continued confusion over management of GBS in pregnancy. ACOG
Newsletter. 1994;38:1,10
8. Siegel JD, McCracken GH Jr, Threlkeld N, Milvenan B, Rosenfeld CR. Single dose penicillin prophylaxis against neonatal group B streptococ-cal infections: a controlled trial in 18,738 newborn infants. N Engl J Med. 1980;303:769 –775
9. Siegel JD, McCracken GH Jr, Threlkeld N, DePasse BM, Rosenfeld CR. Single-dose penicillin prophylaxis of neonatal group B streptococcal disease. Lancet. 1982;i:1426 –1430
10. Pyati SP, Pildes RS, Jacobs NM, et al. Penicillin in infants weighing two kilograms or less with early-onset group B streptococcal disease. N Engl
J Med. 1983;308:1383–1389
11. Boyer KM, Gotoff SP. Prevention of early-onset neonatal group B strep-tococcal disease with selective intrapartum chemoprophylaxis. N Engl
J Med. 1986;314:1665–1669
12. Boyer KM, Gadzala CA, Burd LI, Fisher DE, Paton JB, Gotoff SP. Selective intrapartum chemoprophylaxis of neonatal group B strepto-coccal early-onset disease: I. Epidemiologic rationale. J Infect Dis. 1983; 148:795– 801
13. Allardice JG, Baskett TF, Seshia MMK, Bowman N, Malazdrewicz R. Perinatal group B streptococcal colonization and infection. Am J Obstet
Gynecol. 1982;142:617– 620
14. Morales WJ, Lim DV, Walsh AF. Prevention of neonatal group B strep-tococcal sepsis by the use of a rapid screening test and selective intra-partum chemoprophylaxis. Am J Obstet Gynecol. 1986;155:979 –983 15. Morales WJ, Lim D. Reduction of group B streptococcal maternal and
neonatal infections in preterm pregnancies with premature rupture of membranes through a rapid identification test. Am J Obstet Gynecol. 1987;157:13–16
16. Tuppurainen N, Hallman M. Prevention of neonatal group B strepto-coccal disease: intrapartum detection and chemoprophylaxis of heavily colonized parturients. Obstet Gynecol. 1989;73:583–587
17. Matorras R, Garcia-Perea A, Omenaca F, Diez-Enciso M, Madero R, Usandizaga JA. Intrapartum chemoprophylaxis of early onset group B streptococcal disease. Eur J Obstet Gynecol Reprod Biol. 1991;40:57– 62 18. American Academy of Pediatrics, Committee on Infectious Diseases.
Guidelines for prevention of group B streptococcal infection by chemo-prophylaxis. Pediatrics. 1992;90:775–778
19. Garland SM, Fliegner JR. Group B streptococcus and neonatal infections: the case for intrapartum chemoprophylaxis. Aust N Z J Obstet
Gynaecol. 1991;31:119 –122
20. Allen UD, Nevas L, King SM. Effectiveness of intrapartum penicillin prophylaxis in preventing early-onset group B streptococcal infection: results of a meta-analysis. Can Med Assoc J. 1993;149:1659 –1665 21. Society of Obstetricians and Gynaecologists of Canada and Canadian
Pediatric Society. National consensus statement on the prevention of early-onset group B streptococcal infections in the newborn. J Soc Obstet
Gynaecol Can. 1994;16:2271–2278
22. Pylipow M, Gaddis M, Kinney JS. Selective intrapartum prophylaxis for group B streptococcus colonization: management and outcome of new-borns. Pediatrics. 1994;93:631– 635
23. Schuchat A, Deaver-Robinson K, Plikaytis BD, Zangwill K, Mohle-Boetani J, Wenger JD. Multistate case-control study of maternal risk factors for neonatal group B streptococcal disease. Pediatr Infect Dis J. 1994;13:623– 629
24. Rouse DJ, Goldenberg RL, Cliver SP, Cutter GR, Mennemeyer ST, Fargason CA. Strategies for the prevention of early-onset neonatal group B streptococcal sepsis: a decision analysis. Obstet Gynecol. 1994; 83:483– 494
25. Gibbs RS, McDuffie RS, McNabb F, Fryer GE, Miyoshi T, Merenstein G. Neonatal group B streptococcal sepsis during 2 years of a universal screening program. Obstet Gynecol. 1994;84:496 –500
26. Ohlsson A, Myhr TL. Intrapartum chemoprophylaxis of perinatal group B streptococcal infections: a critical review of randomized controlled trials. Am J Obstet Gynecol. 1994;170:910 –917
27. Gibbs RS, McGregor JA, Mead PB, Eschenbach DA, Hager WD, Sweet RL. A survey of practices in infectious diseases by obstetrician-gynecologists. Obstet Gynecol. 1994;83:631– 636
28. Jafari HS, Schuchat A, Hilsdon R, Whitney C, Toomey K, Wenger J. Barriers to prevention of perinatal group B streptococcal disease. Pediatr
Infect Dis J. 1995;14:662– 667
29. Yancey MK, Armer T, Clark P, Duff P. Assessment of rapid identifica-tion tests for genital carriage of group B streptococci. Obstet Gynecol. 1992;80:1038 –1047
30. Boyer KM, Gadzala CA, Kelly PH, Burd LI, Gotoff SP. Selective intra-partum chemoprophylaxis of neonatal group B streptococcal early-onset disease: II. Predictive value of prenatal cultures. J Infect Dis. 1983;148:802– 809
31. Yancy MK, Duff P, Kubilis P, Clark P, Frentzen BH. Risk factors for neonatal sepsis. Obstet Gynecol. 1996;87:188 –194
32. Boyer KM, Gadzala CA, Kelly PD, Gotoff SP. Selective intrapartum chemoprophylaxis of neonatal group B streptococcal early-onset disease: III. Interruption of mother-to-infant transmission. J Infect Dis. 1983;148:810 – 816
33. Schuchat A, Whitney C, Zangwill K. Prevention of perinatal group B streptococcal disease: a public health perspective. MMWR. 1996;45:1–24 34. Siegel JD, Cushion NB. Prevention of early-onset group B streptococcal disease: another look at single-dose penicillin at birth. Obstet Gynecol. 1996;87:692– 698
35. Gotoff SP. Chemoprophylaxis of early onset group B streptococcal disease. Pediatr Infect Dis J. 1984;3:401– 403
36. Ghaey K, Tolpin M, Schauf V, et al. Penicillin prophylaxis and the neonatal microbial flora. J Infect Dis. 1985;152:1070 –1073
37. Amstey MS, Gibbs RS. Is penicillin G a better choice than ampicillin for prophylaxis of neonatal group B streptococcal infections? Obstet
Gy-necol. 1994;84:1058 –1059
38. Mohle-Boetani J, Schuchat A, Plikaytis BD, Smith D, Broome CV. Com-parison of prevention strategies for neonatal group B streptococcal infection: a population-based economic analysis. J Am Med Assoc. 1993; 270:1442–1448
39. Yancey MK, Duff P. An analysis of the cost-effectiveness of selected protocols for the prevention of neonatal group B streptococcal infection.
Obstet Gynecol. 1994;83:367–371
The Outcomes of Very Low Birth
Weight Infants: Are We Asking the
Right Questions?
ABBREVIATIONS. VLBW, very low birth weight; IQ, intelligence quotient; CP, cerebral palsy; NICU, neonatal intensive care unit.
Decreases in infant mortality rates in the United States reflect the success of sustaining the lives of increasingly more immature infants. This success generates abiding concern about the outcomes of these infants, and that concern has led to a large number of publications on the outcomes of very low birth weight ([VLBW],1500 g) infants. The extent to which this experience provides results useful for clinical and policy decisions is less clear. Three major concerns are identified. The first is that the research question underlying many studies is framed impre-cisely, and may be addressed with inappropriate study design and outcomes. Moreover, the underly-ing causal pathway is rarely specified. Second, the current focus of most studies is on a relatively nar-row range of neurodevelopmental and cognitive out-comes and fails to capture significant nonneurologic morbidity. Moreover, the ways in which even the neurodevelopmental outcomes are reported provide little guidance to clinicians or policymakers about the functional impact on the individual child or the need for additional services. Finally, the failure to incorporate more complete pathogenetic or concep-tual models of the other factors influencing outcomes
Received for publication Jul 9, 1996; accepted Oct 17, 1996.
also results in missed opportunities to identify po-tential ameliorative strategies and may lead to flawed clinical and policy decisions. A major reshap-ing of the approach to assessreshap-ing the outcomes of VLBW survivors is needed.
The importance of the high prevalence of VLBW among US infants to the relatively high infant mor-tality rates in this country,1and the disproportionate
risk of such infants for childhood morbidity has been well-documented.1,2 Despite repeated clinical and
programmatic interventions, the rate of VLBW births has remained stable for white infants and has re-cently increased for African-American infants.3,4
Thus, the continued decline in infant mortality re-flects the power of modern neonatal care to sustain the lives of very tiny infants. In view of the risk for morbidity conferred by lower birth weight, ongoing assessment of the outcomes of these tiny infants re-mains important.
CURRENT STATUS
This importance is reflected in a steady stream of outcomes studies which have been summarized in meta-analyses5,6 and several less quantitative
re-views.7–16Most reports focus on neurodevelopmental
outcomes with relatively similar definitions of severe impairment (some combination of severe develop-mental delay, or a developdevelop-mental or intelligence quotient (IQ) ,70, and severe cerebral palsy [CP]). The rate of such impairment among survivors has remained low and stable. The point estimate of the prevalence of CP in children born weighing,1500 g is 7.7% (95% confidence intervals of 5.3% to 9.0%) with little difference between those born weighing
,1000 g and those weighing 1000 to 1500 g,5and the
proportions of VLBW children found in the abnor-mal IQ range is 14% for those#1500 g (19%,#1000).6
Because CP and cognitive subnormality are not in-dependent occurrences, rates of overall severe im-pairment tend to be in the same range of 10% to 15% for those ,1500 g with increasing rates of impair-ment with decreasing birth weight.9,10 –16While fewer
studies are available, a clearer picture of the out-comes of the most recent group of survivors, those born weighing ,800 g, is emerging. Among these tiny survivors, rates of severe impairment are higher, in the range of 20% to 35% with very high rates of less severe difficulties.17–20
This latter category of less severe impairment is often very difficult to interpret, generally consisting of ad hoc combinations of neurologic findings, sen-sorineural deficits, and borderline IQ scores. The lack of comparability across studies of such broad cate-gorization of morbidity is but one methodologic flaw recurring in the follow-up literature.5–18,13,16 Others
include the failure to characterize study samples in terms of eligibility for and losses to the cohort, to provide sufficient information to assess the represen-tativeness of the group, and to consider the use of appropriate controls, among other issues. These flaws not only severely constrain the use of rigorous, quantitative summary techniques such meta-analysis and limit any estimate of potential changes over time, they also cast into question the utility of many
of these studies to provide information at the indi-vidual patient or policy level.
What has received much less critical attention is the underlying conceptualization of the problem. This review argues that the described purpose of most published studies is too broad and vague, and addressed with inappropriate study designs. In ad-dition, the outcomes being assessed may be too lim-ited, and not provide information useful for guiding the care for individuals or planning for their services. Finally, even for the outcomes selected, most studies fail to incorporate a specific underlying pathogenetic or conceptual model to identify potential factors in-fluencing the relationship between the initial state (ie, prematurity or low birth weight) and the out-comes observed.
RATIONALE FOR THE STUDY
A clear statement of the purpose of the study or the research question being addressed is a funda-mental element of any investigation to assure appro-priate study design, data collection, and analysis. However, the purpose of many outcome studies is framed so imprecisely that the utility of the study is unclear.
For example, two often cited rationales are to con-tribute to some assessment of the effect of modern neonatal intensive care, or to examine the effect of extreme prematurity or VLBW on development in a natural history of disease approach. The usual study design of a case series or cohort from a single insti-tution is weak for assessing any medical interven-tions,21–23and the now well-documented variation in
complication rates and outcomes among neonatal intensive care units24 –27 (NICUs) raises major
con-cerns about the representativeness of the study pop-ulations for either purpose. The outcomes assessed constitute a rather standard battery of neurologic examination and developmental tests not conceptu-ally well-linked to the independent variable, ie, the mechanisms by which exposure to NICU care or the maturational processes occurring at different stages in premature infants influence specific outcomes are not specified. Almost never explicitly considered is that the study samples are quite heterogeneous for other prenatal and postnatal factors that are well-known to affect child health and development.
Moreover, to be useful even in this limited way, the outcomes of these infants must be described or con-ceptualized in a way relevant to the clinical manage-ment, eg, characterization of children as having a suspect neurologic examination,28 may not provide
information as to indicated therapy or prognosis.
SELECTION OF THE APPROPRIATE OUTCOMES
The outcomes in most studies reflect historical in-terest among early investigators in two disciplinary groups, neurologists and developmental psycholo-gists,9,10,29and the powerful example of the National
Perinatal Collaborative Study,30 –32funded by the
Na-tional Institute of Neurologic Disease and Stroke for the expressed purpose of assessing the risk of peri-natal events for childhood neurodevelopmental mor-bidity. The relevance of the National Perinatal Col-laborative Study model to modern follow-up, however, is questionable. First, neonatal care dif-fered dramatically23 in that era with only a limited
number of VLBW survivors. Second, resources were available to train and supervise assessors carefully, assuring high interrater reliability. Finally, the nature of the study question led to a focus on neurologic findings, including a variety of abnormalities of tone, abnormal sensorineural findings, and cognitive def-icits, not necessarily other types of morbidity or func-tional sequelae.
The reliance on this approach also incurs disad-vantages in terms of policy. Recurrent reporting of certain neurodevelopmental outcomes characterized as severe or moderate handicap has two adverse sequelae. It creates a perception that severe neurode-velopmental disability is an invariant consequence for a high proportion of very premature survivors, and that increased survival of such infants leads to intolerable burdens on the family and contributes substantially to an increase in severe disability in the population. This perception, in turn, influences both individual parental decisions in the context of im-pending preterm delivery and the public debate about access to and financing of neonatal intensive care services. Thus, some serious scholars33interpret
this literature as support for setting birth weight or gestational age limits below which resuscitation or intensive care should not be provided, or the provi-sion of such care considered experimental, even though such limits would save little of the cost of neonatal care34,35and might exacerbate racial
dispar-ities in infant mortality.36
This lay and professional perception is not sup-ported by the low prevalence of severe neurodevel-opmental disability among VLBW survivors, as al-ready noted. Moreover, estimates of the contribution of VLBW children to the burden of neurodevelop-mental morbidity in the population reveal that they account for about one-third of the children with CP with an estimated prevalence of CP of 1.5 to 2.5 per 1000 births.37The prevalence of mental retardation is
12.0/1000 children, and VLBW can be estimated to account for about 10% of those with mental retarda-tion.38In both instances, the majority of children with
these outcomes are of heavier birth weight or born at term, and the extent to which increased survival of
VLBW infants contributes to changes in rates of se-vere impairment is difficult to assess.8
Likewise, the perception that a certain percentage of survivors will have severe disability has limited until recently, examination of current practices for approaches to reducing morbidity. The proportion of VLBW children who develop severe intraventricular bleeding, an antecedent of CP, however, varies by fourfold across different NICUs25 and is influenced
by the sophistication of the hospital of birth,39
sug-gesting that factors other than prematurity per se may influence the rate of adverse events. Indeed, rates of such hemorrhages are lower in infants ex-posed to several specific therapeutic interven-tions,40 – 43 vary with the acuity of the infant’s
condi-tion on admission,44,45 and may decrease with
improvements in survival.46,47All this evidence
sug-gests that modifiable practices in the management of premature delivery and newborn care may influence outcomes.
The second consequence of this traditional focus on a relatively small range of potential outcomes has incurred the disadvantage of incomplete descrip-tions of the postdischarge course of these infants, particularly the functional impact of different types of morbidity and response in terms of appropriate services. Experienced investigators have begun to redefine outcomes relying on more recent, broader conceptual models13,14 that tend to define health as
multidimensional and emphasize dysfunction re-lated to health problems. Recent studies of VLBW children at school age have relied on instrumentation to operationalize the World Health Organization def-inition of health,48 to adapt the World Health
Orga-nization’s approach to characterizing disability to VLBW children,49,50and to develop quality-adjusted
life-years,51–54resulting in a broader characterization
of an array of overlapping and interactive morbidity among these children.16 The picture that emerges
more clearly from these studies is that children who were VLBW experience poorer health along a variety of dimensions including physical health problems such as asthma with associated limitations in ability to engage in usual childhood activities, and difficul-ties with specific developmental actividifficul-ties especially in visual-perception tasks and expressive language, slower physical growth, behavioral problems and poorer social-emotional development. This observed functional impairment translates into lower aca-demic achievement scores55,56and poorer school
per-formance.57,58 These newer studies are closer to the
medical and educational resources required by each of these children are quite different, and the educa-tional prognosis for the mildly affected child is likely to be less sanguine than the moderately affected one. While a positive step in better assessments of out-come, experience with the current instruments indi-cates that much more research needs to be done, both conceptually and methodologically. The limited instru-mentation currently available for assessing child health status is often derived from modifications of adult in-struments. While achieving continuity between adult and child experience, this approach conceptually fails to incorporate the notion of a developing organism for which the experience of ill health may serve to deflect the child from a developmental trajectory in ways that are difficult to assess. Further, instruments based on adult models become increasingly problematic for very young children. Methodologically, much work remains to be done on validation in specific health conditions or special populations like VLBW children, the factors influencing proxy reporters (ie, parents), the longitudi-nal trajectories of these instruments (as most studies are cross-sectional), the implications of findings on health status measures for health and social services, and the development of instrumentation for different ethnic and linguistic groups.
ATTRIBUTION OF CAUSALITY
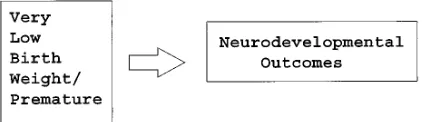
These broader definitions of outcome also raise interesting, and, as yet, barely addressed questions about causality and potential ameliorative interven-tions. The underlying causal model in most studies is relatively simple: outcome in premature/low birth weight children can be attributed to the prematurity or its complications (Fig 1). Thus, these studies tend to ignore the theoretical and empirical experience of factors influencing child health and development.
To illustrate this point, multiple regression analy-ses have been performed for five selected health outcomes and other factors among children born weighing,1000 g and assessed at age 8 to 10 years and summarized schematically in Table 1. The de-scription of the overall study and more detailed anal-yses have been previously published,48,58 – 61 and the
definitions and actual results are located in the Ap-pendices. The outcomes were selected to cover phys-ical health (limits in usual activities attributable to health and maternal rating of child health) social and emotional well-being (behavior problems, child com-petence) and cognitive development (IQ). Factors po-tentially influencing these outcomes have been se-lected to illustrate the effects of the severity of the neonatal course (length of stay), sociodemographic factors (race, maternal education, and family in-come), current child illness (asthma), maternal
phys-ical (self-rating) and mental health (General Health Questionnaire), and environmental exposures (smoking in household). Compared with normal birth weight or heavier birth weight infants, those born #1000 g had poorer health on all these mea-sures.53,65,66
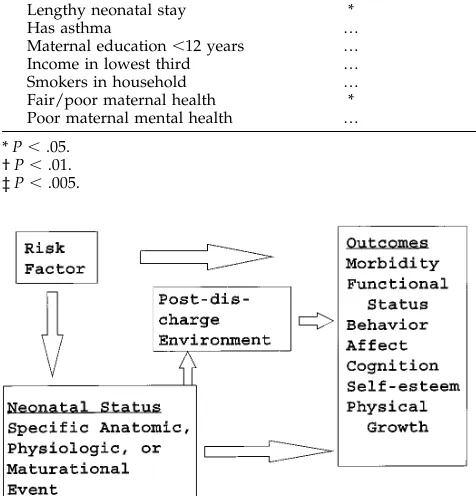
As the results of the regression analyses reveal, the factors influencing the outcomes vary. The first two outcomes that reflect physical health status are re-lated to severity of the neonatal course, the presence of child current chronic illness, and maternal health status with only modest effects of socioeconomic status as indicated by income or maternal education. In contrast, measures of social and emotional status are more heavily influenced by maternal mental health, and also parental smoking and income. The most profound effects of socioeconomic status are seen with cognitive development, although severity of the neonatal course also plays a role. These find-ings could be predicted from the literature on each of these individual outcomes, and suggest a far more complex situation than the simple paradigm of cau-sality underlying most follow-up studies (Fig 2).
More importantly, they suggest that postdischarge interventions might enhance infant outcomes regard-less of neonatal status. Indeed, recent evidence sug-gests that developmentally focused interventions during the neonatal stay and in early childhood lead to improvements in psychosocial development even among very preterm infants.62,63
CONCLUSIONS AND RECOMMENDATIONS
The intent of this review is not to disparage pre-vious efforts at characterizing the outcomes of very premature infants. In fact, more is probably known about their outcomes then for many other conditions or problems in clinical medicine. Rather, the purpose is to argue that advances in many relevant areas from the imaging of immature brains to the measures of effectiveness of complex medical services require a reconceptualization and refocusing of this activity if our knowledge is to advance.
The first element of this refocusing is a more careful specification of the question being addressed and se-lection of research designs and measures appropriate to the question. Assessment of the outcomes of specific complications of prematurity should be based on the anatomic location or pathogenesis of the insult and conducted at an appropriate age. Neurologic outcomes are important in these children, but neurodevelopmen-tal assessments should reflect the activities influenced by the areas of the brain affected by neonatal lesions and be performed when such functions can be as-sessed. Likewise, pulmonary function and physical growth are probably as important as outcomes for chil-dren with chronic lung disease as IQ, as noted in a recent trial.64In other words, the focus must move from
descriptive studies to testing more specific hypotheses about the factors causing disability.
More general assessments designed to provide guidance for management should rely on conceptu-alization of health status and health-related quality of life now emerging to avoid idiosyncratic descrip-tions. In addition, new ways of reporting findings
must be found to reflect this more complex picture. The usual approach is to report descriptive group statistics for one or more outcome measures such as average IQs or the percentages of children with a specific problem. The fact that children born very prematurely on average score lower on virtually all outcomes than those of heavier birth weight conveys the impression that all immature children do uni-formly poorly,20 an impression not consistent with
clinical experience. More informative are profiles of outcomes, preferably in terms that provide some notion of the level of dysfunction associated with specific findings or scores,13,50 an approach proven
useful in studies with adults.
Coupled with better outcomes assessment is the need for better characterization of the neonatal experi-ence to estimate the effect of variations in neonatal care practices on the emergence and severity of childhood health and developmental problems. The source of variation in neonatal complications across units is not well-understood, although a portion of it must reflect the severity of the infant’s status on admission not captured by birth weight, gestational age, and Apgar score. Neonatal admission severity scores for physio-logic status and intensity of therapeutic intervention have now been developed,65–67but have not yet been
used with longer term outcomes.
In addition to better characterization of neonatal sta-tus, better characterization of other environmental fac-tors influencing outcomes is needed based on the liter-ature on chronic illness in childhood68 (related to
asthma or reactive airway disease), social-emotional development69(related to behavior problems) and
cog-nitive development70,71 (IQ and its subscales). Such
broader conceptual frameworks would include precon-ceptional and prenatal factors influencing human growth and development including genetic defects and congenital malformations, as well as postnatal factors influencing outcomes beyond neonatal events. Also in-cluded would be postdischarge interventions such as early childhood educational programs, now docu-mented to be of benefit to the VLBW population.62
A final challenge is the problem of distilling the information into a form to facilitate decision making at the individual and population levels. At the level of individual decision-making where parents and clinicians are engaged in agreeing on appropriate levels of intervention before and after delivery, the current outcomes literature provides little sense of the impact of even the limited types of morbidity ascertained for resources needed and level of func-tional impairment. Instead, this level of interpreta-tion is left to the clinicians (both nurses and doctors) who are known to overestimate the degree of sever-ity both acutely on admission72 and long-term, and
who may fail to consider parental and child values on the quality of the child’s life.73,74 Clearly,
varia-tions occur among both parents and clinicians, as to what is acceptable, or what may be intolerable. How-ever, the decision-making process is not facilitated when the practical consequences of the decision are not well-delineated and filtered through two sets of unexamined values.
At the policy level, clearer understanding of the functional capacities and potential ameliorative in-terventions may lead to more appropriate policy rec-ommendations. Clearly, both neonatal and longer term costs are substantial and of concern particularly juxtaposed to those for normal birth weight or term children.75 Although the use of term comparison
groups in the estimation of the relative risk of mor-bidity occurring in VLBW children is a methodologic advance long-recommended,7their use for
cost-effec-tiveness arguments needs more careful examination. For example, neurodevelopmental outcomes for ex-tremely premature infants (,750 g) are comparable to or better than those of children with other acute, life-threatening events requiring intensive medical inter-vention.76–80 Despite this comparability in outcomes,
the current framing of the debate has led to the percep-tion of such extreme futility that in the recent Oregon
TABLE. Summary of Factors Influencing Outcomes Among Children,1000 grams at Birth Assessed at School Age Limitations in
Usual Activities Due to Health
Maternal Rating of Child Health
Behavior Problems
Social Competence
Cognition (IQ)
Race … * … … …
Lengthy neonatal stay * † … … *
Has asthma … † … … …
Maternal education,12 years … … … … …
Income in lowest third … … … * †
Smokers in household … … * … …
Fair/poor maternal health * * … … …
Poor maternal mental health … … ‡ * …
* P,.05. † P,.01. ‡ P,.005.
Medicaid waiver, neonatal intensive care for infants 500 to 700 g ranks substantially below treatment of human immunodeficiency virus and only slightly above liver transplant for nonalcoholic cirrhosis, in terms of priority.81 This situation may, indeed, reflect
an accurate ranking, but currently is not derived from empiric comparisons but the impressions of the clini-cians involved.
The purpose of this discussion is not to provide an apologia for neonatal intensive care to all premature infants regardless of the outcomes, but to argue for a more sophisticated and rigorous approach to the pro-cess. Otherwise, we will continue to fail to recognize opportunities to reduce the morbidity and functional impairment for these tiny infants, to come to limited and sometimes flawed decisions about their care, and potentially to advocate inappropriate policy strategies.
What is known about the outcomes of very premature infants creates a strong sense of urgency to pursue research and implement strategies that will reduce the number of such births. However, even in those coun-tries with the lowest prematurity rates, the rate has, to this point, never gone to zero. Thus, we must strive to improve the care and outcomes of current and (hope-fully fewer) future very premature infants.
Marie C. McCormick, MD, ScD
Department of Maternal and Child Health Harvard School of Public Health
Joint Program in NeonatologyHarvard Medical School Boston, MA 02115
ACKNOWLEDGMENTS
This work was supported in part by a contract from the Na-tional Institute of Child Health (NICHD) and the Maternal and
APPENDIX 1. Definitions and Statistical Results for Table 1 Summary of Child Health and Development Outcomes Measures and Covariates
Child Health and Developmental Outcome
Physical health A 14-item scale of maternal report of limits in activities of daily living by health problems scored dichotomously as present or absent, modified from a scale in the Rand Corporation National Health Insurance Study.82High scores indicate more disability.
Maternal rating of health status A 6-item scale of 5-point Likert items eliciting maternal assessment of past and current health, and susceptibility to illness.82Higher scores as associated with better health.
Behavior problems A 28-item index of maternal report of negative behaviors scored dichotomously such that higher score indicate worse behavior.83
Child social competence A 36-item scale of 4-point Likert items eliciting maternal report of child’s competence relative to other children in areas of social and academic functioning with higher scores indicating greater competence.84
Cognitive functioning Intelligence quotient (IQ) as measured by the Wechsler Intelligence Scale for Children.85
Covariates
Child race Coded as 15nonwhite, 05other
Neonatal length of stay Coded as 15 .75 percentile for birth weight (estimate of severity of neonatal course67,86),
05#75% le.
Asthma Maternal report that a doctor told her that the child had asthma.
Maternal education Maternal educational attainment in child’s infancy, coded as 15 ,12 years, 05$12 years. Income Total family income at time of interview (child 8–10 years of age) coded as 15lowest third
for sample, 05upper two-thirds.
Smoker Maternal report that at least one individual in the home smoked at time of interview. Maternal rating of her health Maternal rating of her own health on a single question with 5 possible responses from
“excellent” to “fair” or “poor” coded as 15fair/poor.87
Maternal emotional health Maternal report on the General Health Questionnaire (GHQ) as fielded in the National Institute of Mental Health Epidemiologic Area Catchment Survey with scores above 5 indicating clinically significant distress.88,89
APPENDIX 2. Multiple Regression Analyses of Factors Associated With Health and Developmental Outcomes at School Age for Children Born Weighing#1000 g
Health and Developmental Outcomes
Physical Health
Maternal Rating of Health
Behavior Problem Index
Social Competence
IQ
Intercept 14.93 20.03 9.34 113.70 101.59
Nonwhite race 20.303 1.488* 0.250 21.61 5.217
Neonatal length of stay 1.342* 22.070* 21.101 25.700 27.225*
Asthma 0.165 22.255† 2.417 1.204 3.4110
Maternal education,12 years 20.046 1.291 21.236 1.242 23.718
Income in lowest third 0.683 22.197‡ 1.738 26.848* 210.028†
Smoker in household 20.112 20.325 2.221* 22.300 0.815
Maternal health as fair/poor 2.2475* 22.750* 2.964 21.029 21.699
Maternal mental health score 0.743 21.202 3.531‡ 27.052* 0.815
F (df) 4.833§ 5.192 3.364‡ 2.309* 2.728†
(8,177) (8,178) (8,161) (8,133)
R2 0.186 0.196 0.142 0.108 0.149
Child Health Bureau (MCHB) (N01-HD-5–2928), and grants from the Robert Wood Johnson Foundation (RWJF)(9104) and the William T. Grant Foundation, (86 – 0401–92) as well as grants from the NICHD, MCHB, RWJF, and Pew Charitable Trusts in support of the Infant Health and Development Program, and HD-30956.
The author wishes to acknowledge the technical assistance of Nancy Ralph and Urmi Bhaumik, MBBS, MS.
REFERENCES
1. Preventing Low Birthweight. Washington, DC: National Academy Press; 1985
2. McCormick MC. The contributions of low birthweight to infant mortal-ity and childhood morbidmortal-ity. N Engl J Med. 1985;312:82–90
3. US Deparment of Health and Human Services. Health United States 1994. Hyattsville, MD: US Department of Health and Human Services; 1995. 95–1232. Publication No. (PHS)
4. Guyer B, Strobino DM, Ventura SJ, Singh GK. Annual summary of vital statistics-1994. Pediatrics. 1995;96:1029 –1039
5. Escobar GJ, Littenberg B, Pettiti DB. Outcome among surviving very low birth weight infants: a meta-analysis. Arch Dis Child. 1991;66: 204 –211
6. Aylward GP, Pfeiffer SI, Wright A, Verhulst SJ. Outcomes studies of low birth weight infants published in the last decade: a meta-analysis.
J Pediatr. 1989;115:515–520
7. Kitchen WH, Ryan MM, Richards A, et al. Changing outcomes over 13 years of very low birth weight infants. Sem Perinatol. 1982;4:373–389 8. McCormick MC. Has the prevalence of handicapped infants increased
with improved survival of the very low birth weight infant? Clin
Peri-natol. 1993;20:263–277
9. Scott D, Spiker D. Research on the sequelae of prematurity: early learning, early intervention and later outcomes. Sem Perinatol. 1989;13: 495–505
10. Hoy EA, Bill JM, Sykes DM. Very low birth weight: a long term developmental impairment. Int Behav Devel. 1988;11:37– 67
11. Kuban KCK, Leviton A. Cerebral palsy. N Engl J Med. 1994;330:188 –195 12. Ornstein M, Ohlsson A, Edmonds J, Asztalos E. Neonatal follow-up of very low birth weight/extremely low birth weight infants to school-age: a critical overview. Acta Paediatr Scand. 1991;80:741–748
13. McCormick MC. Long-term follow-up of infants discharged from neo-natal intensive care units. JAMA. 1989;261:1767–1772
14. Ens-Dokkum MH, Schreuder A, Veen S, Verloove-Vanhorick SP, Brand R, Ruys JH. Evaluation of the care for the pre-term infant: review of the literature on follow-up on preterm and low birth weight infants.
Paedi-atr Perinatal Epidemiol. 1992;6:434 – 459
15. Neonatal Intensive Care for Low Birth Weight Infants. Cost and Effectiveness:
Health Technology Case Study 38. Washington, DC: US Congress, Office
of Technology Assessment; 1987
16. Hack M, Klein NK, Taylor HG. Long-term developmental outcomes of low birth weight infants. The Future of Children. 1995;5:176 –196 17. Msall MC, Buck GE, Rogers RT, Merke D, Catarzaro NL, Zorn WA. Risk
factors for major neurodevelopmental impairment and need for special education resources in extremely premature infants. J Pediatr. 1991;118: 606 – 610
18. Hoffman EL, Bennett FC. Birth weight less than 800 grams: Changing outcomes and influences of gender and gestation number. Pediatrics. 1990;86:27–34
19. Bernbaum J, Hoffman-Williamson M, Workman K, McCormick M. Cog-nitive abilities and educational needs of,800 gm infants at school age.
Pediatr Res. 1992;31:243. Abstract
20. Hack M, Taylor G, Klein N, Eibeu R, Schatschneider C, Mercuri-Minich N. School-age outcomes in children with birth weights under 750 g.
N Engl J Med. 1994;331:753–757
21. Rossi PH, Freeman HE. Evaluation: A Systematic Approach. 5th ed. New-bury Park, CA: Sage Publications; 1993
22. Boyle MH, Torrance GW, Sinclair JL, Horwood SP. Economic evalua-tion of neonatal intensive care for very low birthweight infants. N Engl
J Med. 1983;308:1330
23. McCormick MC, Richardson DK. Long term costs of perinatal disabil-ities. In: Tauesch HW, Ballard RH, Avery ME, eds. Schaffer Avery’s
Diseases of the Newborn. 6th ed. Philadelphia, PA: WB Saunders Co; In
press
24. Avery ME, Tooley WH, Keller JB, et al. Is chronic lung disease in low birth weight infants preventable? A survey of eight centers. Pediatrics. 1987;79:26 –30
25. Hack M, Horbar JD, Malloy MH, Tyson JE, Alright E, Wright L. Very low birth weight outcomes of the National Institute of Child Health and Human Development neonatal network. Pediatrics. 1991;87:587–597
26. Horbar JD, McGuiliffe TL, Adler SM, et al. Variability in 28-day out-comes for very low birth weight infants in 11 neonatal intensive care units. Pediatrics. 1988;82:554 –559
27. International Neonatal Network. The CRIB (Clinical Risk Index for Babies) score: a tool for assessing initial risk and comparing perfor-mance of neonatal intensive care units. Lancet. 1993;342:193–198 28. Teplin SW, Burchinal M, Johnson-Martin N, Humphrey RA, Kraybill
EN. Neurodevelopmental, health and growth status at age 6 years of children with birth weights less than 1001 grams. J Pediatr. 1991;118: 768 –777
29. Knobloch H, Rider R, Harper P, Pasamanick B. Neuropsychiatric se-quelae of prematurity. A longitudinal study. JAMA. 1956;161:581–585 30. Niswander KR, Gordon M. The Women and Their Pregnancies.
Philadel-phia, PA: WB Saunders Co; 1972
31. Hardy JB, Drage JS, Jackson EC. The First Year of Life. Baltimore, MD: Johns Hopkins University Press; 1979
32. Broman SH, Nichols PL, Kennedy WA. PreSchool IQ. Prenatal and Early
Developmental Conciliate. Hillsdale, NJ: Lawrence Erlbaum Associates;
1975
33. Tyson J. Evidence-based ethics and the care of premature infants. The
Future of Children. 1995;5:197–213
34. Stolz JW. Restricting access to NICU care elevates mortality with min-imal economic savings. Pediatr Res. 1995;37:275. Abstract
35. Meadows W, Reimshisel T, Lantos J. Birth weight-specific mortality for extremely low birth weight infants vanishes by four days of life: epi-demiology and ethics in the neonatal intensive care unit. Pediatrics. 1996;97:636 – 643
36. Barfield WD, Wampler NS, Wise PH. Mandated non-resuscitation: ra-cial discrimination against premature black infants? Pediatr Res. 1995; 37:249. Abstract
37. Murphy CC, Yeargin-Allsopp M, Decoufle P, Drews CD. Prevalence of cerebral palsy among ten-year-old children in metropolitan Atlanta, 1985 through 1987. J Pediatr. 1993;123:S13-S19
38. Yeargin-Allsopp M, Murphy CC, Oakley GP, Sikes RK. A multiple source method for studying the prevalence of developmental disabili-ties in children: The Metropolitan Atlanta Developmental Disabilidisabili-ties Study. Pediatrics. 1992;89:624 – 630
39. Grether JK, Nelson KB, Emery ES, Cummins SK. Prenatal and perinatal factors and cerebral palsy in very low birth weight infants. J Pediatr. 1996;128:407– 414
40. Ment LR, Oh W, Ehrenkranz RA, Phillip AG et al. Low-dose endo-methacin therapy and extension of intraventricular hemorrhage: a multi-center trial. J Pediatr. 1994;124:951–955
41. Crowley P, Chalmers I, Keirse MJNC. The effects of corticosteroid administration before preterm delivery: an overview of the evidence from controlled trials. Br J Obstet Gynaecol. 1990;97:11–15
42. Nelson KB, Guther JK. Can magnesium sulfate reduce the risk of cerebral palsy in very low birthweight infants? Pediatrics. 1995;95: 263–269
43. Fujiwara T, Konishi M, Chida S, et al. Surfactant replacement therapy with a single post ventilatory dose of a reconstituted bovine surfactant in preterm neonates with respiratory distress syndrome: final analyses of a multi-center, double-blind randomized trial and comparison with similar trials. Pediatrics. 1990;86:753–764
44. Gray J, Richardson DK, McCormick MC, Workman K, Goldmann DA. Score for acute neonatal physiology (SNAP) and risk of intraventricular hemorrhage (IVH). Pediatr Res. 1992;31:249. Abstract
45. Anderson C, Richardson D, Leviton A. Illness severity during the first 24 hours of life and increased incidence of ROP, BPD, and IVH in VLBW infants. Pediatr Res. 1995;37:248. Abstract
46. Saigal S, Rosenbaum P, Hattersley B, Milner R. Decreased disability rate among 3-year-old survivors weighing 501 to 1000 grams at birth and born to residents of a geographically defined region from 1981 to 1984 compared with 1977 to 1980. J Pediatr. 1989;114:839 – 846
47. The Victorian Infant Collaborative Study Design Group. Improvement of outcome for infants of birth weight under 1000g. Arch Dis Child. 1991;66:765–769
48. McCormick MC, Brooks-Gunn J, Workman-Daniels K, Turner J, Peckham GJ. The health and developmental status of very low birth weight children at school age. JAMA. 1992;267:2204 –2208
49. Schreuder AM, Veen S, Ens-Dokkum MH, Verloove-Vanhorick SP, Brand R, Ruys JH. Standardized method of follow-up assessment of preterm infants at the age of 5 years: use of the WHO classification of impairments, disabilities and handicaps. Paediatr Perinatal Epidemiol. 1992;6:363–380
preterm and very-low-birth weight infants at five years of age. Lancet. 1991;338:33–36
51. Saigal S, Rosenbaum P, Stoskopf B, et al. Comprehensive assessment of the health status of extremely low birth weight children at eight years of age: comparison with a reference group. J Pediatr. 1994;125:411– 417 52. Saigal S, Fieny D, Furlong W, Rosenbaum P, Burows E, Torrance G.
Comparison of health-related quality of life of extremely low birth weight children and a reference group of children at age eight years.
J Pediatr. 1994;125:418 – 425
53. Saigal S, Fieny DH, Furlong WJ, Rosenbaum PL, Burrows E. Self-perceived health status and health-related quality of life of extremely low-birth-weight infants at adolescence. JAMA. 1996;276:453– 459 54. Saigal S, Furlong WJ, Rosenbaum PL, Fieny DH. Do teens differ from
parents in rating health-related quality of life? A study of premature and control teen/parent dyads. Pediatr Res. 1995;37:271. Abstract 55. Saigal S, Szatmari P, Rosenbaum P, Campbell D, King S. Cognitive
abilities and school performance of extremely low birth weight children and matched term control children at age 8 years: a regional study.
J Pediatr. 1991;118:751–760
56. Hack M, Breslau N, Aram D, Weissman B, Klein N, Borowski-Clark E. The effect of very low birth weight and social risk on neurocognitive abilities at school age. J Devel Behav Pediatr. 1992;13:412– 420 57. Saigal S, Rosenbaum P, Szatmari P, Campbell D. Learning disabilities
and school problems in a regional cohort of extremely low birthweight (,1000 g) children: a comparison with term controls. J Dev Behav Pediatr. 1991;12:294 –300
58. Klebanov PK, Brooks-Gunn J, McCormick MC. School achievement and failure in very low birth weight children. J Dev Behav Pediatr. 1991;12: 294–300
59. McCormick MC, Baker J, Brooks-Gunn J, Turner J, Workman-Daniels K, Peckham GJ. Cohort reconstruction: which infants can be restudied at school age? Pediatr Perinat Epidemiol. 1991;5:410 – 422
60. McCormick MC, Brooks-Gunn J, Turner J, Workman-Daniels K, Peckham GJ. Maternal rating of child health at school age: does the vulnerable child syndrome persist? Pediatrics. 1993;92:380 –388 61. McCormick MC, Brooks-Gunn J, Turner J, Workman-Daniels K. The
behavioral and emotional well-being of school age children of different birth weights. Pediatrics. 1996;97:855– 859
62. McCormick MC, McCarton C, Tonascia J, Brooks-Gunn J. Early educa-tional intervention for very low birth weight infants: results from the Infant Health & Development Program. J Pediatr. 1993;123:527–533 63. Gilkerson L, Gorski PA, Panitz P. Hospital-based intervention for preterm
infants and their families. In: Meisels SJ, Shonkoff JP, eds. Handbook of Early
Childhood Intervention. Cambridge, England: Cambridge University Press;
1990
64. Jones R, Wincott E, Elbourne D, Grant A. Controlled trial of dexameth-asone in neonatal chronic lung disease: a 3-year follow-up. Pediatrics. 1995;96:987–906
65. Richardson DK, Gray JE, McCormick MC, Workman-Daniels K, Goldmann DA. Score for acute neonatal physiology (SNAP): a physio-logic severity index for neonatal intensive care. Pediatrics. 1993;91: 617– 623
66. Richardson DK, Gray JE, McCormick MC, Workman-Daniels K, Goldman DA. Birth weight and illness severity: independent predictors of neonatal mortality. Pediatrics. 1993;91:969 –975
67. Gray JE, Richardson DK, McCormick MC, Workman-Daniels K, Goldmann DA. Neonatal therapeutic index scoring system (NTISS): a therapy-based severity of illness index. Pediatrics. 1992;90:561–567 68. Hobbs N, Perrin JM, eds. Issues in the Care of Children With Chronic
Illness. San Francisco, CA: Jossey-Bass Publishers; 1985
69. Levin MD, Carey WB, Crocker AC, Gross RT, eds.
Developmental-behavioral Pediatrics. Philadelphia, PA: WB Saunders Co; 1983
70. Bronfenbrenner U. Ecology of the family as a context for human devel-opment research perspectives. Dev Psychol. 1986;22:723–742
71. Sameroff AJ, Fiese BH. Transactional regulation and early intervention. In: Meisels SJ, Shonkoff JP, eds. Handbook of Early Childhood Intervention. Cambridge, England: Cambridge University Press; 1990
72. Stevens SM, Richardson DK, Gray JE, Goldmann DA, McCormick MC. Estimating mortality risk: an analysis of clinicians’ judgments.
Pediat-rics. 1994;93:945–950
73. Lee SK, Penner PL, Cox M. Comparison of the attitudes of health care professionals and parents towards active treatment of very low birth weight infants. Pediatrics. 1991;88:110 –114
74. Lee SK, Penner PL, Cox M. Impact of very low birth weight infants on the family and its relation to parental attitudes. Pediatrics. 1991;88: 105–109
75. Lewit EM, Baker LS, Corman H, Shiono PH. The direct cost of low birth weight. The Future of Children. 1995;5:35–56
76. Pollack IF. Brain tumors in children. N Engl J Med. 1994;331:1500 –1507 77. Koskiniemi M, Kyyka T, Nybo T, Jarho L. Long-term outcome after severe brain injury in preschoolers is worse than expected. Arch Pediatr
Adolesc Med. 1995;149:249 –254
78. Pomeroy SL, Holmes SJ, Dodge PR, Feigen RD. Seizures and other neurologic signals of bacterial meningitis in children. N Engl J Med. 1990;323:1651–1657
79. Taylor HG, Mills EL, Ciampi A et al. The sequelae of hemophilus influenzae meningitis in school-age children. N Engl J Med. 1990;323: 1657–1663
80. Franco SM, Cornelius VE, Andrews BF. Long-term outcome of neonatal meningitis? Am J Dis Child. 1992;146:567–571
81. Dixon J, Welch HG. Priority setting: lessons from Oregon. Lancet. 1991; 337:891– 894
82. Eisen M, Donald CA, Ware JE, Brook RH. Conceptualization and
Mea-surement of Health for Children in the Health Insurance Study. Santa
Monica, CA: Rand; 1984. (Publication No. R-2313-NEW)
83. Peterson JL, Zill N. Marital description, parent-child relationships, and behavior problems in children. Marriage Fam. 1986;48:295–307 84. Harter S. The perceived competence scale for children. Child Dev. 1982;
53:87–97
85. Wechsler D. Wechsler Intelligence Scale for Children. New York, NY: Psychological Corporation; 1974
86. Scott DT, Bauer CR, Kraemer J, Tyson J. A neonatal health index for preterm infants. Pediatr Res. 1989;25:263. Abstract
87. Ries PW. Americans Assess Their Health: United States, 197f. National Center for Health Statistics. Series 10, No 142. DHHS Pub No: (PHS)83–11570. Washington, DC: US Government Printing Office; 1983
88. Goldberg DP. The Detection of Psychiatric Illness by Questionnaire. Maudsley Monograph 21. London, England: Oxford University Press; 1972
89. Regier DA, Myers JK, Kraemer M, et al. The NIMH Epidemiologic Catchment Area Program. Historical context, main objective, and study population characteristics. Arch Gen Psychiatry. 1984;41: 934 –941
The Status of Pediatric Practice
Guidelines
ABBREVIATIONS. IOM, Institute of Medicine; AAP, American Academy of Pediatrics; EPSDT, Early Periodic Screening Diagno-sis and Treatment; GAPS, Guidelines for Adolescent Preventive Services; AHCPR, Agency for Health Care Policy and Research.
Clinicians caring for children increasingly encoun-ter practice guidelines. Guidelines have emerged as a driving force in American medicine. They are ap-pearing more regularly in academic journals, and are often the basis of audits by health insurers. Pediatri-cians are no longer shielded from this component of the quality of care revolution.
Because of the expanded presence of guidelines in the daily work of clinicians, and the substantial ex-penditure of time and resources by government, medical societies, hospitals, and insurers in guide-line-related activities, we convened a conference to review the status of pediatric practice guidelines. The goal of the conference was to establish a dialogue
Guidelines from Agency for Health Care Policy Research are available by calling 1-800-358-9295; guidelines from the American Academy of Pediat-rics are available by calling 1-847-228-5005 (ask for Publications). Received for publication Oct 2, 1996; accepted Oct 8, 1996.
Reprint requests to (H.B.) Boston City Hospital, Maternity 415, 818 Harrison Ave, Boston, MA 02118.
DOI: 10.1542/peds.99.6.869
1997;99;869
Pediatrics
Marie C. McCormick
Questions?
The Outcomes of Very Low Birth Weight Infants: Are We Asking the Right
Services
Updated Information &
http://pediatrics.aappublications.org/content/99/6/869
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/99/6/869#BIBL
This article cites 73 articles, 18 of which you can access for free at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.99.6.869
1997;99;869
Pediatrics
Marie C. McCormick
Questions?
The Outcomes of Very Low Birth Weight Infants: Are We Asking the Right
http://pediatrics.aappublications.org/content/99/6/869
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.