Preterm Infant
’
s Early Crying Associated With Child
’
s
Behavioral Problems and Parents
’
Stress
WHAT’S KNOWN ON THIS SUBJECT: Preterm infants are at an increased risk of regulatory difficulties during infancy and of behavioral problems in childhood. In the full-term population, persistent crying problems that last beyond 3 months of age have been related to later behavioral problems.
WHAT THIS STUDY ADDS: Excessive crying by a preterm infant may reflect an increased risk for later behavioral problems and higher parenting stress even years later. Therefore, it is clinically relevant to assess systematically the crying behavior of preterm infants.
abstract
OBJECTIVE:To study how the early crying behavior of preterm infants at term, 6 weeks, and 5 months of corrected age is related to later behavioral problems at age 3 and 4 years and parenting stress at 2 and 4 years.
METHODS:The study group included 202 live-born, low birth weight infants (birth weight #1500 g) born from January 2001 through December 2006 at the Turku University Hospital, Finland. A Baby Day Diary was used to assess the preterm infants’ crying behavior at term, 6 weeks, and 5 months of corrected age. The children’s behavior was assessed using the Child Behavior Check List at 3 and 4 years old, and parenting stress was assessed by using the Parenting Stress Index when the child was 2 and 4 years old.
RESULTS:The duration and frequency of crying bouts in infancy was associated with Child Behavior Check List scores at 4 years old and to both mothers’and fathers’stress when the child was 2 and 4 years old.
CONCLUSIONS: Early excessive crying, especially if lasting up to 5 months of corrected age, is a clinically relevant signal in preterm infants because it may reflect infants’ regulatory problems and/or parenting stress. The crying behavior of preterm infants should be systematically inquired about at well-baby clinics.Pediatrics2014;133: e339–e345
AUTHORS:Riikka Korja, PhD,aMira Huhtala, MD,bJonna
Maunu, MD, PhD,aPäivi Rautava, MD, PhD,cLeena Haataja,
MD, PhD,b,dHelena Lapinleimu, MD, PhD,band Liisa
Lehtonen, MD, PhD,bon behalf of the PIPARI Study Group
Departments ofaChild Psychiatry,bPediatrics, anddChild Neurology, Turku University and Turku University Hospital, Turku, Finland; andcClinical Research Centre in Turku University Hospital and Department of Public Health, University of Turku, Finland
KEY WORDS
preterm infant, crying, behavior, parenting stress
ABBREVIATIONS
CBCL—Child Behavior Check List PSI—Parenting Stress Index
All authors are responsible for the reported research. All of the authors have participated in the concept; the design, analysis and interpretation of data; and the drafting or revising of the manuscript. In addition, all authors have approved the manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-1204 doi:10.1542/peds.2013-1204
Accepted for publication Oct 28, 2013
Address correspondence to Riikka Korja, PhD, Department of Child Psychiatry, Turku University Hospital, Kiinanmyllynkatu 4-8, 20520 Turku, Finland. E-mail: riikka.korja@utu.fi
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:Funding for the full-time research work was received from the Emil Aaltonen Foundation and by the Hospital District of South-West Finland. The funding sources had no role in the study design; in the collection, analysis, or interpretation of data; in the writing of the article; or in the decision to submit it for publication.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated
they have no potential conflicts of interest to disclose.
difficulties during infancy and for be-havioral problems in childhood.1–4During
infancy, 1 sign of regulatory problems is excessive crying and fussing. It has been suggested that an infant’s crying pattern is biologically based but may be modified by environmental factors, such as care-giving styles and physical holding.5–8In
test situations in previous studies, pre-term infants exhibited more irritability and difficulties in negative affect and state regulation.9,10However, in the home
environment, preterm infants have been shown to be comparable to full-term in-fants in the duration and the frequency of crying during thefirst months of life.11,12
Infants’prolonged crying is a common concern for parents; it causes family stress and frequent help seeking.13–15
Parents of preterm infants may be even more vulnerable to an infant’s prolonged crying; they may be overly sensitive to their infant’s negative signals and may already be stressed about his or her well-being. Mothers of preterm infants illus-trate more psychological distress during thefirst months after birth than mothers of full-term infants.16,17
Preterm infants’ behavioral, emotional, and neurologic problems at later ages have been shown to be multietiologic and explained in part by neurologic and cog-nitive deficits due to prematurity1,2,18–21
and psychosocial factors.22–24The role
of the preterm infant’s regulatory com-petence in the development of later be-havioral symptoms is still unknown. Persistent crying problems that last be-yond 3 months of age have been related to later hyperactivity and other behav-ioral problems in the full-term pop-ulation.25–27A meta-analysis showed that
full-term, healthy children with regu-latory problems, including excessive crying during infancy and sleeping problems, were more likely to experi-ence behavioral problems in child-hood than children without regulatory
milial problems, such as low socioeco-nomic status, maternal anxiety and depression, and problems in the mother-child relationship.26On the basis of this
meta-analysis, the authors suggested that initial deficits in regulatory compe-tencies and the control of stimuli may be early markers for similar processes of inadequate behavior control in child-hood.26More studies are needed for
better understanding of the early mark-ers and risk factors of behavioral prob-lems, especially in at-risk infants.
Given that there are no studies on early crying and later behavioral problems in preterm infants, we studied whether the duration and frequency of crying bouts at term, 6 weeks, and 5 months of corrected age were associated with (1) parent-reported behavioral problems when the child was 3 and 4 years old and/or (2) parenting stress related to the child when the child was 2 and 4 years old.
METHODS
Subjects and Procedure
This prospective study was part of a regional, multidisciplinary, follow-up study (Development and Functioning Outcome of Very Low Birth Weight In-fants From Infancy to School Age; the PIPARI Study). The Ethical Committee of the Hospital District of Southwest Finland approved the study protocol. Parents gave informed consent after receiving written and oral information.
The subjects were born at the Turku University Hospital, Finland, between January 2001 and December 2006; 259 families of very low birth weight pre-term children (birth weight#1500 g) were invited to participate in the study. From the 259 invited families, 6 declined to participate, and 40 infants died during the neonatal period. Among the remain-ing 213 families, 10 were excluded. Of these, 5 infants lived outside the catchment area of the hospital, 3 had
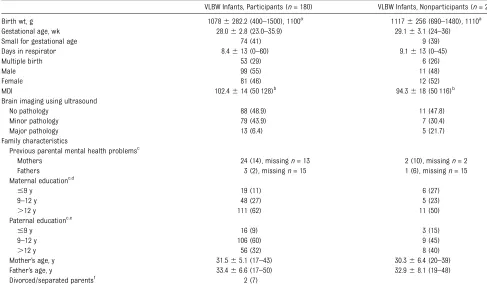
because of language problems. The characteristics of the study partic-ipants are presented in Table 1.
Neonatal background data were col-lected prospectively from medical rec-ords. The parents were asked for parental background data when the child was born and when child was 2 years’ cor-rected age. The brain pathology was
de-fined based on the cranial ultrasound examinations, which were obtained for all preterm infants. The infants were categorized into the 3 groups according to pathologic brain-imagingfindings: (1) normal, (2) minor brain pathology, and (3) major brain pathology. Children’s cognitive development was measured using Bayley Scales II28at 2 years’
cor-rected age. Infant medical records and family characteristics are presented in Table 1.
preterm infants of nonresponders. No other differences were found between nonresponders and responders.
Crying behavior of the preterm infants was assessed at term, 6 weeks, and 5 months’corrected age using the Baby
Day Diary.29 This well-validated method
tracks 5 categories of infant behavior: fussing, crying, sleeping, awake content, and feeding.29In the data analysis, the
combined crying and fussing behavior was assessed in 2 dimensions, the
du-ration and the frequency of crying bouts, which were calculated as a mean for a day. Descriptive values of the infant’s crying behavior are shown separately in the participants and in the nonpar-ticipants in Table 2. The parents (or a nurse in case of hospitalization) kept the diary for 3 days. The diary entries were to be completed on days the children were not ill or receiving vaccinations.
Children’s behavioral, social, and atten-tion problems were assessed at ages 3 and 4 using the CBCL for Ages 1.5–5.30
The CBCL 1.5–5 includes 100 items. Thirty-six items measure internalizing problems, and 24 items measure exter-nalizing problems, which are not mutu-ally exclusive. In this study, we used the total score of CBCL and scales of externalizing and internalizing problems TABLE 1 Characteristics of the Preterm Infants and Their Parents in Participants and Nonparticipants
VLBW Infants, Participants (n= 180) VLBW Infants, Nonparticipants (n= 23) Birth wt, g 10786282.2 (400–1500), 1100a 11176256 (690–1480), 1110a Gestational age, wk 28.062.8 (23.0–35.9) 29.163.1 (24–36)
Small for gestational age 74 (41) 9 (39)
Days in respirator 8.4613 (0–60) 9.1613 (0–45)
Multiple birth 53 (29) 6 (26)
Male 99 (55) 11 (48)
Female 81 (46) 12 (52)
MDI 102.4614 (50 128)b
94.3618 (50 116)b
Brain imaging using ultrasound
No pathology 88 (48.9) 11 (47.8)
Minor pathology 79 (43.9) 7 (30.4)
Major pathology 13 (6.4) 5 (21.7)
Family characteristics
Previous parental mental health problemsc
Mothers 24 (14), missingn= 13 2 (10), missingn= 2
Fathers 3 (2), missingn= 15 1 (6), missingn= 15
Maternal educationc,d
#9 y 19 (11) 6 (27)
9–12 y 48 (27) 5 (23)
.12 y 111 (62) 11 (50)
Paternal educationc,e
#9 y 16 (9) 3 (15)
9–12 y 106 (60) 9 (45)
.12 y 56 (32) 8 (40)
Mother’s age, y 31.565.1 (17–43) 30.366.4 (20–39)
Father’s age, y 33.466.6 (17–50) 32.968.1 (19–48)
Divorced/separated parentsf
2 (7)
Numbers are mean6SD (range) orn(%) unless otherwise noted. Small for gestational age is defined as a birth weight#2.0 SD according to the age- and gender-specific Finnish growth charts. MDI, Mental Development Index of Bayley Scales II; VLBW, very low birth weight.
aMedian.
bP,.05,x2= 4.24.
cAsked when the child was born.
dMissing data,n= 3.
eMissing data,n= 5.
fAsked when the child was 2 years’corrected age; missingn= 21.
TABLE 2 Descriptive Values of the Crying Variables and a Group Comparison Between Participants and Nonparticipants
Participants (n= 180) Nonparticipants (n= 23)
Participants (n= 180) Highest Quartile (25%)
Mean SD Mean SD
Duration of crying
At term 136.4 82.1 137.1 95.9 .178.3 min/d At 6 wk 126.1 70.3 135.7 79.1 .163.3 min/d At 5 mo 77.28a 45.9a 111.4a 97.8a .106.6 min/d Frequency of crying
At term 9.8 5.8 8.2 5.0 .12.6 bouts/d
At 6 wk 10.6 6.6 9.2 6.5 .14.3 bouts/d
At 5 mo 7.8 5.6 6.9 5.0 .10.7 bouts/d
aP,.05,x2= 4.24.
have been reported in detail elsewhere.31
Only 10 infants (7.1%) had a total score
.90 percentile.31 The questionnaires
were sent by mail 2 weeks before the planned assessment point. The parents completed the questionnaire based on the child’s behavior during the past 2 months. At the 3-year assessment, 64% of CBCL questionnaires were completed by mothers, 6% of questionnaires were completed by fathers, and 30% of ques-tionnaires were completed jointly by both mothers and fathers. At the 4-year as-sessment, 72% of CBCL questionnaires were completed by mothers only, 6% of questionnaires were completed by fathers, and 21% of questionnaires were completed jointly by both mothers and fathers. Data included only opposite-gender parents.
Parenting stress related to the child’s behavior and temperament was as-sessed using the PSI when the child was 2 and 4 years old.32The questionnaire
in-cluded 120 items. The PSI consisted of a child domain (6 subscales), a parent domain (7 subscales), and life stress evaluation. Only the total score of the child’s domains was used in the analysis of the association between crying and parental stress. The total score of pa-rents’domains was used as a control variable in the analysis of the associa-tion between crying and child’s behav-ior. The assessments were used as a continuous measure. The descriptive values of the PSI in this population have been reported in detail elsewhere.31The
questionnaires were sent by mail 2 weeks before the planned assessment point to all fathers and mothers, in-cluding parents living in separate households. In 80% of participating families, both parents completed the questionnaire.
Statistics
The associations between background variables and nonparticipation were
x
test for trend in ordinal variables, and logistic regression in continuous vari-ables. The associations of the duration and frequency of crying to childhood behavioral problems and to parenting stress were analyzed using a mixed, repeated-measures analysis using the SAS MIXED procedure with compound symmetry covariance structure. Un-standardized regression coefficients are presented in tables. The essential medical factors of the infant and family characteristics were controlled to help to explain the relationship between early crying and later behavior and parenting stress. Controlled variables included the child’s brain pathology found by neonatal ultrasound, gesta-tional age, small for gestagesta-tional age status, and the duration of mechanical respiratory support, as well as the parents’educational level, single par-enthood, and parents’previous mental health issues. In addition, the associa-tion between early crying and a child’s behavior was analyzed by controlling maternal stress (ie, the total score of parents’domain by using PSI).
The correlations between crying vari-ables were studied by using the Pearson correlation coefficient. The data were analyzed by using SAS for Windows, version 9.2 (SAS Institute, Cary, NC). Differences were considered statisti-cally significant if thePvalue was#.05.
RESULTS
Potentially confounding infant factors (gender, gestational age, small for gestational age status, length of the respiratory treatment, and brain pa-thology) were not associated with any of the CBCL or PSI subscales. The potentially confounding family factors (parents’ education, family structure, or mother’s previous mental health problems) also were not associated with the CBCL or PSI subscales. However, parental stress
fi
every subscale of CBCL and with the total score of child’s domain in PSI. Fur-thermore, married mothers reported less child-related stress (PSI) than un-married mothers.
The duration of crying at 6 weeks’and 5 months’corrected age was associated with both the externalizing and in-ternalizing symptoms and with the to-tal score of behavioral symptoms at age 4 years. Furthermore, the frequency of crying bouts at 6 weeks’ and 5 months’of corrected age was associ-ated with the externalizing symptoms and with the total score of behavioral symptoms but not with the internalizing symptoms at 4 years old. There were no statistically significant associations be-tween the duration of crying at 6 weeks and at 5 months and the total score of behavioral symptoms at 3 years, al-though P values were ,.10. Further-more, the frequency of crying was not significantly associated at 5 months with externalizing symptoms or with the total score of behavioral symptoms at 3 years, althoughPvalues were,.10.
crying to childhood behavior and pa-rental stress are presented in Tables 3 and 4. Diagnostic plots indicated that the effect of crying on the later behav-ior seems to be approximately linear across the entire range.
The duration of crying at term correlated with the duration of crying at 6 weeks (r= 0.51,P,.0001) and at 5 months (r= 0.26,P,.0001). The duration of crying at 6 weeks correlated with the duration of crying at 5 months of corrected age (0.42,P,.0001). Furthermore, the fre-quency of crying at term correlated with the frequency of crying at 6 weeks (r= 0.71,P,.0001) and at 5 months (r= .51,P,.0001). The frequency of crying at 6 weeks correlated with the frequency of crying at 5 months of corrected age (0.75,P,.0001).
DISCUSSION
The current study demonstrates that longer duration and higher frequency of crying bouts in preterm infants were associated with a higher prevalence of parent-reported behavioral symptoms and higher parental stress for mothers and fathers when the child was at preschool age. The relation of infant crying to childhood behavior and par-enting stress was adjusted for several infants’medical factors, the parents’ socioeconomic circumstances, and parent mental health factors. Associa-tion was stronger at 5 months’and at 6 weeks corrected age than at term. The frequency and the duration of crying correlated strongly among the 3 time points. Our results suggest that per-sistent crying reported at 5 months’
corrected age is related to the later parent-reported behavioral problems. Ourfindings also suggest that infants’ early regulatory problems are more related to externalizing symptoms than to internalizing symptoms. However, it is possible that the internalizing symp-toms are more difficult to recognize as potential externalizing symptoms at preschool age. Ourfindings are consis-tent with the studies of full-term infants who cried excessively beyond thefirst 3 months and exhibited a higher preva-lence of externalizing behavioral prob-lems and more family distress.13,25–27
Our findings support the suggestion that ineffective regulatory competences may be an early precursor of the less effective regulation of behavior later in childhood.26This may be even more
ev-ident in preterm infants because of bi-ological vulnerability.
The possible explanations for preschool behavioral problems that occur after excessive infant crying might be bi-ological, psychosocial, or both. Com-bined with preterm birth, prolonged crying may complicate the development of attachment between a preterm infant and the parents, potentially causing behavioral problems at a later age. Crying is a vital capability for a newborn infant, but when an infant cries often and for long periods, the parents are un-derstandably concerned and stressed when they do not receive positive TABLE 3 Associations Between Crying Behavior Measures and Child’s Behavior Analyzed by
Repeated Measures
Child’s Behavior Duration of Crying (min/d) Frequency of Crying Bouts (bouts/d)
Term, E (SE) 6 Wk, E (SE) 5 Mo, E (SE) Term, E (SE) 6 Wk, E (SE) 5 Mo, E (SE) CBCL total at 3 0.20 (0.15) 0.35 (0.21)#
0.64 (0.33)#
0.17 (0.22) 0.29 (0.21) 0.48 (0.26)#
CBCL total at 4 0.21 (0.19) 0.72 (0.22)** 0.95 (0.33)** 0.03 (0.25) 0.49 (0.22)* 0.65 (0.27)* CBCL internal at 3 0.09 (0.06) 0.08 (0.07) 0.12 (0.11) 0.02 (0.09) 0.02 (0.08) 0.12 (0.09) CBCL internal at 4 0.09 (0.06) 0.22 (0.08)** 0.24 (0.11)* 0.14 (0.08) 0.10 (0.08) 0.12 (0.09) CBCL external at 3 0.05 (0.08) 0.16 (0.09)#
0.27 (0.14)#
0.01 (0.10) 0.11 (0.09) 0.18 (0.10)#
CBCL external at 4 0.07 (0.07) 0.29 (0.09)** 0.46 (0.14)** 0.13 (0.10) 0.25 (0.09)** 0.32 (0.11)**
Analyses were controlled for the child’s brain pathology, gestational age, birth weight, small for gestational age status, and duration of mechanical respiratory support or by the parents’educational level, single parenthood, parents’previous mental health problems, and maternal stress. E, the unstandardized regression coefficient describes how much the CBCL/PSI score is estimated to increase if the duration of crying is increased to 10 min or if the frequency of crying is increased to 1 bout. * Significant atP,.05.
** Significant atP,.01. ***P,.001.
#P,.10.
TABLE 4 Associations Between Crying Behavior Measures and Parent’s Child-Related Stress Analyzed by Repeated Measures
Child’s Behavior: PSI Child Score Duration of Crying (min/d) Frequency of Crying Bouts (bouts/d)
Term, E (SE) 6 Wk, E (SE) 5 Mo, E (SE) Term, E (SE) 6 Wk, E (SE) 5 Mo, E (SE) Father’s report
At age 2 0.42 (0.27) 0.56 (0.26)* 0.06 (0.42) 0.66 (0.33) 0.55 (0.30) 0.33 (0.34) At age 4 0.66 (0.25)** 0.94 (0.28)** 0.35 (0.42) 0.49 (0.39)* 0.56 (0.30) 0.52 (0.32) Mother’s report
At age 2 0.76 (0.22)** 0.83 (0.28) 1.03 (0.43)* 1.07 (0.33)** 0.80 (0.28)* 1.11 (0.34)** At age 4 0.82 (0.22)*** 1.02 (0.26)*** 0.83 (0.42)* 0.93 (0.33)** 0.42 (0.28) 0.63 (0.35)
Analyses were controlled for the child’s brain pathology, gestational age, birth weight, small for gestational age status, and duration of mechanical respiratory support or by the parents’ educational level or single parenthood and for the parents’previous mental health problems. E, the unstandardized regression coefficient describes how much the CBCL/PSI score is estimated to increase if the duration of crying is increased to 10 min or if the frequency of crying is increased to 1 bout.
*P,.05. **P,.01. ***P,.001.
response to infants’ regulatory needs. Preterm birth and the related concerns for the health of the child challenge parents and increase their risk for stress, depression, and anxiety.8,9It has
been previously indicated that pro-longed crying in preterm infants, but not in full-term infants, is associated with less maternal emotional involve-ment and communication, suggesting that the mothers of preterm infants are more vulnerable to the impact of pro-longed crying.33Furthermore, ourfi
nd-ings indicated a strong association between maternal stress and parent-reported behavioral problems. This re-sult suggests that parental stress may have a mediating role between crying and behavior. However, the association was also discovered when the effect of maternal stress was controlled. The association between crying and behav-ior might also reflect some underlying neurologic issues or other physical components, which were not controlled in the current study. On the other hand, even in early infancy, crying problems may reflect parenting problems. In full-term infants, the relation between ex-cessive early crying and later behav-ioral problems is strongest in families with multiple problems.8These possible
explanations for the association be-tween early crying and later behavioral and parenting problems are not mu-tually exclusive but can act simulta-neously.
Assessing infants’ crying and chil-dren’s behavior with parental reports
maternal-reported dysregulation at 6 months and maternal-reported behav-ior problems but not with youths’ self-reported problems, suggesting that a mother’s psychological well-being and social factors partly explain those associations. However, in the current study, the relation between crying and a child’s behavior was ad-justed for the parent’s mental health factors. Furthermore, both parents completed the questionnaires at pre-school age, and nurses partiallyfilled out the crying diary. Using several reporters diminishes the effect of the reporting bias and increases the data’s credibility. Another limitation of this study was the lack of a control group of full-term infants. Therefore, this study does not indicate whether the relation between crying and behavior also exists in full-term infants. The third limitation of this study is the in-complete follow-up. Preterm infants of the nonresponding families cried more at 5 months than in the responding families, which is in line with a pre-vious study showing more behavioral problems in the sample of dropouts.34
Therefore, we had a limited opportu-nity to assess the role of extremes in crying duration.
CONCLUSIONS
Our study showed that regulatory problems in early infancy are associ-ated with parent-reported preschool behavioral problems and parenting stress. Biological vulnerability combined
contribute to the strong association between infant crying and later parent-reported behavioral problems. In the clinical context, excessive crying re-ported at 5 months may be a sign of an infant’s regulatory and/or parenting problems. Accordingly, it is clinically rel-evant to inquire systematically about the crying behavior of preterm infants at well-baby clinics. For families re-porting increased infant crying, targeted treatment and preventive interventions should be developed to enhance preterm infants’ regulatory capacity and to re-duce parental stress.
ACKNOWLEDGMENTS
The PIPARI Study Group includes Mikael Ekblad, BM; Satu Ekblad, RN; Eeva Ekholm, MD, PhD; Leena Haataja, MD, professor; Mira Huhtala, MD; Pentti Kero, MD, PhD; Riikka Korja, PhD; Harry Kujari, MD; Helena Lapinleimu, MD, PhD; Liisa Lehtonen, MD, PhD; Marika Leppänen, MD; Annika Lind, MA; Hanna Manninen, MD; Jonna Maunu, MD, PhD; Jaakko Matomäki, MSc; Petriina Munck, MA; Pekka Niemi, professor; Pertti Palo, MD, PhD; Riitta Parkkola, MD, PhD; Jorma Piha, MD, professor; Liisi Rautava, MD, PhD; Päivi Rautava, MD, professor; Hellevi Rikalainen, MD, PhD; Katriina Saarinen, physiotherapist; Elina Savonlahti, MD; Matti Sillanpää, MD, professor; Suvi Stolt, PhD; Päivi Tuomikoski-Koiranen, RN; Milla Ylijoki, MD, PhD; and Tuula Äärimaa, MD, PhD. We thank Jaakko Matomäki for his help and advice in the data analysis.
REFERENCES
1. Ferrari F, Grosoli MV, Fontana G, Cavazzuti
GB. Neurobehavioural comparison of
low-risk preterm and fullterm infants at term
conceptional age. Dev Med Child Neurol.
1983;25(4):450–458
2. Bhutta AT, Cleves MA, Casey PH, Cradock
MM, Anand KJS. Cognitive and behavioral
outcomes of school-aged children who
were born preterm: a meta-analysis.JAMA.
2002;288(6):728–737
3. Minde K.Prematurity and Serious Medical
Conditions in Infancy. Handbook of Infant
Mental Health. New York, NY: Guildford
Press; 2002:211–234
4. Hayes B, Sharif F. Behavioural and
emotional outcome of very low bir th
weight infants—literature review.
J Matern Fetal Med. 2009;22(10):849–
856
5. Brazelton TB. Crying in infancy.Pediatrics.
6. Barr RG. The normal crying curve: what do we really know? Dev Med Child Neurol. 1990;32(4):356–362
7. St James-Roberts I, Halil T. Infant crying patterns in thefirst year: normal commu-nity and clinical findings.J Child Psychol Psychiatry. 1991;32(6):951–968
8. Rautava P, Lehtonen L, Helenius H, Sillanpää M. Effect of newborn hospitalization on family and child behavior: a 12-year follow-up study.Pediatrics. 2003;111(2):277–283
9. Thoman EB, Graham SE. Self-regulation of stimulation by premature infants. Pediat-rics. 1986;78(5):855–860
10. Wolf MJ, Koldewijn K, Beelen A, Smith B, Hedlund R, de Groot IJM. Neurobehavioral and developmental profile of very low birthweight preterm infants in early in-fancy.Acta Paediatr. 2002:91:930–938
11. Barr RG, Chen S, Hopkins B, Westra T. Cry-ing patterns in preterm infants. Dev Med Child Neurol. 1996;38(4):345–355
12. Maunu J, Kirjavainen J, Korja R, et al; PIPARI Study Group. Relation of prematurity and brain injury to crying behavior in infancy. Pediatrics. 2006;118(1). Available at: www. pediatrics.org/cgi/content/full/118/1/e57
13. Rautava P, Helenius H, Lehtonen L. Psycho-social predisposing factors for infantile colic.BMJ. 1993;307(6904):600–604
14. Forsyth BW, Leventhal JM, McCarthy PL. Mothers’perceptions of problems of feed-ing and cryfeed-ing behaviors. A prospective study.Am J Dis Child. 1985;139(3):269–272
15. St James-Roberts I. Infant crying and sleeping: helping parents to prevent and manage problems. Prim Care. 2008;35(3):
547–567, viii
16. Singer LT, Salvator A, Guo S, Collin M, Lilien L, Baley J. Maternal psychological distress
and parenting stress after the birth of a very low-birth-weight infant.JAMA. 1999; 281(9):799–805
17. Davis L, Edwards H, Mohay H, Wollin J. The impact of very premature birth on the psychological health of mothers.Early Hum Dev. 2003;73(1-2):61–70
18. Chapieski ML, Evankovich KD. Behavioral effects of prematurity. Semin Perinatol. 1997;21(3):221–239
19. Janssens A, Uvin K, Van Impe H, Laroche SMF, Van Reempts P, Deboutte D. Psycho-pathology among preterm infants using the Diagnostic Classification Zero to Three. Acta Paediatr. 2009;98(12):1988–1993
20. Hack M, Youngstrom EA, Cartar L, et al. Behavioral outcomes and evidence of psy-chopathology among very low birth weight infants at age 20 years. Pediatrics. 2004; 114(4):932–940
21. Heinonen K, Räikkönen K, Pesonen AK, et al. Behavioural symptoms of attention deficit/ hyperactivity disorder in preterm and term children born small and appropriate for gestational age: a longitudinal study.BMC Pediatr. 2010;10:91
22. Miceli PJ, Goeke-Morey MC, Whitman TL, Kolberg KS, Miller-Loncar C, White RD. Brief report: birth status, medical complications, and social environment: individual differ-ences in development of preterm, very low birth weight infants. J Pediatr Psychol. 2000;25(5):353–358
23. Elgen I, Sommerfelt K, Markestad T. Population based, controlled study of behavioural prob-lems and psychiatric disorders in low birth-weight children at 11 years of age.Arch Dis Child Fetal Neonatal Ed. 2002;87(2):F128–F132
24. Huhtala M, Korja R, Lehtonen L, Haataja L, Lapinleimu H, Rautava P; PIPARI Study Group. Parental psychological well-being and behavioral outcome of very low birth weight infants at 3 years.Pediatrics. 2012; 129(4). Available at: www.pediatrics.org/ cgi/content/full/129/4/e937
25. Wolke D, Rizzo P, Woods S. Persistent infant crying and hyperactivity problems in
mid-dle childhood. Pediatrics. 2002;109(6): 1054–1060
26. Hemmi MH, Wolke D, Schneider S.
Associ-ations between problems with crying,
sleeping and/or feeding in infancy and long-term behavioural outcomes in
child-hood: a meta-analysis.Arch Dis Child. 2011; 96(7):622–629
27. Hyde R, O’Callaghan MJ, Bor W, Williams
GM, Najman JM. Long-term outcomes of
infant behavioral dysregulation.Pediatrics. 2012;130(5). Available at: www.pediatrics.
org/cgi/content/full/130/5/e1243
28. Bayley N. Bayley Scales of Infant De-velopment—II. San Antonio, TX:
Psycholog-ical Corporation; 1993
29. Barr RG, Kramer MS, Boisjoly C,
McVey-White L, Pless IB. Parental diary of infant cry and fuss behaviour. Arch Dis Child.
1988;63(4):380–387
30. Achenbach T.Manual for the Child Behavior Checklist 4–18 and 1.5–5. Profile.
Burling-ton, VT: Department of Psychiatry, Univer-sity of Vermont; 2001
31. Huhtala M, Korja R, Lehtonen L, et al; PIPARI
Study Group. Parental psychological
well-being and cognitive development of very low birth weight infants at 2 years. Acta
Paediatr. 2011;100(12):1555–1560
32. Abidin RR. Parenting Stress Index. Pro-fessional Manual. Odessa, FL: Psychological
Assessment Resources, 1995
33. Korja R, Maunu J, Kirjavainen J, et al; PIPARI Study Group. Mother-infant interaction is
influenced by the amount of holding in
preterm infants.Early Hum Dev. 2008;84(4): 257–267
34. Wolke D, Waylen A, Samara M, et al.
Se-lective drop-out in longitudinal studies and non-biased prediction of behaviour
dis-orders. Br J Psychiatry. 2009;195(3):249–
256
DOI: 10.1542/peds.2013-1204 originally published online January 6, 2014;
2014;133;e339
Pediatrics
Lapinleimu and Liisa Lehtonen
Riikka Korja, Mira Huhtala, Jonna Maunu, Päivi Rautava, Leena Haataja, Helena
Services
Updated Information &
http://pediatrics.aappublications.org/content/133/2/e339 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/133/2/e339#BIBL This article cites 28 articles, 13 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
ub
http://www.aappublications.org/cgi/collection/psychosocial_issues_s Psychosocial Issues
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2013-1204 originally published online January 6, 2014;
2014;133;e339
Pediatrics
Lapinleimu and Liisa Lehtonen
Riikka Korja, Mira Huhtala, Jonna Maunu, Päivi Rautava, Leena Haataja, Helena
Parents' Stress
Preterm Infant's Early Crying Associated With Child's Behavioral Problems and
http://pediatrics.aappublications.org/content/133/2/e339
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.