abdomen and pelvis with contrast which then revealed anterior neck mass along the midline level four measuring 5x10x7, thyroid homogenously enhanced with no calcification within. Subsequently an incisional biopsy was done.
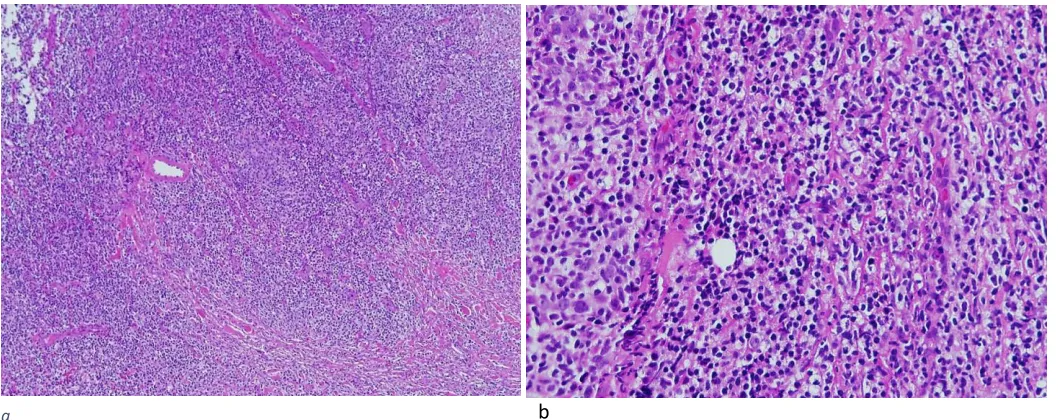
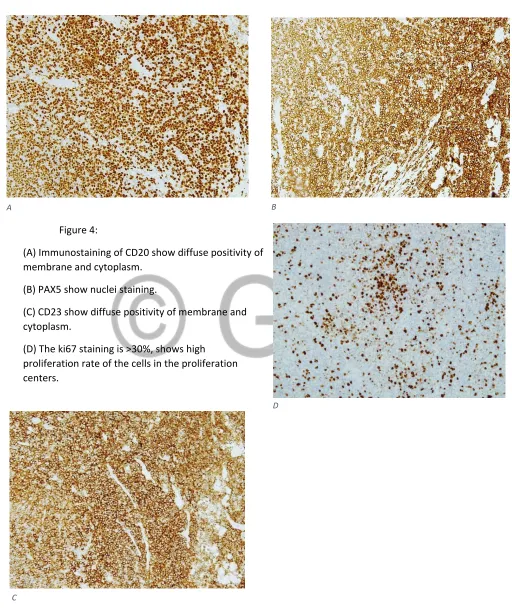
medium cells have round nuclei with dispersed chromatin, centrally located eosinophilic nucleoli and slightly basophilic cytoplasm. Foci of sclerotic bands were present. There are scattered reactive mature T-cells are observed in the background. The neoplastic lymphoid cells demonstrated strong positive immunostaining for B-cell markers, CD 20 and CD 79a. The CD3, CD 23, PAX5 were also strongly positive. Mitoses were minimal. The Ki-67 proliferative index were generally low, but show high proliferation rate of the cells within the proliferation centers.
Figure 1- 55 years old gentleman with an anterior neck swelling.
b
Figure 3. Microscopic findings (hematoxylin-eosin stain)
(a) Low magnification exhibits diffuse proliferation of neoplastic lymphoid cell (dark and paler areas) (x40).
(b) Higher magnification of monotonous neoplastic lymphoid cells exhibits regular nuclear outline and minimal cytoplasm(x400).
Figure 4:
(A) Immunostaining of CD20 show diffuse positivity of membrane and cytoplasm.
(B) PAX5 show nuclei staining.
(C) CD23 show diffuse positivity of membrane and cytoplasm.
(D) The ki67 staining is >30%, shows high proliferation rate of the cells in the proliferation centers.
Figure A B
A B
C
3. Discussion and Conclusion
Malignant lymphomas represent approximately 5 percent of all malignant neoplasm of the head and neck and may involve nodal or extra-nodal sites . The head and neck is the second most frequent anatomical site of extra-nodal lymphomas 1 and should be considered as the differential diagnosis of any patients who presented with neck mass especially in the young adult patients.
Small lymphocytic lymphoma (SLL) is synonym with Chronic lymphocytic leukemia (CLL). It is a neoplasm constituted of monomorphic small mature B cells that co-express CD5 and CD23 immunostains. CLL/SLL counts for 7% of non-Hodgkin lymphomas9,10 .
CLL is established by present of monoclonal B- racteristic morphology and phenotype of CLL in the peripheral blood. The term of SLL is used when the circulating CLL cell count < 5x109/L and involvement of nodal, and secondary lymphoid tissues such as the spleen, lymph nodes, and Waldeyer ring. The common extra-nodal involvements are skin, gastrointestinal tract, kidneys or CNS 12 . SLL is diagnosed in 10- 20% of cases, and about 20% evolve into frank CLL13.
Microscopically, SLL shows diffuse architectural effacement by a proliferation of small mature lymphocytes with patchy paler proliferation centres14 . The small lymphocyte exhibits scant cytoplasm, round nucleus, clumped chromatin, and occasionally a small nucleolus. There are some cases which the small lymphoid cells show moderate nuclear irregularity, which can lead to a differential diagnosis of mantle cell lymphoma. Mitotic activity is usually very low15 . CD20 and CD23 expression is usually stronger in cells of the proliferation centres than in the diffuse areas Follicular dendritic cell meshworks are present in some cases, and may be associated with the proliferation centres. About 2-8% of patients with CLL progress to DLBCL (Reiter’s disease), and < 1% develop classic Hodgkin lymphoma 16.
CT and MR are preferred imaging techniques for assessment of enlarged lymph nodes, bony abnormalities, and calcifications. The CT appearance of lymph nodes is isodense with muscle and necrosis is seldom seen. MR imaging is preferred to view evident of extension of lymphoma to different fascial planes and for intracranial extension. CT and MR imaging however cannot distinguish HL from NHL, and cannot differentiate their various subtypes, necessitating a pathologic diagnosis.
REFERENCES
1. T.Vega, P.Lin and,L. Jeffery Medeiros “Extranodal Lymphomas Of the Head And Neck” Annals of Diagnostic Pathology, vol 9, 2005 pp 340-350. doi.org/10.1016/j.anndiagpath.2005.09.020.
2. Burton, G., Atwater, S., Borowitz, M., & Huang, A. (1990). Extranodal Head and Neck Lymphoma: Prognosis and Patterns of Recurrence. Archives Of Otolaryngology - Head And Neck
Surgery, 116(1), 69-73. doi: 10.1001/archotol.1990.01870010073021.
3. Alfred L. Weber, A. Rahemtullah and Judith A. Ferry “ Hodgkin and non-Hodgkin Lymphoma of the head and neck:clinical, pathologic, and imaging evaluation”, neuroimag Clin Am vol 13, 2003, pp 371-392. doi:10.1016/S1052-5149(03)00039-X.
4. PEDERSEN, R., & PEDERSEN, N. (1996). Primary non-Hodgkin's lymphoma of the thyroid gland: a population based study. Histopathology, 28(1), 25-32. doi: 10.1046/j.1365-2559.1996.268311.x.
5. Aozasa, K., Inoue, A., Tajima, K., Miyauchi, A., Matsuzuka, F., & Kuma, K. (1986). Malignant lymphomas of the thyroid gland: Analysis of 79 patients with emphasis on histologic prognostic factors. Cancer, 58(1), 100-104. doi:
10.1002/1097-0142(19860701)58:1<100::aid-cncr2820580118>3.0.co;2-1.
6. Sa A Wang et al. “Hodgkin’s lymphoma of the thyroid:a clinicopathologic study of five cases and review of the literature”, modern pathology, vol 18, 2005 pp 1577-1584.
doi:10.1038/modpathol.3800501.
7. Jonathan Ben-Ezra, Jerome S. Burke, William G. Swartz et al “ Small Lymphocytic Lymphoma : A Clinicopathalogic Analysis of 268 Cases,” Blood journal, vol 73, Feb 1989, pp 579-587.
8. Freeman et al. “ Occurrence And Prognosis Of Extranodal Lymphoma,” American Cancer Society, vol 29 January 1972, pp 252-260.
9. H. Rowley et al “ Lymphoma Presenting To Head and Neck Clinic,” Clin. Otolaryngol. 1995, vol 20, pp 139-144.
10. Gary V. Burton, MD; Susan Atwater, MD; Michael J. Borowitz, MD, PhD; Andrew T. Huang, MD, “Extranodal Head and Neck Lymphoma,” Arch Otolaryngology Head and Neck Surgery, vol 116, January 1990.
11. Ismail Essadi, Nabil Ismaili, Elmehdi Tazi, Sanaa Elmajjaoui, Ammar Saidi, Mohammed Ichou and Hassan Errihani “Primary lymphoma of the head and neck: two case reports and review of the literature,” cases journal 2008. doi:10.1186/1757-1626-1-426.
12. Morton LM, Wang SS, Devesa SS, et al. (2006). Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. Blood. 107:265-76. PMID:16150940.
14. Hallek M, Cheson BD, Catovsky D, et al. (2008). Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic
Lymphocytic Leukemia updat- ing the National Cancer Institute-Working Group 1996 guidelines. Blood. 111:5446-56. PMID:18216293
15. Ratterman M, Kruczek K, Sula S, et al. (2014). Extramedullary chronic lympho- cytic leukemia: systematic analysis of cases reported between 1975 and 2012. Leuk Res. 38:299- 303. PMID:24064196.
16. Rauen KA (2013). The RASopathies. Annu Rev Genomics Hum Genet. 14:355-69. PMID:23875798.
17. Lennert K, editor. (197S). Malignant lym- phomas other than Hodgkin's disease. New York: Springer Verlag.
18. Bonzheim I, Salaverria I, Haake A, et al. (2011). A unique case of follicular lymphoma provides insights to the clonal evolution from follicular lymphoma in situ to manifest follicular lymphoma. Blood. 118:3442-4. PMID:21940830.