AllStreptococcus bovisblood culture isolates recovered from January 2003 to January 2010 (nⴝ52) at the Hospital Universitario Ramo´n y Cajal were reidentified on the basis of their genetic traits using new taxonomic criteria. Initial identification was performed by the semiautomatic Wider system (Fco. Soria-Melguizo, Spain) and the API 20 Strep system (bioMe´rieux, France). All isolates were reidentified by PCR amplification and sequencing of both the 16S rRNA and sodA genes and by mass spectrometry using matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS; Bruker, Germany). Results of 16S rRNA/sodA gene sequencing were as follows: Streptococcus gallolyticus subsp. gallolyticus, 14/14 (number of isolates identified by 16S rRNA/number of isolates identified bysodAgene sequencing);Streptococcus gallolyti-cussubsp.pasteurianus, 24/24;Streptococcusspp., 7/0;Streptococcus infantariussubsp.infantarius, 0/2; Strepto-coccus lutetiensis, 0/5;Leuconostoc mesenteroides, 4/0; andLactococcus lactis, 3/3. MALDI-TOF MS identified 27
S. gallolyticusisolates but not at the subspecies level, 4L. mesenteroidesisolates, 3L. lactisisolates, and 6S. lutetiensisisolates, whereas 12 isolates rendered a nonreliable identification result. Pulsed-field gel electro-phoresis grouped allS. gallolyticussubsp.gallolyticusisolates into 3 major clusters clearly different from those of theS. gallolyticussubsp.pasteurianusisolates, which, in turn, exhibited no clonal relationship. The percent-ages of resistance to the tested antimicrobials were 38% for erythromycin, 23% for fosfomycin, 10% for levofloxacin, 6% for tetracycline, and 4% for co-trimoxazole. The most frequent underlying diseases were hepatobiliary disorders (53%), endocarditis (17%), and malignancies (12%). We conclude that sequencing of thesodAgene was the most discriminatory method and thatS. gallolyticussubsp.pasteurianusappears to have a higher genetic diversity thanS. gallolyticussubsp.gallolyticus.
Streptococcus bovis, a nonenterococcal group D Streptococ-cus, can be found as part of the human gastrointestinal micro-biota in 5 to 16% of individuals (17). However, it causes bac-teremia and endocarditis, particularly in men and in the elderly (7, 8). The association ofS. bovisbacteremia and colon tumors was established in the late 1970s (14). Moreover, recent studies have described a frequent association between its isolation and chronic liver and biliary tract disorders (10).
Streptococcal taxonomy has progressively changed accord-ing to the description of new species originally grouped asS. bovis. During the late 1990s and at the beginning of the first decade of the 2000s, several authors renamedS. bovisbiotype I asStreptococcus gallolyticussubsp. gallolyticus(21), biotype II/1 asStreptococcus lutetiensis(18), and finally, biotype II/2 as
S. gallolyticussubsp.pasteurianus(20).
Clinicians still remain unfamiliar with the new taxonomy of
S. bovis species, mostly due to the complexity of the current nomenclature and specific identification requirements based on molecular microbiology techniques not available in routine clinical laboratories. Nevertheless, due to their specific disease association and their microbiology features, a proper
identifi-cation of theS. bovisisolates is needed. The aim of this study was to review allS. bovisbacteremic episodes documented over the last 7 years at the Hospital Universitario Ramo´n y Cajal, focusing on the new taxonomy and the probable association of different subspecies and pathologies.
MATERIALS AND METHODS
Bacterial identification.AllS. bovisisolates (n⫽52, from 51 patients) causing bacteremia recovered from blood cultures between January 2003 and January 2010 were studied. Initially,S. bovisidentification was routinely performed using the commercial API 20 Strep gallery (bioMe´rieux, Marcy l’Etoile, France) and the semiautomated Wider system (Fco. Soria Melguizo, Madrid, Spain) (5). The ability to grow on bile esculin agar (BD, NY) was determined after 24 h of incubation at 37°C. Isolates were tested for the presence of Lancefield streptococcal antigen D by agglutination using a Slidex Strepto Plus kit (bioMe´rieux, Marcy l’Etoile, France).
Subsequently, both 16S rRNA gene PCR with universal primers (primer 16-F [5⬘-AGGATTAGATACCCTGGTAGTCCA-3⬘] and primer 16-R [5⬘-AGGCCC GGGAACGTATTCAC-3⬘]) andsodAPCR with degenerate primers (primerdl [5⬘-CCITAYICITAYGAYGCIYTIGARCC-3⬘] and primerd2[5⬘-ARRTART AIGCRTGYTCCCAIACRTC-3⬘]) were performed (18). Amplicons (500 bp for 16S rRNA and 609 bp forsodA) were sequenced using an ABI Prism 377 automated sequencer (Perkin Elmer, Norwalk, CT) after purification with ExoSAP-IT (Amersham, Bucks, United Kingdom). Sequences were aligned us-ing the ClustalW tool from the website www.ebi.ac.uk, and phylogenetic trees were constructed with TreeView software (Michael Eisen, Stanford University, Stanford, CA).
Mass spectrometry using a Bruker Biotyper MALDI78 TOF MS matrix-as-sisted laser desorption ionization–time of flight mass spectrometry (MALDI TOF MS) system (Bruker Daltonics, Germany) was also performed as part of the bacterial reidentification scheme (3).
* Corresponding author. Mailing address: Servicio de Microbi-ología, Hospital Universitario Ramo´n y Cajal, Ctra. Colmenar, Km 9,1, 28034 Madrid, Spain. Phone: 34 91 336 8542. Fax: 34 91 336 8809. E-mail: [email protected].
䌤Published ahead of print on 13 July 2011.
3228
on May 16, 2020 by guest
http://jcm.asm.org/
Antimicrobial susceptibility testing.Susceptibility testing (microdilution method) was performed using Wider panels for Gram-positive organisms, and the results were interpreted according to Clinical and Laboratory Standards Institute criteria (5, 6).
Genetic diversity.Clonal relatedness was determined by pulsed-field gel electro-phoresis (PFGE) using a protocol initially described forStreptococcus suisserotype 2 (15). A dendrogram was constructed using the Phoretix (version 5.0) software (Nonlinear Dynamics Ltd., United Kingdom) on the basis of the Dice coefficient.
Patients.Clinical charts of all patients were reviewed with the approval of the Ethics Committee of the Hospital Universitario Ramo´n y Cajal to assess both demographic and clinical data as well as diagnostics and treatments. All patients in whom colonic pathologies were suspected were submitted to examination by colonoscopy. A possible biliary source of bacteremia was assigned if there was a clinical or surgical diagnosis of acute cholecystitis or cholangitis, after the exclu-sion of other possible foci of infection.
RESULTS
Isolates previously identified asStreptococcus boviswere re-identified using the current nomenclature. All 52 isolates,
in-cluding the nonstreptococcal ones, had a clear positive reac-tion with the latex agglutinareac-tion test for group DStreptococcus. Initial data from the API 20 Strep system were not available, and contemporary profiles corresponded to 29 S. bovis II/2 isolates (which included 24S. gallolyticus subsp.pasteurianus
and 5S. lutetiensisisolates, according to the sodA identifica-tion), 14S. bovisI isolates, 2S. bovisII/4 isolates, 3 Lactococ-cus lactisisolates, and 4Leuconostocsp. isolates.
Nucleotide sequences of 16S rRNA amplicons (500 bp) al-lowed the classification of the isolates asStreptococcus gallo-lyticus subsp. gallolyticus (n ⫽ 14), Streptococcus gallolyticus
subsp.pasteurianus(n⫽24),Streptococcusspp. (n⫽7), Lac-tococcus lactis(n⫽3), andLeuconostoc mesenteroides(n⫽4) (Fig. 1).
Isolates were also reclassified on the basis of the nucleotide sequence of an internal fragment of thesodA gene asS. gal-FIG. 1. Clustering of 16S rRNA nucleotide sequences obtained from all 52 isolates and constructed by TreeView software.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:2.585.137.476.51.513.2]lolyticussubsp.gallolyticus(n⫽14),S. gallolyticussubsp. pas-teurianus(n⫽24),Streptococcus infantariussubsp.infantarius
(n⫽2),Streptococcus lutetiensis(n⫽5), andL. lactis(n⫽3). The sevenStreptococcussp. isolates not identified at the spe-cies level by the 16S rRNA sequence analysis were character-ized asS. infantariussubsp.infantariusandS. lutetiensisusing
sodAgene amplification and sequencing. Negative results for
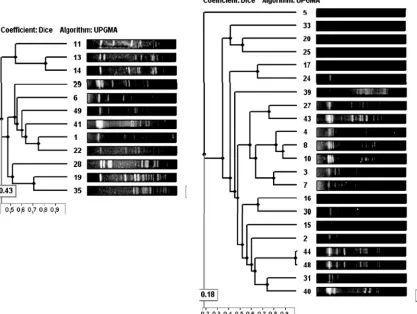
sodAamplification were consistently obtained in the 4 isolates previously identified as L. mesenteroides by 16S rRNA se-quencing. ThesodAnucleotide phylogenetic analysis discrim-inated theS. gallolyticussubsp.pasteurianusisolates into two clusters (Fig. 2), although the amino acid sequences remained identical (Fig. 3). However, several amino acid differences were detected in theS. gallolyticussubsp.gallolyticusgroup.
Finally, MALDI-TOF MS identified 27 S. gallolyticus iso-lates but not subspecies, 4L. mesenteroidesisolates, 3L. lactis
isolates, and 6S. lutetiensis isolates, whereas in 12 isolates a nonreliable identification result was obtained.
PFGE analysis with SmaI digestion grouped allS. gallolyticus
subsp.gallolyticusisolates into 3 major clusters clearly different from those of the S. gallolyticussubsp. pasteurianus isolates, which, in turn, exhibited no related PFGE patterns among them (Fig. 4).
[image:3.585.130.458.76.509.2]Antimicrobial susceptibility results are shown in Table 1. All isolates remained susceptible to penicillin, ampicillin, amoxi-cillin-clavulanate, oxacillin, quinupristin-dalfopristin, linezolid, and rifampin. Resistance to the glycopeptides vancomycin and teicoplanin was observed only inL. mesenteroidesisolates. As expected, all streptococcal isolates (n⫽45) showed low-level resistance to aminoglycosides. Additionally, 16 isolates exhib-ited high-level resistance (MIC50,⬎1,000 mg/liter) to strepto-mycin, whereas high-level resistance to gentamicin was not
FIG. 2. Clustering ofsodAnucleotide sequences obtained from non-Leuconostocisolates (n⫽48) and constructed by TreeView software.
on May 16, 2020 by guest
http://jcm.asm.org/
observed. Resistance percentages for the other antimicrobials tested varied according to the bacterial species (Table 1).
When clinical data from all 51 patients with documentedS. bovis bacteremia were considered, the patients’ median age was 73.5⫾ 15 years (range, 27 to 98 years; mode, 82 years). The gender distribution was 28 males (54.9%) and 23 females (45.1%). A mean of 6.5 episodes per year was documented, with the maximum (n ⫽ 10 episodes) occurring in 2005. An accumulation of cases between April and June (n ⫽21) was
observed, with the incidence from October to December being lower (n ⫽ 7). Blood samples for culture were obtained in different wards, with the emergency unit being the most fre-quent (51%), followed by the general medicine unit (16%), intensive care unit (10%), gastroenterology unit (8%), and others (15%). The most frequent symptoms at hospital admis-sion were fever and abdominal pain.
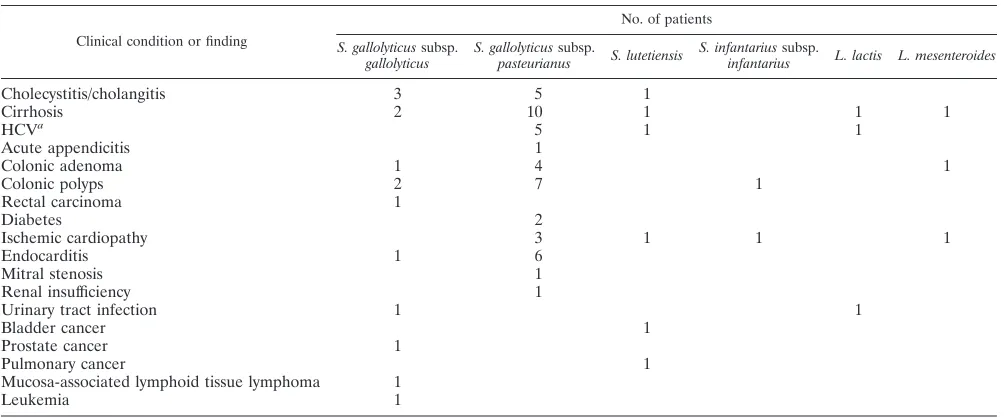
[image:4.585.43.549.92.227.2]The patients’ underlying diseases are shown in Table 2. The most common feature detected was hepatobiliary disorder
FIG. 3. Comparison of the amino acid sequences for the differentsodAalleles of thesodAprotein detected.
FIG. 4. Dendrogram obtained for the 24S. gallolyticussubsp.pasteurianusand 14S. gallolyticussubsp.gallolyticusisolates using the unweighted-pair group method using average linkages method and Phoretix (version 5.0) software.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.84.501.387.701.2](53%), followed by endocarditis (17.6%), cardiovascular dis-ease (11.7%), diverticulitis and/or colon polyps (11.7%), diges-tive tract carcinomas (8%), ferropenic anemia (6%), and other malignancies (4%). Only one patient died during the emic episode. Interestingly, a female had two different bacter-emic episodes separated by 3 years, and these were caused by genetically differentS. gallolyticussubsp.pasteurianusisolates.
DISCUSSION
The formerS. bovis group is, at present, divided into four major subspecies (12), with two of them (S. gallolyticussubsp.
gallolyticus, formerly S. bovis biotype I, and S. gallolyticus
subsp.pasteurianus, formerly S. bovisbiotype II/2) being ge-netically closely related and the other two (S. infantariussubsp.
infantariusandS. lutetiensis, namedS. infantariussubsp.coliby some authors [2] and formerlyS. bovisbiotype II/1) being more distantly related.Streptococcus gallolyticussubsp.macedonicus
is also a member of the group, but it is generally considered nonpathogenic for humans. However, mainly due to discrep-ancies still remaining, a deeply genetics-based classification is awaited.
A clear association betweenS. gallolyticussubsp.gallolyticus
causing bacteremia and/or endocarditis and the presence of
colon cancer has been reported (1, 4, 11). Nevertheless, the basis of this association is still not completely understood. In this study, half of the patients had hepatobiliary disorders, whereas endocarditis or cardiovascular diseases were observed in only 17.6 and 11.7% of the patients, respectively. Colonic polyps and carcinomas of the gastrointestinal tract were diag-nosed in 11.7 and 8% of the patients, respectively. When only those patients withS. gallolyticussubsp.gallolyticusbacteremia (n ⫽ 14) were considered, malignances had previously been diagnosed in 7 of them (50%), although some of them were not related to the gastrointestinal tract (lymphoma, leukemia, or prostate carcinoma), even though colonoscopy exploration was not performed in all patients.
Different authors suggest a positive association betweenS. gallolyticus subsp. gallolyticus isolation and male and elderly patients and endocarditis (7, 18). In our case, the gender dis-tribution was balanced (55% of male individuals), the age of presentation was about 70 years, and endocarditis was detected in only 17% of patients. Our results are in concordance with those recently published by another Spanish group (9).
During the study period, 76,089 blood samples from patients with suspected bacteremia were processed in our laboratory. From these, 6,935 (9.1%) were positive, and 52 of them
ren-TABLE 2. Patients’ clinical features
Clinical condition or finding
No. of patients
S. gallolyticussubsp. gallolyticus
S. gallolyticussubsp.
pasteurianus S. lutetiensis
S. infantariussubsp.
infantarius L. lactis L. mesenteroides
Cholecystitis/cholangitis 3 5 1
Cirrhosis 2 10 1 1 1
HCVa 5 1 1
Acute appendicitis 1
Colonic adenoma 1 4 1
Colonic polyps 2 7 1
Rectal carcinoma 1
Diabetes 2
Ischemic cardiopathy 3 1 1 1
Endocarditis 1 6
Mitral stenosis 1
Renal insufficiency 1
Urinary tract infection 1 1
Bladder cancer 1
Prostate cancer 1
Pulmonary cancer 1
Mucosa-associated lymphoid tissue lymphoma 1
Leukemia 1
a
HCV, hepatitis C virus.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:5.585.42.540.83.171.2] [image:5.585.42.545.508.717.2]dered anS. bovisidentification (0.74%), although considering the data from our present work, only 45 isolates in fact corre-sponded to this species (0.64%). During the same period, 270 cases of infective endocarditis were diagnosed at the Hospital Universitario Ramo´n y Cajal, and these were mostly due to
Staphylococcus aureus (30.7%), coagulase-negative staphylo-cocci (17.4%), andEnterococcus(13.3%).S. boviswas identi-fied in 7 cases (6S. gallolyticussubsp.pasteurianusisolates and 1S. gallolyticussubsp.gallolyticusisolate), representing 2.6% of all cases of endocarditis (E. Navas et al., unpublished results). Surprisingly, 4Leuconostoc mesenteroidesand 3Lactococcus lactisisolates causing bacteremia were initially identified asS. bovis by the semiautomated system used in our laboratory. When reidentification was obtained by 16S rRNA gene se-quencing, the bacteria were reidentified using the same system, and it was observed that the misleading identification was due to their slow biochemical reactivity; at 24 h of incubation the identification was againS. bovis, whereas at 48 h, the identifi-cation was correct. Moreover, vancomycin resistance in Leu-conostocisolates was observed only at 48 h. Another important factor to be considered is the positive agglutination of our
Leuconostoc and Lactococcus isolates for Lancefield antigen D. We were unable to find similar references to this finding, and this fact has been demonstrated only forPediococcussp. isolates (16).
As it has been described by other authors (13, 19), we de-tected differences in isolate identification between the 16S rRNA and the sodA gene sequencing methods, with partial sequencing of thesodAgene being considered the most accu-rate method of identification. Recently, a high concordance between MALDI-TOF MS andsodA nucleotide sequencing has been described (12), although in our experience, the Bruker technology is not yet able to identify Streptococcus
isolates, especiallyS. gallolyticus subsp.pasteurianus. The re-sults obtained with the contemporary API 20 Strep system agree with thesodA sequencing classifications, although 5S. lutetiensisisolates showed the same profile as the S.gallolyticus
subsp. pasteurianus isolates. Nevertheless, the API 20 Strep system can be considered a useful method to discriminate the two mainS. gallolyticussubspecies, but from clinical and epi-demiological points of view, it could also be of interest to further discriminate S. infantarius subsp. infantarius and S. lutetiensisusing thesodAanalysis.
In spite of many efforts that have been made to improveS. bovis group identification, data from genetic studies remain unavailable. The multilocus sequence typing tool has not yet been developed, and there has been only one reference de-scribing high genetic diversity among ItalianS. bovisisolates, which was determined by PFGE (22). In our experience, high genetic diversity was also observed among the 45 streptococcal isolates.
Our study demonstrated that in a routine clinical microbi-ology laboratory, incorporation of a MALDI-TOF MS system will partially solve the problems with identification of members of theS. bovisgroup. Nevertheless, this system will indicate the presence ofS. gallolyticusand further molecular testing can be performed if needed. The presence of data entries in the da-tabase for differentS. gallolyticussubspecies should be a goal for future MALDI-TOF MS systems for testing of other spe-cies.
ACKNOWLEDGMENTS
R.D.C. has a Miguel Servet contract (CB05/137) from the Instituto de Salud Carlos III-FIS. M.R.-B. has a contract from the Instituto de Salud Carlos III-FIS, project AI07/90034. This work was partially funded by the European Project TROCAR (HEALTH-F3-2008-223031).
REFERENCES
1.Abdulamir, A. S., R. R. Hafidh, and F. A. Bakar.2011. The association of Streptococcus bovis/gallolyticuswith colorectal tumors: the nature and the underlying mechanisms of its etiological role. J. Exp. Clin. Cancer Res.30:11. 2.Beck, M., R. Frodl, and G. Funke.2008. Comprehensive study of strains previously designatedStreptococcus bovisconsecutively isolated from human blood cultures and emended description ofStreptococcus gallolyticusand Streptococcus infantariussubsp.coli.J. Clin. Microbiol.46:2966–2972. 3.Bizzini, A., C. Durussel, J. Bille, G. Greub, and G. Prod’hom.2010.
Perfor-mance of matrix-assisted laser desorption ionization–time of flight mass spectrometry for identification of bacterial strains routinely isolated in a clinical microbiology laboratory. J. Clin. Microbiol.48:1549–1554. 4.Boleij, A., R. M. Schaeps, and H. Tjalsma.2009. Association between
Strep-tococcus bovisand colon cancer. J. Clin. Microbiol.47:516.
5.Canto´n, R., et al.2000. Evaluation of the Wider system, a new computer-assisted image-processing device for bacterial identification and susceptibil-ity testing. J. Clin. Microbiol.38:1339–1346.
6.Clinical and Laboratory Standards Institute.2007. Performance standards for antimicrobial susceptibility testing; 17th informational supplement. Doc-ument M100-S17. Clinical and Laboratory Standards Institute, Wayne, PA. 7.Corredoira, J., et al.2008. Characteristics ofStreptococcus bovisendocarditis and its differences with Streptococcus viridansendocarditis. Eur. J. Clin. Microbiol. Infect. Dis.27:285–291.
8.Durante-Mangoni, E., et al.2008. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch. Intern. Med.168:2095–2103.
9.Ferna´ndez-Ruiz, M., et al.2010.Streptococcus bovisbacteraemia revisited: clinical and microbiological correlates in a contemporary series of 59 pa-tients. J. Infect.61:307–313.
10.Gonza´lez-Quintela, A., C. Martínez-Rey, J. C. Castroagudin, M. C. Rajo-Iglesias, and M. J. Domínguez-Santalla.2001. Prevalence of liver disease in patients withStreptococcus bovisbacteraemia. J. Infect.42:116–119. 11.Gupta, A., R. Madani, and H. Mukhtar.2010.Streptococcus bovis
endocar-ditis, a silent sign for colonic tumour. Colorectal Dis.12:164–171. 12.Hinse, D., et al.2011. Differentiation of species of theStreptococcus bovis/
equinus-complex by MALDI-TOF mass spectrometry in comparison tosodA sequence analyses. Syst. Appl. Microbiol.34:52–57.
13.Hoshino, T., T. Fujiwara, and M. Kilian.2005. Use of phylogenetic and phenotypic analyses to identify nonhemolytic streptococci isolated from bac-teremic patients. J. Clin. Microbiol.43:6073–6085.
14.Klein, R., et al.1977. Association ofStreptococcus boviswith carcinoma of the colon. N. Engl. J. Med.297:800–802.
15.Luey, C. K., et al.2007. Rapid pulsed-field gel electrophoresis protocol for subtyping ofStreptococcus suisserotype 2. J. Microbiol. Methods68:648–650. 16.Murray, P. R., E. J. Baron, J. H. Jorgensen, M. A. Pfaller, and R. H. Yolken (ed.).2003. Manual of clinical microbiology, 8th ed. American Society for Microbiology, Washington, DC.
17.Noble, C. J.1978. Carriage of group D streptococci in the human bowel. J. Clin. Pathol.31:1182–1186.
18.Poyart, C., G. Quesne, and P. Trieu-Cuot.2002. Taxonomic dissection of the Streptococcus bovisgroup by analysis of manganese-dependent superoxide dismutase gene (sodA) sequences: reclassification of ‘Streptococcus infan-tariussubsp.coli’ asStreptococcus lutetiensissp. nov. and ofStreptococcus bovisbiotype II.2 asStreptococcus pasteurianussp. nov. Int. J. Syst. Evol. Microbiol.52:1247–1255.
19.Sasaki, E., R. Osawa, Y. Nishitani, and R. A. Whiley.2004. Development of a diagnostic PCR assay targeting the Mn-dependent superoxide dismutase gene (sodA) for identification ofStreptococcus gallolyticus. J. Clin. Microbiol. 42:1360–1362.
20.Schlegel, L., et al.2000. Streptococcus infantarius sp. nov.,Streptococcus infantariussubsp.infantariussubsp. nov. andStreptococcus infantariussubsp. colisubsp. nov., isolated from humans and food. Int. J. Syst. Evol. Microbiol. 50:1425–1434.
21.Schlegel, L., F. Grimont, E. Ageron, P. A. D. Grimont, and A. Bouvet.2003. Reappraisal of the taxonomy of theStreptococcus bovis/Streptococcus equinus complex and related species: description ofStreptococcus gallolyticussubsp. gallolyticussubsp. nov.,S. gallolyticussubsp.macedonicussubsp. nov. and S. gallolyticussubsp.pasteurianussubsp. nov. Int. J. Syst. Evol. Microbiol.53: 631–645.
22.Tripodi, M. F., R. Fortunato, R. Utili, M. Triassi, and R. Zarrilli.2005. Molecular epidemiology ofStreptococcus boviscausing endocarditis and bac-teraemia in Italian patients. Clin. Microbiol. Infect.11:814–819.