Heel-Lancing in Newborns: Behavioral and Spectral
Analysis Assessment of Pain Control Methods
WHAT’S KNOWN ON THIS SUBJECT: Newborns may experience pain, and this pain experience can alter clinical outcome, brain development, and subsequent behavior. Various pain control methods are known to alleviate pain in newborns, but these have not yet been evaluated concurrently and by objective methods.
WHAT THIS STUDY ADDS: We evaluated several simple, common pain control methods by using concomitantly the Neonatal Facial Coding System, physiologic markers of pain, and spectral analysis of heart rate variability, thereby obtaining an objective
multidimensional evaluation of the efficacy of these methods.
abstract
OBJECTIVE:Pain experience can alter clinical outcome, brain develop-ment, and subsequent behavior in newborns, primarily in preterm infants. The aims of this study were (1) to evaluate several simple, commonly used methods for pain control in newborns and (2) to eval-uate the concordance between behavioral and autonomic cardiac re-activity to pain in term neonates during heel-lancing.
METHODS:A prospective study was conducted of 180 term newborn infants who were undergoing heel-lancing for routine neonatal screen-ing of phenylketonuria and hypothyroidism. Newborns were assigned to 6 groups: (1) control (no pain relief intervention); (2) nonnutritive sucking; (3) holding by mother; (4) oral glucose solution; (5) oral for-mula feeding; or (6) breastfeeding. Outcome measures included the Neonatal Facial Coding System score; cry duration; and autonomic variables obtained from spectral analysis of heart rate variability be-fore, during, and after heel-lancing.
RESULTS:Infants with no pain control showed the highest pain mani-festation compared with newborns to whom pain control was pro-vided. Infants who breastfed or received an oral formula showed the lowest increase in heart rate (21 and 23 beats per minute, respectively, vs 36; P⬍.01), lowest neonatal facial score (2.3 and 2.9, respectively, vs 7.1;P⬍.001), lowest cry duration (5 and 13 seconds, respectively, vs 49;P⬍.001), and lowest decrease in parasympathetic tone (⫺2 and
⫺2.4, respectively, vs 1.2;P⬍.02) compared with the other groups.
CONCLUSIONS:Any method of pain control is better than none. Feed-ing and breastfeedFeed-ing durFeed-ing heel-lancFeed-ing were found to be the most effective methods of pain relief.Pediatrics2009;124:e921–e926 AUTHORS:Amir Weissman, MD,aMichal Aranovitch, RN,
MSc,b,cShraga Blazer, MD,b,dand Etan Z. Zimmer, MDa,b
Departments ofaObstetrics and Gynecology anddNeonatology,
Rambam Health Care Campus, andbRappaport Faculty of
Medicine, Technion–Israel Institute of Technology, Haifa, Israel; andcDepartment of Neonatology, Lady Davis Carmel Medical
Center, Haifa, Israel
KEY WORDS
newborn, autonomic nervous system, heart rate, spectrum analysis, pain, analgesia
ABBREVIATIONS
HRV— heart rate variability ECG— electrocardiogram
NFCS—Neonatal Facial Coding System LF—low-frequency
HF— high-frequency
This trial has been registered at www.clinicaltrials.gov (identifier NCT00396838).
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0598 doi:10.1542/peds.2009-0598
Accepted for publication Jun 4, 2009
Address correspondence to Amir Weissman, MD, Department of Obstetrics and Gynecology, Rambam Health Care Campus, 8 Ha’Aliyah St, Haifa 35254, Israel. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
dures in nurseries and NICUs. These procedures are frequently performed without any pain relief. Throughout the history of neonatal care, pain and pain prevention in newborns have been un-recognized or undertreated. Recently, developmental physiology has pro-vided evidence that newborn infants, even the extremely preterm, have the basic neuronal circuitry needed for the processing of nociceptive infor-mation and are capable of mounting behavioral and physiologic distress responses to noxious stimulation. Moreover, infants may even experi-ence pain more acutely than older chil-dren and adults and may be more vul-nerable to its long-term effects.1–3 It has been recommended that the pain that newborns experience during med-ical procedures be minimized. Guide-lines, recommendations, and policy statements for the prevention of pain have been published throughout the world.3,4 Unfortunately, these recom-mendations are not yet fully imple-mented universally.5,6
Pain reaction typically comprises be-havioral and autonomic reactions.7 Be-cause self-reporting of pain is not ap-plicable to newborn infants, surrogate markers for neonatal pain assessment are used. Behavioral and physiologic parameters have been suggested, but no single method is exclusively related to pain response. Physiologic markers of pain usually include changes in heart rate, respiratory rate, blood pressure, and oxygen saturation. Be-havioral indicators include changes in facial expressions, body movements, and crying; however, these may be ab-sent in some neonates who are neuro-logically impaired, pharmaconeuro-logically treated, or intubated. The most effec-tive and safest way to decrease pain in neonates is yet unknown, although var-ious pain relief methods have been
ad-clude oral sucrose or glucose solution given before the procedure,8 breast-feeding,9 nonnutritive sucking,8 and skin-to-skin contact.10These methods have been shown to reduce pain in pre-term and pre-term neonates.
Heart rate has been frequently used as an objective physiologic marker of nox-ious events. Spectral analysis of heart rate variability (HRV) has emerged as a promising tool in the evaluation of the sympathovagal balance and the auto-nomic nervous system equilibrium during health and disease.11,12Because of their objective nature, these methods may be of special importance in new-borns, who cannot self-report during painful interventions, and serve as com-plementary means for the detection of the state of the autonomic nervous sys-tem during painful procedures.
Although there is abundant informa-tion on various pain relief techniques for newborns, there is a paucity of data regarding their effects on the auto-nomic nervous system during painful procedures. The aims of this study were (1) to evaluate several simple, commonly used methods for pain re-lief in newborns that measure physio-logic and behavioral variables nonin-vasively and assessing their effects on the autonomic nervous system and (2) to evaluate the concordance between behavioral and autonomic cardiac re-activity indicators of pain in term neo-nates during heel-lancing.
METHODS
Study Design
The local research ethics institutional review committee approved the study, and informed consent was obtained from the mother of each infant en-rolled in the study. Included were healthy newborns who were delivered at ⱖ37 weeks’ gestation and had an Apgar score of ⱖ7 at 5 minutes. All
comple-tion of the painful procedure (recovery period, phase 3).
Behavioral Data Acquisition
The infant’s face was video-recorded continuously by a trained nurse during the baseline, painful, and recovery pe-riods. The detailed facial activity was assessed by using the Neonatal Facial Coding System (NFCS),13,14 which in-cludes 7 predefined facial actions (brow bulge, eye squeeze, nasolabial furrow, open mouth, vertical mouth stretch, horizontal mouth stretch, and taut tongue). The NFCS was obtained from the last 30 seconds of the baseline period, the first 30 seconds after heel-lancing, and the first 30 seconds of the recovery period. The observer was not blinded to the group assignment.
Physiologic Signal Acquisition
Three standard surface chest elec-trodes were used to record a continu-ous ECG. Signals were digitally sam-pled to disk at 500 Hz by using a personal computer– based data acqui-sition system. Surface ECG activity was recorded continuously during the baseline, heel-lancing, and recovery periods. R waves were detected from the sampled ECG, and the R-R interbeat intervals were computed. Segments of interbeat intervals (2 minutes each) were selected from (1) the resting baseline period within 5 minutes be-fore the lancing, (2) the heel-lancing period starting 10 seconds after the prick and including the squeezing of the heel, and (3) the recovery period 2 minutes after the termination of the procedure. The epoch duration of 2 minutes was based on the need for a stable behavioral state and the ab-sence of gross movement artifact. Power spectral estimates of heart rate were quantified by using the area (power) of the spectrum in a low-frequency (LF) region (0.04 – 0.15 Hz) and a high-frequency (HF) region (0.15– 0.80 Hz), as well as by the ratio
of LF and HF power (LF-HF). All physio-logic and spectral analyses were per-formed by 1 of the study members, who was blinded to the newborns’ group assignment.
ECG Data Processing
The ECG was recorded through a 12-bit analog/digital data acquisition card (National Instruments, Austin, TX) with a sampling frequency of 500 Hz and stored in a binary format in a com-puter for offline studies. The signals were collected in a modified lead I or II configuration in an attempt to maxi-mize the R wave amplitude. The digi-tized ECG was then processed and an-alyzed via customized software to detect the R wave peaks. The R point of each QRS complex was defined, and the interval between 2 adjacent R points (the R-R interbeat interval) was computed. All intervals were visually inspected and manually edited, when necessary, to exclude noise and arti-facts. The edited segments accounted for⬍1% for each infant. A 2-minute “clean” segment of data was used for the analyses.
HRV Measures
Time Domain Analysis
HRV was evaluated in accordance with the guidelines of the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.11 The vari-ables computed were heart rate, mean N-N interval (normal to normal), SD of all intervals, and the square root of the mean squared differences between R-R intervals.
Frequency Domain Analysis
The power spectrum of the interbeat intervals was obtained by an autore-gressive model, applying an order of 16. Three frequency bands were de-fined: the very low frequency band (⬍0.03 Hz) related mainly to
thermo-regulation, the LF band (0.03– 0.15 Hz) related mainly to baroreflex control of arterial blood pressure that is modu-lated by both the parasympathetic and the sympathetic arms of the auto-nomic nervous system, and the HF band (0.15– 0.80 Hz) primarily was at-tributed to respiratory sinus arrhyth-mia and modulated by the parasympa-thetic system. The area under the respective frequency bands was inte-grated and expressed in absolute units. Total power and LF-HF ratio, re-garded as an index of sympathovagal balance, were also computed.
Statistical Analysis
A group-by-phase repeated measures analysis of variance was used to com-pare outcome measures across study periods (phase 1: baseline before heel-lancing; phase 2: heel-heel-lancing; phase 3: recovery period). Correlations be-tween the variables were examined by using Spearman rank-order correla-tions. Spectral variables with skewed distributions (HF and LF) were ana-lyzed after logarithmic transformation of the absolute values. A difference was considered statistically signifi-cant forP⬍.05. Group size was calcu-lated by a priori power analysis aiming at a power of 80% to allow a difference of 20% at a 2-sided significance level of 5% in each of the variables that we ex-amined. It indicated that a sample size of 25 participants would be adequate.
RESULTS
formula as compared with the control group (2.3⫾ 2.5 and 2.9 ⫾ 2.4, re-spectively, vs 7.1⫾1.15, respective-ly;P⬍.001). This was corroborated by the shortest crying duration in these 2 groups (5 and 13 seconds, respectively, vs 49 seconds in the control group;P⬍.001) and the low-est increase in heart rate (21 and 24 beats per minute, respectively, vs 37 beats per minute in the control group;P⬍.01).
Differences between baseline and painful periods in the LF spectral band (representing the sympathetic arm) were lowest in newborns who were formula fed or breastfed. The auto-nomic nervous system balance repre-sented by the LF-HF ratio showed vagal influence to be higher in the formula-fed and breastformula-fed newborns (positive numbers signify that the sympathetic arm dominates, whereas negative numbers denote the opposite: higher vagal dominance). We did not find significant differences between the groups in any of the variables during the recovery period (phase 3).
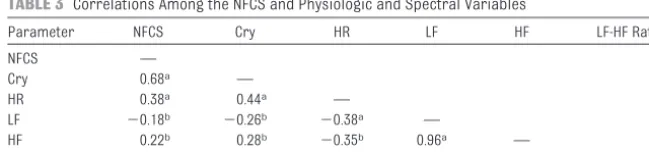
Correlations Between Behavioral and Physiologic Markers of Pain
Significant correlations were found between the NFCS and the duration of cry and between the increase in heart rate and the NFCS (Table 3).
Correlations Between Behavioral and Autonomic Markers of Pain
There were significant correlations be-tween the NFCS and the HF spectral power (which represents vagally me-diated effects) and the LF spectral power (which represents the sympa-thetic arm) and the LF-HF ratio (repre-senting the autonomic balance). The duration of cry was significantly corre-lated with heart rate and all spectral
variables (Table 3). Gender and mode of delivery had no significant effect on outcome measures.
DISCUSSION
In the past, pain management in new-borns has been either disregarded or underestimated. Various painful pro-cedures, sometimes performed on a daily basis, have been performed with no or only minimal pain relief mea-sures provided. In the past decade, it has been shown that newborns experi-ence pain during these invasive proce-dures. The more preterm the newborn, the more frequent is the exposure to these noxious procedures. Pain experi-ence in preterm infants or medically
(n⫽29) (n⫽30) (n⫽29) (n⫽31) (n⫽30) (n⫽31) Gestational age at birth, mean⫾SD, wk 39.8⫾1.5 39.6⫾1.2 39.4⫾1.1 39.5⫾1.3 39.1⫾1.4 39.7⫾1.2 Birth weight, mean⫾SD, g 3368⫾382 3364⫾460 3390⫾356 3157⫾397 3227⫾417 3398⫾428 Apgar at 5 min, mean⫾SD 9.8⫾0.5 9.9⫾0.3 9.9⫾0.3 9.9⫾0.3 9.9⫾0.2 9.7⫾1.7 Gender, M/F 16/13 15/15 16/13 15/16 13/17 16/15 Vaginal/cesarean delivery 21/8 21/9 18/11 19/12 17/13 21/7
No statistically significant differences were found among the groups in each of the variables.
TABLE 2 Differences Between the Painful and Baseline Periods in the Various Groups
Parameter Control Pacifier Holding Glucose Formula-feeding Breastfeeding NFCS 7.10⫾1.15 4.90⫾2.20a 4.80⫾2.40a 6.80⫾0.90 2.30⫾2.50a 2.90⫾2.40a
Duration of cry, s 48.9⫾23.5 32.5⫾26.0 27.1⫾20.5 26.4⫾16.2b 5.0⫾8.2a 13.3⫾9.2a
HR increase, beats per minute 36.5⫾19.5 36.5⫾22.2 40.5⫾18.7 27.8⫾17.6 21.4⫾12.9a 23.5⫾14.5b
HF, ms2/Hz ⫺33.6⫾70.3 ⫺11.1⫾49.2 ⫺21.3⫾60.2 0.8⫾49.0 5.8⫾47.0 4.7⫾45.9
LF, ms2/Hz ⫺138.0⫾127.0 ⫺111.0⫾164.0 ⫺144.0⫾227.0 ⫺117.0⫾141.0 ⫺93.0⫾129.0 ⫺92.0⫾230.0
LF-HF ratio 1.2⫾4.8 ⫺1.0⫾3.4 0.7⫾7.6 ⫺1.8⫾3.4b ⫺2.0⫾4.1c ⫺2.4⫾5.9c
HR indicates heart rate.
aP⬍.001. bP⬍.01, and cP⬍.02 versus control.
TABLE 3 Correlations Among the NFCS and Physiologic and Spectral Variables
Parameter NFCS Cry HR LF HF LF-HF Ratio NFCS —
Cry 0.68a —
HR 0.38a 0.44a —
LF ⫺0.18b ⫺0.26b ⫺0.38a —
HF 0.22b 0.28b ⫺0.35b 0.96a —
LF-HF ratio ⫺0.21b ⫺0.27b ⫺0.38a 0.97a ⫺0.94a —
HR indicates heart rate.
compromised neonates has been re-ported to have far-reaching conse-quences not only in the short-term but also in the long-term and can alter pain sensitivity, brain development, and even subsequent behavior.1,3,15–17
The interpretation of the newborn’s reactions to painful procedures is hampered by the limited sensitivity of our assessment methods, by the large variability of the newborn’s re-sponse to painful stimuli, and by the subjective nature of interpreting these data in clinical situations. These limitations have been extensively discussed.2–4
There is now a growing awareness of the need to minimize neonatal pain during painful procedures; therefore, guidelines have been issued for pre-venting or minimizing neonatal pain and its adverse consequences.2,4There is still a considerable gap between awareness and implementation of pain control methods to minimize neo-natal pain, however—a problem that seems to be worldwide.5,6
In this study, we compared 5 simple, common pain control methods by us-ing the “gold standard” behavioral method, the NFCS, along with accepted physiologic markers of pain and a more complex method of spectral analysis of HRV that reveals the state of the autonomic nervous system and
the sympathovagal balance during the noxious event.18This multidimensional assessment technique gave us the ability to compare various pain con-trol methods and various pain as-sessment methods concomitantly and to correlate the outcomes by an objective approach.
We noted less diminution in both HF and LF (a decrease that is commonly associated with acute painful stimuli in newborns)1,18in all treated groups as compared with the control group. This finding was greatest in the formula-fed and breastfed newborns. The autonomic tone as indicated by the LF-HF ratio significantly shifted toward the vagal arm in newborns who were breastfed or formula-fed as compared with the control group, in whom the autonomic system showed sympa-thetic activation commonly associated with acute pain reaction.19Thus, spec-tral analysis was of assistance in ob-jectively quantifying pain perception among the groups. Furthermore, the significant correlations that we found between the NFCS (the gold standard) and other physiologic and spectral markers suggest that spectral analysis may be used as an objective complemen-tary method to the NFCS in assessing pain in nonverbal, neurologically af-flicted, or intubated newborns. Spectral analysis has been previously applied to discriminate between healthy and
diseased individuals and to identify al-terations of normal physiologic pro-cesses; however, this method has been infrequently used for the assessment of pain in newborns. Although it may seem to be a complex approach to as-sisting clinical intuition, it has some in-valuable advantages, mainly the objec-tive representation that it confers to the autonomic nervous system state during painful procedures.
The most important finding that we no-ticed by using the various methods of analysis was that all of these simple and common pain control methods were better at relieving pain com-pared with no action taken at all. This finding encourages us to assert that it may be unethical to disregard these techniques during painful procedures in vulnerable newborns. Breastfeeding or bottle-feeding were found to be good pain relief methods. Neonatal pain prevention is the expectation of the parents and should be the goal of the medical staff; therefore, family members or staff may be recruited to help during these procedures, and nursing mothers should be encour-aged to breastfeed during the proce-dure. If family members believe that they cannot withstand the procedure, hear their infant crying, or see the heel-lancing, then bottle-feeding seems to be a good alternative.
REFERENCES
1. Oberlander TF, Grunau RE, Whitfield MF, Fitzgerald C, Pitfield S, Saul JP. Behavioral pain responses in former extremely low birth weight infants at four months’ cor-rected age.Pediatrics.2000;105(1). Avail-able at: www.pediatrics.org/cgi/content/ full/105/1/e6
2. Anand KJ; International Evidence-Based Group for Neonatal Pain. Consensus state-ment for the prevention and managestate-ment of pain in the newborn.Arch Pediatr Ado-lesc Med.2001;155(2):173–180
3. American Academy of Pediatrics Committee on Fetus and Newborn; American Academy of Pediatrics Section on Surgery; Canadian
Paediatric Society Fetus and Newborn Committee, Batton DG, Barrington KJ, Wallman C. Prevention and management of pain in the neonate: an update [published correction appears inPediatrics. 2007; 119(2):425]. Pediatrics. 2006;118(5): 2231–2241
4. Anand KJ. Clinical importance of pain and stress in preterm neonates.Biol Neonate.
1998;73(1):1–9
5. Gray PH, Trotter JA, Langbridge P, Doherty CV. Pain relief for neonates in Australian hospitals: a need to improve evidence-based practice.J Paediatr Child Health.
2006;42(1–2):10 –13
6. Lago P, Guadagni A, Merazzi D, et al. Pain management in the neonatal intensive care unit: a national survey in Italy. Paediatr Anaesth.2005;15(11):925–931
7. Craig KD, Whitfield MF, Grunau RV, Linton J, Hadjistavropoulos HD. Pain in the preterm neonate: behavioural and physiological indices.Pain.1993;52(3):287–299 8. Carbajal R, Chauvet X, Couderc S,
Olivier-Martin M. Randomized trial of analgesic effects of sucrose, glucose, and pacifiers in term neo-nates.BMJ.1999;319(7222):1393–1397 9. Carbajal R, Veerapen S, Couderc S, Jugie M,
Ville Y. Analgesic effect of breastfeeding in
10. Gray L, Watt L, Blass EM. Skin-to-skin contact is analgesic in healthy newborns.Pediatrics.
2000;105(1). Available at: www.pediatrics.org/ cgi/content/full/105/1/e14
11. Heart rate variability: standards of mea-surement, physiological interpretation, and clinical use. Task Force of the European So-ciety of Cardiology and the North American Society of Pacing and Electrophysiology.
Circulation.1996;93(5):1043–1065 12. Akselrod S, Gordon D, Ubel FA, Shannon DC,
Berger AC, Cohen RJ. Power spectrum anal-ysis of heart rate fluctuation: a quantitative
13. Grunau RV, Craig KD. Pain expression in neo-nates: facial action and cry.Pain.1987;28(3): 395– 410
14. Grunau RV, Johnston CC, Craig KD. Neonatal facial and cry responses to invasive and non-invasive procedures.Pain.1990;42(3): 295–305
15. Anand KJ, Scalzo FM. Can adverse neonatal experience alter brain development and subsequent behavior?Biol Neonate.2000; 77(2):69 – 82
16. Grunau RE, Oberlander TF, Whitfield MF, Fitzgerald C, Lee SK. Demographic and
thera-105–112
17. Hermann C, Hohmeister J, Demirakc¸a S, Zohsel K, Flor H. Long-term alteration of pain sensitivity in school-aged children with early pain experiences.Pain.2006;125(3): 278 –285
18. Lindh V, Wiklund U, Hakansson S. Heel lancing in term new-born infants: an evaluation of pain by frequency domain analysis of heart rate variability.Pain.1999;80(1–2):143–148 19. Carr DB, Goudas LC. Acute pain.Lancet.
DOI: 10.1542/peds.2009-0598 originally published online October 19, 2009;
2009;124;e921
Pediatrics
Amir Weissman, Michal Aranovitch, Shraga Blazer and Etan Z. Zimmer
Control Methods
Heel-Lancing in Newborns: Behavioral and Spectral Analysis Assessment of Pain
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/5/e921 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/5/e921#BIBL This article cites 17 articles, 6 of which you can access for free at:
Subspecialty Collections
edicine_sub
http://www.aappublications.org/cgi/collection/anesthesiology:pain_m
Anesthesiology/Pain Medicine
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2009-0598 originally published online October 19, 2009;
2009;124;e921
Pediatrics
Amir Weissman, Michal Aranovitch, Shraga Blazer and Etan Z. Zimmer
http://pediatrics.aappublications.org/content/124/5/e921
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.