ANALYSIS OF THE EFFECTS OF TRANSDERMAL MAGNESIUM-CHLORIDE ON MUSCLE FORCE, ENDURANCE, AND RECOVERY IN RECREATIONALLY ACTIVE COLLEGE-AGED INDIVIDUALS WITH PRIOR RESISTANCE TRAINING
– METHODOLOGICAL CONSIDERATIONS
by
Andrei Michael Sergeyev
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with honors in the Department of Exercise and
Sport Science
2020
Thesis Committee:
Dr. Erik D. Hanson
Dr. Joshua Beaver
Table of Contents
CHAPTER 1: INTRODUCTION...4
Magnesium Overview...4
Magnesium in the Body...5
Biochemistry of Magnesium...6
Oral Magnesium Supplementation...6
Transdermal Magnesium-Chloride...7 Research Questions...9 Hypotheses...9 Limitations...10 Delimitations...10 Significance...11
CHAPTER 2: REVIEW OF LITERATURE...12
Magnesium...12
Magnesium Availability...13
Magnesium and Exercise Performance...15
CHAPTER 3: METHODOLOGY...17
Participants...17
Design and Procedures...17
Pilot Procedures...18
Final Procedures...20
Study Evaluations and Measurements...23
CHAPTER 4: RESULTS...26
Participants...26
Pilot 1 – Transdermal Magnesium Supplementation Had No Effect on Muscle Function...26
Pilot 2 – Addition of Fat Gripz™ Increases Fatigue of Forearms...28
Pilot 3 - Laying Prone Improves Isometric Forearm Contraction...29
Pilot 4 – Lengthening the Time Interval Between Contractions Reduces Force Decline...31
Pilot 1...32
Pilot 2...34
Pilot 3...36
Pilot 4...37
Implications...38
Limitations and Strengths...38
Conclusion...40
CHAPTER 1: INTRODUCTION
The nutrition supplement market has been an exponentially expanding market1 that
is already valued at $50 billion2 annually. Nearly half of Americans claim to use them3,
yet most of the supplements on the market are unproven to work4. In athletics, being the
best is often separated by a few centimeters or fractions of seconds, therefore, athletes will often take extra measures to ensure that they have every advantage they can get, hoping to gain that edge. A potential consequence of this mindset is that the athlete will often times use products that are unstudied or unsafe. One category of these growing supplements is magnesium, with approximately 25% of Americans self-reporting magnesium supplementation3. Despite the fact that magnesium is the second most
abundant cation in the body, the research assessing the specific effects of magnesium supplementation in athletics has gathered little scientific interest.
Magnesium Overview
Magnesium is an essential atom that is used as a co-factor in more than 300 enzymatic processes, several of which are essential for metabolism and exercise performance including glycolysis5–7. Given its importance in regulating charges the
synthesis of adenosine triphosphate (ATP) from adenosine diphosphate (ADP), a correlation between magnesium and energy availability could potentially be expected6.
of the American population8,9. Magnesium deficiency has been linked to gastrointestinal
issues, renal abnormalities, many endocrine and metabolic syndromes, such as diabetes mellitus, and has been linked to osteoporosis, muscular weakness and tremors, cardiac arrhythmia, hypertension, and atherosclerotic vascular syndrome8. Many magnesium
supplements today are taken orally and are accompanied with several side effects including gastrointestinal discomfort, which may limit its usage prior to an athletic even or workout10. Despite its importance to homeostasis, most individuals are unaware they
are magnesium deficient, as the test for the condition is not included in the standard electrolyte test and requires a specific test to determine9.
Magnesium in the Body
Magnesium is primarily stored within the cells, 90%-95% of which is bound to ligands such as ATP, ADP, citrates, nucleic acids, and other proteins8. 60% of
the stored magnesium in the body is stored in the skeleton, 39% intracellularly (majority of this is found in skeletal muscle) and the remaining 1% is stored extracellularly. Serum levels are typically 0.7-1.0 mmol/L and rarely change even if the rest of the body is magnesium deficient11,12. The main form of absorptivity of the magnesium cation is
dependent on diffusion through a electrolyte gradient; therefore, the amount of the cation that enters the cell is based primarily on the extracellular concentration of magnesium available to be transported into the cell13. Therefore it should be expected that as the
Biochemistry of Magnesium
Magnesium is a vital cation in the human body and perhaps the with a notable role in energy production. It is used as a cofactor, stabilizing the charge of several enzymatic processes through glycolysis, gluconeogenesis, and the Krebs Cycle6. In the majority of
cases, the charges stabilized are essential for the creation of valuable oxidizing agents to be used in the electron transport chain, as well as, in the synthesis of ATP6. Through
exercise, as ATP is used, the demand is subsequently increased. As such, the metabolic pathways involved in energy production need to increase in response6,14–16. While there
are many roles magnesium plays in the myriad enzymatic processes of metabolism, the most prominent is it’s electrostatic regulation of the phosphate groups added and removed during ATP anabolism and catabolism6,7,17. Magnesium has been known to
increase in functionality as it increases in abundance,7 including being closely linked to
the kinetics and stabilization of the creatine phosphate reaction and several enzymatic processes in both anaerobic and aerobic glycolysis, including the formation of pyruvate, an essential metabolite in regards to glycolysis and the citric acid cycle6,7,17,18. It can
therefore be concluded that if more magnesium is introduced to the tissue, then there will be more metabolic activity6,7,17.
Oral Magnesium Supplementation
magnesium to increased athletic performance in the measures of muscle force and endurance 23,24 (see Magnesium and Exercise Performance). However, oral magnesium
may not practical in an athletic setting. Oral magnesium’s ability to be absorbed in the intestine varies between 24-76%25. This could be unreliable for an athlete would be
unable to predict the amount of magnesium they are supplementing and who also would have to wait for the magnesium to enter the blood stream through the digestive system. Furthermore, oral magnesium also comes with side-effects that include stomach irritation, vomiting, and diarrhea26. These side-effects can be severe limiting factors and can reverse
any benefit the supplement may have during an athlete’s performance.
Transdermal Magnesium-Chloride
Transdermal magnesium-chloride (tMgCl2) could be an effective and risk-less
method of delivering magnesium to the tissue for use during exercise. The use of this product has multiple anecdotal claims touting its effectiveness, including claims from Jason Beaulieu (Strength and Conditioning Coach of the UNC Women’s Basketball team) and Travis Mash (former world champion powerlifter, current weight-lifting coach), stating that they perceived a noticeable difference in their muscle recovery when using the supplement. However, supporting scientific evidence of these claims is currently lacking. To date, 2 studies have been done looking at the effects of this supplement, one of these studies27 found that there was no significant difference in the
Overview and Biochemistry of Magnesium), 5 minutes may be insufficient time for the product to effectively pass through to skin the underlying tissue; furthermore, given that magnesium effects the metabolic pathways of predominately short-term energy sources, this study looked at the effects of aerobic exercise (3 minute bouts of increasing resistance), which would utilize longer term energy usage, which magnesium may have a lesser effect onto. Based on these factors, this study looking at acute effects of this supplement on muscle endurance may not have used the best methods to see the result they were looking for.
The other study that examined the effects of tMgCl2 (Alzer, et al, unpublished
data) applied supplement over 4 days and tested the effects of muscle soreness and force recovery following eccentric exercise. The initial data from this study suggests that there does not seem to be a significant chronic effect of tMgCl2 on muscle soreness or
recovery. However, as with the previous study, these methods may not have been the ideal conditions for positive effects with use of this supplement. The chronic effects of magnesium supplementation may not lead to an increase in magnesium available for exercise, some studies showing that the amount of available magnesium may even decrease due to a feedback loop leading to increased storage and excretion20. Studying the
acute magnesium, as soon as it becomes available to the cells may be the best course of action of testing the effectiveness of this supplement.
Presently, there have been no studies that test the effectiveness of a tMgCl2
based on the roles that magnesium plays in several metabolic pathways, its ability to permeate effectively to the tissue, as well as already being studied to improve muscle force and endurance, an acute application of a tMgCl2 supplement can be expected to
improve muscle performance. In order to determine transdermal magnesium chloride’s role on muscle force, recovery, and endurance, this study sought to iron out some of the methodological considerations in finding the best protocol of testing these
Research Questions
The overarching research question for the broader study that this project was part of was to determine if tMgCl2 increase maximal isometric force production, enhance force
recovery following a forearm fatigue protocol, and increase muscle endurance and decrease perceived maximal exertion compared to placebo? To do this, we sought to determine the following methods questions.
1. How might posture and arm orientation affect the testing of the maximum isometric force in the forearm?
2. Are repeating isometric holds an effective method of fatiguing the forearms?
3. Are isometric strength tests with a time interval between contractions an effective way of measuring muscle recovery?
1. Arm position will not effective and posture will not affect the testing of maximum isometric force in the forearm
2. Repeated isometric holds are not an effective method of fatiguing the forearms. 3. Repeated isometric strength tests are not an effective way of measuring muscle recovery.
Limitations
1. Lack of true experimental control such as controlling for the dominant versus non-dominant arms or testing with the magnesium supplement versus a placebo.
2. Since magnesium deficiency is such a common condition compounding with the difficulty to test, it will not be known for certain whether or not we are testing magnesium deficient individuals.
3. If subjects are accustomed to a high magnesium diet, including the foods they consume or through supplements, they may not stop this for the intervention.
Delimitations
1. During their familiarization session, they will be asked to disclose whether or not they have any known magnesium deficiency.
amount of magnesium had been consumed, they will either be excluded or their testing rescheduled.
Significance
CHAPTER 2: REVIEW OF LITERATURE
Magnesium
The therapeutic role of magnesium has been well known and has been used dating back centuries with the Dead Sea. Magnesium has been shown to effectively treat eclampsia and preeclampsia, uncommon ventricular tachycardia, asthma and many other conditions28. Furthermore, its role in exercise performance has also been well
documented. Magnesium supplementation in gerbils has proved to delay muscle fatigue, enhance glucose utilization, as well as increase the swimming time significantly, showing that it also increases endurance29. In humans, supplemental magnesium has been shown
to increase muscle strength and power; increasing peak knee extension by 20% (a significant amount), suggesting a key role of magnesium in the many glycolytic metabolism actions23,30. Supplemental magnesium has been proven to improve cellular
function as well; the serum total creatine kinase and creatine kinase isoenzyme MB, and serum lactate concentration all decreased in magnesium deficient female rowers who received supplemental magnesium salts 30. These studies have been made in magnesium
deficient populations, there is conflicting evidence regarding the effectiveness of supplemental magnesium in population with healthy magnesium levels. According to one study, supplemental magnesium in a population of marathon runners with adequate magnesium status did not have any improvements in cellular or muscle function when given supplemental magnesium 30,31. However, having adequate magnesium levels has
regulation of the uptake and release of hormones, nutrients, and neurotransmitters which would help maintain cell membrane potential 32.
Magnesium Availability
Oral magnesium has shown to potentially increase force production in handgrip strength tests, countermovement jumps, maximal quadriceps torque, and isometric trunk flexion 23,33. Oral magnesium is however associated with gastrointestinal side effects
which may limit its use immediately prior to an athletic performance. Studies have shown that the tMgCl2 gets 100% absorbed through the skin34. Despite this, transdermal
application of magnesium-chloride has had varying evidence regarding its ability to reach the serum, where magnesium levels are usually measured32,34. However there is evidence
that shows that the application of magnesium-chloride leads to an increase in intra-cellular magnesium levels35. This would suggest that through application of
magnesium-chloride, the magnesium would reach and be available to the cells. The intracellular magnesium concentration is the significant contributing factor in regards to muscle function and recovery.
In this study a transdermal magnesium cream will be used. When applied directly to the skin, a magnesium-chloride cream showed to permeate significantly through the skin, having the most availability 1-2 hours post application34. This transdermal
One potential issue when testing the effects of magnesium in an acute manner is whether or not the magnesium may permeate throughout circulation and affect a region that is not being observed. Previous research suggests that in an athletic population, magnesium applied transdermally does not increase serum levels significantly, suggesting that the magnesium may not circulate through the body in a fashion that would affect a non-treated part of the body36.
The idea of magnesium supplementation improving bodily functions is a complicated one to take on simply because magnesium is already an essential ion in the human body, the body is already using it all times, therefore the question is more about whether or not the body uses the extra magnesium to do what it always does more efficiently or does more than it usually does. There are more than 300 essential enzymatic reactions in the human body in which magnesium is essential37. Despite its importance,
there is a possibility that nearly half of Americans are magnesium deficient 9. Magnesium
deficiency may lead to poor muscle recovery as well chronic inflammatory responses in the body as the cellular repair and growth pathways typically initiated after muscle contraction and damage may be attenuated 32. The current recommended dietary intake of
magnesium for a male aged 18-40 years old is 400 mg/day 9. However, a study conducted
supplementation. The method of supplementation has historically been through oral injection of magnesium supplements or injection of foods high in magnesium such as whole wheat, spinach, and various nuts. However, the particular method that leads to an increase in muscle performance has not been firmly established5,28,29,34. Magnesium
toxicity is an extremely rare condition that occurs only when magnesium concentrations reach 5-15 mmol/l in the plasma, which may cause cardiac arrest, muscular paralysis, and respiratory arrest. This plasma concentration is extremely high and it is unlikely to be reached unless the individual already has hypocalcemia, hyperkalemia, and uremia13.
Magnesium and Exercise Performance
Furthermore, magnesium is known to play a key role in the active transport of calcium and potassium ions into the cell; these both play a key factor in nerve impulse conduction, muscle conduction, vasomotor tone, and normal heart rhythm26. All of which
are linked to increased muscle performance, linking magnesium availability with increased muscle force, endurance, and recovery39,40.
One such study indicated that oral magnesium supplementation increased muscle force production during handgrip strength, countermovement jumps, maximal quadriceps torque, and isometric trunk flexion23. In this study, 2 groups subjects aged 18-30, with no
supplementation had an average of 105% more magnesium ingested (144% of the Recommended Daily Allowance of ~310 mg). Strength increased in both groups, but, the magnesium supplemented group, saw a significantly greater increase in force following the strength training. This study also used adjusted measures to ensure that the differences in force can be directly attributed to magnesium.
In another study24 with a 2 day design, a group of 13 subjects aerobically trained
athletes, aged 29-44 were either placed in an acute (1-week) or chronic (4 week) strategy, where they would either get a magnesium-citrate supplement (300 mg/day elemental Mg2+) or a placebo. They were asked to perform 80% of their 1-repetition maximum until
failure. The results of this study showed that there was no decrease in force outputs with the magnesium supplementation, however, the control group saw a 17.7% decrease in force production in the acute intervention group24, leading to the conclusion that the
CHAPTER 3: METHODOLOGY
Participants
The inclusion criteria for the parent study included healthy men and women between the ages of 18 and 35, who were recreationally active (30+ minutes of exercise at least twice a week), and who had prior experience with resistance training or gripping exercise (e.g. rock climbing and gymnastics). The exclusion criteria included anyone with an 1) acute wrist or forearm injury resulting in surgery in the six months prior, 2) known magnesium deficiency or who was currently taking magnesium supplements, 3)taking chronic pain medication, 4) history with cardiovascular or respiratory conditions which were exacerbated by exercise, 5) who was currently taking diuretics or glucocorticoids in the six months prior, 6) who had orthopedic surgery on an upper extremity in the 6-8 months prior, or 7) had a metabolic condition that was exacerbated by exercise. For the methodological validations, a total of 14 participants were tested between all pilot trials, 12 male (M) and two female (F). In the first experiment four participants were tested (4 M); in the second four participants participated (3 M, 1 F); in the third pilot there were four participants (3 M, 1 F); and in the final experiment there were two participants (2 M).
Design and Procedures
arm, condition A, (2) nondominant arm, condition A, (3) dominant arm, condition B, or (4) nondominant arm, condition B. Condition A was the cream and spray labeled A, and Condition B was applying the cream and spray labeled B. The creams were labeled by the manufacturer prior to shipment and their contents will only be revealed at the conclusion of data collection. One condition contained the magnesium-chloride and another contained a placebo. They were placed into their selected groups by a random number selection selecting from a random pool.
Pilot Procedures
To determine the best methodology to test our research questions, a series of pilot tests were carried out, where each protocol was adjusted to compensate for any issues that became apparent through the preceding test. In all of the pilot tests, participants would come in twice. The first visit would be the control test, where all tests were done without the MgCl2 supplement. For the first experiment, the participants would return
of rest in-between. This was immediately followed by the recovery protocol, which had the participant in the same posture that they completed the maximum force protocol and giving a two second maximum contraction every 30 seconds for five minutes. On the experimental testing days, there was a 30 minute absorption period that preceded all of the testing.
The second round of pilot testing exclusively saw changes in the fatigue protocol; the maximum isometric force and the recovery protocols remained the same. The fatigue protocol now consisted of the participant hanging from the pull up bar, now equipped with a Fat Gripz™, a thick, foam-like sleeve that can be placed around a bar; this was done to ensure that the targeted muscles (in the forearm) were the ones that were being fatigued. The rest of the protocol remained the same. They would hang from the pull up bar three times until failure with one minute of rest in-between each trial.
isometric strength protocol, where the participant would lay prone, with their shoulder in 90 degrees of flexion, giving a two second maximum contraction every 30 seconds for five minutes. Beginning with this pilot test, the absorption period for the magnesium chloride supplement was increased from 30 minutes to 60 minutes.
The final round of pilot testing all took place on the same day, with no magnesium supplementation. The procedures were identical to the third round of pilot testing with the sole difference of the recovery protocol consisting of a two second contraction every 45 seconds, rather than 30 seconds, for five minutes.
Final Procedures
complete along with a list of magnesium rich foods that should have been avoided 24 hours prior to their second visit.
Figure 1. Timeline of Events for Intervention Testing (Day 2)
Study Evaluations and Measurements
Perceived Muscle Fatigue Visual Analog Scale
A 0-10 scale was presented to the participants with both the control and experimental parameters to determine the participants perceived muscle fatigue. 0 is no fatigue at all and 10 is extreme fatigue.
Treadmill Walking Warmup
Participants walked on a treadmill at a speed of 2.5 mph and at an incline of 7 degrees, to increase whole body circulation in preparation for the intervention protocol to ensure peak performance and decrease injury risk. This test was performed twice on Visit 2, once before the baseline maximum strength testing and once after the 1-hour absorption period.
Isometric Strength Test
twice during the intervention meeting; once to assess their baseline maximum strength and the other to determine their maximum strength following the supplement application.
Forearm Fatigue Protocol
The 3 sets, holding a dumbbell equipped with Fat Gripz™ until failure with 1 minute between each repetition acted as a forearm endurance test. Based on how long the participants were able to hang on to the dumbbell each time, this test wasperformed bilaterally, following the application of the supplement. The participants’ forearms are meant to get fatigued through this protocol so that their recovery can subsequently be tested (see Recovery Protocol).
Recovery Protocol
While prone with their elbow set at 0 degrees, participants performed one maximum isometric strength tests every 45 seconds for 5 minutes. This test was used to determine if and how quickly the participants’ strength could return to their maximum strength. This was performed bilaterally, following the participants’ fatigue protocol.
Pain and Discomfort Scale
Statistical Analysis
CHAPTER 4: RESULTS
Participants
Participants were active, healthy men with no history of wrist or forearm surgery
within the last 6 months. They all were recreationally active and participated in resistance training. On average the participants (n=14) were 170.2 cm tall and weighed 75.4 kg.
Through this preliminary testing, each protocol was tested and shifted in order to determine a feasible method of testing maximum isometric force in the forearm, forearm muscle fatigue and endurance, and forearm muscle recovery. The statistics were
determined for each of the maximum isometric force and total fatigue time protocols through a paired t-test; and the statistics for the fatiguing time per trial and the recovery protocol were done via 2-way repeated measures ANOVA.
Pilot 1 – Transdermal Magnesium Supplementation Had No Effect on Muscle Function
Figure 2. Maximum isometric force produced by forearm with and without magnesium supplementation (n=4).
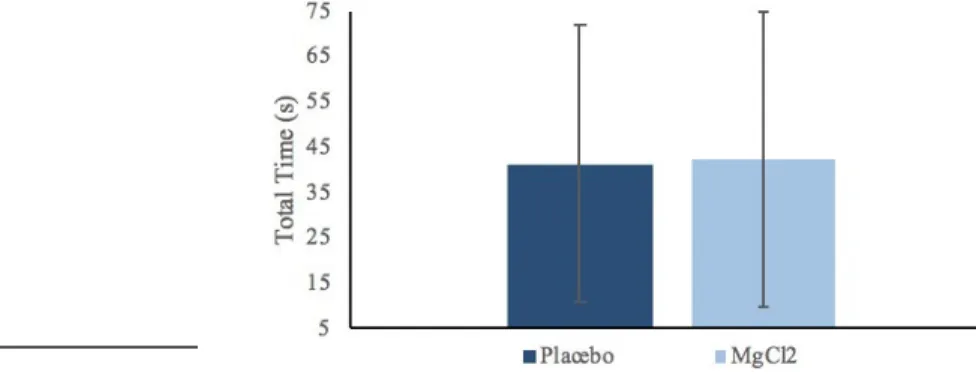
Figure 4. Hang time decreases in subsequent sets and is not affected by magnesium supplementation (n=4).
*P<0.05 versus trial 1
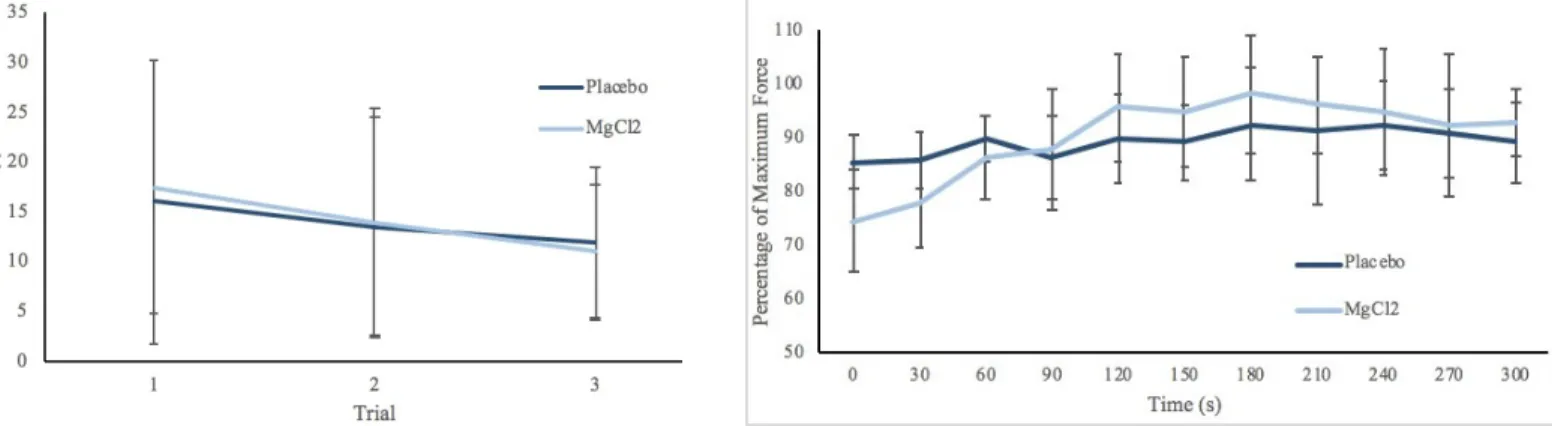
Figure 5. Recovery of maximal isometric force over 5 minutes. Data are presented relative to peak isometric strength (n=4).
The maximum force produced by the forearms was similar the same with and without the magnesium supplementation (P=0.943, Figure 2). The fatigue protocol saw an increase in total time of the three body weight hangs (P=0.131, Figure 3). In the magnesium supplemented individuals, there was a steady decline through all three trials, but there was a slight increase in the hang times from the second to the third body weight hang for the placebo. Overall, there was a difference over time for the protocol (P=0.003, Figure 4). Based on the statistical parameters, there was not a significant difference
between conditions, however, with a greater sample size a difference may be seen (P=0.131). The recovery slopes were similar for both the supplemented and the non-supplemented groups. The non-non-supplemented group began at a higher relative force than the supplemented group. The supplemented group had a more steady positive trend of recovery while the non-supplemented group had a positive trend to begin with, but this
*
trend was lost following 120 s; there was a difference in the participants’ force production over time (P=0.005), but no difference between conditions (P=0.684), or the conditions x time interaction (P=0.546, Figure 5). The post hoc did not indicate significance between any specific time points. There was a decrease in maximal force following the fatigue protocol for both the supplemented (34.8%±13.6 decrease, P=0.004) and placebo groups (24.5%±10.7 decrease, P=0.012).
Pilot 2 – Addition of Fat Gripz™ Increases Fatigue of Forearms
Figure 6. Maximum force produced by forearm with and without magnesium supplementation (n=4).
*P<0.05 versus placebo
Figure 7. Total hang time with Fat Gripz across three trials with and without magnesium supplementation (n=4).
Figure 8. Length of Body Weight Hang for each of the 3 consecutive trials (n=4).
Figure 9. Percentage of Max Force Recovered Over Time (n=4).
There was a decrease in maximum isometric force from the placebo to the MgCl2
Pilot 3 - Laying Prone Improves Isometric Forearm Contraction
Figure 10. Maximum force produced by forearm with and without magnesium supplementation (n=4).
Figure 11. Total hang time across three trials with and without magnesium supplementation (n=4).
Figure 12. Length of Body Weight Hang for each of the 3 consecutive trials (n=4).
* P<0.05 versus Trial 1
Figure 13. Percentage of Max Force Recovered Over Time (n=4) Both conditions show signs of recovery, however, they both show decline after their peak had been reached.
* P<0.05 versus 30 s # P<0.05 versus 180 s
There was a slight decrease in the maximum isometric force between the supplemented group and the supplemented group (P=.444, Table 10). The
non-*
*
*
#
# #
supplemented trial showed the participants had a greater overall hold time than the supplemented trials (P=.937, Figure 11). When comparing individual trials in the fatigue protocol, there was a greater decrease from the first to the second trial in the non-supplemented group; the non-supplemented group showed a consistent decline in amount of time the participants could hang on to the dumbbell between trials, here there was a big difference in progression of dumbbell hold time between trials (P=0.003, Figure 12). In recovery, the supplemented group began at a higher relative strength than the supplemented group and then reached the peak recovered force quicker than the non-supplemented group. There was also a strong difference of the relative maximum force production during the recovery protocol over time (P<0.001 Figure 13). There was a decrease in maximal force following the fatigue protocol for both the supplemented (19.8%±9.4 decrease, P=0.041) and placebo groups (22.7%±9.3 decrease, P=0.009).
There was a general trend of the relative force recovered increasing before reaching its peak. Following the peak being reached, the relative force decreased slightly. There was a difference of force production over time (P= 0.040, Figure 14). The post hoc indicated that significance was not reached between time points, however, there were some trends that indicated differences between the points at 135 s and 225 s versus 45 s (P=0.070, P=0.070), and 135 s versus 225 s (P= 0.070).
Figure 14. Percentage of Max for Recovered for
CHAPTER 5: DISCUSSION
The goal with the pilot testing was to optimize the data collection and testing protocols for maximum isometric force, forearm endurance, and forearm recovery. Each pilot test presented an opportunity to explore different methodical considerations that may influence the study results. The goals were to 1) find a mechanism of determining maximum force of the individual in a way that would reduce any learning effect 2) fatigue the forearm in a specific enough manner to introduce a way of measuring any potential effect on endurance that could be seen between conditions 3) determine whether or not recovery of the muscle was affected by the protocol, variables including increased fatiguing from the test itself were avoided. We found that a maximum isometric forearm contraction and recovery protocol would work best with the participant laying prone on a bench, their shoulder at 90 degrees of flexion, with 45 seconds of rest between each recovery contraction. The most practical fatigue protocol was found to be one that would be standardized for each participant, holding a dumbbell equipped with a thick grip (Fat Gripz™) that was standardized to maximal grip strength. In the end, a final protocol was eventually reached that we believed tested the experimental conditions in an effective way.
Pilot 1
body. They were then asked to give a two second contraction, at which point the maximum force produced was collected. The forearm was used because of extensive previous research that used this muscle group as its focus in determining muscle performance 41–45. Contractions lasting more than one second have been shown to
increase the metabolic systems that become activated46; therefore the time of our
contractions were kept greater than one second to attempt to get any of the potential metabolic effects that magnesium may have. The data for the two conditions was collected on separate days, allowing for the use of their dominant arm with both conditions. The data collected suggests that there was no difference between the two conditions. This could have been due to the lack of affect by the supplementation or by the positioning of the participant. The fatigue protocol consisted of the participant was carried out by having the participant hang from a bare pull-up bar until failure three consecutive times, with one minute of rest in-between each trial. This method was originally chosen due to its proven ability to fatigue the upper body muscles47,48. The
or the condition tests. Suggesting that the protocol in itself may have been flawed in its ability to determine recovery.
After discussions with the participants, it was pointed out and determined from the data and the feedback we received that the hanging wasn’t so much fatiguing their forearms, which we were testing, but were rather fatiguing their hand, which created the variability in the fatiguing. To counter this, moving forward, a Fat Gripz™ would be added to the bar, as that would localize the force of the body hang away from the hands and towards the forearms49.
Pilot 2
for five minutes. Similar to pilot 1, there was no consistent difference in recovery times. There was a more gradual upwards trend in recoveries that were supplemented with the magnesium supplement, however, the lack of any recovery whatsoever for the non-supplemented trials suggested that the protocol may be flawed in its ability to accurately determine the recovery of the muscle.
The maximum isometric strength protocol and recovery protocol both evolved due to the discovery of literature50,51 that indicated that a prone posture with the participant in
the forearm muscle fatigue appeared to be problematic. This compounded with the minimized decrease in force compared to pilot 1 suggested that perhaps the body weight hangs were a perhaps too great of a load to produce significant and consistent effects of fatiguing the relatively weak forearm muscles when compared to other upper extremity muscles in young adults52. There may be a greater variation between the load that the
person would have to carry (their weight) and the strengths of their forearms. To standardize this, the protocol shifted towards a fatiguing protocol that was more specific to the individuals, to ensure that the load they would have to carry would be more or less consistent between participants. Now, the participants would be asked to, while also prone, hold a dumbbell with the Fat Gripz™ that was 50% of their maximum forearm contraction. This would again be done three times until failure consecutively.
Pilot 3
Pilot 4
For this final test, only the recovery protocol was altered and it was tested on non-supplemented individuals. Here there was a significant difference between of the force production over time; particularly, there were the greatest differences in the earlier force productions (0 s – 45 s) compared to the later ones. This suggests that the new recovery protocol succeeded at examining the increase of early force productions (signifying the beginning of force recovery) over time, all culminating into an eventual plateau which is significantly different from the early stages (force maximally recovered).
Implications
Limitations and Strengths
introduced with the final study, the differences in the post hoc analyses should become more obvious. The small sample size was intentional to be able to quickly test a new experiment and determine the further steps that should be made to the protocol.
Some strengths of this study include the ability to test the same arm of each individual for both the control and the supplemented tests. This allowed for the results of each individual to be compared with themselves, which reduces the variability compared to a between-subjects approach. Another strength that is tied with the paired nature of this study is that, the randomization of arm dominance was not necessary. The dominant arm was always the one being testing, which again increased the strength of our abilities to use the results of our experiments to guide our protocol and reduced additional learning affects that could have been seen.
Conclusion
Magnesium is a vital cation in the human body and plays a role of over 300 enzymatic processes5–7. Some research has explored transdermal magnesium-chloride’s
potential role in muscle function with chronic application, but to date, no research has been done on the acute effects of such a supplement. Through this study, we have determined through preliminary testing the method that best tests the determination of forearm muscle force, endurance, and recovery. Based on the final protocol for this study, the efficacy of a transdermal magnesium-chloride supplement on acute muscle
REFERENCES
1. Maughan RJ, Greenhaff PL, Hespel P. Dietary supplements for athletes: Emerging trends and recurring themes. J Sports Sci. 2011. doi:10.1080/02640414.2011.587446
2. Manson JAE, Bassuk SS. Vitamin and mineral supplements what clinicians need to know. JAMA - J Am Med Assoc. 2018. doi:10.1001/jama.2017.21012
3. Bailey RL, Gahche JJ, Lentino C V., et al. Dietary Supplement Use in the United States, 2003–2006. J Nutr. 2011. doi:10.3945/jn.110.133025
4. Amagase H. US dietary supplement labeling rules and the possibility of medical cost reduction. J Nutr Sci Vitaminol (Tokyo). 2015. doi:10.3177/jnsv.61.S136
5. Finstad EW, Newhouse IJ, Lukaski HC, Mcauliffe JE, Stewart CR. The effects of magnesium supplementation on exercise performance. Med Sci Sports Exerc. 2001. doi:10.1097/00005768-200103000-00024
6. Blanco A, Blanco G. Medical Biochemistry.; 2017. doi:10.1038/199943a0
7. Wacker WEC. THE BIOCHEMISTRY OF MAGNESIUM. Ann N Y Acad Sci. 1969. doi:10.1111/j.1749-6632.1969.tb13003.x
9. Rosanoff A, Weaver CM, Rude RK. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr Rev. 2012. doi:10.1111/j.1753-4887.2011.00465.x
10. Driscoll MS, Kwon EKM, Skupsky H, Kwon SY, Grant-Kels JM. Nutrition and the deleterious side effects of nutritional supplements. Clin Dermatol. 2010. doi:10.1016/j.clindermatol.2010.03.023
11. Chiuve SE, Korngold EC, Januzzi JL, Gantzer M Lou, Albert CM. Plasma and dietary magnesium and risk of sudden cardiac death in women. Am J Clin Nutr. 2011. doi:10.3945/ajcn.110.002253
12. Ford ES, Mokdad AH. Dietary Magnesium Intake in a National Sample of U.S. Adults. J Nutr. 2018. doi:10.1093/jn/133.9.2879
13. Saris NEL, Mervaala E, Karppanen H, Khawaja JA, Lewenstam A. Magnesium: An update on physiological, clinical and analytical aspects. Clin Chim Acta. 2000. doi:10.1016/S0009-8981(99)00258-2
14. Baker JS, McCormick MC, Robergs RA. Interaction among skeletal muscle metabolic energy systems during intense exercise. J Nutr Metab. 2010. doi:10.1155/2010/905612
16. Esbjörnsson-Liljedahl M, Sundberg CJ, Norman B, Jansson E. Metabolic response in type I and type II muscle fibers during a 30-s cycle sprint in men and women. J Appl Physiol. 1999. doi:10.1152/jappl.1999.87.4.1326
17. Garfinkel L, Garfinkel D. Magnesium regulation of the glycolytic pathway and the enzymes involved. Magnesium. 1985.
18. Nihei T, Noda L, Morales M. Properties and Equilibrium Constant of the Adenosine catalyzed Reaction. J Biol Chem. 1961.
19. Matias CN, Santos DA, Monteiro CP, et al. Magnesium intake mediates the association between bone mineral density and lean soft tissue in elite swimmers. Magnes Res. 2012. doi:10.1684/mrh.2012.0317
20. Volpe SL. Magnesium and the Athlete. Curr Sports Med Rep. 2015. doi:10.1249/JSR.0000000000000178
21. Soria M, González-Haro C, López-Colón JL, Llorente MT, Escanero JF. Submaximal exercise intensities do not provoke variations in plasma magnesium concentration in well-trained euhydrated endurance athletes with no magnesium deficiency. Magnes Res. 2011. doi:10.1684/mrh.2011.0279
23. Brilla LR, Haley TF. Effect of magnesium supplementation on strength training in humans. J Am Coll Nutr. 1992. doi:10.1080/07315724.1992.10718233
24. Kass LS, Poeira F. The effect of acute vs chronic magnesium supplementation on exercise and recovery on resistance exercise, blood pressure and total peripheral resistance on normotensive adults. J Int Soc Sports Nutr. 2015. doi:10.1186/s12970-015-0081-z
25. GRAHAM LA, CAESAR JJ, BURGEN AS. Gastrointestinal absorption and excretion of Mg 28 in man. Metabolism. 1960.
26. Gröber U, Schmidt J, Kisters K. Magnesium in prevention and therapy. Nutrients. 2015. doi:10.3390/nu7095388
27. Gulick DT, Agarwal M, Josephs J, Reinmiller A, Zimmerman B. Effects of MagProTM on muscle performance. J Strength Cond Res. 2012.
doi:10.1519/JSC.0b013e31823f2863
28. Guerrera MP, Volpe SL, Mao JJ. Therapeutic uses of magnesium. Am Fam Physician. 2009.
29. Zhang Y, Xun P, Wang R, Mao L, He K. Can Magnesium Enhance Exercise Performance? Nutrients. 2017. doi:10.3390/nu9090946
31. Terblanche S, Noakes TD, Dennis SC, Marais DW, Eckert M. Failure of Magnesium Supplementation to Influence Marathon Running Performance or Recovery in Magnesium-Replete Subjects. Int J Sport Nutr. 2016. doi:10.1123/ijsn.2.2.154
32. Sircus M. Transdermal Magnesium Therapy. Igarss 2014. 2014. doi:10.1007/s13398-014-0173-7.2
33. Santos DA, Matias CN, Monteiro CP, et al. Magnesium intake is associated with strength performance in elite basketball, handball and volleyball players. Magnes Res. 2011. doi:10.1684/mrh.2011.0290
34. Gröber U, Werner T, Vormann J, Kisters K. Myth or reality-transdermal magnesium? Nutrients. 2017. doi:10.3390/nu9080813
35. Piccini F, Ragazzoni G, Valentini L, Faloia E, Gobbi P. Intracellular absorption of transdermal magnesium demonstrated by ESEM-EDS. Ital J Anat Embryol. 2014.
36. Kass L, Rosanoff A, Tanner A, Sullivan K, McAuley W, Plesset M. Effect of transdermal magnesium cream on serum and urinary magnesium levels in humans: A pilot study. PLoS One. 2017. doi:10.1371/journal.pone.0174817
37. Bohl CH, Volpe SL. Magnesium and exercise. Crit Rev Food Sci Nutr. 2002. doi:10.1080/20024091054247
the relationship between magnesium and sport. Magnes Res. 1990.
39. Methenitis S, Karandreas N, Spengos K, Zaras N, Stasinaki AN, Terzis G. Muscle Fiber Conduction Velocity, Muscle Fiber Composition, and Power Performance. Med Sci Sports Exerc. 2016. doi:10.1249/MSS.0000000000000954
40. Behringer M, Grützner S, Montag J, McCourt M, Ring M, Mester J. Effects of stimulation frequency, amplitude, and impulse width on muscle fatigue. Muscle and Nerve. 2016. doi:10.1002/mus.24893
41. Schoenfeld BJ, Ratamess NA, Peterson MD, Contreras B, Tiryaki-Sonmez G. Influence of Resistance Training Frequency on Muscular Adaptations in Well-Trained Men. J Strength Cond Res. 2015. doi:10.1519/JSC.0000000000000970
42. Kim J, Lang JA, Pilania N, Franke WD. Effects of blood flow restricted exercise training on muscular strength and blood flow in older adults. Exp Gerontol. 2017. doi:10.1016/j.exger.2017.09.016
43. Paternostro-Sluga T, Grim-Stieger M, Posch M, et al. Reliability and validity of the Medical Research Council (MRC) scale and a modified scale for testing muscle strength in patients with radial palsy. J Rehabil Med. 2008. doi:10.2340/16501977-0235
45. Selig SE, Carey MF, Menzies DG, et al. Moderate-intensity resistance exercise training in patients with chronic heart failure improves strength, endurance, heart rate variability, and forearm blood flow. J Card Fail. 2004. doi:10.1016/S1071-9164(03)00583-9
46. Sheikholeslami-Vatani D, Ahmadi S, Chehri B, Tadibi V. The effect of changes in concentric-eccentric contraction time ratio on hormonal response to resistance exercise in trained men. Sci Sport. 2018. doi:10.1016/j.scispo.2017.11.004
47. Casajús JA, Leiva MT, Villarroya A, Legaz A, Moreno LA. Physical performance and school physical education in overweight Spanish children. Ann Nutr Metab. 2007. doi:10.1159/000105459
48. Walsh AS, Seifert L, Button C CJ. The effect of additional load and maximal fatigue on perceived horizontal reach- and grasp-ability in a whole body reaching task. In: 4th International Rock Climbing Research Association (IRCRA) Congress. ; 2018.
49. Krings BM, Shepherd BD, Swain JC, et al. Impact of Fat Grip Attachments on Muscular Strength and Neuromuscular Activation During Resistance Exercise. J Strength Cond Res. 2019. doi:10.1519/jsc.0000000000002954
50. Kuzala EA, Vargo MC. The relationship between elbow position and grip strength. Am J Occup Ther Off Publ Am Occup Ther Assoc. 1992. doi:10.5014/ajot.46.6.509
Grip Strength. Eur Sci J. 2014.