...
The European Journal of Public Health, Vol. 26, No. 6, 1017–1022
ß The Author 2016. Published by Oxford University Press on behalf of the European Public Health Association. All rights reserved. doi:10.1093/eurpub/ckw050 Advance Access published on 9 April 2016
...
Does social policy moderate the impact of
unemployment on health? A multilevel analysis
of 23 welfare states
Faraz Vahid Shahidi1, Arjumand Siddiqi1,2, Carles Muntaner1,3,4
1 Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, Canada 2 Gillings School of Global Public Health, University of North Carolina, Chapel Hill, NC, USA 3 Bloomberg School of Nursing, University of Toronto, Toronto, Ontario, Canada
4 Department of Public Health Sciences, Korea University, Seoul, South Korea
Correspondence:Faraz Vahid Shahidi, Dalla Lana School of Public Health, University of, Toronto, 155 College Street, Toronto, Ontario, Canada M5T 3M7, Tel: +1 905 484 0570, Fax: +1 416 978 1883, e-mail: [email protected]
Background: The magnitude of observable health inequalities between the unemployed and their employed counterparts differs considerably across countries. Few attempts have been made to test theoretical explanations for this cross-national variation. Moreover, existing studies suffer from important theoretical and methodological limitations. This study addresses these limitations and investigates whether differences in the generosity of social protection policies and in public attitudes towards those policies explain why unemployment-related health inequalities are steeper in some societies than in others. Methods: Multilevel logistic modelling was used to link contextual-level variables on social protection policies and public attitudes in 23 European countries to individual-level data on self-rated health from the 2012 wave of the European Social Survey. Results: The magnitude of inequalities in self-rated health between the unemployed and their employed counterparts varies significantly across countries as a function of cross-national differences in the level of social protection awarded to the unemployed and the level of public support for the welfare state.Conclusions:The results provide empirical support for the claim that governments can play a more active role in mitigating unemployment-related health inequalities by expanding the generosity and scope of social protection policies. Whether such an expansion of social protection will take place in the current climate of fiscal austerity is a political question whose implications merit the attention of population health scholars.
...
Introduction
H
ealth inequalities between the unemployed and their employed counterparts have been observed across the landscape of advanced capitalist countries.1However, the magnitude of these un-employment-related health inequalities differs considerably across countries.2 Although sophisticated theoretical frameworks exist with which to explain this cross-national diversity,3,4few attemptshave been made to test their proposed explanations.5,6Moreover, existing studies suffer from important theoretical and methodo-logical limitations. The present study addresses these limitations and conducts a multilevel analysis across 23 European countries to determine whether cross-national differences in the magnitude of unemployment-related health inequalities can be explained by dif-ferences in the generosity of social protection policies and in public attitudes towards those policies.
Unemployment and health
Population health researchers have long been interested in the rela-tionship between unemployment and health.7–9 Much of this interest is attributable to the role of unemployment as a fundamental determinant of health: one that influences multiple pathways—both material and psychosocial—that lead to multiple sources of morbidity and morality.7,10,11Materialist explanations, whose theor-etical underpinnings are rooted in classical sociological accounts of economic deprivation, argue that the loss of earnings associated with unemployment deteriorates the socioeconomic position of unemployed persons and, by extension, undermines their ability to secure the material pre-requisites for health.12,13 Psychosocial
accounts of the association between unemployment and health argue that unemployment strips individuals of a principal mechanism through which status and esteem are defined and perceived.14–16 Those who experience unemployment are said to suffer from status-related anxieties attributable to their relative position in the social hierarchy that are not conducive to good health.17 Given that employment constitutes a central means through which individuals meet both the material and the psycho-social demands characteristic of life in capitalist societies, there is a strong case to be made that unemployment incurs both material and psychosocial disadvantages to the individual.18
While the materialist and psychosocial approaches shed important light on the micro-level pathways that link unemployment to poor health outcomes, there is also a need to understand the macro-level (e.g. national) contexts that condition these pathways.19 These macro-level contexts may play an important role in modifying these pathways and, by extension, in explaining differences in the magnitude of unemployment-related health inequalities that are observed across those contexts.
Explaining cross-national differences
Although social inequalities in health have been observed in all societies, they are noticeably steeper in some societies than in others.20 Several theoretical frameworks have been proposed to explain this cross-national variation.2–4,21–25Research on the associ-ation between unemployment and health has largely neglected these theoretical accounts.5Indeed, few empirical studies have awarded explicit empirical attention to the effect on this association of the
national context in which unemployment occurs. There are two notable exceptions.
McLeodet al.2have highlighted differences in the configuration of social and labour market institutions as important sources of cross-national variation in the health-related consequences of unemploy-ment. Comparing the USA and Germany, the authors argue that unemployment-related health inequalities are smaller in Germany due to the country’s more encompassing social and labour market institutions. To the extent that they limit their analysis to two countries, however, their study is significantly constrained with respect to its explanatory capacity. Our study overcomes this limitation by conducting an analysis on a larger sample of 23 countries.
Drawing from the literature on welfare regime typologies,26–28 Bambra and Eikemo1 similarly assess whether unemployment-related health inequalities vary systematically across these countries as a function of the qualitative orientation of their respective welfare states. In contrast to their expectations, however, the authors find that unemployment-related health inequalities are not smallest in the generous welfare states of Scandinavia, but rather in the rudimentary welfare states of Southern Europe. Despite the counterintuitive nature of these findings, they are concordant with prior analyses, which tend to conclude that health inequalities are not consistently smallest in Scandinavian countries.28
A number of potential explanations have been offered to explain this paradox.28 Welfare regime typologies developed in previous decades may not account for significant social policy changes that have taken place over time. Regime typologies also neglect important differences across policy areas. For example, Bambra and Eikemo1
rely on a regime typology whose generosity scores reflect three different dimensions of state intervention: unemployment benefits, sickness insurance and pensions. However, countries characterized by high overall generosity scores may not necessarily score high in the area of unemployment benefits. This is the case for most Scandinavian countries.29The apparent disjuncture between the the-oretical ‘black box’ of welfare regime typologies and empirical findings on health inequalities suggests that studies should use more sensitive measures of welfare state generosity. For this reason, our analysis adopts an institutional approach to comparative welfare state research that is better suited to the task of capturing the programmatic characteristics of specific social protection policies. In demonstrating the advantages associated with an institutional approach, our study contributes to ongoing discussions about how best to operationalize differences in welfare state policies for com-parative analyses of health outcomes.30,31
While population health researchers have increasingly turned to the welfare state as a useful lens through which to explain cross-national differences in health inequalities, the existing literature has thus far neglected to consider theories that assign explanatory significance to attitudinal contexts. Public attitudes towards the welfare state may nevertheless play an important role in explaining those cross-national differences by conditioning the psychosocial experience of unemployment and shaping the generosity of social protection policies.16,32
Building on existing theoretical frameworks,3,4this study takes as
its point of departure the claim that the magnitude of unemploy-ment-related health inequalities within a given society is linked to the generosity of welfare state policies as well as the attitudinal contexts in which those inequalities manifest. Our analysis tests two hypotheses in particular.
Hypothesis 1: unemployment-related health inequalities will be smaller in countries that award more generous levels of social protection to the unemployed.
Hypothesis 2: unemployment-related health inequalities will be smaller in countries characterized by more favourable public attitudes towards the welfare state.
Methods
Data
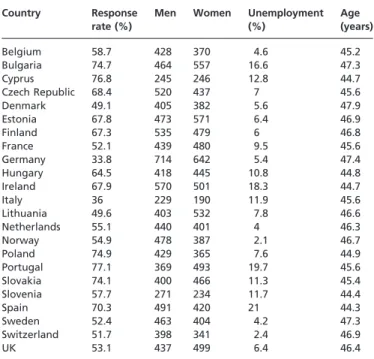
Individual-level data were retrieved from the 2012 wave of the European Social Survey. A sample of 22 123 observations for indi-viduals aged 25–65 years were collected from 23 countries: Belgium, Bulgaria, Cyprus, the Czech Republic, Denmark, Estonia, Finland, France, Germany, Hungary, Ireland, Italy, Lithuania, the Netherlands, Norway, Poland, Portugal, Slovakia, Slovenia, Spain, Sweden, Switzerland and UK. Table 1 describes the key characteris-tics of the study sample.
Individual-level variables
The principal individual-level variables included in the analysis were self-rated health and unemployment status. Self-rated health was measured using a single five-category item asking people to rate their overall health. The item was dichotomized due to a limited number of responses for some scale categories. We distinguish between ‘good’ self-rated health (good or very good) and ‘poor’ self-rated health (fair, bad or very bad). Unemployment status was measured using a series of questions asking respondents about their main activity during the previous seven days. The association between unemployment and health was measured by comparing the unemployed who are actively seeking work to people in paid work. Individuals who identify as permanently sick, disabled, retired, involved in community or military service, enrolled in school, engaged in unpaid domestic labour or unemployed but not actively seeking work were excluded from the analysis. Age, gender and years of education were included in the analysis as individual-level controls. We tested for non-linear relationships with age and education and determined the linear terms to be adequate fits. Individual-level variables were centred around their respective means in order to facilitate the interpretation of interaction terms in the analysis. A design weight was included to correct for sampling biases resulting from the fact that some countries included in the survey were not able to give all individuals the same probability of selection.
Table 1 Descriptive characteristics of the study sample
Country Response rate (%)
Men Women Unemployment (%)
Age (years)
Belgium 58.7 428 370 4.6 45.2
Bulgaria 74.7 464 557 16.6 47.3
Cyprus 76.8 245 246 12.8 44.7
Czech Republic 68.4 520 437 7 45.6
Denmark 49.1 405 382 5.6 47.9
Estonia 67.8 473 571 6.4 46.9
Finland 67.3 535 479 6 46.8
France 52.1 439 480 9.5 45.6
Germany 33.8 714 642 5.4 47.4
Hungary 64.5 418 445 10.8 44.8
Ireland 67.9 570 501 18.3 44.7
Italy 36 229 190 11.9 45.6
Lithuania 49.6 403 532 7.8 46.6
Netherlands 55.1 440 401 4 46.3
Norway 54.9 478 387 2.1 46.7
Poland 74.9 429 365 7.6 44.9
Portugal 77.1 369 493 19.7 45.6
Slovakia 74.1 400 466 11.3 45.4
Slovenia 57.7 271 234 11.7 44.4
Spain 70.3 491 420 21 44.3
Sweden 52.4 463 404 4.2 47.3
Switzerland 51.7 398 341 2.4 46.9
UK 53.1 437 499 6.4 46.4
Contextual-level variables
The principal contextual-level variables included in the analysis were the generosity of social protection awarded to the unemployed (Hypothesis 1) and the extent of public support for the welfare state (Hypothesis 2). The level of social protection awarded to the unemployed was operationalized using national unemployment insurance replacement rates, which reflect the generosity of benefit payments as a percentage of one’s previous income. Data on un-employment insurance replacement rates were retrieved from the ‘Comparative Welfare Entitlements Dataset 2’.33Due to restrictions in the availability of data, replacement rates are for the year 2010. Public support for the welfare state was measured using two items available in the 2012 wave of the European Social Survey. These items asked respondents to agree or disagree with the statements: ‘how important do you think it is for democracy in general that the government takes measures to reduce differences in income levels?’ and ‘how important do you think it is for democracy in general that the government protects all citizens from poverty?’ Possible answers ranged on a scale from 0 to 10, representing ‘not at all important for democracy in general’ and ‘extremely important for democracy in general’, respectively. Responses to these two survey items were averaged and aggregated by country in order to construct a cross-national index of public support for the welfare state. Table 2 lists values for these contextual-level variables. Gross domestic product per capita and the unemployment rate were included in the analysis as contextual-level controls.
Analysis
The relative odds of reporting poor self-rated health were calculated by applying a series of logistic regression analyses disaggregated by country. Multilevel interactions between individual-level and contextual-level variables were analyzed through a series of six analytic stages. In stage one, a one-way analysis of variance was used to examine whether there were overall differences in self-reported health across countries. In stage two, a cross-over effects
model was used to assess the association between the contextual-level variables and overall contextual-levels of self-reported health across countries. In stage three, a random coefficients model was used to test whether random variation is observed in the country-specific associations between unemployment and self-rated health. In stages four and five, multilevel models were operated to visualize potential interactions between unemployment and the contextual-level variables, individually. In the sixth and final step, a full multilevel model was run that included both of the contextual-level variables. Three-way interactions with gender were included in the latter stages of the analysis to account for the possibility that the contextual effects we are attempting to capture do not impact men and women in the same way.
Results
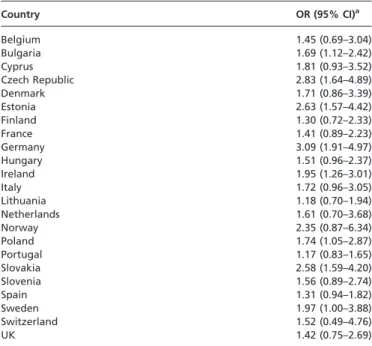
Country-level associations between unemployment and poor self-rated health are listed in table 3. While unemployment-related health inequalities are found in all 23 countries, considerable cross-national variation can be observed in the magnitude of those inequalities. Sensitivity analysis was performed using linear regression to account for the non-collapsibility of ORs. Similar patterns of cross-national variation were observed. The results are available upon request.
Results from the multilevel modelling are presented in table 4. Model 1 depicts the one-way analysis of variance. The significance of the random intercept estimate suggests that there is a random variance in self-rated health across countries to be explained. In Model 2, we test whether this random variance can be explained by way of the contextual-level variables. A small but significant as-sociation is observed between our control variable for gross domestic product per capita and overall variation in self-reported health across countries. No other significant associations are observed.
Model 3 estimates a random coefficients model. The results of this model indicate that unemployment, age and gender are associated with an increase in the odds of reporting poor heath, while years of education completed is associated with a decrease in the odds. As expected, the random variance for unemployment is also significant, indicating that the association between unemployment and health
Table 2 Contextual-level variables
Country Unemployment
insurance replacement rate (%)
Index of public support for the welfare state
Belgium 67 8.2
Bulgaria 76 9.1
Cyprus 54 9.2
Czech Republic 38 7.6
Denmark 56 7.7
Estonia 50 8.3
Finland 57 8.2
France 71 8.4
Germany 60 8.3
Hungary 51 8.7
Ireland 39 8
Italy 55 9.1
Lithuania 47 8.1
Netherlands 83 7.6
Norway 67 8.1
Poland 26 8.8
Portugal 78 8.8
Slovakia 63 7.9
Slovenia 70 9.1
Spain 80 9.1
Sweden 62 8.4
Switzerland 73 8.1
UK 49 8.0
Net replacement rates for Cyprus and UK are from the Organisation for Economic Co-operation and Development (OECD). Net replace-ment for Cyprus if from the year 2007.
Table 3 Odds of reporting poor self-rated health among the unemployed compared with the employed
Country OR (95% CI)a
Belgium 1.45 (0.69–3.04)
Bulgaria 1.69 (1.12–2.42)
Cyprus 1.81 (0.93–3.52)
Czech Republic 2.83 (1.64–4.89)
Denmark 1.71 (0.86–3.39)
Estonia 2.63 (1.57–4.42)
Finland 1.30 (0.72–2.33)
France 1.41 (0.89–2.23)
Germany 3.09 (1.91–4.97)
Hungary 1.51 (0.96–2.37)
Ireland 1.95 (1.26–3.01)
Italy 1.72 (0.96–3.05)
Lithuania 1.18 (0.70–1.94)
Netherlands 1.61 (0.70–3.68)
Norway 2.35 (0.87–6.34)
Poland 1.74 (1.05–2.87)
Portugal 1.17 (0.83–1.65)
Slovakia 2.58 (1.59–4.20)
Slovenia 1.56 (0.89–2.74)
Spain 1.31 (0.94–1.82)
Sweden 1.97 (1.00–3.88)
Switzerland 1.52 (0.49–4.76)
UK 1.42 (0.75–2.69)
a: Adjusted for age, gender and education.
varies across national contexts. The three remaining models attempt to explain this cross-national variation.
To test the first hypothesis, Model 4 includes an interaction term between the unemployment variable and the level of social protection awarded to the unemployed. To test the second hypothesis, Model 5 includes an interaction term between the un-employment variable and the extent of public support for the welfare state. Both interaction terms are significant, indicating that the magnitude of unemployment-related health inequalities varies cross-nationally as a function of these contextual factors. The direction of these interaction terms suggests that the odds of reporting poor health among the unemployed are smaller in countries characterized by more generous levels of social protection for the unemployed and more favourable public attitudes towards the welfare state. The three-way interactions with gender were not significant. They are not included in table 4 but available upon request.
Model 6 represents a full multilevel analysis that includes both sets of interaction terms. In this combined model, the interaction term between the generosity of social protection and unemployment is no longer significant. This would seem to suggest that a significant portion of the contextual impact of social protection policies on the unemployment–health relationship is mediated through the reciprocal relationship that these policies share with public attitudes towards the welfare state.
Discussion
There are several limitations to the analysis. First, while the European Social Survey provides rigorous comparative data, the criteria by which individuals rate their own health may differ across national contexts.34 Second, the analysis does not offer an
assessment of all the contextual factors that may potentially be shaping cross-national differences in the magnitude of unemploy-ment-related health inequalities. Third, recent contributions in the welfare state literature on the dualisation of the welfare state have demonstrated that the experience of social protection varies not only across national contexts but also between individuals situated within the same national context.35Our use of a national measure of social protection neglects this important dimension of within-country variation. Fourth, social protection policies have an impact on whether non-employed persons are actively seeking work or, alter-natively, choose to be economically inactive.36The presence of
cross-national variation in social protection policies may therefore have
biased our study sample by giving rise to undesirable selection effects. Our results have likely been influenced by such selection effects although the direction of the bias is unclear. Finally, by attributing a single fixed-effect for education to all countries, our results have not adjusted for the potential confounding effect of cross-national variation in the relationship between education and health .
The results of our analysis suggest that differences in the level of social protection awarded to the unemployed and in public attitudes towards the welfare state help to explain why unemployment-related health inequalities are steeper in some societies than in others. In particular, we have found that more generous levels of social protection and more favourable public attitudes towards the welfare state are associated with narrower inequalities in self-reported health between the unemployed and the employed.
On a first account, our results suggest that institutionalized mechanisms of income maintenance provide a protective buffer against the adverse health-related consequences of unemployment. This is in line with previous research, which has shown that welfare state policies play an important role in maintaining the health of individuals exposed to unemployment and other socioeconomic dis-locations.13,37This study builds on these individual-level findings and indicates that, at the cross-national level, unemployment-related health inequalities are narrower in countries characterized by greater levels of social protection for the unemployed. Notably, policies in support of the unemployed are not randomly distributed across societies. On the contrary, they exhibit distinctly political patterns of development over time and across space.26Scholarship on the unemployment–health relationship must therefore account for social protection policies and for the political forces shaping them if this body of research is to provide a comprehensive explan-ation for that relexplan-ationship.38
On a second account, the results of our analysis indicate that the psychosocial context in which unemployment occurs conditions its relationship with health. We have found that the adverse health-related consequences of unemployment are less severe in countries where there is greater public support for the welfare state and, by extension, for those who depend on it (e.g. the unemployed). Theoretically, we suggest that the stigma attributable to the experience of unemployment is reduced in environments characterized by greater levels of public support for the welfare state. The adverse psychosocial implications of unemployment for individual-level perceptions of status and esteem are likely to be attenuated in these environments.18To our knowledge, this is the Table 4 Multilevel logistic regression of poor self-rated health in 23 European welfare states
Model 1 Model 2 Model 3 Model 4 Model 5 Model 6
OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)
Fixed effects
Unemployment 1.76(1.53–2.03) 1.73(1.53–1.97) 1.80(1.59–2.04) 1.79(1.59–2.02)
Education 0.94
(0.93–0.95) 0.94
(0.93–0.95) 0.94
(0.93–0.95) 0.94
(0.93–0.95)
Age 1.05(1.04–1.05) 1.05(1.04–1.05) 1.05(1.04–1.05) 1.05(1.04–1.05)
Gender 1.25
(1.18–1.34) 1.26
(1.18–1.34) 1.26
(1.18–1.34) 1.26
(1.18–1.34)
Unemployment rate 1.00 (0.96–1.05) 1.00 (0.95–1.05) 1.00 (0.95–1.06) 1.00 (0.95–1.06)
GDP Per capita 0.99
(0.98–1.00) 0.99
(0.98–1.00) 0.99
(0.98–1.00) 0.99
(0.98–1.00)
RRa 1.03 (0.91–1.17) 1.03 (0.91–1.18) 1.03 (0.91–1.18)
PA 1.07 (0.72–1.60) 1.09 (0.717–1.66) 1.08 (0.70–1.67)
Unemployment
RRa 0.93
(0.90–0.97) 0.96 (0.92–1.01)
UnemploymentPA 0.76(0.67–0.86) 0.80(0.70–0.91)
Random effects
Intercept 0.23(0.07) 0.13(0.04) 0.26(0.08) 0.16(0.05) 0.15(0.05) 0.16(0.05)
Unemployment 0.04
(0.02) 0.02 (0.02) 0.02 (0.02) 0.01 (0.02)
Covariance 0.02 (0.04) 0.00 (0.03) 0.00 (0.03) 0.00 (0.03)
RR = replacement rate, PA = public attitudes.
P< 0.05,
P< 0.01,
P< 0.001.
a: ORs are estimated for a 10% increase in the replacement rate.
first study to provide evidence of a relationship between public attitudes towards the welfare state and population health outcomes. Our findings also suggest that the welfare state and attitudinal characteristics of national contexts do not operate independently from one another. There appears to be a reciprocal relationship between the generosity of social protection policies and the public support for those policies. In contexts where the unemployed are awarded greater levels of social protection, public attitudes towards the welfare state appear to be more favourable. Our results, therefore, suggest that there is a need for the social health sciences to pay greater attention to the complex interactions linking policies and public attitudes.32
Our study adds to a growing body of literature encouraging a shift in the focus of social epidemiological research away from problem description and towards the identification of actionable policy inter-ventions that have the potential to promote the health of popula-tions.39 Through the application of an institutional approach to comparative welfare state research, we have generated evidence in favor of the salutary effects of social protection policies and public attitudes for the adverse health-related consequences of unemploy-ment. These results provide empirical support for the broader claim that governments can play a more active role in mitigating unemployment-related health inequalities by expanding the generosity and the scope of unemployment protection policies. In an era of heightened unemployment, it is significant that the gov-ernments of advanced capitalist economies have thus far proven unwilling to expand their welfare states, choosing instead to subscribe to an increasingly entrenched politics of fiscal austerity.40 Whether an expansion of social protection will take place in this climate of austerity remains a political question whose implications merit the attention of population health scholars.
Funding
This work was funded by the Lupina Foundation and the Comparative Program on Health and Society at the University of Toronto.
Conflicts of interest: None declared.
Key points
The magnitude of unemployment-related health inequalities between the unemployed and their employed counterparts varies across countries.
Few attempts have been made to explain this cross-national variation and existing studies suffer from important theor-etical and methodological limitations.
The results of the study suggest that social protection policies and public attitudes towards the welfare state moderate the impact of unemployment on health.
The study demonstrates the advantages associated with an institutional, as opposed to typological, measure of welfare state generosity.
The study is the first to provide evidence of an association between public attitudes towards the welfare state and population health outcomes.
References
1 Bambra C, Eikemo TA. Welfare stare regimes, unemployment and health: a com-parative study of the relationship between unemployment and self-reported health in 23 European countries.J Epidemiol Community Health2009;63:92–8.
2 McLeod C, Hall PA, Siddiqi A, et al. How society shapes the health gradient: work-related health inequalities in a comparative perspective.Ann Rev Public Health
2012;33:59–73.
3 Muntaner C, Chung H, Solar O, et al. A macro-level model of employment relations and health inequalities.Int J Health Services2010;40:215–21.
4 Hall PA, Lamont M. editors.Successful Societies: How Institutions and Culture Affect Health. Cambridge: Cambridge University Press, 2009.
5 Hammarstro¨m A, Janlert U. An agenda for unemployment research: a challenge for public health.Int J Health Services2005;35:765–77.
6 Be´land F, Birch S, Stoddart G. Unemployment and health: contextual-level influences on the production of health in populations.Soc Sci Med2002;55:2033–52.
7 Bartley M. Unemployment and ill health: understanding the relationship.
J Epidemiol Community Health1994;48:333–7.
8 Bartley M, Ferrie J, Montgomery SM. Health and labour market disadvantage: unemployment, non-employment and job insecurity. In: Marmot M, Wilkinson RG, editors.Social Determinants of Health. Oxford: Oxford University Press, 2006: 78–96.
9 Dooley D, Fielding J, Levi L. Health and unemployment.Ann Rev Public Health
1996;17:449–65.
10 Janlert U, Hammarstro¨m A. Which theory is best? Explanatory models of the association between unemployment and health. BMC Public Health
2009;9:235–43.
11 Muntaner C, Solar O, Vanroelen C, et al. Unemployment, informal work, precarious employment, child labour, slavery, and health inequalities: pathways and mechanisms.Int J Health Services2010;40:281–95.
12 Price RH, Choi JN, Vinokur AD. Links in the chain of adversity following job loss: how financial strain and loss of personal control lead to depression, impaired functioning, and poor health.J Occup Health Psychol2002;7:302–12.
13 Rodriguez E. Keeping the unemployed healthy: the effect of means-tested and en-titlement benefits in Britain, Germany, and the United States.Am J Public Health
2001;91:1403–11.
14 Jahoda M. Work, employment, and unemployment: values, theories, and approaches in social research.Am Psychologist1981;36:184–91.
15 Fergusson DM, Horwood LJ, Woodward LJ. Unemployment and psychosocial adjustment in young adults: causation or selection?Soc Sci Med2001;53:305–20.
16 Gallie D, Marsh C, Vogler C.Social Change and the Experience of Unemployment. Oxford: Oxford University Press, 1994.
17 Starrin B, Aslund C, Nilsson KW. Financial stress, shaming experiences and psychosocial ill-health: studies into the finances-shame model.Soc Indic Res
2009;91:283–98.
18 Nordenmark M, Strandh M. Towards a sociological understanding of mental well-being among the unemployed: the role of economic and psychosocial factors.
Sociology1999;33:577–97.
19 Muntaner C. Social capital, social class, and the slow progress of psychosocial epidemiology.Int J Epidemiol2004;33:674–80.
20 Mackenbach J, Stirbu I, Roskam AR, et al. Socioeconomic inequalities in health in 22 European countries.N Engl J Med2008;358:2468–81.
21 Hall PA, Lamont M. Why social relations matter for politics and successful societies.
Ann Rev Polit Sci2013;16:49–71.
22 Lundberg O, Yngwe MA, Stja¨rne MK, et al. The role of welfare state principles and generosity in social policy programmes for public health: an international comparative study.Lancet2008;372:1633–40.
23 Chung H, Muntaner C. Welfare state matters: a typological multilevel analysis of wealthy countries.Health Policy2007;80:328–39.
24 Eikemo TA, Bambra C, Judge K, et al. Welfare state regimes and differences in self-perceived health in Europe: a multilevel analysis.Soc Sci Med
2008;66:2281–95.
25 Navarro V, Muntaner C, Borrell C, et al. Politics and health outcomes.Lancet
2006;368:1033–7.
26 Esping-Andersen G.The Three Worlds of Welfare Capitalism. Princeton, NJ: Princeton University Press, 1990.
27 Ferragina E, Seeleib-Kaiser M. Welfare regime debate: past, present, futures?Policy Politics2011;39:583–611.
28 Dahl E, Fritzell J, Lahelma E, et al. Welfare state regimes and health inequalities. In: Siegrist J, Marmot M, editors.Social Inequalities in Health: New Evidence and Policy Implications. Oxford: Oxford University Press, 2006: 193–222.
29 Scruggs L, Allan J. Welfare-state decommodification in 18 OECD countries: a replication and revision.J Eur Soc Policy2006;16:55–72.
30 Bergqvist K, Yngwe MA, Lundberg O. Understanding the role of welfare state characteristics for health and inequalities – an analytical review.BMC Public Health
2013;13:1234.
31 Ferrarini T, Nelson K, Sjo¨berg O. Decomposing the effect of social policies on population health and inequalities: an empirical example of unemployment benefits.
Scand J Public Health2014;42:635–42.
32 Larsen CA. The institutional logic of welfare attitudes: how welfare regimes influence public support.Comp Polit Stud2008;41:145–68.
33 Scruggs L, Jahn D, Kuitto K.Comparative Welfare Entitlements Dataset 2. Version 2014-3. University of Connecticut and University of Greifswald, 2014.
34 Jylha¨ M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model.Soc Sci Med2009;69:307–16.
35 Emmenegger P, Ha¨usermann S, Palier B, et al.The Age of Dualization: The Changing Face of Inequality in Deindustrializing Societies. Oxford: Oxford University Press, 2012.
36 Erlinghagen M, Knuth M. Unemployment as an institutional construct? Structural differences in non-employment between selected European countries and the United States.J Soc Policy2010;39:71–94.
37 O’Campo P, Molnar A, Ng E, et al. Social welfare matters: a realist review of when, how, and why unemployment insurance impacts poverty and health.Soc Sci Med
2015;132:88–94.
38 Muntaner C, Borrell C, Ng E, et al. Politics, welfare regimes, and population health: controversies and evidence.Sociol Health Illness2011;33:946–64.
39 O’Campo P, Dunn J.Rethinking Social Epidemiology: Towards a Science of Change. New York, NY: Springer Publishing, 2012.
40 Karanikolos M, Mladovsky P, Cylus J, et al. Financial crisis, austerity, and health in Europe.Lancet2013;381:1323–31.
...
The European Journal of Public Health, Vol. 26, No. 6, 1022–1027
ß The Author 2016. Published by Oxford University Press on behalf of the European Public Health Association. All rights reserved. doi:10.1093/eurpub/ckw072 Advance Access published on 3 June 2016
...
Occupational, social and medical characteristics of early
prenatal leave in France
Sole`ne Vigoureux1, Be´atrice Blondel1, Virginie Ringa2,3, Marie-Jose`phe Saurel-Cubizolles1
1 INSERM UMR 1153, Obstetrical, Perinatal and Pediatric Epidemiology Research Team (EPOPe´), Center for Epidemiology and Statistics Sorbonne Paris Cite´, DHU Risks in Pregnancy, Paris Descartes University, 75014 Paris, France
2 INSERM UMR 1018, CESP Centre for Research in Epidemiology and Population Health, Gender, Sexuality and Health Team, Universite´ Paris-Saclay, Univ. Paris-Sud, UVSQ, Kremlin-Biceˆtre F-94276, France
3 Institut National d’Etudes De´mographiques (INED), F-75020 Paris, France
Correspondence:Sole`ne Vigoureux, INSERM U1153-EPOPe´, Hoˆpital Tenon Baˆtiment Recherche, 4 rue de la Chine, 75020 Paris, France, Tel: 33 1 56 01 83 70, Fax: 33 1 43 26 89 79; e-mail: [email protected]
Background:In France, most women of childbearing age work. The prenatal leave law in France protects women during pregnancy and their employment. We aimed to describe how long before delivery women stopped working and analyse the association between occupational, social and medical factors and early prenatal leave (before 24 weeks’ gestation).Methods:The sample was extracted from the 2010 French National Perinatal Survey. Women were interviewed in French maternity units during a 1-week period. We focused on all women with a singleton live birth who were working during pregnancy (n= 10 149). Women were interviewed between delivery and discharge to collect information on employment, date of leave, sociodemographic and medical characteristics. Results: Among women who worked during pregnancy, 27.5% reported early occupational leave (before 24 weeks’ gestation). Early occupational leave was more frequent among women with unstable jobs (fixed-term vs. non–fixed-term contract: adjusted odds ratio aOR = 1.60 [95% confidence interval 1.40–1.84]) and with less-qualified occupational categories (manual workers vs. managers and upper-intellectual positions: aOR = 2.96 [2.30–3.82]), even after adjusting for sociodemographic and other employment characteristics. Women with a pathological or at risk pregnancy left work earlier than other women. After stratification on type of pregnancy there was still a higher rate of early leave for women with less qualified occupational group.Conclusion:In France, social vulnerability of pregnant women, linked to low sociodemographic situation or low occupational categories, is associated with early leave during pregnancy, even after stratification on type of pregnancy.
...
Introduction
I
n France, most women of childbearing age work. The average age of mothers having a first child is about 28 years; the fertility rate is among the highest in Europe: two children per woman in 2014.1The Perinatal French Surveys have shown a steadily increasing rate of occupational activity of women during pregnancy, from 53% in 19722to 66% in 2003.3The first laws protecting women during pregnancy were imple-mented at the beginning of the 20th century from data showing that women without rest at the end of pregnancy were at increased risk of low birthweight babies. The French law was elaborated to protect women during pregnancy and their expected children and to protect
women in employment.4 Women cannot be dismissed on the grounds of a pregnancy, and the employer should adjust the schedule and the conditions of the job during the pregnancy. The timing of prenatal leave has been stable since 1975: women stop working at 35 weeks’ gestation (WG; i.e. 6 weeks before the due date of delivery) for a first or second child and at 33 WG (8 weeks before the due date) for the third or additional child. Since 1978, the duration of postnatal leave that is compensated has been 10 weeks (first or second child) or 18 weeks (third or additional child) to 22 weeks (multiple pregnancy). A 2-week additional leave for pathological pregnancy, on medical prescription is compensated totally and may be taken at any time during the pregnancy. Since