Copyright © 2001, American Society for Microbiology. All Rights Reserved.
Rapid Identification of Yeasts in Positive Blood Cultures by
a Multiplex PCR Method
HSEIN CHANG CHANG,
1SHIANG NING LEAW,
1AY HUEY HUANG,
2TSU LAN WU,
3ANDTSUNG CHAIN CHANG
4*
Institute of Biomedical Engineering
1and Department of Medical Technology, College of Medicine,
4National Cheng
Kung University, Department of Pathology, National Cheng Kung University Hospital,
2and Department
of Clinical Pathology, Linko Medical Center, Chang Gung Memorial Hospital,
3Tainan 701, Taiwan, Republic of China
Received 6 December 2000/Returned for modification 30 April 2001/Accepted 20 July 2001
Yeasts are emerging as important etiological agents of nosocomial bloodstream infections. A multiplex PCR
method was developed to rapidly identify clinically important yeasts that cause fungemia. The method
ampli-fied the internal transcribed spacer 1 (ITS1) region between the 18S and 5.8S rRNA genes and a specific DNA
fragment within the ITS2 region of
Candida albicans
. With this method,
C
.
albicans
produced two amplicons,
whereas other species produced only one. Through sequence analysis, the precise lengths of the PCR products
were found to be as follows:
C
.
glabrata
(482 or 483 bp),
C
.
guilliermondii
(248 bp),
C
.
parapsilosis
(229 bp),
C
.
al-bicans
(218 or 219 and 110 bp),
C
.
tropicalis
(218 bp),
Cryptococcus neoformans
(201 bp), and
C
.
krusei
(182 bp).
The PCR products could be effectively separated by disk polyacrylamide gel electrophoresis. The method was
used to test 249 positive blood cultures (255 isolates), from which the following species (strain number) were
isolated:
C
.
albicans
(128),
C
.
tropicalis
(51),
C
.
glabrata
(28),
C
.
parapsilosis
(23),
C. neoformans
(9),
C
.
krusei
(5),
C
.
guilliermondii
(3), and other, minor species (8). The test sensitivity of the method was 96.9% (247 of 255
isolates). The eight minor species were either misidentified (one strain) or not identified (seven strains). From
the time at which a positive bottle was found, the multiplex PCR could be completed within 8 h; the present
method is simpler than any previously reported molecular method for the identification of blood yeasts.
Yeasts are emerging as important etiological agents of
bloodstream infections (22, 23), a complication associated with
a high mortality rate (1, 3). This problem is compounded by an
increase in resistance to antifungal agents, particularly the
azoles (8, 18, 22, 25, 28, 29, 31) and amphotericin B (19).
Bloodstream fungal infections constitute a serious health
prob-lem because of the excessive hospital stay, added health care
costs, and high morbidity and mortality attributed to the
dis-eases (39).
Candida albicans
,
C. tropicalis
,
C. glabrata
,
C. parapsilosis
,
C. krusei
, and
Cryptococcus neoformans
are the most common
yeasts causing bloodstream infections (2, 23). These six species
may account for 95 to 98% of all blood yeasts (19, 23, 27).
C. guilliermondii
and other, minor species may be isolated
occasionally (2, 32). The rates of isolation of the major yeast
species causing fungemia have been determined in several
studies:
C. albicans
(50 to 59%), C.
tropicalis
(11 to 25%),
C. glabrata
(8 to 18%),
C. parapsilosis
(7 to 15%),
C. krusei
(2
to 4%),
C. neoformans
(⬃2%), and other species (⬃2%) (1, 19,
23, 27, 28). Therefore, rapid identification of blood yeasts
could be targeted solely for these species, although the
possi-bility of other, rarely encountered species always exists.
Fluconazole, which has a low level of toxicity, has been
reported to be as effective as amphotericin B for the treatment
of candidemia in patients without neutropenia (26), although
C. glabrata
and
C. krusei
are innately more resistant to
flucon-azole. The MIC50s of fluconazole for
C. krusei
and
C. glabrata
are 32 and 16
g/ml, respectively; both values are much higher
than those for
C. albicans
(0.25
g/ml),
C. tropicalis
(1
g/ml),
and
C. parapsilosis
(1
g/ml) (23). Therefore, earlier
informa-tion regarding the species causing fungemia may help
physi-cians to select appropriate antifungal agents and regimens to
treat patients. The rate of isolation of
C. glabrata
from blood
cultures has increased from 8% during the period from 1952 to
1992 to 18 to 20% in recent surveys (22, 23). This increase
might be due to the widespread use of fluconazole for
prophy-laxis and treatment of candidiasis, affirming the need for more
rapid and accurate identification.
At present, the identification of yeasts in positive blood
cultures by use of conventional morphological and metabolic
characteristics requires from one to several days after isolation.
In order to decrease that time, methods devised for the rapid
diagnosis of fungal infections include detection of antibody
(42), cell wall mannan (5), enolase (37), and specific antibody
in combination with PCR to detect
C. albicans
DNA (15).
Efforts have been directed toward molecular testing, such as
the use of rRNA genes (rDNA), for species identification.
PCR followed by hybridization of the amplicons with
species-specific probes has also been used to detect a variety of fungi
(6, 7, 9–11, 21, 24, 30, 35, 36). Nested PCR (13, 17, 20, 33) or
PCR followed by restriction enzyme analysis (16, 41) has also
been used to detect several fungal pathogens. The above
meth-ods have shown promise for the diagnosis of fungal infections
but have problems that prevent their routine use in a clinical
laboratory. For example, the DNA hybridization technique
normally involves multiple steps of incubation and washing
* Corresponding author. Mailing address: Department of Medical
Technology, College of Medicine, National Cheng Kung University,
1 University Rd., Tainan 701, Taiwan, Republic of China. Phone:
886-6-235-3535, ext. 5790. Fax: 886-6-236-3956. E-mail: tsungcha@mail
.ncku.edu.tw.
3466
on May 15, 2020 by guest
http://jcm.asm.org/
under stringently controlled conditions, which are both
time-consuming and cumbersome. The use of nested PCR or PCR
in conjunction with restriction enzyme analysis, however, may
add needless complexity to assay procedures.
Recently, a fluorescent capillary electrophoresis system was
developed to identify fungi by use of the length variability of
the internal transcribed spacer 2 (ITS2) genetic region (34).
However, the fragment lengths of the ITS2 regions were
sim-ilar in several important yeasts that cause fungemia, thereby
preventing the identification of some species. The aim of the
present study was to evaluate a multiplex PCR method for the
identification of
C. neoformans
and
Candida
species that are
frequently isolated from blood cultures. The method was based
on the size variability of the ITS1 regions in different species
and on the amplification of a specific DNA fragment of the
ITS2 region of
C. albicans
.
MATERIALS AND METHODS
Yeast strains.A total of 22 stock yeast cultures were used in this study (Table 1). Among these cultures, 18 strains were obtained from the Culture Collection and Research Center (CCRC, Hsinchu, Taiwan), and the remaining 4 strains were clinical isolates.
DNA extraction from pure cultures.Stock cultures of yeasts were subcultured on Sabouraud dextrose agar (Difco, Detroit, Mich.) and incubated at 37°C. Col-onies of these strains were suspended in saline to obtain the turbidity of a 0.5 McFarland standard at a 530-nm wavelength. Two microliters of cell suspension was added to 18l of microLYSIS solution (Microzone Limited, East Sussex, United Kingdom) in a 0.2-ml Eppendorf tube and overlaid with 20l of steril-ized mineral oil. The tube was heated in a thermal cycler (OmniGen; Hybaid Limited, Middlesex, United Kingdom) using the following temperature profile, as recommended by the manufacturer: 65°C, 5 min; 96°C, 2 min; 65°C, 4 min; 96°C, 1 min; 65°C, 1 min; 96°C, 30 s; and 30°C, 5 min. After cycling, the lysis solution-DNA mixture was used directly for PCR amplification or stored at
⫺20°C for further use.Escherichia coliATCC 25922,Staphylococcus aureus0400, Klebsiella pneumoniae 03583, Enterobacter cloacae 00109, andStreptococcus pneumoniae0424 were cultivated on blood agar at 37°C for 18 to 24 h, and the bacterial DNA was extracted in a manner similar to that used for pure yeast cultures.
Clinical specimens.Blood samples were collected from the National Cheng Kung University Medical Center, Tainan, Taiwan, and from Chang Gung Me-morial Hospital. BACTEC blood culture bottles (Becton Dickinson Microbiol-ogy Systems, Cockeysville, Md.) were normally inoculated with 3 to 10 ml of blood from patients, inserted into the BACTEC NR660 instrument (Becton Dickinson Microbiology Systems), and incubated at 37°C. Gram stain smears of aliquots from positive bottles were prepared to check for the presence of yeasts. A total of 249 positive blood culture bottles containing yeasts were analyzed in this study. The blood yeasts isolated on subculture plates were identified by conventional procedures based on phenotypic and biochemical reactions (38).
Isolation of yeast DNA from positive blood cultures.The method of Fujita et al. (9) was used with a small modification to extract yeast DNA from the positive culture broths. An aliquot (0.2 ml) of positive broth containing yeasts was added to 0.8 ml of TE buffer (10 mM Tris-HCl, 1 mM EDTA [pH 8.0]) containing 0.05% proteinase K (Worthington Biochemical Inc., Lakewood, N.J.) and 0.05% Tween 20. The cell suspension was incubated at 55°C for 30 min and then centrifuged at 8,000⫻gfor 10 min in a microcentrifuge. The pellet was washed with 0.5 ml of TE buffer containing 0.5% Tween 20 and then with 0.5 ml of SE solution (1 M sorbitol, 0.1 M EDTA). After centrifugation at 8,000⫻gfor 10 min, the pellet was suspended in 0.5 ml of Lyticase solution (10 mg/ml; Sigma Chemical Co., St. Louis, Mo.) and incubated at 37°C for 1 h. After centrifuga-tion, the pellet was suspended in 10l of TE buffer, and 1l of the suspension was added to 19l of microLYSIS solution. The suspension was heated in a thermal cycler to extract yeast DNA as previously described for pure cultures. Seven randomly selected positive blood cultures containing bacteria were pro-cessed in the same manner for DNA extraction. In addition, DNA was extracted from two blood samples from healthy individuals for PCR assay.
PCR amplification.The fungus-specific, universal primers ITS1 (5⬘-TCC GTA GGT GAA CCT GCG G-3⬘) and ITS2 (5⬘-GCT GCG TTC TTC ATC GAT GC-3⬘) (40) were used to amplify a small conserved portion of the 18S rDNA region, the adjacent ITS1, and a small portion of the 28S rDNA region. In addition,C. albicans-specific primers CA3 (5⬘-GGT TTG CTT GAA AGA CGG TAG-3⬘) and CA4 (5⬘-AGT TTG AAG ATA TAC GTG GTA G-3⬘) (12) were also included in the PCR mixture to amplify a portion of the ITS2 region of C. albicans. The four primers (ITS1, ITS2, CA3, and CA4) were synthesized at TIB MOLBIOL (Berlin, Germany). Multiplex PCR was performed with 2l (1 to 5 ng) of template DNA in a total reaction volume of 50l consisting of 10 mM Tris-HCl (pH 8.3), 50 mM KCl, 1.5 mM MgCl2, 0.8 mM deoxyribonucleoside triphosphates (0.2 mM each), 3.2M primers (ITS1 and ITS2, 0.4M each; CA3 and CA4, 1.2M each),TaqDNA polymerase (1.25 U), and 50l of a mineral oil overlay. PCR was carried out with an OmniGen thermal cycler under the following conditions: initial denaturation, 94°C, 3 min; 35 cycles of denaturation (94°C, 1 min), annealing (60°C, 1 min), and extension (72°C, 1 min); and final extension, 72°C, 5 min. A negative control run was performed with each test run by replacing the template DNA with sterilized water in the PCR mixture. A positive culture broth containingC. albicanswas run in parallel with unknown samples, and this culture broth was used as a positive control.
Limit of detection ofC.albicansin blood.To determine the limit of detection of the multiplex PCR, whole blood was seeded withC. albicansCCRC 20512 to reach a concentration of 2⫻105CFU/ml. The seeded blood was serially diluted 10-fold with whole blood, and 0.2 ml of the diluted samples was used for PCR as described above. The cell numbers (CFU per milliliter) of the diluted cell suspensions were determined by the plate count method (11) with Sabouraud dextrose agar as the culture medium. Plates were incubated at 35°C for 48 h before enumeration.
Determination of the lengths of the PCR products.To determine the precise lengths of the PCR products amplified by primers ITS1 and ITS2, the amplicons were purified by using a PCR cleanup kit (Viogene, Sunnyvale, Calif.) and were directly cycle sequenced in both directions with an ABI Prism 377 automated system (Applied Biosystems, Taipei, Taiwan). The size of the fragment amplified fromC. albicansby primers CA3 and CA4 was determined in a similar way. For each species, two to five strains were sequenced in both directions to determine the precise lengths of the amplicons (Table 1). The PCR products of several minor species (C. famata,C. lusitaniae,C. pelliculosa,Rhodotorula rubra, and Trichosporon beigelii) isolated in this study were also sequenced to determine the precise lengths of their amplicons.
[image:2.587.43.282.92.368.2]Disk PAGE.PCR products were analyzed by disk polyacrylamide gel electro-phoresis (PAGE) (4) with a minigel system (Mini-Protean II; Bio-Rad, Hercules,
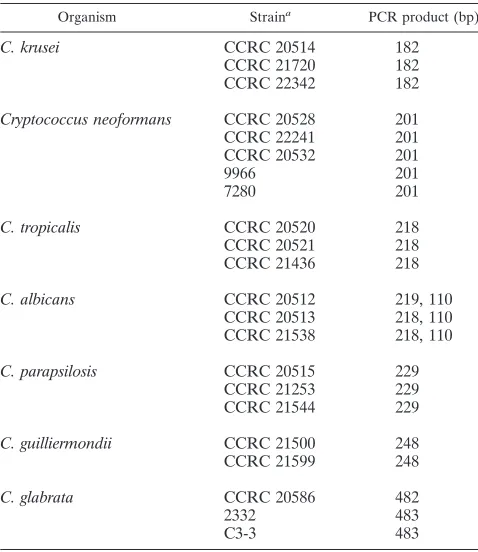
TABLE 1. Pure yeast cultures used in this study and
the lengths of PCR products
Organism Straina PCR product (bp)
C. krusei
CCRC 20514
182
CCRC 21720
182
CCRC 22342
182
Cryptococcus neoformans
CCRC 20528
201
CCRC 22241
201
CCRC 20532
201
9966
201
7280
201
C. tropicalis
CCRC 20520
218
CCRC 20521
218
CCRC 21436
218
C. albicans
CCRC 20512
219, 110
CCRC 20513
218, 110
CCRC 21538
218, 110
C. parapsilosis
CCRC 20515
229
CCRC 21253
229
CCRC 21544
229
C. guilliermondii
CCRC 21500
248
CCRC 21599
248
C. glabrata
CCRC 20586
482
2332
483
C3-3
483
aStrains without a CCRC designation were clinical isolates.
on May 15, 2020 by guest
http://jcm.asm.org/
Calif.). The running gel had an acrylamide concentration of 9% and was 0.75 mm in thickness. The time required for running electrophoresis was 3 h. After electrophoresis, the gels were stained with ethidium bromide (0.5g/ml) and viewed with an IS-1000 digital imaging system (Alpha Innotech Corporation, San Leandro, Calif.). In addition to the 50-bp DNA ladder, equal amounts (20l) of the PCR products amplified fromC. glabrataCCRC 20586 (482 bp),C. guillier-mondiiCCRC 21500 (248 bp),C. parapsilosisCCRC 20515 (229 bp),C. albicans CCRC 20512 (219 and 110 bp),C. tropicalisCCRC 20520 (218 bp),C. neofor-mansCCRC 20528 (201 bp), andC. kruseiCCRC 20514 (182 bp) were mixed to serve as markers for species identification. The species markers were run in parallel with the PCR products amplified from unknown samples to facilitate side-by-side comparisons between the markers and the PCR products amplified from the blood samples.
Definition of test sensitivity and specificity.For identification of the seven yeast species (C. albicans,C. tropicalis,C. parapsilosis,C. glabrata,C. krusei, C. guilliermondii, andC. neoformans) in blood cultures, the sensitivity of the multiplex PCR was defined as the number of strains of these species correctly identified (true positives) divided by the total number of yeast strains isolated. The test specificity was defined as the number of strains which did not belong to the above seven species and were not identified as any one of the seven major species (true negatives) divided by the total number of strains not included in these seven species (14).
RESULTS
Fragment analysis of PCR products.
Through sequence
analysis, the precise lengths of the PCR products amplified by
the fungus-specific, universal primers ITS1 and ITS2 were
de-termined:
C. krusei
(182 bp),
C. neoformans
(201 bp),
C.
tropi-calis
(218 bp),
C. albicans
(218 or 219 bp),
C. parapsilosis
(229
bp),
C. guilliermondii
(248 bp), and
C. glabrata
(482 or 483 bp)
(Table 1). Different strains of the same species produced PCR
products having the same length or differing in length by only
1 bp, and the PCR products of different species could be
separated more easily by disk PAGE than by agarose gel
elec-trophoresis. This was especially true for separating
C.
parapsi-losis
(229 bp) from
C. tropicalis
(218 bp). Another problem was
that amplicons of the ITS1 regions of
C. albicans
(218 or 219
bp) and
C. tropicalis
(218 bp) had the same mobility on
poly-acrylamide gels (Fig. 1, lanes 4 and 6). In order to discriminate
between these two species, primers CA3 and CA4, which are
specific for
C. albicans
(12), were included in the PCR mixture,
and an additional product was obtained for the organism (Fig.
1, lane 4). With the multiplex approach,
C. albicans
produced
two amplicons (218 or 219 and 110 bp) (Fig. 1, lane 4), whereas
each of the remaining six species produced only one.
Species designation was possible by comparing the
electro-phoretic mobilities of the amplicons with the commercial 50-bp
DNA ladder (Fig. 1, lane 1). Species identification was
facili-tated by running PCR products in parallel with the species
markers containing amplicons of the seven individual species
(Fig. 1, lane 5), enabling side-by-side comparisons of an
un-known with the species markers.
Limit of detection of the PCR.
The limit of detection of the
multiplex PCR for
C. albicans
CCRC 20512 artificially
inocu-lated in whole blood was approximately 20 CFU/ml (data not
shown). With serially diluted DNA in water, the limit of
de-tection of the PCR was 4 pg of
C. albicans
DNA per assay. The
limit of detection of yeast DNA was very close to that (10 pg
DNA) reported by Jaeger et al. (13) and was approximately
equal to 100 cells (37 fg of DNA per cell of
C. albicans
).
Identification of yeasts in positive blood cultures.
A total of
249 positive blood cultures containing yeasts were analyzed by
the multiplex PCR for species identification. From these blood
cultures, 255 strains of yeasts were isolated. The most
fre-quently isolated species was
C. albicans
(128 strains, 50.4%),
followed by
C. tropicalis
(51 strains, 19.7%),
C. glabrata
(28
strains, 11%),
C. parapsilosis
(23 strains, 9.1%),
C. neoformans
(9 strains, 3.5%),
C. krusei
(5 strains, 2%),
C. guilliermondii
(3
strains, 1.2%), and other species (8 strains, 3.1%) (Table 2).
All strains of the above species, except for the eight minor
species, were correctly identified, resulting in a test sensitivity
of 100% for each of the above seven species (Table 2).
How-ever, the test sensitivity for the PCR assay was 96.9%, based on
the total number (247 strains) of yeasts identified divided by
the total number (255 strains) of yeasts isolated.
Among the 249 positive blood cultures, 16 were mixed
cul-tures. Ten of these mixed cultures were from polymicrobial
infections, with one strain of yeast and one strain of bacterium
being isolated from each of the 10 blood samples. Coexisting
bacteria in blood specimens did not produce any detectable
PCR products and did not interfere with yeast identification
(Fig. 2, lanes 6 and 7). The remaining six mixed cultures were
polyfungal, with each containing two yeast strains, which could
FIG. 1. Multiplex PCR using primers ITS1, ITS2, CA3, and CA4.
Lane 1, 50-bp DNA ladder. Lanes 2 to 4,
C
.
krusei
CCRC 20514,
C. neoformans
CCRC 20528, and
C
.
albicans
CCRC 20512,
respec-tively. Lane 5, species markers formulated from amplicons of the seven
major yeast species; the bands from top to bottom were PCR products
of
C
.
glabrata
,
C
.
guilliermondii
,
C
.
parapsilosis
,
C
.
tropicalis
and
C.
albicans
,
C. neoformans
,
C
.
krusei
, and
C
.
albicans
, respectively. Lanes
6 to 9,
C
.
tropicalis
CCRC 20520,
C
.
parapsilosis
CCRC 20515,
C
.
[image:3.587.48.282.70.240.2]guilliermondii
CCRC 21500, and
C
.
glabrata
CCRC 20586, respectively.
TABLE 2. Results of multiplex PCR for the identification of
the seven major yeast species that cause fungemia
Organism No. of strains %
Tested Identified Misidentified Sensitivity Specificity
C. albicans
128
128
0
100
C. tropicalis
51
51
0
100
C. glabrata
28
28
0
100
C. parapsilosis
23
23
0
100
C. neoformans
9
9
0
100
C. krusei
5
5
0
100
C. guilliermondii
3
3
0
100
Other species
8
0
1
a87.5
aR. rubrawas misidentified asC. parapsilosis.
on May 15, 2020 by guest
http://jcm.asm.org/
be simultaneously identified by the multiplex PCR. Three
ex-amples are shown in Fig. 2; lane 2 depicts PCR products from
a mixed culture of
C. albicans
and
C. glabrata
, lane 3 contains
a mixed culture of
C. albicans
and
C. parapsilosis
, and lane 4
contains a mixed culture of
C. tropicalis
and
C. glabrata
. All
isolates from these mixed cultures were confirmed by
conven-tional isolation and identification methods.
Specificity of the multiplex PCR.
The eight miscellaneous
strains included three strains of
Candida
spp. and one strain of
each of the following species:
C. famata
,
C. lusitaniae
,
C.
pel-liculosa
,
R. rubra
, and
T. beigelii
. As shown in Fig. 3, the
elec-trophoretic mobilities of amplicons of
C. pelliculosa
(262 bp,
lane 2),
C. famata
(236 bp, lane 3),
T. beigelii
(196 bp, lane 6),
C. lusitaniae
(147 bp, lane 8), and one undetermined
Candida
species (lane 9) were different from those of the seven species
markers; hence, the five species were not identified. However,
the PCR products amplified from
R. rubra
(232 bp; Fig. 3, lane
5) and
C. parapsilosis
(229 bp, lane 4) were only 3 bp apart;
therefore,
R. rubra
was misidentified as
C. parapsilosis
,
result-ing in a test specificity of 87.5% (seven of eight strains). The
relatively low specificity was due to the limited proportion
(3.1%; 8 of 255 strains) of minor yeast species recovered from
positive blood cultures.
The sample of whole blood (Fig. 2, lane 8) was negative, as
were seven randomly selected positive blood cultures
contain-ing the followcontain-ing bacteria:
E. coli
,
S. aureus
,
K. pneumoniae
,
Pseudomonas aeruginosa
,
Serratia marcescens
,
E. cloacae
, and
S. pneumoniae
(data not shown). Furthermore, no PCR
prod-ucts were obtained by using template DNA extracted from
pure cultures of
E
.
coli
03190 and ATCC 25922,
S
.
aureus
0400,
K
.
pneumoniae
03583,
E. cloacae
00109, and
S. pneumoniae
0424 (data not shown).
DISCUSSION
This report describes the use of multiplex PCR to identify
the most frequently encountered yeasts in blood cultures. The
method used universal fungal primers ITS1 and ITS2 to
am-plify a conserved portion of the 18S rDNA region, the adjacent
ITS1 region, and a small portion of the 5.8S rDNA region,
yielding products with variable sizes among the major species
causing fungemia. Another primer pair (CA3 and CA4) was
used to amplify a specific DNA fragment of the ITS2 region of
C. albicans
. With disk PAGE, the PCR products could be
effectively separated and recognized, even though they differed
by a few base pairs. From the time at which a blood culture
become positive, the multiplex method reduced the
identifica-tion time for yeasts from approximately 1 to 3 days by routine
identification methods to about 8 h. Another advantage of the
method was that multiple yeast species coexisting in a blood
culture could be detected at the same time (Fig. 2, lanes 2 to 4).
It is generally perceived that DNA extraction from yeasts
either by lysis of enzymes (9, 21, 36) or by bead sonication (34)
followed by phenol-chloroform extraction is the most tedious
and cumbersome step of a PCR-based identification method
and limits its use in a routine clinical laboratory. We found that
a commercial extraction kit (microLYSIS) was an effective and
simple method for extracting DNA from pure yeast cultures
within 30 min. The only step used for DNA extraction with this
kit was heating of yeast cell suspensions in the lysis solution in
a thermal cycler, eliminating the use of phenol-chloroform and
alcohol for DNA purification and precipitation, respectively.
However, for extraction of yeast DNA from blood cultures, we
found that a prior step of lysing blood cells with proteinase K
followed by Lyticase digestion of the yeast cell walls was
nec-essary to obtain good results.
The efficacy of the multiplex method relies on several
fac-tors. First, the concentration of yeast cells in positive blood
cultures normally exceeds 10
5CFU/ml (2). Second, fungal
rDNA has a high copy number (40 to 80 copies per haploid
genome) (40). Third, fungemia is usually caused by a limited
number of fungal species. The most commonly encountered
yeast species (
C. albicans
,
C. tropicalis
,
C. glabrata
,
C.
parapsi-FIG. 3. Identification of minor yeast species present in positive
blood cultures by the multiplex PCR. Lane 1, 50-bp DNA ladder. Lane
2,
C
.
pelliculosa
. Lane 3,
C
.
famata
. Lane 4, species markers. Lane 5,
R. rubra
. Lane 6,
T. beigelii
. Lane 7, species markers. Lane 8,
C
.
lus-itaniae
. Lane 9,
Candida
sp.
R. rubra
(lane 5) was misidentified as
C
.
parapsilosis
.
FIG. 2. Identification of yeasts present in mixed cultures by the
multiplex PCR. Lane 1, 50-bp DNA ladder. Lane 2,
C
.
albicans
and
C. glabrata
. Lane 3,
C
.
albicans
and
C
.
parapsilosis
. Lane 4,
C
.
tropicalis
and
C
.
glabrata
. Lane 5, species markers. Lane 6,
C
.
albicans
and
E. coli
. Lane 7,
C
.
tropicalis
and
E. cloacae
. Lane 8, sample of human
blood. Lane 9, negative control.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:4.587.46.283.71.240.2]losis
,
C. krusei
, and
C. neoformans
) may represent
ⱖ
95% of the
total yeasts recovered from blood cultures (19, 23, 26).
Finally, Turenne et al. determined that universal fungal
primers ITS3 and ITS4 and an automated system of
fluores-cent capillary electrophoresis could be used to determine the
sizes of amplicons of the ITS2 genetic regions of some fungi
(34). However, even with this sophisticated technique, it was
still difficult to differentiate the PCR products of
C. albicans
(279 bp) and
C. krusei
(282 bp) by chromatographic retention
times. Adapting this approach to the multiplex PCR method
developed in this study, however, produced a method with a
high sensitivity (96.9%). The relatively low specificity (87.5%)
was due to a limited proportion (3.1%; 8 of 255 strains) of the
minor yeast species recovered from our blood cultures.
Start-ing from a positive blood culture, this method can be
com-pleted within 8 h and is simpler than any previously reported
molecular method for the identification of blood yeasts.
ACKNOWLEDGMENTS
This work was supported by grant NSC 89-2314-B-006-101 from the
National Science Council, Taipei, Taiwan, Republic of China.
We thank the medical technicians at the Department of Pathology,
National Cheng Kung University Medical Center, for help in
identi-fying all the clinical blood isolates.
REFERENCES
1.Beck-Sague, C., and W. R. Jarvis.1993. Secular trends in the epidemiology of nosocomial fungal infections in the United States, 1980–1990. National Nosocomial Infections Surveillance System. J. Infect. Dis.167:1247–1251. 2.Chang, H. C., J. J. Chang, A. H. Huang, and T. C. Chang.2000. Evaluation
of a capacitance method for direct antifungal susceptibility testing of yeasts in positive blood cultures. J. Clin. Microbiol.38:971–976.
3.Chen, Y. C., S. C. Chang, C. C. Sun, L. S. Yang, W. C. Hseih, and K. T. Luh. 1997. Secular trends in the epidemiology of nosocomial fungal infections at a teaching hospital in Taiwan, 1981 to 1993. Infect. Control Hosp. Epide-miol.18:369–375.
4.Cooper, T. G.1977. The tools of biochemistry, p. 228–231. John Wiley & Sons, Inc., New York, N.Y.
5.de Repentigny, L., L. D. Marr, J. W. Keller, A. W. Carter, R. J. Kuykendall, L. Kaufman, and E. Reiss.1985. Comparison of enzyme immunoassay and gas-liquid chromatography for the rapid diagnosis of invasive candidiasis in cancer patients. J. Clin. Microbiol.21:972–979.
6.Einsele, H., H. Hebart, G. Roller, J. Lo¨ffler, I. Rothenho¨fer, C. A. Mu¨ller, R. A. Bowden, J.-A. van Burik, D. Engelhard, L. Kanz, and U. Schumacher. 1997. Detection and identification of fungal pathogens in blood by using molecular probes. J. Clin. Microbiol.35:1353–1360.
7.Elie, C. M., T. J. Lott, E. Reiss, and C. J. Morrison.1998. Rapid identifi-cation ofCandidaspecies with species-specific DNA probes. J. Clin. Micro-biol.36:3260–3265.
8.Espinel-Ingroff, A., C. W. Kish, Jr., T. M. Kerkering, R. A. Fromtling, K. Bartizal, J. N. Galgiani, K. Villareal, M. A. Pfaller, T. Gerarden, M. G. Rinaldi, and A. Fothergill.1992. Collaborative comparison of broth mac-rodilution and micmac-rodilution antifungal susceptibility tests. J. Clin. Micro-biol.30:3138–3145.
9.Fujita, S.-I., B. A. Lasker, T. J. Lott, E. Reiss, and C. J. Morrison.1995. Microtitration plate enzyme immunoassay to detect PCR-amplified DNA fromCandidaspecies in blood. J. Clin. Microbiol.33:962–967.
10.Hee Shin, J., F. S. Nolte, and C. J. Morrison.1997. Rapid identification of Candidaspecies in blood cultures by a clinically useful PCR method. J. Clin. Microbiol.35:1454–1459.
11.Henry, T., P. C. Iwen, and S. H. Hinrichs.2000. Identification ofAspergillus species using internal transcribed spacer regions 1 and 2. J. Clin. Microbiol. 38:1510–1515.
12.Huang, C. H.1996. Specific identification of yeasts on the bases of PCR-amplified ribosomal DNA immobilized by covalent bond on the piezoelectric quartz crystal. Ph.D. thesis. National Taiwan University, Taipei, Taiwan. 13.Jaeger, E. E. M., N. M. Carroll, S. Choudhury, A. A. S. Dunlop, H. M. A.
Towler, M. M. Matheson, P. Adamson, N. Okhravi, and S. Lightman.2000. Rapid detection and identification ofCandida,Aspergillus, andFusarium species in ocular samples using nested PCR. J. Clin. Microbiol.38:2902– 2908.
14.McClure, F. D.1990. Design and analysis of quantitative collaborative stud-ies: minimum collaborative program. J. Assoc. Off. Anal. Chem.73:953–960. 15.Miyakawa, Y., T. Mabuchi, and Y. Fukazawa.1993. New method for
detec-tion ofCandida albicans in human blood by polymerase chain reaction. J. Clin. Microbiol.31:3344–3347.
16.Morace, G., L. Pagano, M. Sanguinetti, B. Posteraro, L. Mele, F. Equitani, G. D’Amore, G. Leone, and G. Fadda.1999. PCR-restriction enzyme analysis for detection ofCandidaDNA in blood from febrile patients with hemato-logical malignancies. J. Clin. Microbiol.37:1871–1875.
17.Nagai, H., Y. Yamakami, A. Hashimoto, I. Tokimatsu, and M. Nasu.1999. PCR detection of DAN specific forTrichosporonspecies in serum of patients with disseminated trichosporonosis. J. Clin. Microbiol.37:694–699. 18.Newman, S. L., T. P. Flanigan, A. Fisher, M. G. Rinaldi, M. Stein, and K.
Vigilante.1994. Clinically significant mucosal candidiasis resistant to flucon-azole treatment in patiens with AIDS. Clin. Infect. Dis.19:684–686. 19.Nguyen, M. H., J. E. Peacock, Jr., A. J. Morris, D. C. Tanner, M. L. Nguyen,
D. R. Snydman, M. M. Wagener, M. G. Rinaldi, and V. L. Yu.1996. The changing face of candidemia: emergence of non-Candida albicansspecies and antifungal resistance. Am. J. Med.100:617–623.
20.Niesters, H. G. M., W. H. F. Goessens, J. F. M. G. Meis, and W. G. V. Quint. 1993. Rapid, polymerase chain reaction-based identification assays for Can-didaspecies. J. Clin. Microbiol.31:904–910.
21.Park, S., M. Wong, S. A. E. Marras, E. W. Cross, T. E. Kiehn, V. Chaturvedi, S. Tyagi, and D. S. Perlin.2000. Rapid identification ofCandida dubliniensis using a species-specific molecular beacon. J. Clin. Microbiol.38:2829–2836. 22.Pfaller, M. A., R. N. Jones, S. A. Messer, M. B. Edmond, and R. P. Wenzel. 1998. National surveillance of nosocomial blood stream infection due to species ofCandidaother thanCandida albicans: frequency of occurrence and antifungal susceptibility in the SCOPE Program. Diagn. Microbiol. Infect. Dis.30:121–129.
23.Pfaller, M. A., S. A. Messer, R. J. Hollis, R. N. Jones, G. V. Doern, M. E. Brandt, and R. A. Hajjeh.1999. Trends in species distribution and suscep-tibility to fluconazole among blood stream isolates ofCandidaspecies in the United States. Mycology33:217–222.
24.Posteraro, B., M. Sanguinetti, L. Masucci, L. Romano, G. Morace, and G. Fadda.2000. Reverse cross blot hybridization assay for rapid detection of PCR-amplified DNA fromCandidaspecies,Cryptococcus neoformans, and Saccharomyces cerevisiae in clinical samples. J. Clin. Microbiol.38:1609– 1614.
25.Price, M. F., M. T. LaRocco, and L. O. Gentry.1994. Fluconazole suscepti-bilities ofCandidaspecies and distribution of species recovered from blood cultures over a 5-year period. Antimicrob. Agents Chemother.38:1422–1424. 26.Rex, J. H., J. E. Bennett, A. M. Sugar, P. G. C. Pappas, M. van der Horst, J. E. Edwards, R. G. Washburn, W. M. Scheld, A. W. Karchmer, A. P. Dine, M. J. Levenstein, and C. D. Webb.1994. A randomized trial comparing fluconazole with amphotericin B for the treatment of candidemia in patients without neutropenia. N. Engl. J. Med.331:1325–1330.
27.Rex, J. H., M. A. Pfaller, A. L. Barry, P. W. Nelson, and C. D. Webb.1995. Antifungal susceptibility testing of isolates from a randomized multicenter trial of fluconazole versus amphotericin B as treatment of non-neutropenic patients with candidemia. Antimicrob. Agents Chemother.39:40–44. 28.Rex, J. H., M. G. Rinaldi, and M. A. Pfaller.1995. Resistance ofCandida
species to fluconazole. Antimicrob. Agents Chemother.39:1–8.
29.Ruhnke, M., A. Eigler, I. Tennagen, B. Geiseler, E. Engelmann, and M. Trautmann. 1994. Emergence of fluconazole-resistant strains ofCandida albicansin patients with recurrent oropharyngeal candidosis and human immunodeficiency virus infection. J. Clin. Microbiol.32:2092–2098. 30.Sandhu, G. S., B. C. Kline, L. Stockman, and G. D. Roberts.1995. Molecular
probes for diagnosis of fungal infections. J. Clin. Microbiol.33:2913–2919. 31.Sanguineti, A., J. K. Carmichael, and K. Campbell. 1993.
Fluconazole-resistantCandida albicansafter long-term suppressive therapy. Arch. Intern. Med.153:1122–1124.
32.Simor, A. E., G. Goswell, L. Louie, M. Lee, and M. Louie.1997. Antifungal susceptibility testing of yeast isolates from blood cultures by microbroth dilution and the E Test. Eur. J. Clin. Microbiol. Infect. Dis.16:693–697. 33.Skladny, H., D. Buchheidt, C. Baust, F. Krieg-Schneider, W. Seifarth,
C. Leib-Mo¨sch, and R. Hehlmann.1999. Specific detection ofAspergillus species in blood and bronchoalveolar lavage samples of immunocompro-mised patients by two-step PCR. J. Clin. Microbiol.37:3865–3871. 34.Turenne, C. Y., S. E. Sanche, D. J. Hoban, J. A. Karlowsky, and A. M.
Kabani.1999. Rapid identification of fungi by using the ITS2 genetic region and an automated fluorescent capillary electrophoresis system. J. Clin. Mi-crobiol.37:1846–1851.
35.Van Burik, J.-A., D. Myerson, R. W. Schreckhise, and R. A. Bowden.1998. Panfungal PCR assay for detection of fungal infection in human blood specimens. J. Clin. Microbiol.36:1169–1175.
36.Wahyuningsih, R., H.-J. Freisleben, H.-G. Sonntag, and P. Schnitzler.2000. Simple and rapid detection ofCandida albicansDNA in serum by PCR for diagnosis of invasive candidiasis. J. Clin. Microbiol.38:3016–3021. 37.Walsh, T. J., W. Hathorn, J. D. Sobel, W. G. Merz, V. Sanchez. S. M. Maret,
H. R. Muckley, M. A. Pfaller, R. Schanfele, C. Silvia, E. Navarron, J. Lecciones, P. Chandrasekar, J. Lee, and P. A. Pizzu.1991. Detection of circulatingCandidaenolase by immunoassay in patients with cancer and invasive candidiasis. N. Engl. J. Med.324:1026–1031.
38.Warren, N. G., and K. C. Hazen.1999.Candida,Cryptococcus, and other
on May 15, 2020 by guest
http://jcm.asm.org/
yeasts of medical importance, p. 1184–1199.InP. R. Murray, E. J. Baron, M. A. Pfaller, F. C. Tenover, and R. H. Yolken (ed.), Manual of clinical microbiology, 7th ed. American Society for Microbiology, Washington, D.C. 39.Weinstein, M. P., M. L. Towns, S. M. Quartey, S. Mirrett, L. G. Reimer, G.
Parmigiani, and L. B. Reller.1997. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of microbiol-ogy, epidemiolmicrobiol-ogy, and outcome of bacteremia and fungemia in adults. Clin. Infect. Dis.24:584–602.
40.White, T. J., T. Bruns, S. Lee, and J. Taylor.1990. Amplification and direct
sequencing of fungal ribosomal RNA genes for phylogenetics, p. 315–322.In M. A. Innis, D. H. Gefland, J. J. Sninsky, and T. J. White (ed.), PCR protocols: a guide to methods and applications. Academic Press, Inc., San Diego, Calif. 41.Williams, D. W., M. J. Wilson, M. A. O. Lewis, and A. J. C. Potts.1995.
Identification ofCandidaspecies by PCR and restriction fragment length polymorphism analysis of intergenic spacer regions of ribosomal DNA. J. Clin. Microbiol.33:2476–2479.
42.Young, R., and J. Bennett.1971. Invasive aspergillosis. Absence of detectable antibody response. Am. Rev. Respir. Dis.104:710–716.