Acid-Fast Bacilli (AFB) by Use of the ReaSLR Method
Sheetal Verma,aTapan N. Dhole,aManoj Kumar,aSaurabh Kashyapb
Department of Microbiology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, Indiaa; Department of Community Medicine, King George’s Medical University, Chowk, Lucknow, Indiab
The ReaSLR methodology developed for sputum processing is a novel, low-cost, and simple technique that has improved the sensitivity of smear microscopy for the diagnosis of tuberculosis (TB). Sample processing consists of rapid liquefaction of the sputum specimen with the ReaSLR reagent, followed by syringe filtration, concentration by centrifugation, and use of the sedi-ment for smear microscopy. The performance of the ReaSLR kit was evaluated on 150 sputum samples and was compared with that of the modified Petroff method for sputum decontamination and concentration. Ziehl-Neelsen staining was performed for smear microscopy after processing by these two techniques; simultaneously, culture on Lowenstein-Jensen (LJ) medium was done to evaluate the two methods. The efficiency of smear microscopy was 18/150 (12%) with the modified Petroff method com-pared to 47/150 (31.33%) with the ReaSLR method, and this difference was statistically significant (P<0.001). The ReaSLR method for smear microscopy demonstrated a sensitivity and specificity of 90.47% and 91.6%, respectively, whereas the modi-fied Petroff method showed a sensitivity and specificity of 40.47% and 99.07%, respectively, compared to those of culture, which was used as the gold standard. With the newer ReaSLR method, the kappa coefficient () was 0.8, which implies an excellent pos-itive agreement. The ReaSLR method was found to be more senspos-itive than the conventional method for sputum smear micros-copy. The newer ReaSLR method holds promise for adoption in TB control programs across the globe, as it was found suitable for the laboratory diagnosis of pulmonary TB. Further large-scale studies are needed to evaluate other aspects of this method.
T
uberculosis (TB), an airborne infectious disease, continues to be a major global health problem. About 9 million new cases of TB are diagnosed and close to 2 million people die of the disease each year. The majority of cases occur in Africa (30%) and Asia (55%), with India and China accounting for about 35% of all such cases (1). With the emergence of multidrug-resistant tuberculosis (MDR-TB) (around 0.4 to 0.5 million cases each year), the sce-nario is becoming more challenging (2).The threat of TB is alarming, and the disease can be controlled only by an effective TB control program. Early case detection is a crucial step in the control of the disease, and this relies solely on the detection of acid-fast bacilli (AFB) in clinical samples. Sputum microscopy with Ziehl-Neelsen (ZN) staining has been a reliable tool for decades, especially in the setting of developing countries, but it has only a 40 to 60% sensitivity for the diagnosis of pulmo-nary TB (3). It has the advantages of low cost, a need for minimal expertise, rapid processing, and simplicity but has the disadvan-tage of a lack of sensitivity (4,5,6). The methods of decontami-nation, liquefaction, and concentration before the ZN staining improve the yield and allow identification of the AFB in the spu-tum sample (7,8). There is a need to upgrade the existing simple diagnostic techniques without complicating them further to in-crease sensitivity of case detection (5,6).
N-Acetyl-L-cysteine (NALC) with 2% sodium hydroxide
(NaOH) and the modified Petroff method are among the popular techniques for mucus digestion which allow concentration of AFB in the processed smear, but they are cumbersome and tedious and require special equipment (9). NALC-NaOH and the modified Petroff method have shown improvement, with sensitivities vary-ing between 60 and 86% (6,10,11). Various other studies using modifications like the universal sample processing (USP) method (8), household bleach (10), carboxypropylbetaine (12), phenol
ammonium sulfate (13), and chitin (14) have reported sensitivi-ties varying from 65 to 85%.
The aim of this prospective blinded study was to evaluate the performance of a new technique called ReaSLR sputum sample processing (ReaMetrix India Pvt. Ltd., Bangalore, India) for its AFB smear sensitivity and specificity for the diagnosis of TB. In this method, ready-to-use tablets with a chaotrope along with re-ducing agents exert mucolytic activity, which ensures the effective release of the trapped mycobacteria in the sputum sample. A fil-tration system (using a syringe to remove insoluble particles) im-proves visualization of AFB in the smear. The diagnostic accuracy and performance of this novel technique for sputum processing were compared to those of the well-established modified Petroff method in a hospital-based setting. The new method described here is a processing technique and not a diagnostic test.
MATERIALS AND METHODS
Study population.A total of 150 sputum samples were obtained from patients with clinically suspected pulmonary TB attending either an inpa-tient or outpainpa-tient clinic in our hospital between October 2012 and Jan-uary 2013. The samples were processed in the Department of Microbiol-ogy mycobacteriolMicrobiol-ogy laboratory at Sanjay Gandhi Institute of Medical Sciences (Lucknow, India).
Specimen collection.Early-morning mucus expectorate was collected by each patient after proper instructions were given; only one sample from
Received24 June 2013 Returned for modification23 July 2013 Accepted14 August 2013
Published ahead of print21 August 2013
Address correspondence to Tapan N. Dhole, [email protected].
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.01570-13
on May 16, 2020 by guest
http://jcm.asm.org/
each patient was included in the study. The procedures were performed in the biological safety level 3 facility in the microbiology laboratory of the Sanjay Gandhi Institute of Medical Sciences. Samples were processed on the same day they were collected and, in case of delay, were stored for less than 24 h at 4°C before processing. Each sample was split into two por-tions after homogenization, and these porpor-tions were transferred into 20-ml plastic conical tubes. Samples with a volume of⬍4 ml were ex-cluded from the study. A 2-ml volume was used for the ReaSLR method, and the rest of the sample (xml) was used for the modified Petroff method.
Specimen processing by ReaSLR methodology.The ReaSLR reagent kit contains two components, ready-to-use tablets of the ReaSLR reagent, which includes a chaotrope and reducing agents, and a ready-to-use sy-ringe for filtration. In a 15-ml centrifuge tube, one tablet of the reagent was added to approximately 2 ml of the sputum sample. The cap on the sample was closed, and the reagent was mixed by inverting the tube 10 to 15 times. The tube was incubated at room temperature for 10 min for complete liquefaction. The digested sample was poured through the sy-ringe for filtration into another 15-ml centrifuge tube to remove any in-soluble particulate matter. This tube was centrifuged at 3,000⫻gfor 10 min at room temperature. The tube was uncapped, and the supernatant was removed, leaving behind approximately 100l of solution. The pellet was not disturbed while the supernatant was removed. The pellet was resuspended, and a suitable volume (⬃1 drop, 50l) was transferred onto the glass slide to make the smear for a standard acid-fast staining protocol. The ReaSLR method was used only to visualize AFB by microscopy with ZN staining.
Specimen processing by the NaOH method and modified Petroff procedure.Toxml of sputum in McCartney tubes, double the volume of sterile 4% NaOH solution was added aseptically. The caps were tightened, and the contents were mixed well by inverting the tubes. The bottles were then placed in a shaker and kept in a 37°C incubator for 15 min. The tubes were removed, and 15 ml of sterile distilled water was added, mixed well, and centrifuged at 3,000⫻g for 15 min. The McCartney tubes were carefully removed from the centrifuge without shaking. The supernatant fluid was discarded slowly into a container with a 5% phenol solution. To the sediment, 50 ml sterile distilled water was added, and the pellet was washed. The supernatant was decanted, and the sediment was used for smears and culture (15). One drop of sediment was used to prepare the slides for AFB microscopy using the standard ZN staining technique.
AFB smears and ZN staining.After the slides were processed by the two methods described above, they were given a code number and were heat fixed. Thereafter, ZN staining was performed according to a previ-ously described method (9), and the stained slides were read blindly by a qualified microbiologist. The stained smears were scanned under⫻1,000 magnification with a light microscope. Smears were scored as 1⫹(10 to 99 AFB in 100 fields), 2⫹(1 to 10 AFB per field), 3⫹(⬎10 AFB per field), scanty (1 to 9 AFB per 100 oil immersion fields), or negative (no AFB in 100 fields) according to the Revised National Tuberculosis Control Pro-gramme (RNTCP) guidelines (16).
Culture. After decontamination/concentration by the modified Petroff method, 200l of resuspended pellet was inoculated into Lowen-stein-Jensen (LJ) medium. The culture tubes were incubated at 37°C for 8 weeks before being reported as negative. The cultures were read weekly, and the suspect (white or buff-colored) colonies were examined micro-scopically after ZN staining. TheMycobacteriumisolates were identified by morphology, growth rate, pigmentation, and ZN staining (9). The colonies were classified asMycobacterium tuberculosiscomplex (MTC) or
Mycobacterium aviumcomplex (MAC) colonies (pigmented mycobacte-ria and rapid growth in⬍7 days). The MAC colonies were not further characterized to the species level. The cultures that showed any contami-nation during incubation were further decontaminated with 1% cetrim-ide agar, reinoculated into the LJ medium, and again incubated for a maximum of 8 weeks (17).
Statistical analysis.In this study, the efficiency of the test tool was calculated as (total number of positive cases/total number of analyzed cases)⫻100. The sensitivity ([Tp/(Tp⫹Fn)]⫻100) and specificity ([Tn/(Tn⫹Fp)]⫻100) (where Tp is the total number of true positives, Tn is the total number of true negatives, Fp is the total number of false positives, and Fn is the total number of false negatives) were also deter-mined. In addition, the positive predictive value was calculated as Tp obtained/total number of positives, and the negative predictive value was calculated as Tn obtained/total number of negatives. The positive concor-dance between the culture and the performed microbiological tests was assessed using the kappa coefficient (), where⬎0.75 indicates excellent agreement,ⱕ0.75 indicates fair agreement,ⱖ0.4 indicates good agree-ment, and⬍0.4 indicates poor agreement (18). The significance level was determined by the chi-square (2) test with the help of SPSS (version
15.10). A difference was considered statistically significant at aPvalue of
⬍0.05. The culture on LJ medium was used as the gold standard in the present study.
RESULTS
The ReaSLR method was evaluated by using smear microscopy and was compared with the modified Petroff method for sputum processing on 150 sputum specimens from patients suspected of having active pulmonary TB.
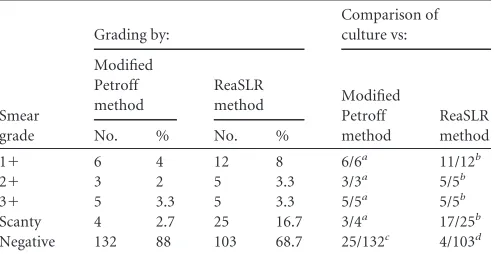
[image:2.585.299.546.87.214.2]Efficiency of AFB microscopy by the two processing meth-ods.The overall rate of positivity for smear microscopy was 18/ 150 (12%) sputum samples with the modified Petroff method compared to 47/150 (31.33%) sputum samples for the ReaSLR method. The numbers of positive samples graded as 3⫹(n⫽5) were similar for the two methods with no significant difference (P⬎0.05). There were 2 additional samples detected in the 2⫹ category by the ReaSLR method (n⫽5) compared to the number detected by the modified Petroff method (n⫽3). The ReaSLR method detected a greater number of positive samples graded as 1⫹or scanty. The modified Petroff method detected 6 samples in the grade 1⫹category, whereas the ReaSLR method detected an additional 6 samples (n⫽12) from the same group (Table 1). The most important difference was seen with the smears graded as scanty. Most of the positive samples missed by the modified Petroff method were graded as scanty by the ReaSLR method. The TABLE 1Distribution of smear and culture results after processing by both techniques
Smear grade
Grading by:
Comparison of culture vs:
Modified Petroff method
ReaSLR
method Modified Petroff method
ReaSLR method
No. % No. %
1⫹ 6 4 12 8 6/6a 11/12b
2⫹ 3 2 5 3.3 3/3a 5/5b
3⫹ 5 3.3 5 3.3 5/5a 5/5b
Scanty 4 2.7 25 16.7 3/4a 17/25b Negative 132 88 103 68.7 25/132c 4/103d
aNumber of positive results on culture/total number of positive results by the modified
Petroff method on microscopy.
bNumber of positive results on culture/total number of positive results by the ReaSLR
method on microscopy.
cNumber of positive results on culture/total number of negative results by the modified
Petroff method by microscopy.
dNumber of positive results on culture/total number of negative results by the ReaSLR
method by microscopy.
on May 16, 2020 by guest
http://jcm.asm.org/
modified Petroff method detected 4 samples in the scanty cate-gory, whereas the ReaSLR method detected 25 positive samples in the scanty group (Table 1). Differences in grading of the samples by the two methods are shown inTable 2.
Sensitivity and specificity of the ReaSLR and modified Petroff methods in comparison with cultures.The overall rate of positivity for cultures in the present study was 42/150 (28%). Out of the 42 culture-positive isolates obtained, 38 were identified as MTC species and 4 were MAC species. In this study, only three LJ slants were found to be contaminated in the course of the incuba-tion period. After redecontaminaincuba-tion with 1% cetrimide and re-inoculation on the fresh LJ slants was done, and after incubation for 8 weeks, there was no visible growth or further contamination seen.
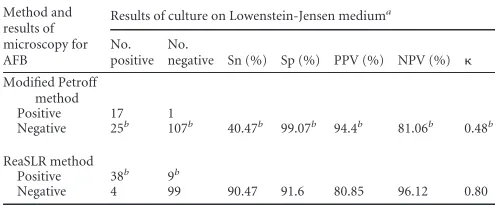
The sensitivity of the modified Petroff method was 40.47%, and the specificity was 99.07%, with positive and negative predic-tive values of 94.4% and 81.06%, respecpredic-tively, compared with those for the culture, which was the gold standard for diagnosis. The kappa coefficient for positive agreement was calculated ( ⫽ 0.48) and showed good agreement between the modified Petroff method and the culture. When the newer ReaSLR method was compared with the culture, the sensitivity improved to 90.47%, with a specificity of 91.6% and positive and negative predictive values of 80.85% and 96.12%, respectively. The positive agree-ment also showed an improveagree-ment, and thevalue was 0.8, which indicates excellent positive agreement for the new method (Table 3).
Most of the samples (n⫽16) identified as positive by the con-ventional method were also positive by the ReaSLR method, but 2 samples were positive only by the modified Petroff method. Out of these 2, only 1 was positive by culture. This might have been due to an unequal distribution of the sample by the tech-nical staff (Table 2).
Comparison of the ReaSLR and modified Petroff methods. Out of the 132 samples deemed negative by the modified Petroff method (smear-negative samples), the ReaSLR method detected 22 additional samples that were also positive by culture, thereby showing an enhancement in the sensitivity of 45.66%, which was statistically significant (P ⬍ 0.001). Among the additional 22 ReaSLR smear-positive and culture-positive samples, 14 were graded as scanty, 5 had a score of 1⫹, 2 had a score of 2⫹, and 1 had a score of 3⫹, suggesting that the modified Petroff method can lead to false results in specimens with lower bacterial loads due to a lack of technical expertise during smear preparation or faulty reading of the slides.
The ReaSLR method showed an enhancement in the sensitivity of 50% (P⬍0.001) over that of the Petroff method (90.47% and 40.47% sensitivities for the ReaSLR and modified Petroff
meth-ods, respectively). On the contrary, there was a decrease in speci-ficity with the ReaSLR method (91.6% specispeci-ficity) compared to that with the modified Petroff method (99.07% specificity).
DISCUSSION
Microscopy for AFB has been considered the key to diagnosis of TB and for monitoring the progress of TB patients (19). The major constituent of a TB sputum sample is mucin protein; mycobacte-rial cells in the sputum are localized in mucin monomers, which readily polymerize to develop highly complex hydrophobic struc-tures (12). Decontamination and concentration methods using various types of substances and their modifications have been re-ported to show improvements in the yield of AFB by microscopy, but the high cost and specialized training needed have been lim-iting factors for their widespread use (11). Smear sensitivities vary among laboratories, and there is a need to evaluate newer methods which can easily be adapted for large-scale use (20).
The technique described here was evaluated in a setting with a high prevalence of TB and low resources. An increase in the pos-itivity rate from 12% to 31.33% in smear microscopy was seen when samples were processed by the ReaSLR method over that of the modified Petroff method. The 50% increase in overall sensi-tivity (P⬍0.001) with the ReaSLR method (90.47%) over that of the modified Petroff method (40.47%) was the most significant finding of this study. The increase with the new method is believed to be the result of rapid liquefaction and subsequent concentra-tion of the mycobacterial cells along with the use of a syringe as an efficient filtration system. The clear debris-free background after processing by the ReaSLR method improved the visualization of AFB, and as a result, samples with a lower bacillary load were easily detected.
The smear-negative cases have significant importance, as 30% of pulmonary TB cases are negative for AFB on microscopy (21, 22). Several investigators have used different techniques which have indicated that smear-negative TB cases pose a serious threat to the effective functioning of TB control programs (23). Among the 132 smear-negative samples, the ReaSLR method detected 22 additional samples which were subsequently positive by culture, with an enhancement in sensitivity of 45.66% (P⬍0.001). The salient finding was that the new ReaSLR method detected 25 pos-itive samples in the scanty group, whereas the modified Petroff method detected only 4 samples in the same group.
[image:3.585.297.546.97.200.2]In this study, only one case was reported negative by the ReaSLR TABLE 2Grading distribution by Ziehl-Neelsen staining performed on
sputum smears after processing by both the modified Petroff and ReaSLR methods
Modified Petroff method grade
No. graded by ReaSLR as:
1⫹ 2⫹ 3⫹ Scanty Negative Total
1⫹ 5 0 0 0 1 6
2⫹ 1 1 1 0 0 3
3⫹ 0 2 3 0 0 5
Scanty 0 0 0 3 1 4
Negative 6 2 1 22 101 132
[image:3.585.41.286.99.174.2]Total 12 5 5 25 103 150
TABLE 3Sensitivity, specificity, positive and negative predictive values, and positive correlation of AFB microscopy results by both
decontamination methods compared with culturea
Method and results of microscopy for AFB
Results of culture on Lowenstein-Jensen mediuma
No. positive
No.
negative Sn (%) Sp (%) PPV (%) NPV (%)
Modified Petroff method
Positive 17 1
Negative 25b 107b 40.47b 99.07b 94.4b 81.06b 0.48b
ReaSLR method
Positive 38b 9b
Negative 4 99 90.47 91.6 80.85 96.12 0.80
aSn, sensitivity, Sp, specificity; PPV, positive predictive value; NPV, negative predictive
value;, positive correlation.
bAgreement between microscopy and culture results.
on May 16, 2020 by guest
http://jcm.asm.org/
method but graded as 1⫹by the modified Petroff method, and this case was found to be culture positive also. This difference in results might be due to unequal sample distribution during pro-cessing, as it is known that mycobacteria tend to form aggregates, clumps, and cords (24). It was observed that 9/42 (21.4%) smear-positive cases detected by microscopy using the ReaSLR method did not eventually grow on culture after 8 weeks. This can be explained by the fact that the microscopy-detected AFB were ei-ther nonviable or dead due to the effect of antitubercular drugs, as patients undergoing treatment were not excluded from the study. This may also be the reason for the lower positive predictive value of the new test (80.85%) compared to that of the modified Petroff method (94.4%).
Another published study reported a sensitivity as high as 85% and a specificity of 97% with the use of a combination of phenol and ammonium sulfate for sputum liquefaction (13). With the hypertonic saline-sodium hydroxide (HS-SH) method, the sensi-tivity value for microscopy was 73.5% and without concentration was 58.3% (4). The USP method compatible with culturing on solid and liquid media demonstrated a sensitivity and specificity of 98.2% and 91.4%, respectively, compared to 68.6% and 92.6% for the direct method (8).
The significant drawback of the modified Petroff method is the requirement for daily preparation of the reagents, which is often cumbersome in the daily routine practice of laboratories (9). In contrast, the advantage of the ReaSLR kit is that the reagent tablets can normally be stored at room temperature without any deteri-oration in their physical appearance. The proposed method uses a filtration system which efficiently removes debris, making the background clearer for interpretation of the results. The average cost of the NALC-NaOH/modified Petroff method is about $1.00 per clinical specimen, and the cost of a commercial kit is $3.50. The average cost of each tablet along with the syringe used for the ReaSLR method is about $0.50 per sample. The limitation of the ReaSLR method is that the test cannot be performed with sputum samples of⬍2 ml, as the tablets require aⱖ2-ml volume for dis-solution. In the present study, the ReaSLR method was not evalu-ated for its usefulness in culture. Therefore, further studies are needed to determine important issues like its effects on culture and to directly perform susceptibility testing in the presence of the ReaSLR reagent.
Smear microscopy is the most important weapon in TB control programs in developing countries, like India. In most of the re-source-limited countries where treatment is initiated on the basis of smear microscopy results alone because culture is time-con-suming, the new method might be very useful for the early initia-tion of antitubercular treatment (ATT). The ReaSLR method has a high sensitivity and can identify TB infections in patients effi-ciently, which would help to curb the transmission of TB and ensure an effective cure. Therefore, it is suggested that the ReaSLR method for smear preparation be adopted in the future by TB control programs in developing countries for the detection of AFB.
In conclusion, we found an increased difference in sensitivity between the ReaSLR method and the modified Petroff concentra-tion method for sputum smear microscopy when performed in patients with clinically suspected TB. The method described here is simple and easy, requires a minimal infrastructure, and is a better alternative to conventional methods for sputum process-ing. We believe that this new technique for sputum processing is a breakthrough milestone for the diagnosis of TB. In the future,
further field evaluations are needed to demonstrate the benefits of the ReaSLR method before it can be widely recommended for sputum processing on a large scale.
ACKNOWLEDGMENT
We thank ReaMetrix India Pvt. Ltd. (Bangalore, India) for providing the ReaSLR kits.
REFERENCES
1.WHO.2010. The Global Plan to Stop TB 2011–2015: transforming the fight towards elimination of tuberculosis. World Health Organization, Geneva, Switzerland. http://www.stoptb.org/assets/documents/global /plan/TB_GlobalPlanToStopTB2011-2015.pdf.
2.WHO.2010. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010. Global report on surveillance and response. WHO/HTM/TB/2010.3. World Health Organization, Geneva, Switzerland.http://whqlibdoc.who.int /publications/2010/9789241599191_eng.pdf.
3.Colebunders R, Bastian I.2000. A review of the diagnosis and treatment of smear-negative pulmonary tuberculosis. Int. J. Tuberc. Lung Dis.4:97– 107.
4.Morcillo N, Imperiale B, Palomino JC.2008. New simple decontamina-tion method improves microscopic detecdecontamina-tion and culture of mycobacte-rium in clinical practice. Infect. Drug Resist.1:21–26.
5.Ganoza CA, Ricaldi JN, Chauca J, Rojas G, Munayco C, Agapito J, Palomino JC, Guerra H.2008. Novel hypertonic saline-sodium hydrox-ide (HS-SH) method for decontamination and concentration of sputum samples forMycobacterium tuberculosismicroscopy and culture. J. Med. Microbiol.57(Part 9):1094 –1098.
6.Steingart KR, Ng V, Henry M, Hopewell PC, Ramsay A, Cunningham J, Urbanczik R, Perkins MD, Aziz MA, Pai M.2006. Sputum processing methods to improve sensitivity of smear microscopy for tuberculosis: a systematic review. Lancet Infect. Dis.6:664 – 674.
7.Saxena S, Mathur M, Talwar VK.2001. Detection of tubercle bacilli in sputum: application of sodium hypochlorite concentration method. J. Commun. Dis.33:241–244.
8.Chakravorty S, Dudeja M, Hanif M, Tyagi JS.2005. Utility of universal sample processing methodology, combining smear microscopy, culture, and PCR, for diagnosis of pulmonary tuberculosis. J. Clin. Microbiol. 43:2703–2708.
9.Kent PT, Kubica GP.1985. Public health microbiology, a guide for the level III laboratory. Centers for Disease Control, Atlanta, GA.
10. Habeenzu C, Lubasi D, Fleming AF.1998. Improved sensitivity of direct microscopy for detection of acid-fast bacilli in sputum in developing countries. Trans. R. Soc. Trop. Med. Hyg.92:415– 416.
11. Apers L, Mutsvangwa J, Magwenzi J, Chigara N, Butterworth A, Mason P, Van der Stuyft P. 2003. A comparison of direct microscopy, the concentration method and the mycobacteria growth indicator tube for the examination of sputum for acid-fast bacilli. Int. J. Tuberc. Lung Dis. 7:376 –381.
12. Thornton CG, MacLellan KM, Brink TL, Jr, Lockwood DE, Romagnoli M, Turner J, Merz WG, Schwalbe RS, Moody M, Lue Y, Passen S.1998. Novel method for processing respiratory specimens for detection of my-cobacteria by using C18-carboxypropylbetaine: blinded study. J. Clin. Mi-crobiol.36:1996 –2003.
13. Selvakumar N, Rahman F, Garg R, Rajasekaran S, Mohan NS, Thya-garajan K, Sundaram V, Santha T, Frieden TR, Narayanan PR.2002. Evaluation of the phenol ammonium sulfate sedimentation smear micros-copy method for diagnosis of pulmonary tuberculosis. J. Clin. Microbiol. 40:3017–3020.
14. Farnia P, Mohammadi F, Zarifi Z, Tabatabee DJ, Ganavi J, Ghazisaeedi K, Farnia PK, Gheydi M, Bahadori M, Masjedi MR, Velayati AA.2002. Improving sensitivity of direct microscopy for detection of acid-fast bacilli in sputum: use of chitin in mucus digestion. J. Clin. Microbiol.40:508 – 511.
15. Kantor Nd, Kim JS, Frieden T, Laszlo A, Luelmo F, Norval PY, Rieder H, Valenzuela P, Weyer K.1998. Laboratory services in tuberculosis control. Part III. Culture. WHO/TB/98.258. WHO, Geneva, Switzerland. 16. Revised National Tuberculosis Control Programme.2005. Guidelines for quality assurance of smear microscopy for diagnosing tuberculosis. Central TB Division, Directorate General of Health Services, Ministry of Health and Family Welfare, New Delhi, India.http://www.tbcindia.nic.in /pdfs/RNTCP%20Lab%20Network%20Guidelines.pdf.
on May 16, 2020 by guest
http://jcm.asm.org/
17. Nagarajan P, Anbarasu S, Kumar V, Selvakumar N.2012. Recovery of
Mycobacterium tuberculosisfrom Löwenstein-Jensen media contaminated with other organisms. Int. J. Tuberc. Lung Dis.16:230 –231.
18. Fleiss JL, Levin BCP.2004. The measurement of interrater agreement, p 598 – 626.InShewhart WA (ed), Statistical methods for rates and propor-tions, 3rd ed. John Wiley & Sons, Hoboken, NJ.
19. Huebner RE, Good RC, Tokars JI.1993. Current practices in mycobac-teriology: results of a survey of state public health laboratories. J. Clin. Microbiol.31:771–775.
20. Scott CP, Dos Anjos Filho L, De Queiroz Mello FC, Thornton CG, Bishai WR, Fonseca LS, Kritski AL, Chaisson RE, Manabe YC.2002. Comparison of C18-carboxypropylbetaine and standardN-acetyl-L -cysteine-NaOH processing of respiratory specimens for increasing tuberculosis smear sensitivity in Brazil. J. Clin. Microbiol.40:3219 –3222.
21. Brugière O, Vokurka M, Lecossier D, Mangiapan G, Amrane A, Milleron B, Mayaud C, Cadranel J, Hance AJ. 1997. Diagnosis of smear-negative pulmonary tuberculosis using sequence capture poly-merase chain reaction. Am. J. Respir. Crit. Care Med.155:1478 –1481. 22. Behr MA, Warren SA, Salamon H, Hopewell PC, Ponce de Leon A, Daley CL, Small PM.1999. Transmission ofMycobacterium tuberculosisfrom pa-tients smear-negative for acid-fast bacilli. Lancet353:444 – 449.
23. WHO.2002. Global tuberculosis control: surveillance, planning, financing. WHO report 2002. WHO/CDS/TB/2002.295. World Health Organization, Geneva, Switzerland.http://apps.who.int/iris/bitstream/10665/75938/1/9789 241564502_eng.pdf.
24. McCarter YS, Ratkiewicz IN, Robinson A.1998. Cord formation in Bactec medium is a reliable, rapid method for presumptive identification of Myco-bacterium tuberculosiscomplex. J. Clin. Microbiol.36:2769 –2771.