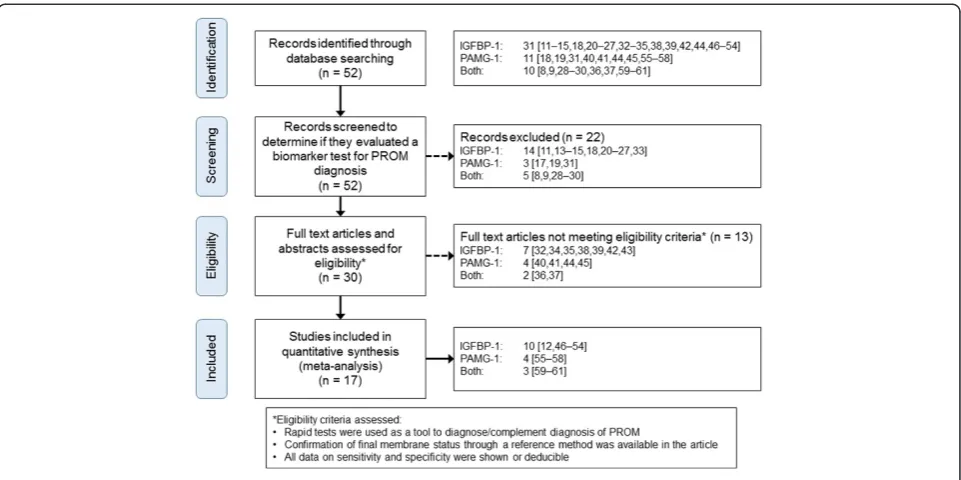
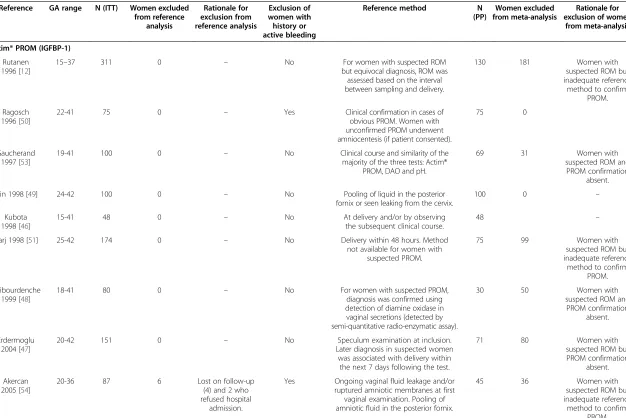
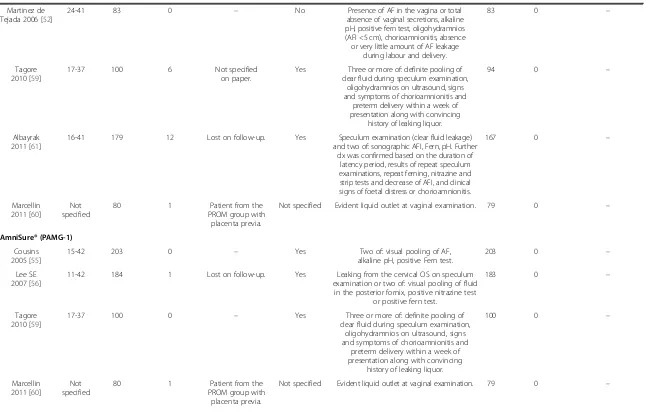
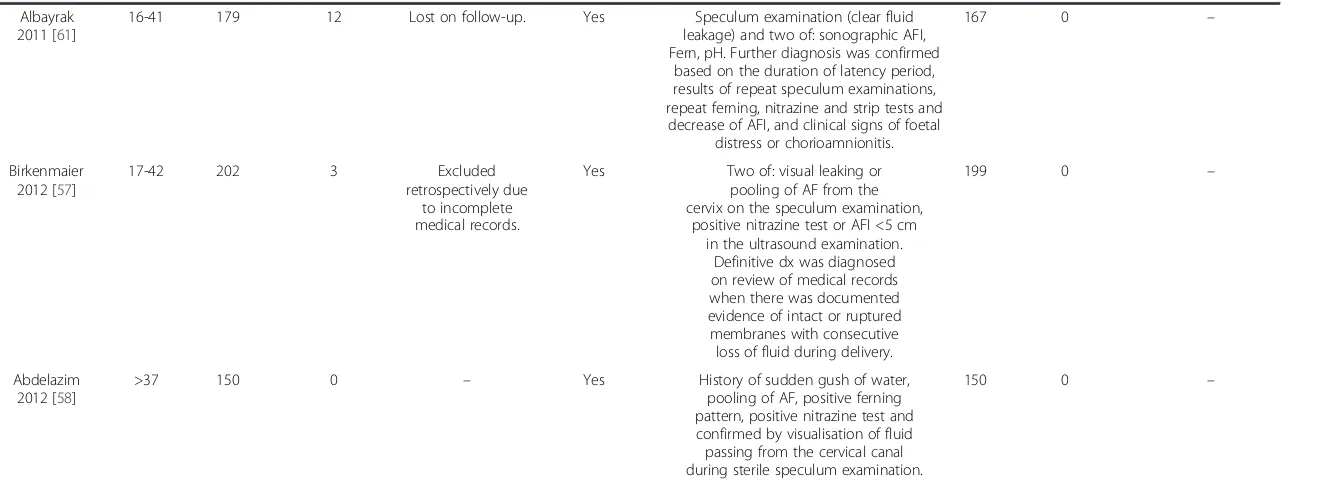
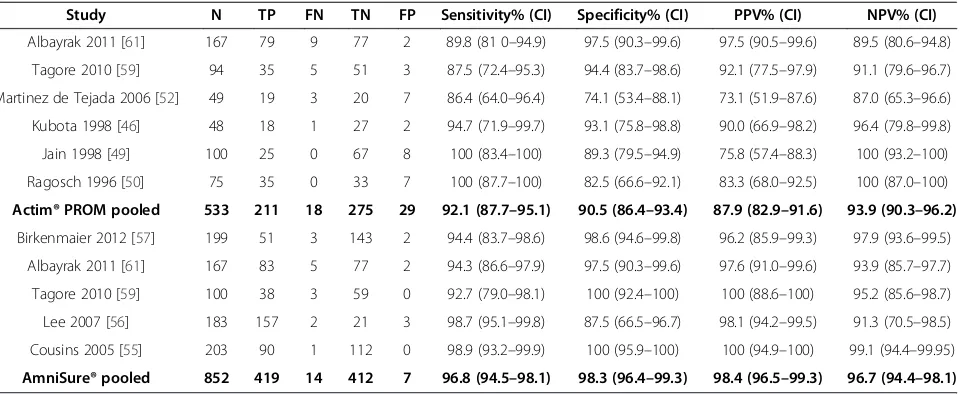
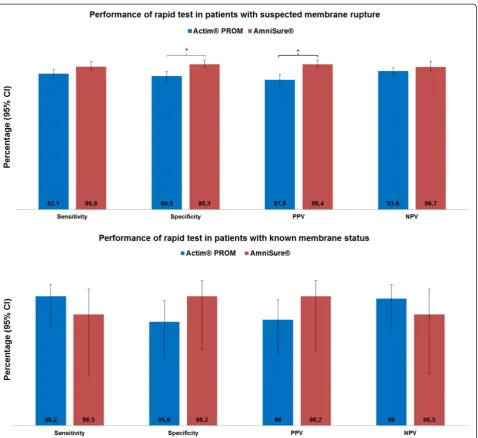
Meta analysis of studies on biochemical marker tests for the diagnosis of premature rupture of membranes: comparison of performance indexes
Full text
Figure

Related documents
Similar to the findings in our study, a study revealed that individual factors, such as health literacy and self-efficacy, have a great effect on improving the quality of life
Figure-5: Cell proliferation (%) of HeLa cancer cell line by Methylthiazolyldiphenyl-tetrazolium bromide (MTT) assay treated with standard Thymoquinone (TQ) and extracted TQ from
Firstly, the collected AFC data was preprocessed; Secondly, according to the main factors influencing passenger's route choice, the most possible routes were screened out; Then
High speed camera, velocity measurement moving target detection, interface differencing, shooting range
The algorithm based on subcarrier and each antenna signal is detected by hierarchical frequency domain equalization method until all signals on the antenna are
Moreover, relatively higher treatment expenditure was reported by the participants with education of matriculate and above, who spent around 17.89% of their monthly income on
A kind of obstacle avoidance strategy of intelligent vehicle global path planning based on particle swarm optimization is proposed to optimize path planning algorithm
Barnase; Molecular Dynamics Simulation; Salt Bridge; Hydrogen
