Coronary Stents and Chronic Anticoagulation
Angelos Sourgounis, MD; Janusz Lipiecki, MD; Ted S. Lo, MD; Martial Hamon, MD
C
ase Presentation:
A 76-year-old
man was admitted with
retroster-nal chest pain. The ECG on admission
showed inferolateral ST depression,
and troponin levels were elevated,
con-firming the diagnosis of an acute
cor-onary syndrome. The patient had a
history of hypertension and aortic
valve replacement with a metallic
bileaflet valve 7 years before. He was
being treated with warfarin and
low-dose aspirin and had an international
normalized ratio (INR) of 2.5.
Coro-nary angiography revealed a long
sub-occlusive lesion of the proximal right
coronary artery. At that point, there
was a question about the optimal
treat-ment for this patient regarding the type
of stent to be selected and the need for
future combined antiplatelet and
anti-coagulation treatment.
Percutaneous Coronary
Intervention and
Warfarin Treatment
Oral anticoagulation was routinely
used for coronary stent thrombosis
prevention during the first era of
stents.
1It has since been replaced by the
combination of aspirin and a
thienopyri-dine because studies have shown a
def-inite advantage of the antiplatelet
com-bination on coronary events
2– 4and on
reducing the risk of access-site bleeding
complications. However,
⬇
5%
5,6of
patients undergoing percutaneous
cor-onary intervention (PCI) also present
with an indication for oral
anticoagu-lation therapy. In such cases, the type
of stent selected; the use of oral
anti-coagulants, antiplatelets, or their
com-binations; the target INR; and the
du-ration of treatment are essential
considerations in relation to the risk of
stent thrombosis/thromboembolic
events and bleeding risk. With the
introduction and widespread use of
drug-eluting stents (DES) in recent
years and given the necessity for
longer duration of dual antiplatelet
therapy, the issue of concurrent
warfa-rin and antiplatelet therapy has become
even more important. The existing
guidelines do not offer a convincing
solution to these issues. For acute
cor-onary syndrome patients with an
indica-tion for anticoagulaindica-tion, triple therapy
(warfarin, aspirin, and clopidogrel) for
the minimum time possible and a
maintenance regimen of warfarin plus
aspirin are recommended after stent
implantation
7–9; for patients with atrial
fibrillation, double therapy of warfarin
plus clopidogrel is recommended as
maintenance.
10However, these
recom-mendations are based on a low level of
evidence. Recently, the use of bare
metal stents (BMS) was recommended
with triple therapy for 1 month,
fol-lowed by warfarin plus aspirin; DES
are to be avoided, but when they are
used, clopidogrel therapy for 1 year
was recommended.
11However, these
recommendations do not specify the
optimal treatment according to the
var-ious indications for anticoagulation or
the duration of treatment, nor do they
take into account the estimated
throm-bosis and bleeding risks.
As a result, there is a significant
variation in the regimens followed for
patients on anticoagulation who have
had a stent implanted, as was
demon-strated in a survey among
interven-tional cardiology centers worldwide.
12Data from an acute coronary syndrome
patient registry
6show that triple
ther-apy is the most commonly used (60%
of acute coronary syndromes),
fol-lowed by double antiplatelet therapy
(used in 31%), whereas warfarin plus
aspirin or clopidogrel is used in a
minority of patients. However, no
ran-domized trial demonstrating the
effi-cacy and safety of triple therapy has
yet been conducted.
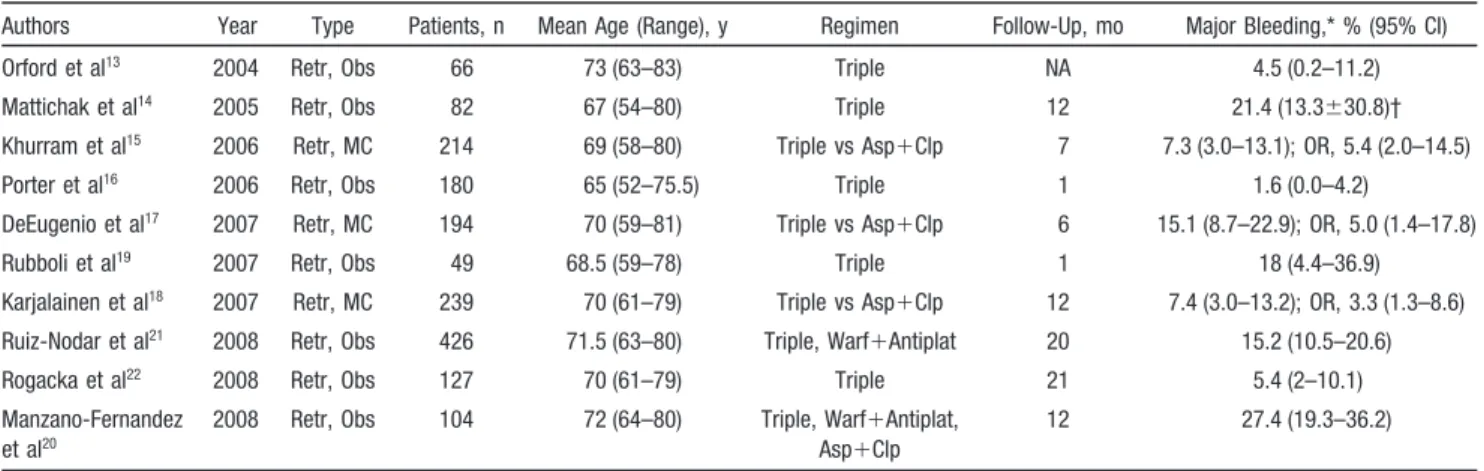
A small number of retrospective
studies have examined the safety of
triple therapy (Table 1)
13–22and have
demonstrated a significant occurrence
of major bleeding episodes, ranging
from 4.5% to 27.4% of patients. Data
From the Department of Cardiology, University Hospital of Caen, Normandy (A.S., T.S.L., M.H.); Department of Cardiology, University Hospital of Clermont-Ferrand, Clermont-Ferrand (J.L.); and INSERM U744, Institute Pasteur de Lille (M.H.), Lille, France.
Correspondence to Professor Martial Hamon, Service des Maladies de Coeur et des Vaisseaux, Centre Hospitalier Universitaire de Caen, Avenue Côte de Nacre, 14033 Caen, Normandy, France. E-mail [email protected]
(Circulation. 2009;119:1682-1688.) © 2009 American Heart Association, Inc.
Circulationis available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.108.834861
1682
from the 3 published matched cohort
studies show that the relative risk of
major bleeding is 4 times higher with
triple therapy than with a standard
double antiplatelet regimen (Figure 1).
On the other hand, it has been recently
demonstrated that double antiplatelet
therapy is much less efficient than
warfarin alone in preventing embolic
episodes in atrial fibrillation patients.
23Even fewer data are available on the
efficacy of triple therapy, especially in
patients with mechanical valves. Two
recent studies
18,21that compared the
efficacy of double antiplatelet therapy
with combinations, including
combi-nations with warfarin, showed
contra-dictory results in the occurrence of
major adverse cardiac events.
Assessment of
Individual Risk
Clearly, each of the possible
treat-ments has its pros and cons. The first
step in the selection of the appropriate
therapy is to assess the risk for each
individual, and balancing embolic risk
and bleeding risk is crucial in making
this decision. Recently published data
6have suggested that cardiologists take
bleeding risk into account more than
embolic risk, which may have resulted
in underuse of warfarin. Although the
choice is often based on the subjective
empirical estimation of the treating
physician, validated schemes for
esti-mating risk are available, and their use
is encouraged. The CHADS2 score, a
well-tested scheme that has the
advan-tage of simplicity, successfully
strati-fies atrial fibrillation patients
accord-ing to risk for stroke. The CHADS2
score is calculated from 5 risk factors:
congestive heart failure, hypertension,
age
⬎
75 years, diabetes mellitus, and
prior stroke or transient ischemic attack.
Two points are given for prior stroke; all
the other risk factors are assigned 1
point. A CHADS2 score of 0 to 1
iden-tifies patients at low risk, a score of 2 to
3 marks patients at intermediate risk, and
a score of 4 to 6 indicates high-risk
patients.
24,25Unlike atrial fibrillation, other
con-ditions put patients at a uniformly high
risk of embolism. Patients with a
me-chanical valve prosthesis have an
an-nual risk of thrombotic complications
without anticoagulation that ranges
from 10% up to 91%, depending on the
type, position, and number of
prothe-ses.
26Patients who have experienced
an episode of venous
thromboembo-lism are at an annual risk of 6% to 9%
for a subsequent episode. The required
duration of anticoagulant treatment is
3 months for an episode resulting from
transient causes and
⬎
6 months for a
recurrent or idiopathic episode.
27A
substantial number of patients who
Table.
Triple Therapy and Major Bleeding
Authors Year Type Patients, n Mean Age (Range), y Regimen Follow-Up, mo Major Bleeding,* % (95% CI) Orford et al13 2004 Retr, Obs 66 73 (63–83) Triple NA 4.5 (0.2–11.2)
Mattichak et al14 2005 Retr, Obs 82 67 (54–80) Triple 12 21.4 (13.3⫾30.8)†
Khurram et al15 2006 Retr, MC 214 69 (58–80) Triple vs Asp⫹Clp 7 7.3 (3.0–13.1); OR, 5.4 (2.0–14.5)
Porter et al16 2006 Retr, Obs 180 65 (52–75.5) Triple 1 1.6 (0.0–4.2)
DeEugenio et al17 2007 Retr, MC 194 70 (59–81) Triple vs Asp⫹Clp 6 15.1 (8.7–22.9); OR, 5.0 (1.4–17.8)
Rubboli et al19 2007 Retr, Obs 49 68.5 (59–78) Triple 1 18 (4.4–36.9)
Karjalainen et al18 2007 Retr, MC 239 70 (61–79) Triple vs Asp⫹Clp 12 7.4 (3.0–13.2); OR, 3.3 (1.3–8.6)
Ruiz-Nodar et al21 2008 Retr, Obs 426 71.5 (63–80) Triple, Warf⫹Antiplat 20 15.2 (10.5–20.6)
Rogacka et al22 2008 Retr, Obs 127 70 (61–79) Triple 21 5.4 (2–10.1)
Manzano-Fernandez et al20
2008 Retr, Obs 104 72 (64–80) Triple, Warf⫹Antiplat, Asp⫹Clp
12 27.4 (19.3–36.2) Retr indicates retrospective; Obs, observational; MC, matched cohort; Asp, aspirin; Clp, clopidogrel; OR, odds ratio; Warf, warfarin; and Antiplat, antiplatelet. *Midpoint-adjusted Wald interval.
†Transfusions.
Figure 1.Major bleeding in matched cohort trials. Warf indicates warfarin; Asp, aspirin, Clop, clopidogrel, and RR, relative risk.
undergo PCI with stent implantation
after an acute myocardial infarction
develop left ventricular thrombus and
are at increased risk of embolism (6%
to 12% annually), so anticoagulation
therapy is recommended for at least 3
months for these patients.
28The next step in risk assessment is
to estimate the bleeding risk of the
patient. Major bleeding in patients
un-der anticoagulant treatment is not rare;
the yearly incidence of intracranial
hemorrhage was reported to be 0.3% in
an elderly population.
29Risk
stratifica-tion schemes developed so that
indi-vidual bleeding risk can be objectively
estimated
30 –32include the Outpatient
Bleeding Risk Index, which classifies
patients into 3 risk categories; 1 point
is applied for age
⬎
65 years, 1 point
for history of stroke, and 1 point for
history of gastrointestinal bleeding; an
additional point is applied if any one of
the following conditions exists:
ane-mia (hematocrit
⬍
30%), renal
dys-function (creatinine
⬎
15 mg/L), or
dia-betes.
30A score of 0 is defined as low
risk, 1 to 2 as intermediate risk, and 3 to
4 as high risk for bleeding. This index
has been prospectively validated and
shown to achieve acceptable
discrimina-tion among the categories of risk.
32,33Finally, the selection of the
appro-priate therapy is influenced by the
estimated restenosis risk, which
deter-mines whether a DES is necessary.
The clinical, lesion, and procedural
variables that define high risk for
re-stenosis after BMS implantation are
well established
34; however, the
con-comitant treatment with warfarin urges
less liberal use of DES for restenosis
prevention because of the risk of
in-creased bleeding inherent in
anticoag-ulation treatment.
Therapeutic Options
Triple Therapy
The combined use of warfarin, aspirin,
and clopidogrel is, in theory, the
op-tion that ensures the best protecop-tion
against embolic episodes and stent
thrombosis. Only 2 studies have
pro-vided data on the efficacy of triple
therapy, showing that its stroke rate is
comparable to that on warfarin
mono-therapy; substantially more data are
available on major bleeding caused by
the triple combination. Using data
from the 3 matched cohort studies
(Figure 1), one can estimate that,
add-ing warfarin to standard double
anti-platelet therapy, the number needed to
harm for 1 year inducing a major
bleeding episode was 14. An indirect
comparison with the protection
pro-vided can be done using data from the
Atrial Fibrillation Clopidogrel Trial
With Irbesartan for Prevention of
Vas-cular Events (ACTIVE W) study,
23accepting similar rates of stroke for
triple therapy and warfarin
mono-therapy. In the ACTIVE W trial, the
number needed to treat to prevent a
stroke with warfarin compared with
dual antiplatelet therapy was 100. This
comparison strongly discourages the
extensive use of triple therapy and
urges careful selection of patients, but
it probably also urges limiting the
du-ration of this treatment.
Warfarin Plus Aspirin
The combination of warfarin plus
as-pirin has been studied much more
ex-tensively, although the studies were
done before the introduction of latest
generation of stents, including DES. A
meta-analysis of these studies
demon-strated the superiority of double
anti-platelet therapy over warfarin plus
as-pirin in patients with an end point of
death, myocardial infarction, or need
for revascularization, whereas there
was no significant difference in the
occurrence of stent thrombosis and
major bleeding.
35However, an
ad-justed indirect meta-analysis based on
a much larger number of patients and
more recent studies
36showed that the
combination of warfarin plus aspirin
with a target INR of 2 to 3 was as
efficient as aspirin plus clopidogrel in
preventing major adverse events in
patients recovering from an acute
cor-onary syndrome. The combination of
aspirin and warfarin was associated
with a lower risk of stroke but
in-creased risk of major bleeding. The
number needed to harm to cause a
major bleeding episode is 77 compared
with 14 with triple therapy. However,
the 2 recent trials that provided data on
the efficacy of this combination
spe-cifically in PCI patients showed a high
incidence of stent thrombosis (15.2%)
and unscheduled PCI (17.2%),
respec-tively, mainly during the first month of
treatment. However, the studies
in-cluded a small number of patients.
18,37Warfarin Plus Clopidogrel
Limited data are available on the
safety and efficacy of this
combina-tion. In the 2 studies that have
ad-dressed the combination,
18,37it
pre-sented common major bleeding
complications (11.1%) but good
effi-cacy against stroke (0% to 4.4%) and
stent thrombosis (0%). However,
be-cause these data were derived from a
small number of patients, further
stud-ies are needed to clarify the issue and
to support the use of this combination.
Aspirin Plus Clopidogrel
The efficacy of the antiplatelet
combi-nation against stent thrombosis is well
established, especially in the case of
DES. In addition, experts suggest
war-farin treatment when the risk of stroke
is
⬎
2%; for lower-risk patients, the
benefits from stroke prevention are
counterbalanced by the increased
bleeding risk, so it is logical to suggest
this combination only to patients with
a CHADS2 score of 0 to 1. In a
recently published study,
38patients
with atrial fibrillation and a CHADS2
score of 1 had a yearly stroke risk of
1.25% while taking aspirin plus
clopi-dogrel, which can be considered
ac-ceptable, considering the high bleeding
risk of other options.
Incorporating the existing data, we
provide an algorithm for appropriate
treatment selection in various
situa-tions in Figure 2.
Other Considerations
Acute Coronary Syndromes
According to current guidelines,
aspi-rin treatment is recommended
defini-tively for acute coronary syndrome
patients whether or not they underwent
PCI. Clopidogrel is recommended for
at least 12 months, especially in the
case of coronary stenting. However, in
the case of coronary stenting with
BMS, the gain from prolonged
clopi-dogrel treatment in patients at
interme-diate or high risk for bleeding can be
assumed to be neutralized by the
in-creased bleeding complications;
there-fore, we suggest the same strategy as
for elective PCI for these patients.
Access-Site Selection
It is generally accepted that coronary
angiography and PCI can be safely
performed by femoral access after
dis-continuing warfarin and achieving an
INR of
⬍
1.5.
39Manual-pressure
he-mostasis and artery closure devices
have been used during diagnostic
an-giography with a low incidence of
bleeding complications in fully
antico-agulated patients.
40,41However, the
usual strategy is to withhold warfarin
before transfemoral PCI and to restart
after the procedure using intravenous
heparin or low-molecular-weight
hep-arin as a bridge until adequate
antico-agulation with warfarin is
reestab-lished in patients at high risk for
embolism. Many of the bleeding
com-plications are reported to happen
dur-ing this crossover period from heparin
to oral anticoagulation.
16The radial
approach has also been used
success-fully for coronary angiography with no
incidence of major bleeding
complica-tions in fully anticoagulated
pa-tients
42,43and
has
consistently
achieved fewer bleeding complications
during PCI compared with the femoral
approach.
44,45Compared with the
ra-dial approach, femoral access has been
a strong predictor of access-site
com-plications after PCI in patients treated
with warfarin.
46The possibility of
per-forming PCI by the radial approach
without withholding warfarin, thereby
avoiding bleeding or thrombotic
com-plications during the crossover period,
makes the radial approach the first
choice for these patients, especially
during emergency procedures.
Gastric Protection
Proton pump inhibitors are used in
acute coronary syndrome patients
con-sidered at high risk for hemorrhage
47despite the absence of a randomized
trial evaluating their usefulness after
PCI. However, on the basis of data
from a case-control study
48and the
documented effectiveness of
esome-prazole in reducing bleeding caused by
antiplatelet medications,
49proton
pump inhibition can be recommended
for patients at medium or high risk for
bleeding. Omeprazole has been shown
to potentiate the anticoagulant action
of warfarin
50and to decrease the
inhib-itory effect of clopidogrel on
plate-lets
51; therefore, its use has to be
un-dertaken with caution in this category
of patients.
52Optimal Level of Anticoagulation
Dual treatment with warfarin and
aspi-rin has been shown to be favorable
compared with aspirin monotherapy
only in patients under tight INR
con-trol and an aim of 2 to 3.
53In the
Coronary stent and need for chronic anticoagulation What is the embolic risk?
What is the bleeding risk? High (>=6%) or
Medium (3-5%)
Low (<3%)
Avoid DES
Warf+Asp+Clop 1 month*; then Warf+Asp definitively† Consider CABG
Avoid DES if possible If BMS: Warf+Asp+Clop 1month; then Warf+Asp definitively† If DES: Warf+Asp+Clop 12 months; then Warf+Asp definitively
If BMS: Warf+Asp+Clop 1month‡; then Warf+ Asp definitively† If DES: Warf+Asp+Clop 12 months; then Warf+Asp definitively High Medium Low
If BMS: Asp+Clop for 1 month, then Asp+ Warf
If DES: Asp+Clop 12 months,
then Asp+Warf Figure 2.Flow chart for the selection of
appropriate treatment. Abbreviations as in Figure 1. *Consider adding PPI to any com-bination that includes aspirin. †Alternatively, warfarin⫹clopidogrel (less evidence for this combination). ‡For acute coronary syn-drome, warfarin⫹aspirin⫹clopidogrel 12 months, then warfarin⫹aspirin.
studies that have provided relevant
data, most major bleeding events
oc-curred at INR levels
⬍
3.
13,17,20For the
duration of concurrent antiplatelet
ad-ministration, an INR target of 2 to 2.5
under close observation seems to be
the best choice. When warfarin therapy
is required for a short period of time
(eg, venous thromboembolism, left
ventricular thrombus), PCI should be
postponed, if possible, until
comple-tion of warfarin therapy.
Prosthetic Valves
Current guidelines recommend
vita-min K antagonists plus low-dose
aspi-rin for patients with mechanical valves
and coronary disease. However,
long-term triple therapy could increase
bleeding complications to
unaccept-able levels, especially when a high
INR target (
ⱖ
3) is needed because of
valve or patient characteristics.
Al-though there are no data available that
address this specific subgroup of
pa-tients, it seems appropriate to shorten
the duration of triple therapy as much
as possible and to restrict the use of
DES only to patients at low calculated
risk for bleeding and with an INR of
no more than 2.5.
How Should We Manage
Our Example Patient?
Having taken into account the patient’s
age and the necessity of anticoagulant
treatment, we performed PCI with a
BMS. Triple therapy and a proton
pump inhibitor were prescribed for 1
month, followed by warfarin with an
INR target of 2.5 and aspirin 75 mg
indefinitely.
Conclusions
Available data show a remarkably
in-creased rate of major bleeding
compli-cations during prolonged treatment
with warfarin, aspirin, and
thienopyri-dine. This strongly suggests limiting
the time of its administration as much
as possible, especially in patients with
a high profile for bleeding risk. This
might be accomplished in the future by
using stents that recruit endothelial
progenitor cells and accelerate
endo-thelialization. A combination of
war-farin and 1 antiplatelet agent seems to
be a better choice for long-term
treat-ment after stent implantation,
balanc-ing the risks of thromboembolic events
and stent thrombosis with the risk of
major bleeding. Randomized trials in
progress are expected to further clarify
this issue.
Disclosures
None.
References
1. Serruys PW, de Jaegere P, Kiemeneij F, Macaya C, Rutsch W, Heyndrickx G, Emanuelsson H, Marco J, Legrand V, Materne P. A comparison of balloon-expandable-stent implantation with balloon angioplasty in patients with coronary artery disease: Benestent Study Group.N Engl J Med. 1994;331:489 – 495. 2. Bertrand ME, Legrand V, Boland J, Fleck E, Bonnier J, Emmanuelson H, Vrolix M, Missault L, Chierchia S, Casaccia M, Niccoli L, Oto A, White C, Webb-Peploe M, Van Belle E, McFadden EP. Randomized multi-center comparison of conventional anticoagu-lation versus antiplatelet therapy in unplanned and elective coronary stenting: the Full Anti-coagulation Versus Aspirin and Ticlopidine (FANTASTIC) study. Circulation. 1998;98: 1597–1603.
3. Leon MB, Baim DS, Popma JJ, Gordon PC, Cutlip DE, Ho KK, Giambartolomei A, Diver DJ, Lasorda DM, Williams DO, Pocock SJ, Kuntz RE. A clinical trial com-paring three antithrombotic-drug regimens after coronary-artery stenting: Stent Antico-agulation Restenosis Study Investigators.
N Engl J Med. 1998;339:1665–1671. 4. Urban P, Macaya C, Rupprecht HJ,
Kiemeneij F, Emanuelsson H, Fontanelli A, Pieper M, Wesseling T, Sagnard L. Ran-domized evaluation of anticoagulation versus antiplatelet therapy after coronary stent implantation in high-risk patients: the Multicenter Aspirin and Ticlopidine Trial After Intracoronary Stenting (MATTIS).
Circulation. 1998;98:2126 –2132. 5. Oudot A, Steg PG, Danchin N, Dentan G,
Zeller M, Sicard P, Buffet P, Laurent Y, Janin-Manificat L, L’Huillier I, Beer JC, Makki H, Morel P, Cottin Y. Impact of chronic oral anticoagulation on management and outcomes of patients with acute myo-cardial infarction: data from the RICO survey.Heart. 2006;92:1077–1083. 6. Wang TY, Robinson LA, Ou FS, Roe MT,
Ohman EM, Gibler WB, Smith SC Jr, Peterson ED, Becker RC. Discharge anti-thrombotic strategies among patients with acute coronary syndrome previously on warfarin anticoagulation: physician practice in the CRUSADE registry. Am Heart J. 2008;155:361–368.
7. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, Chavey WE 2nd, Fesmire FM, Hochman JS, Levin TN, Lincoff AM, Peterson ED, Theroux P, Wenger NK, Wright RS, Smith SC Jr, Jacobs AK, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Com-mittee to Revise the 2002 Guidelines for the Management of Patients With Unst-able Angina/Non–ST-Elevation Myocardial Infarction): developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons: endorsed by the American Asso-ciation of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine.Circulation. 2007;116: e148 – e304.
8. Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, Hochman JS, Krumholz HM, Lamas GA, Mullany CJ, Pearle DL, Sloan MA, Smith SC Jr, Anbe DT, Kushner FG, Ornato JP, Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Halperin JL, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B, Tarkington LG, Yancy CW. 2007 Focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines: developed in collabo-ration with the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Man-agement of Patients With ST-Elevation Myo-cardial Infarction, writing on behalf of the 2004 writing committee. Circulation. 2008; 117:296 –329.
9. King SB 3rd, Smith SC Jr, Hirshfeld JW Jr, Jacobs AK, Morrison DA, Williams DO, Feldman TE, Kern MJ, O’Neill WW, Schaff HV, Whitlow PL, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Page RL, Riegel B, Tarkington LG, Yancy CW. 2007 Focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines: 2007 Writing Group to Review New Evidence and Update the ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention, writing on behalf of the 2005 writing committee. Circulation. 2008;117: 261–295.
10. Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE,
Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Zamorano JL. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibril-lation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Com-mittee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collabo-ration with the European Heart Rhythm Association and the Heart Rhythm Society.
Circulation. 2006;114:e257– e354. 11. Becker RC, Meade TW, Berger PB,
Ezekowitz M, O’Connor CM, Vorchheimer DA, Guyatt GH, Mark DB, Harrington RA. The primary and secondary prevention of coronary artery disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th edition). Chest. 2008;133:776S– 814S.
12. Rubboli A, Colletta M, Sangiorgio P, Di Pasquale G. Antithrombotic treatment after coronary artery stenting in patients on chronic oral anticoagulation: an international survey of current clinical practice. Ital Heart J. 2004;5:851– 856.
13. Orford JL, Fasseas P, Melby S, Burger K, Steinhubl SR, Holmes DR, Berger PB. Safety and efficacy of aspirin, clopidogrel, and warfarin after coronary stent placement in patients with an indication for anticoagu-lation.Am Heart J. 2004;147:463– 467. 14. Mattichak SJ, Reed PS, Gallagher MJ, Boura
JA, O’Neill WW, Kahn JK. Evaluation of safety of warfarin in combination with anti-platelet therapy for patients treated with coronary stents for acute myocardial infarction. J Interv Cardiol. 2005;18: 163–166.
15. Khurram Z, Chou E, Minutello R, Bergman G, Parikh M, Naidu S, Wong SC, Hong MK. Combination therapy with aspirin, clopi-dogrel and warfarin following coronary stenting is associated with a significant risk of bleeding. J Invasive Cardiol. 2006;18: 162–164.
16. Porter A, Konstantino Y, Iakobishvili Z, Shachar L, Battler A, Hasdai D. Short-term triple therapy with aspirin, warfarin, and a thienopyridine among patients undergoing per-cutaneous coronary intervention. Catheter Cardiovasc Interv. 2006;68:56 – 61. 17. DeEugenio D, Kolman L, DeCaro M, Andrel
J, Chervoneva I, Duong P, Lam L, McGowan C, Lee G, Ruggiero N, Singhal S, Greenspon A. Risk of major bleeding with concomitant dual antiplatelet therapy after percutaneous coronary intervention in patients receiving long-term warfarin therapy.Pharmacotherapy. 2007;27:691– 696.
18. Karjalainen PP, Porela P, Ylitalo A, Vikman S, Nyman K, Vaittinen MA, Airaksinen TJ,
Niemela M, Vahlberg T, Airaksinen KE. Safety and efficacy of combined antiplatelet-warfarin therapy after coronary stenting.Eur Heart J. 2007;28:726 –732.
19. Rubboli A, Colletta M, Herzfeld J, Sangiorgio P, Di Pasquale G. Periprocedural and medium-term antithrombotic strategies in patients with an indication for long-term anti-coagulation undergoing coronary angiography and intervention.Coron Artery Dis. 2007;18: 193–199.
20. Manzano-Fernandez S, Pastor FJ, Marin F, Cambronero F, Caro C, Pascual-Figal DA, Garrido IP, Pinar E, Valdes M, Lip GY. Increased major bleeding complications related to triple antithrombotic therapy usage in patients with atrial fibrillation undergoing percutaneous coronary artery stenting.
Chest. 2008;134:559 –567.
21. Ruiz-Nodar JM, Marín F, Hurtado JA, Valencia J, Pinar E, Pineda J, Gimeno JR, Sogorb F, Valdés M, Lip GY. Anticoagulant and antiplatelet therapy use in 426 patients with atrial fibrillation undergoing percutaneous coronary intervention and stent implantation.
J Am Coll Cardiol. 2008;51:818 – 825. 22. Rogacka RCA, Michev I, Airoldi F, Latib
A, Cosgrave J, Montorfano M, Carlino M, Sangiorgi G, Castelli A, Godino C, Magni V, Aranzulla T, Romagnoli E, Colombo A. Dual antiplatelet therapy after percutaneous coronary intervention with stent implan-tation in patients taking chronic oral antico-agulation.J Am Coll Cardiol Intv. 2008;1: 56 – 61.
23. Connolly S, Pogue J, Hart R, Pfeffer M, Hohnloser S, Chrolavicius S, Yusuf S. Clo-pidogrel plus aspirin versus oral anticoagu-lation for atrial fibrilanticoagu-lation in the Atrial Fibrillation Clopidogrel Trial With Irbe-sartan for Prevention of Vascular Events (ACTIVE W): a randomised controlled trial.
Lancet. 2006;367:1903–1912.
24. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Vali-dation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation.JAMA. 2001; 285:2864 –2870.
25. Gage BF, van Walraven C, Pearce L, Hart RG, Koudstaal PJ, Boode BS, Petersen P. Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation. 2004; 110:2287–2292.
26. Ansell J, Hirsh J, Poller L, Bussey H, Jacobson A, Hylek E. The pharmacology and management of the vitamin K antagonists: the Seventh ACCP Conference on Anti-thrombotic and Thrombolytic Therapy.
Chest. 2004;126:204S–233S.
27. Snow V, Qaseem A, Barry P, Hornbake ER, Rodnick JE, Tobolic T, Ireland B, Segal JB, Bass EB, Weiss KB, Green L, Owens DK. Management of venous thromboembolism: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians.
Ann Intern Med. 2007;146:204 –210. 28. Antman EM, Anbe DT, Armstrong PW,
Bates ER, Green LA, Hand M, Hochman JS,
Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr, Alpert JS, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Gregoratos G, Halperin JL, Hiratzka LF, Hunt SA, Jacobs AK. ACC/AHA guidelines for the man-agement of patients with ST-elevation myo-cardial infarction: a report of the American College of Cardiology/American Heart Asso-ciation Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myo-cardial Infarction). Circulation. 2004;110: e82– e292.
29. Shireman TI, Howard PA, Kresowik TF, Ellerbeck EF. Combined anticoagulant-antiplatelet use and major bleeding events in elderly atrial fibrillation patients. Stroke. 2004;35:2362–2367.
30. Landefeld CS, Goldman L. Major bleeding in outpatients treated with warfarin: incidence and prediction by factors known at the start of outpatient therapy. Am J Med. 1989;87:144 –152.
31. Kuijer PM, Hutten BA, Prins MH, Buller HR. Prediction of the risk of bleeding during anticoagulant treatment for venous thrombo-embolism. Arch Intern Med. 1999;159: 457– 460.
32. Shireman TI, Mahnken JD, Howard PA, Kresowik TF, Hou Q, Ellerbeck EF. Devel-opment of a contemporary bleeding risk model for elderly warfarin recipients.Chest. 2006;130:1390 –1396.
33. Beyth RJ, Quinn LM, Landefeld CS. Pro-spective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin.Am J Med. 1998;105: 91–99.
34. Kastrati A, Mehilli J, Dirschinger J, Pache J, Ulm K, Schuhlen H, Seyfarth M, Schmitt C, Blasini R, Neumann FJ, Schomig A. Reste-nosis after coronary placement of various stent types.Am J Cardiol. 2001;87:34 –39. 35. Rubboli A, Milandri M, Castelvetri C,
Cosmi B. Meta-analysis of trials comparing oral anticoagulation and aspirin versus dual antiplatelet therapy after coronary stenting: clues for the management of patients with an indication for long-term anticoagulation undergoing coronary stenting. Cardiology. 2005;104:101–106.
36. Testa L, Zoccai GB, Porto I, Trotta G, Agostoni P, Andreotti F, Crea F. Adjusted indirect meta-analysis of aspirin plus warfarin at international normalized ratios 2 to 3 versus aspirin plus clopidogrel after acute coronary syndromes. Am J Cardiol. 2007;99:1637–1642.
37. Nguyen MC, Lim YL, Walton A, Lefkovits J, Agnelli G, Goodman SG, Budaj A, Gulba DC, Allegrone J, Brieger D. Combining warfarin and antiplatelet therapy after coronary stenting in the Global Registry of Acute Coronary Events: is it safe and effective to use just one antiplatelet agent?
Eur Heart J. 2007;28:1717–1722. 38. Healey JS, Hart RG, Pogue J, Pfeffer MA,
Hohnloser SH, De Caterina R, Flaker G, Yusuf S, Connolly SJ. Risks and benefits of oral anticoagulation compared with
dogrel plus aspirin in patients with atrial fibrillation according to stroke risk: the Atrial Fibrillation Clopidogrel Trial With Irbesartan for Prevention of Vascular Events (ACTIVE-W).Stroke. 2008;39:1482–1486. 39. Bonow RO, Carabello BA, Kanu C, de
Leon AC Jr, Faxon DP, Freed MD, Gaasch WH, Lytle BW, Nishimura RA, O’Gara PT, O’Rourke RA, Otto CM, Shah PM, Shanewise JS, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Hunt SA, Lytle BW, Nishimura R, Page RL, Riegel B. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Man-agement of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiol-ogists: endorsed by the Society for Cardio-vascular Angiography and Interventions and the Society of Thoracic Surgeons.
Circulation. 2006;114:e84 – e231. 40. El-Jack SS, Ruygrok PN, Webster MW,
Stewart JT, Bass NM, Armstrong GP, Ormiston JA, Pornratanarangsi S. Effec-tiveness of manual pressure hemostasis fol-lowing transfemoral coronary angiography in patients on therapeutic warfarin anticoag-ulation.Am J Cardiol. 2006;97:485– 488. 41. Jessup DB, Coletti AT, Muhlestein JB, Barry
WH, Shean FC, Whisenant BK. Elective coronary angiography and percutaneous coronary intervention during uninterrupted
warfarin therapy. Catheter Cardiovasc Interv. 2003;60:180 –184.
42. Hildick-Smith DJ, Walsh JT, Lowe MD, Petch MC. Coronary angiography in the fully anticoagulated patient: the transradial route is successful and safe. Catheter Car-diovasc Interv. 2003;58:8 –10.
43. Lo TS, Buch AN, Hall IR, Hildick-Smith DJ, Nolan J. Percutaneous left and right heart catheterization in fully anticoagulated patients utilizing the radial artery and forearm vein: a two-center experience.
J Interv Cardiol. 2006;19:258 –263. 44. Brasselet C, Tassan S, Nazeyrollas P,
Hamon M, Metz D. Randomised comparison of femoral versus radial approach for percu-taneous coronary intervention using abciximab in acute myocardial infarction: results of the FARMI trial.Heart. 2007;93: 1556 –1561.
45. Chase AJ, Fretz EB, Warburton WP, Klinke WP, Carere RG, Pi D, Berry B, Hilton JD. Association of the arterial access site at angioplasty with transfusion and mortality: the M.O.R.T.A.L study (Mortality Benefit of Reduced Transfusion After Percutaneous Coronary Intervention via the Arm or Leg).
Heart. 2008;94:1019 –1025.
46. Karjalainen PP, Vikman S, Niemela M, Porela P, Ylitalo A, Vaittinen MA, Puurunen M, Airaksinen TJ, Nyman K, Vahlberg T, Airaksinen KE. Safety of percutaneous coronary intervention during uninterrupted oral anticoagulant treatment. Eur Heart J. 2008;29:1001–1010.
47. Schreiner GC, Laine L, Murphy SA, Cannon CP. Evaluation of proton pump inhibitor use in patients with acute coronary syndromes
based on risk factors for gastrointestinal bleed.Crit Pathw Cardiol. 2007;6:169 –172. 48. Chin MW, Yong G, Bulsara MK, Rankin J, Forbes GM. Predictive and protective factors associated with upper gastrointestinal bleeding after percutaneous coronary inter-vention: a case-control study.Am J Gastro-enterol. 2007;102:2411–2416.
49. Chan FK, Ching JY, Hung LC, Wong VW, Leung VK, Kung NN, Hui AJ, Wu JC, Leung WK, Lee VW, Lee KK, Lee YT, Lau JY, To KF, Chan HL, Chung SC, Sung JJ. Clopidogrel versus aspirin and esomeprazole to prevent recurrent ulcer bleeding.N Engl J Med. 2005;352:238 –244.
50. Sutfin T, Balmer K, Bostrom H, Eriksson S, Hoglund P, Paulsen O. Stereoselective inter-action of omeprazole with warfarin in healthy men. Ther Drug Monit. 1989;11: 176 –184.
51. Gilard M, Arnaud B, Cornily JC, Le Gal G, Lacut K, Le Calvez G, Mansourati J, Mottier D, Abgrall JF, Boschat J. Influence of ome-prazole on the antiplatelet action of clopi-dogrel associated with aspirin: the ran-domized, double-blind OCLA (Omeprazole Clopidogrel Aspirin) study. J Am Coll Cardiol. 2008;51:256 –260.
52. Ho PM, Maddox TM, Wang L, Fihn SD, Jesse RL, Peterson ED, Rumsfeld JS. Risk of adverse outcomes associated with concomitant use of clopidogrel and proton pump inhibitors following acute coronary syndrome. JAMA. 2009;301:937–944.
53. Andreotti F, Testa L, Biondi-Zoccai GG, Crea F. Aspirin plus warfarin compared to aspirin alone after acute coronary syn-dromes: an updated and comprehensive meta-analysis of 25,307 patients. Eur Heart J. 2006;27:519 –526.