Coagulase Test Performed on Positive Blood Cultures for Evaluation
and Application in a Clinical Routine Setting
E. Carretto,aM. Bardaro,aG. Russello,aM. Mirra,aC. Zuelli,aD. Barbarinib
Clinical Microbiology Laboratory, IRCCS Arcispedale Santa Maria Nuova, Reggio Emilia, Italya
; Virology and Microbiology Laboratory, Fondazione IRCCS Policlinico San Matteo, Pavia, Italyb
Many studies demonstrate that delayed proper therapy in bloodstream infections caused byStaphylococcus aureusincreases the mor-tality rate, emphasizing the need to shorten the turnaround time for positive blood cultures. Different techniques are currently avail-able, from phenotypic methods to more complex tests such as matrix-assisted laser desorption ionization–time of flight mass spec-trometry (MALDI-TOF), real-time PCR (RT-PCR), and fluorescence in situ hybridization using peptide nucleic acid probes (PNA FISH). This study evaluated the performance of theStaphylococcusQuickFISH BC test (QFT), a novel FISH methodology, compared with the direct tube coagulase test (DTCT) on blood cultures exhibiting Gram-positive cocci in clusters. A total of 173 blood cultures collected from 128 different patients were analyzed using the DTCT, evaluated after both 4 and 24 h, and the QFT. A total of 179 iso-lates were identified using the Vitek2 system. Thirty-five out of 35Staphylococcus aureuswere correctly identified by the QFT (sensitiv-ityⴝ100%), with a specificity of 100% (no green fluorescence was detected for strains different fromS. aureus). The DTCT was posi-tive after 4 h for 28 out of the 35 samples (sensitivityⴝ80%) and after 24 h for 31 out of the 35 samples (sensitivityⴝ88.57%). Among the remaining 144 isolates, one was then identified asCorynebacterium striatumand two asMicrococcus luteus. QFT identified 139 out of the 141 coagulase-negative staphylococci (CoNS) (sensitivityⴝ98.58%), showing again a specificity of 100% (no fluorescent red signals were detected for strains different from CoNS). We also discuss also the implementation process of this methodology in our setting, with particular emphasis on the workflow and the cost-effectiveness.
S
taphylococci are the microorganisms most frequently isolated from blood cultures. Bloodstream infections caused by Staphylo-coccus aureus(SA-BSI) are severe infections, with an incidence that varies greatly around the world: from 19.7 episodes/100.000 per-son-years in a Canadian study (1) to more than 50 episodes/ 100.000 person-years (2), with risk factors known to be advancing age, male gender, community onset, comorbidities (such as alcoholism, immunosuppression, cirrhosis, malignancies, and chronic renal failure), and frequent health care contacts (3). Dif-ferent studies demonstrate that delayed appropriate therapy in SA-BSIs is related to an increase in the mortality rate, as well as prolonging hospital stays and increasing costs (4,5).On the other hand, coagulase-negative staphylococci (CoNS) are the microorganisms most frequently isolated in clinical micro-biology laboratories, but they are often contaminants that raise the laboratory workload. Their treatment leads to antibiotic abuse, increasing microbial resistance. Moreover, the misinter-pretation of the role of CoNS causes side effects, underestimation of the true pathogens, and extra costs (6).
At present, different techniques are available to shorten the turnaround time (TAT) for positive blood cultures, e.g., matrix-assisted laser desorption ionization–time of flight mass spectrom-etry (MALDI-TOF), real-time PCR (RT-PCR), traditional tech-niques, and fluorescence in situ hybridization using peptide nucleic acid probes (PNA FISH). The MALDI-TOF approach seems promising, although the proper preparatory methods are still to be established and some variability in sensitivity is reported (different for Gram-positive and Gram-negative bacteria, provid-ing more reliable results for the latter) (7–9). A real-time PCR approach is available (Gene X-pert MRSA/SA; Cepheid, Sunny-vale, CA); the method is really easy to perform and seems to have
an exquisite sensitivity (10), but its main disadvantage is that it is too expensive, especially for settings managing a large amount of samples. The direct tube coagulase test (DTCT), performed from positive blood cultures, is used for discrimination betweenS. au-reusand CoNS strains; this test is cheap and easy to perform and possesses high specificity but a great inconsistency in sensitivity, ranging from 60% to 100% (11,12).
For different microrganisms, including staphylococci, PNA FISH was extensively studied as an in-house method (13,14) and is now commercially available in clinical practice, allowing for identification of these microorganisms directly from positive blood culture bottles (15,16). In our institution, we use the PNA-FISH from AdvanDx to presumptively identify yeasts and Gram-positive cocci in pairs or chains. Recently, a modification of the technique was developed (QuickFISH BC; AdvanDx, Woburn, MA) (QFT). This modified technique is currently (as of Septem-ber 2012) available only for staphylococci, and it allows for dis-tinction betweenS. aureus and CoNS with a simple and short procedure. The time for processing has been reduced, with faster fixation and hybridization phases (15 min), as well as removal of a wash step. The pathogen detection requires a maximum of 20 min, allowing the clinical microbiologist to report the obtained
Received7 August 2012 Returned for modification15 September 2012
Accepted15 October 2012
Published ahead of print24 October 2012
Address correspondence to E. Carretto, [email protected]. Copyright © 2013, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.02103-12
on May 16, 2020 by guest
http://jcm.asm.org/
identification (ID) together with initial Gram stain result. This technique has been recently validated (11). This study evaluates the performance of this new FISH methodology, comparing it with the DTCT evaluated after 4 h (DTCT4) and 24 h (DTCT24), on different sets of blood cultures showing Gram-positive cocci in clusters (GPCC), collected in a 3-month period in the IRCCS Ar-cispedale Santa Maria Nuova of Reggio Emilia, Italy, in order to assess its usefulness in clinical practice and implementation in routine laboratory workflow.
MATERIALS AND METHODS
Sample selection.Blood cultures were analyzed using the Bactec system (Becton Dickinson, Franklin Lakes, NJ) using the aerobic and anaerobic Bactec PLUS/F medium. During the study period (15 October 2011 to 29 December 2011), all blood cultures showing GPCC (alone or with other forms, such as Gram-negative bacilli or Gram-positive cocci in pairs or chains) were considered eligible. If a set from a patient (aerobic plus anaerobic bottles) was positive, a single bottle was evaluated (the first one which tested positive). If different sets from the same patient revealed GPCC, a single bottle for any set was analyzed, with a maximum of three analyses for a single pa-tient. DTCT4, DTCT24, and QFT were performed on all the samples in-cluded in the study. The samples were then cultured using standard tech-niques, as in CLSI document M47-A (17). The identification of the microorganisms grown from cultures was performed using the Vitek2 system (bioMérieux, Marcy l’Etoile, France), according to the manufacturer’s rec-ommendation. Supplementary identification tests were performed when needed. On a few strains for which identification was not unambiguous even after supplementary tests, we used automated ribotyping (DuPont Qualicon, Wilmington, DE) to achieve the proper species identification (18).
Direct tube coagulase test.Two or three drops (50l) of a positive blood culture broth were added in a tube containing 0.5 ml of rabbit plasma with EDTA (BBL, Cockeysville, MD) and incubated at 35°C. The tubes were read the first time after 4 h and then after 24 h to evaluate DTCT4 or DTCT24, respectively. Any clotting was interpreted as indica-tive ofS. aureus(12).
StaphylococcusQuickFISH BC test.The QFT was performed ac-cording to the procedure of the manufacturer. The procedure started immediately after the detection of GPCC in positive blood cultures. Drops of blood culture sample (100 to 150l) were added into an AdvanDx filter vial. A filter plunger was then inserted into the vial and pushed down to remove the resin beads. Ten microliters of sample was then transferred into the center of the sample area of an AdvanDx QuickFISH slide, previously placed on a workstation heated at 55°C⫾ 1°C. Samples were then fixed with two different solutions (QuickFix-1 plus QuickFix-2 at different times). After smear fixation, 1 drop of
StaphylococcusPNA blue was placed into the center of a coverslip, and then 1 drop ofStaphylococcusPNA yellow was added directly on top of the first one. PNA blue and PNA yellow were mixed until they pro-duced a uniform green color. The coverslip was then applied to the slide placed on the workstation heated at 55°C⫾1°C. This hybridiza-tion phase lasted 15 min. The slides were examined using a fluores-cence microscope with a 100⫻oil objective.S. aureuswas identified as bright green fluorescent cocci in multiple fields of view, whereas CoNS were identified as multiple red fluorescent cocci in multiple fields of view. The QFT slides have built-in positive and negative controls that were read together with the sample. QFT slides were read indepen-dently by different test operators who were blinded to the final results.
RESULTS
During the study period, a total of 173 blood cultures collected from 128 different patients were positive for GPCC. In 13 bottles the Gram stain revealed a mixed culture: we recognized 7 GPCC together with Gram-negative bacilli and 6 GPCC mixed with Gram-positive cocci in chains. QFT and DTCT were performed on all 173 samples.
As shown inTable 1, 179 isolates were identified from the se-lected blood cultures. Six bottles yielded two different staphylo-coccal strains: in one case, we isolatedS. aureusplusS. epidermidis, and in five cases we documented mixed cultures withS. epidermi-disandS. hominis. Thirty-five out of the 179 isolates were identi-fied asS. aureus, 1 isolate was aCorynebacterium striatumstrain which was misidentified by the Gram stain, 2 were identified as
Micrococcus luteus, and 141 strains were CoNS, withS. epidermidis
being the species most represented.
For 18 out of the 141 CoNS, Vitek2 was unable to provide an unequivocal species identification and supplementary pheno-typical tests were needed to achieve the proper identification. In five cases, even these tests did not provide a definitive result, and we analyzed these strains using automated ribotyping. This technique allowed us to correctly identify 2 Staphylococcus hominisstrains, 1Staphylococcus simulansstrain, and 1 Staph-ylococcus capitisstrain, whereas one strain was not identified even by this method (the highest similarity index was 0.64, with
S. epidermidisDUP-20388).
Considering the performance of the DTCT, among the 35S. aureusstrains, 28 were positive after 4 h of incubation (sensitivity for DTCT4⫽80% [28/35]) and 3 were negative after 4 h but positive after 24 h (raising the sensitivity for DTCT24 to 88.57% [31/35]), whereas four bottles remained negative after 24 h. These tests were negative, both after 4 h and after 24 h, for all CoNS. A sample containing bothS. aureusandS. epidermidistested positive by both DTCT4 and DTCT24 and was excluded for computa-tional evaluation of the sensitivity and specificity of the method for CoNS. Thus, regarding CoNS, the DTCT showed a sensitivity and specificity of 100%.
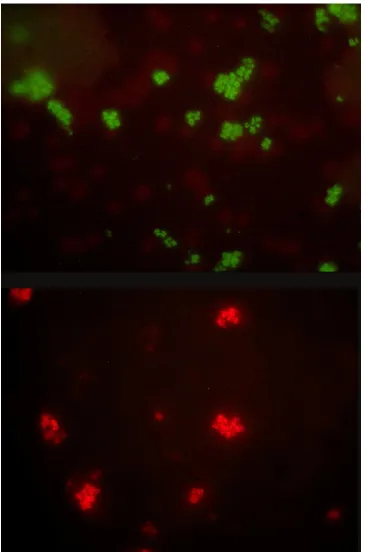
As regards the QFT, the images obtained were brilliant and easily interpretable (Fig. 1). No discrepancies between the QFT results and the phenotypic identification for S. aureus were detected (sensitivity and specificity forS. aureus⫽100%).
[image:2.585.298.545.76.236.2]Among the 144 GPCC different fromS. aureus, QFT showed a red fluorescence for 139 samples. The five samples that did not produce fluorescence were 2Micrococcus luteusstrains, 1 Coryne-bacterium striatum strain, 1 Staphylococcus simulans, and the
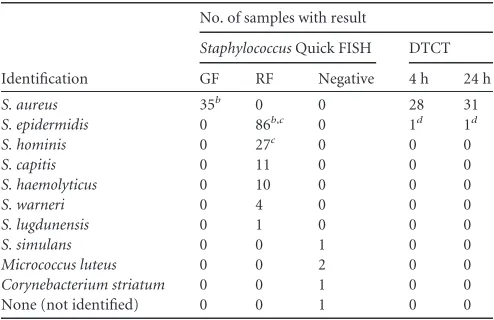
TABLE 1Study synopsisa
Identification
No. of samples with result
StaphylococcusQuick FISH DTCT
GF RF Negative 4 h 24 h
S. aureus 35b 0 0 28 31
S. epidermidis 0 86b,c 0 1d 1d
S. hominis 0 27c 0 0 0
S. capitis 0 11 0 0 0
S. haemolyticus 0 10 0 0 0
S. warneri 0 4 0 0 0
S. lugdunensis 0 1 0 0 0
S. simulans 0 0 1 0 0
Micrococcus luteus 0 0 2 0 0
Corynebacterium striatum 0 0 1 0 0
None (not identified) 0 0 1 0 0
aGF, green fluorescence; RF, red fluorescence.
b
One sample yieldedS. aureusandS. epidermidis.
cFive samples yieldedS. epidermidisandS. hominis.
d
One sample yielding bothS. aureusandS. epidermidiswas positive by the DTCT at 4 h
and 24 h.
on May 16, 2020 by guest
http://jcm.asm.org/
staphylococcal strain we did not manage to identify. The overall sensitivity of the QFT was 97.14% and increased to 98.58% if
Micrococcaceaewere excluded from computation (Table 2). The specificity was 100%, since no fluorescent red signals were de-tected in samples yielding strains different from CoNS.
DISCUSSION
QuickFISH (AdvanDx, Woburn, MA) is a modification of tradi-tional FISH technique, using a simpler and faster protocol. This innovation is now FDA cleared and marked for EC-IVD (a Euro-pean Commission mark forin vitrodiagnostic medical devices)
FIG 1QFT. (Top) green fluorescence ofStaphylococcus aureus; (bottom) red fluorescence of aStaphylococcus epidermidisstrain.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.111.477.65.617.2]and is available for clinical routine use. It has to be expected that the manufacturer will broaden the number of pathogens this new technology can detect. Our study represents an early clinical lab-oratory evaluation of the first product available on this platform after the validation paper of Deck et al. (11).
This molecular procedure is based on the PNA FISH method-ology with shortened fixation and hybridization phases and elim-ination of the washing steps. In our experience the new Quick-FISH appeared quick, reliable, and easy to perform, and it allowed us to reduce TAT compared with those of the DTCT and tradi-tional PNA FISH. Using this method, the microbiologist is able to provide the clinicians with the results of both Gram stain and the presumptive identification of Staphylococcus aureus in half an hour from the bottle positivity.
The performance of the QFT in distinguishingS. aureusand CoNS appeared very good. The five strains which gave a negative result by QFT were 1Corynebacterium striatumstrain (errone-ously considered at Gram stain as GPCC), 2Micrococcus luteus
strains, 1Staphylococcus simulansstrain (which is known not to be targeted by the probes used for the QFT), and 1 staphylococcal strain that we were unable to identify at the species level even using ribotyping techniques. We assume that it could be a species hardly ever isolated in clinical practice, because its fingerprint is not in-cluded in the Riboprinter database, which showed good perfor-mances on clinical CoNS (18). According to these considerations, the sensitivity of the method in CoNS detection is 97.14%, but if we exclude for the computation the twoMicrococcus lutesstrains, the performance of the QFT increases to 98.58% and appears even more impressive. The data are in overall agreement with the sen-sitivity revealed in the validation study (11).
An excellent agreement between the QFT and a standard lab-oratory technique such as the DTCT was demonstrated. As re-gards the DTCT, a wide range of sensitivity is reported in different times and in different papers. Our data are in range with those published in the majority of the studies (11,19–21). It has to be noted that among the four strains which gave negative results after 24 h, in three cases the test repeated the day after provided a pos-itive result, confirming in our experience some kind of intrinsic variability of the method. Thus, our experience confirms that al-though the DTCT is cheaper, its sensitivity was lower than that of the QFT. Furthermore, it should be considered that the DTCT value is poor if the test is performed on the blood cultures that automated instruments reveal as positive in the afternoon, be-cause the results, even after the 4-h analysis, are available only after the closing time of a laboratory that has a workflow of 12 h/day.
To date, different techniques are available to shorten the TAT for positive blood cultures (MALDI-TOF, RT-PCR, traditional techniques, and PNA FISH). In a worldwide period of economic troubles and funding shortage, the microbiologist should make an effort to evaluate the best pharmacoeconomic approach in pro-viding clinicians with preliminary results able to correctly address empirical therapy. These approaches cannot be easily standard-ized because of the high variability of the settings: the laboratory settings (opening time, mixed laboratories, number of cultures processed, automation level, etc.) and the type of the hospital (number of acute-care beds, patients’ typology, numbers of inten-sive care units or transplant units, etc.) should be taken in account carefully.
In general, MALDI-TOF seems a promising tool to allow the presumptive identification of strains directly from blood cultures, but strong validation studies are required to focus the limitations of this technique (if any) and its proper use (7–9).
A previous paper of Brown and Paladino focused on the cost-effectiveness of RT-PCR for methicillin-resistantS. aureus
(MRSA) in reducing mortality rates while being less costly than empirical therapy (22), whereas the work of Hermsen et al. pointed out that DTCT4 and DTCT24 were more cost-effective than RT-PCR and PNA FISH, respectively (16). However, it has to be emphasized that the cost of reagents may vary from country to country and, sometimes, in the same country, from hospital to hospital.
Our clinical microbiology laboratory supports a tertiary hos-pital (1,000 acute care beds), three small hoshos-pitals (both acute care and long-term care beds), and some health care facilities (with long-term care beds). Medical wards are the most represented. More than 12,000 blood culture sets are performed each year (13.42% positive), and the laboratory is open 12 h/day. MALDI-TOF is not still available, whereas Gene X-pert MRSA/SA (Cepheid, Sunnyvale, CA) is available and used. In our setting, the cost of PNA-FISH is two-thirds of the cost of RT-PCR, whereas the DTCT appears unequivocally to be the cheapest test. Cur-rently, the model used in our setting for blood cultures positive for GPCC is based on the DTCT if the positivity is detected in the morning, followed by a RT-PCR for samples positive by the DTCT at 4 h, in order to confirm theS. aureusidentification and evaluate the resistance to methicillin. If a blood culture is positive in the afternoon, it could be more cost-effective to use the QuickFISH to presumptively identifyS. aureusand on these samples perform the RT-PCR. If it is assumed that the future cost of the QFT will be equal to or cheaper than that of PNA FISH, the possibility to use the QFT, which demonstrated a very good sensitivity and speci-ficity forS. aureuswith the advantage of being extremely rapid, will allow work on GPCC-positive samples until the late afternoon for laboratories that have a 12-h/day workflow.
Finally, it has to be emphasized that the hands-on time of the QFT is less than 5 min; the technique is easy, and the slides can be prepared by technicians after only a short training period. The introduction of the method in the laboratory routine therefore has a low implication in modifying the usual workflow.
[image:4.585.40.287.87.184.2]In conclusion, the QuickFISH technology appears robust and reliable, with the major advantage of providing results in half an hour. It can be expected that this technique will be used routinely for all blood cultures to detect all the different pathogens currently detected by traditional PNA FISH, allowing major advantages in reporting preliminary identification together with the Gram stain.
TABLE 2Comparison between the final IDs obtained by conventional techniques and QFTa
Organism(s)
No. of samples with result
Sensitivity of QFT (%) Standard ID
(culture)
QFT
GF RF NF
S. aureus 35 35 100
CoNS 141 139 2 98.56
Others 3 3 100
Total 179 35 139 5
a
GF, green fluorescence; RF, red fluorescence; NF, absence of fluorescence. Other
strains are 2Micrococcus luteusstrains and 1Corynebacterium striatumstrain.
on May 16, 2020 by guest
http://jcm.asm.org/
The results presented in this study confirm the very good perfor-mance of the test on staphylococci and encourage the use of this methodology instead of more traditional FISH.
ACKNOWLEDGMENTS
None of us has any financial interest in AdvanDx, Inc., or received finan-cial support to perform this study.
Kits and disposables were kindly provided by AdvanDx A/S, Denmark. We especially thank Henrik Aspe, Steen Hesthaven, and Lidija Horvat for their helpful support throughout the study.
This work was partially supported by grants from the Scientific Com-mittee of the IRCCS Arcispedale Santa Maria Nuova, Reggio Emilia, to E. Carretto.
REFERENCES
1.Laupland KB, Ross T, Gregson DB.2008.Staphylococcus aureus blood-stream infections: risk factors, outcomes, and the influence of methicillin resistance in Calgary, Canada, 2000 –2006. J. Infect. Dis.198:336 –343. 2.Klevens RM, Morrison MA, Nadle J, Petit S, Gershman K, Ray S,
Harrison LH, Lynfield R, Dumyati G, Townes JM, Craig AS, Zell ER, Fosheim GE, McDougal LK, Carey RB, Fridkin SK, Active Bacterial Core surveillance (ABCs) MRSA Investigators.2007. Invasive methicil-lin-resistantStaphylococcus aureusinfections in the United States. JAMA
298:1763–1771.
3.van Hal SJ, Jensen SO, Vaska VL, Espedido BA, Paterson DL, Gosbell IB. 2012. Predictors of mortality inStaphylococcus aureusbacteremia. Clin. Microbiol. Rev.25:362–386.
4.Paul M, Kariv G, Goldberg E, Raskin M, Shaked H, Hazzan R, Samra Z, Paghis D, Bishara J, Leibovici L.2010. Importance of appropriate empirical antibiotic therapy for methicillin-resistantStaphylococcus au-reusbacteraemia. J. Antimicrob. Chemother.65:2658 –2665.
5.Paul M, Shani V, Muchtar E, Kariv G, Robenshtok E, Leibovici L.2010. Systematic review and meta-analysis of the efficacy of appropriate empiric antibiotic therapy for sepsis. Antimicrob. Agents Chemother.54:4851– 4863.
6.van der Heijden YF, Miller G, Wright PW, Shepherd BE, Daniels TL, Talbot TR.2011. Clinical impact of blood cultures contaminated with coagulase-negative staphylococci at an academic medical center. Infect. Control Hosp. Epidemiol.32:623– 625.
7.Meex C, Neuville F, Descy J, Huynen P, Hayette MP, De Mol P, Melin P.2012. Direct identification of bacteria from positive anaerobic BacT/ Alert(R) blood cultures by MALDI-TOF MS: MALDI Sepsityper(R) kit (Bruker) versus in-house saponin method for bacterial extraction. J. Med. Microbiol.61:1511–1516.
8.Saffert RT, Cunningham SA, Mandrekar J, Patel R.2012. Comparison of three preparatory methods for detection of bacteremia by MALDI-TOF mass spectrometry. Diagn. Microbiol. Infect. Dis.73:21–26.
9.Wüppenhorst N, Consoir C, Lorch D, Schneider C.2012. Direct iden-tification of bacteria from charcoal-containing blood culture bottles using matrix-assisted laser desorption/ionisation time-of-flight mass spectrom-etry. Eur. J. Clin. Microbiol. Infect. Dis.31:2843–2850.
10. Wolk DM, Struelens MJ, Pancholi P, Davis T, Della-Latta P, Fuller D, Picton E, Dickenson R, Denis O, Johnson D, Chapin K.2009. Rapid detection ofStaphylococcus aureusand methicillin-resistantS. aureus
(MRSA) in wound specimens and blood cultures: multicenter preclinical evaluation of the Cepheid Xpert MRSA/SA skin and soft tissue and blood culture assays. J. Clin. Microbiol.47:823– 826.
11. Deck MK, Anderson ES, Buckner RJ, Colasante G, Coull JM, Crystal B, Della Latta P, Fuchs M, Fuller D, Harris W, Hazen K, Klimas LL, Lindao D, Meltzer MC, Morgan M, Shepard J, Stevens S, Wu F, Fiandaca MJ.2012. Multicenter evaluation of theStaphylococcus Quick-FISH method for simultaneous identification ofStaphylococcus aureusand coagulase-negative staphylococci directly from blood culture bottles in less than 30 minutes. J. Clin. Microbiol.50:1994 –1998.
12. Qian Q, Eichelberger K, Kirby JE.2007. Rapid identification of Staphy-lococcus aureusin blood cultures by use of the direct tube coagulase test. J. Clin. Microbiol.45:2267–2269.
13. Oliveira K, Brecher SM, Durbin A, Shapiro DS, Schwartz DR, De Girolami PC, Dakos J, Procop GW, Wilson D, Hanna CS, Haase G, Peltroche-Llacsahuanga H, Chapin KC, Musgnug MC, Levi MH, Shoe-maker C, Stender H.2003. Direct identification ofStaphylococcus aureus
from positive blood culture bottles. J. Clin. Microbiol.41:889 – 891. 14. Oliveira K, Procop GW, Wilson D, Coull J, Stender H.2002. Rapid
identification ofStaphylococcus aureusdirectly from blood cultures by fluorescence in situ hybridization with peptide nucleic acid probes. J. Clin. Microbiol.40:247–251.
15. Hensley DM, Tapia R, Encina Y.2009. An evaluation of the AdvanDx
Staphylococcus aureus/CNS PNA FISH assay. Clin. Lab. Sci.22:30 –33. 16. Hermsen ED, Shull SS, Klepser DG, Iwen PC, Armbrust A, Garrett J,
Freifeld AG, Rupp ME.2008. Pharmacoeconomic analysis of microbio-logic techniques for differentiating staphylococci directly from blood cul-ture bottles. J. Clin. Microbiol.46:2924 –2929.
17.CLSI.2007. Principles and procedures for blood cultures. Approved guideline. CLSI document M47-A. CLSI, Wayne, PA.
18. Carretto E, Barbarini D, Couto I, De Vitis D, Marone P, Verhoef J, De Lencastre H, Brisse S.2005. Identification of coagulase-negative staphy-lococci other thanStaphylococcus epidermidisby automated ribotyping. Clin. Microbiol. Infect.11:177–184.
19. Goldstein J, Roberts JW.1982. Microtube coagulase test for detection of coagulase-positive staphylococci. J. Clin. Microbiol.15:848 – 851. 20. Lagacé-Wiens PR, Alfa MJ, Manickam K, Karlowsky JA.2007.
Thermo-stable DNase is superior to tube coagulase for direct detection of Staphy-lococcus aureusin positive blood cultures. J. Clin. Microbiol.45:3478 – 3479.
21. Sturm PD, Kwa D, Vos FJ, Bartels CJ, Schulin T.2008. Performance of two tube coagulase methods for rapid identification ofStaphylococcus au-reusfrom blood cultures and their impact on antimicrobial management. Clin. Microbiol. Infect.14:510 –513.
22. Brown J, Paladino JA.2010. Impact of rapid methicillin-resistant Staph-ylococcus aureuspolymerase chain reaction testing on mortality and cost effectiveness in hospitalized patients with bacteraemia: a decision model. Pharmacoeconomics28:567–575.