61 |
P a g e
Asian Journal of Pharmaceutical Science & Technology
e-ISSN: 2248 – 9185
www.ajpst.com
Print ISSN: 2248 – 9177
OPIOID RECEPTORS: AN OVERVIEW
Priyanka P. Pawar*
1, Kundan J. Tiwari
2, Supriya T. Garud
2, Manjula T. Ruparel
21S.M.B.T. College of Pharmacy, Nandi-hills Dhamangaon, Nashik, India. 2
S.M.B.T. Institute of D Pharmacy, Nandi-hills Dhamangaon, Nashik, India.
ABSTRACT
Opioid drugs play important roles in the clinical management of pain were Opioid receptors have been targeted for the treatment of pain. Opioid receptors are widely involve in various physiological and pathophysiological activities, including the regulation of membrane ionic homeostasis, cell proliferation, emotional response, epileptic seizures, immune function, feeding, obesity, respiratory and cardiovascular control as well as some neurodegenerative disorders. The opioid receptors involved in the spinal action of enkephalin for production and/or modulation of analgesia. The two approaches were used as supraspinal and spinal sites. The mu (µ), kappa(k), delta(δ), opioid receptors represent the originally classified receptor subtypes with opioid receptor like -1 (ORL) being the least characterized. All four receptors are protein coupled receptor and activate inhibitory G-proteins.
Key words: Receptor, Pain, Epilepsy, Seizures, Supraspinal.
INTRODUCTION
Receptors are proteins which are, by far, the most important drug targets in medicine. They are implicated in ailment such as pain, depression, Parkinson diseases. Receptors identified by specific neurotransmitter or by hormone which activates them. Thus receptor activated by dopamine is called as dopaminergic receptors, the receptor activated by acetylcholine is called as cholinergic receptor, and receptor activated by adrenergic receptor is called as adrenaline receptor [1].
Morphine and other opioids exert their actions by interacting with specific receptors present on neurons in the CNS and in peripheral tissues. Chemical modification of morphine structure has yielded a number of compounds which have a complex pattern of morphine-like and other agonistic and antagonistic actions that cannot be explained on the basis of a single opioid receptor. Radioligand binding studies have divided the opioid receptors into three types (μ, k, δ); which have been cloned. Each has a specific pharmacological profile and pattern of anatomical distribution in the brain, spinal cord and peripheral tissues [1-3].
The following term are used in describing drug receptor interaction:
Agonist – An agent who activates a receptor to produce an effect similar to that of physiological signal molecules. Inverse agonist – An agent who activates a receptor to produce an effect in the opposite direction to that of the
agonist. Partial agonist –An agent which activates a receptor to produced submaximal effect but antagonizes the action of full agonist.
Antagonist – An agent which prevents the action of an agent on receptor or the subsequent response but does not have any effect of its own.
Ligand – Any molecules which is attached selectively to particular receptors.
The interaction of drug with receptor was analogous a “lock” and “key”. Thus, certain organic compounds would fit properly into the receptor and activate it, leading to a high degree of specificity.
The term opiates refers to narcotic analgesics that are structurally related to morphine, whereas opioids is term used to cover all the synthetic, semisynthetic, naturally occuring, and endogenous compounds that interact with opioid receptors in the body. It is important to appreciate that the opioids are not only compounds which are of use in the relief of pain: there are several other classes of analgesic, including aspirin.
The use of terms opiate and opioid requires some clarification. In addition to having pharmacologic effects similar to morphine, a compound must be antagonized by an opioid antagonist such as naloxone to be classified an opioid [1-3].
Opioid ligands can interact with different opioid receptors as agonists, partial agonists or competitive
62 |
P a g e
antagonists. The overall pattern of effect a particular agentdepends not only on the nature of its interaction with different opioid receptors, but also on its relative affinity for these, example:- morphine is an agonist on mu, kappa, delta receptors, but its affinity for mu receptor is much higher than that for other two. The effects, therefore, are primary the result of mu receptor activation [2, 3].
The opioid receptors belong to family of G-protein coupled receptor. The opioid receptors distributed throughout the brain, spinal cord, and peripheral tissues. The study of the biological functions of opioid receptors in-vivo was aided by the synthesis of selective antagonists and agonist. In-vivo infusion of selective antagonists and agonists were used to establish the receptor types involved in mediating various opioid effects.
The morphine activates analgesic receptors in the central nervous system (CNS) and that this leads to a reduction in the transmission of pain signal to the brain [3].
The morphine act agonist at all three types of receptor (mu, kappa, and delta) and activation leads to a variety of cellular effect depending on the type of receptor involved. These include the opening of potassium ion channels, the closing of calcium ion channel, or the inhibition of neurotransmitter release.
Activation of all three types of opioid receptors (Mu, Kappa, and Delta) can produce antinociception, but there are significant differences in the effects of activating different receptor types, depending on noxious stimulus used. A variety of antinociceptive assays that used different noxious stimuli and different animal species have been used to examine the activity of potential analgesics. Animal model for pain include models of acute pain (example- hot plate, tail flick, paw pressure, and writhing assays), persistent pain (example:- the formalin test), chronic pain (example:- adjuvant induced arthritis) and neuropathic pain (example:- nerve ligation)
TYPES OF OPIOID RECEPTORS
The opioid receptors are activated by morphine. The opioid receptors are mainly classified as three types A) Mu (µ) receptors (Mu for morphine) : MOR 1) Mu1 (µ1) receptor
2) Mu2 (µ2) receptor
B) Kappa () receptors (Kappa for ketocyclazocine) : KOR
1) Kappa1 (1) receptor 2) Kappa3 (3) receptor
C) Delta () receptor (Delta for deferens) : “DOR” 1) Delta1 (1) receptor
2) Delta2 (2) receptor
The fourth type of opioid receptors have been later identified in the 1990s which shows a lot of structural similarity to the classical opioid receptors
D) Nociception / Orphan receptor : NOR
Type A):- Mu (µ) Receptors [Mu for morphine] MOR The mu receptors are found primarily in the brainstem and medial thalamus. The mu receptors is characterized by its high affinity for morphine. The endogenous ligand for mu receptors-peptides called endomorphins 1 and 2, have only recently been found in mammalian brain. They produce biological effects ascribed to mu receptor. Other opioid peptides viz. β-endorphin, enkephalins, and dynorphins bind to mu receptors with lower affinity [1].
Endomorphin-1 (Tyr-Pro-Trp-Phe-NH2) and endomorphin -2 (Tyr-Pro-Phe-NH2) are endogenous opioid peptide with high degree of selectivity for mu receptors. In general agonist at mu receptors produce analgesia, respiratory depression, decreased gastro-intestinal motility, euphoria, feeding and release of hormone. Most clinically used opioid drugs bind to the mu receptors. The opioid drugs bind to the mu receptors. The opioid drugs is morphine, codein, ethylmorphine, methadone, tramadol, fentanyl.
Activation of mu receptors by an agonist causes itching, nausea, slightly reduced blood pressure, miosis, decreased bowel motility often leading to constipation. The overdose of opioids kills through apnea and fatal hypoxia, often caused by combination with alcohol, benzodiazepines or barbiturates. Opioid overdoses can be rapidly reversed through the use of opioid antagonist that is the naloxone is use [1, 4].
The mu receptors also found in intestinal tract which cause constipation. The mu receptors exist either pre-synaptically or post-pre-synaptically depending upon cell type. The mu receptors have high affinity for enkephalins and β-endorphin but low affinity for dynorphins. Naloxone, Naltrexone, pentazocine, Nalorphine, Diprenorphine are the antagonist involved in mu receptors while Fentanyl, Endorphin, Methadone, Pentazocine, Enkephalin, Etorphine, Morphine, Buprenorphine, Levorphanol are agonist involved in kappa receptors.
Two subtypes of mu receptors have been proposed:- 1) Mu1 (µ1) receptor
2) Mu2 (µ2) receptor
Mu1 (µ1) receptor
The mu1 receptor has higher affinity for morphine, mediates supraspinal analgesia and is selectively blocked by naloxonazine. Generally the mu1 receptor located in brain. The function of mu1 receptor is analgesia and physical dependence. The selective agonist of mu1 receptor containing meptazinol and etonitazene.
Mu2 (µ2) receptor
63 |
P a g e
miosis, euphoria, reduced gastrointestinal motility, andphysical dependence.
Type B):- kappa () receptors [kappa for ketocyclazocine] KOR
The kappa receptor defined by its high affinity for ketocyclazocine and dynorphin A. The kappa receptor is a protein. The kappa receptors are primarily found in limbic, brainstem, and spinal cord. The kappa receptor binds to opioid peptide dynorphin as primary endogenous ligand. In addition to dynorphin, a variety of natural alkaloids and synthetic ligands binds to receptor. The kappa receptors may provide a natural addiction control mechanism, and therefore the drug that act as agonists and increase activation of this receptor may have therapeutic potential in the treatment of addiction [1].
Ethylketazocine and bremazocine are two compounds used in early studies to investigate kappa receptors. They are not highly selectivity kappa agonist generally produce analgesia, other effects are respiratory depression (lower ceilling) dysphoria, psychomimetics, miosis, sedation, and reduced gastrointestinal motility.
The kappa receptors are also known for their characteristic diuretic effects, due to their negative regulation of antidiuretic hormone (ADH). The kappa receptors activation by agonist is coupled to the G-protein Gi/Go, which subsequently increases phosphodiaesterase activity. The kappa receptors have been shown to interact with sodium-hydrogen antiporter 3 regulators [1, 4].
The Endomorphine-1 and Morphine are less selective in kappa receptors. Generally Pentazocine, Etorphine, Spiradoline, Dynorphin A, Cyclazocine and Levorphanol are agonist involved in kappa receptors while Naloxone, Naltrexone, Buprenorphine, Diprenorphine, Nor-Binaltorphimine (Nor-BNI) these are the antagonist involved in kappa receptors.
Subtypes of Kappa receptors
Two subtypes of kappa receptors have been proposed:- 1) Kappa1(1) receptor
2) Kappa3(3) receptor
Kappa1 (1) receptor
The kappa1 (1) receptor have mediates analgesia. Generally the kappa1 receptor located in brain.
Kappa3 (3) receptor
The kappa3 (3) receptor have mediates the lower ceiling supraspinal analgesia. Generally the kappa3 receptor located in spinal cord, peripheral sensory neurons. The function of kappa3 receptor is diuresis, dysphoria, miosis, neuroprotection, sedation, and stress etc.
Type C):- Delta () Receptors [Delta for deferens] DOR
The delta receptors have high affinity. The activation of delta receptors produces some analgesia. Delta receptors are present in dorsal horn of spinal cord. The limbic areas are rich in delta receptors. The proconvulsant action is more prominent in delta agonist. In delta receptors the endomorphin have less selective. The non-peptide agonists and antagonist have been design to study the function of delta receptors. Generally Etorphine, Enkephalin, Cyclazocin, levorphinol, Endorphine, Deltorphine are the agonist involved in delta receptors while the Naltrexone, Naltrindol, and Naltrexone are the antagonist involved in the delta receptors [1].
Naltrindol penetrate the CNS and displays antagonist activity that is selective for delta receptors in-vitro, and in-vivo systems. Delta receptors antagonist have been shown critical potential as immunosuppressants [4].
The delta receptors have less serious side effects as compare to mu receptors, for example:- The delta receptors does not cause sedation, euphoria, or physical dependence. Delta receptors have been produce respiratory depression, gastrointestinal motility, affective behaviour and proconvulsants etc [1].
Subtypes of Delta receptors
Two subtypes of delta receptors have been proposed 1) Delta1 (1) receptor
2) Delta2 (2) receptor
Delta1 (1) receptor
The delta1 (1) receptor located in brain. The delta1 receptor produces the analgesia and antidepressant effects.
Delta2 (2) receptor
The delta2 (2) receptor located in amygdala olfactory bulbs, deep cortex, peripheral neurons etc. The delta2 receptor produces convulsant effects and physical dependence.
Type D):- Nociception /Orphan Receptors NOR
The orphan receptors as its endogenous ligand is not known, but endogenous ligand have been identified as polypeptide structure called nociception.
The activation of orphan receptors can either increase or decrease the sensitivity to pain depending on the location of receptor and the method by which agonists are administered. The orphan receptors are located in brain, cortex, spinal cord, amygdale hypothalamus. The function of orphan receptors is anxiety, and depression.
Physiology and pharmacology of opioid receptors A) Opioid effects in the central nervous system and the periphery
64 |
P a g e
Discovery of multiple opioid receptor types current nomenclature
Signal transduction mechanisms
Characterization of opioid receptors
Opioid effect in the central nervous system and periphery
Opioid receptors are found in the both CNS and in periphery. In the CNS different types of opioid receptors (µ, Ƙ, ɗ receptors); exhibit distinct anatomical distributions, and there is considerable species variation in both relative density and receptor distribution. Peripheral receptors mediate some effects of opioids, such as inhibition of gut motility, and for a number of years receptors from tissues such as the guinea pig ileum (GPI) formed the basis of standard bioassays used to assess compounds for opioid activity. Peripheral receptors have also been implicated in analgesia, particularly in cases of inflammation [5-7].
Multiple opioid receptors types
1) Discovery of multiple opioid receptors types and current nomenclature
2) Signal transduction mechanisms 3) Characteristic of opioid receptors
Discovery of multiple opioid receptors types and current nomenclature
Our understanding of Opioid receptors has expanded considerably from the early assumption of a single opioid binding site to the characterization of multiple types of opioid receptors. The initial proposal of opioid receptors by Beckett and Casy in 1954 assumed a single opioid binding site. Multiple opioid receptors were postulated as early the 1960s by both Portoghese (82) and Martin (83). On the basis of the pharmacological profile of variety of opioids, Martin proposed three types of opioid receptors, µ, k, and δ receptors, with morphine, ketocyclazocine, and SKF-10,047 respectively, as the prototypical ligands. The discovery of the enkephalins led to proposal of distinct opioid receptors type, the µ receptor, for these opioid peptides. The existence of three distinct opioid receptor types, the µ, k, and δ receptors, have now been clearly established and these receptors have been cloned. Sigma receptors, however, are not considered opioid receptors because effects associated with this receptor are not reversed by opioid antagonist such as naloxone. Other opioid receptor types have also been proposed but this receptor types are not universally accepted. Although distinctly different from opioid receptors, the ORL1 receptor interacts with the opioid receptors system in regulation of analgesia and other physiological effects [5-7]. In 1996 the “International Union of Pharmacology” (IUPHAR) recommended that OP1, OP2, OP3 be used as the accepted names for δ, k, µ receptors, respectively, to replace the DOR, KOR, and MOR nomenclature typically used in the literature; OP4 have been proposed name for the
related ORL1 receptor. This nomenclature have not gained widespread acceptance, however, and in 2000 the “International Narcotic Research Conference” recommended a modified nomenclature DOP, KOP, MOP, and NOP for δ, k, µ and ORL1 receptors, respectively, which is consistent with the nomenclature requirements of “IUPHAR”.
Signal transduction mechanism
There is considerable evidence that opioid receptors are coupled to G-proteins and produce their effects through these proteins. The structure of cloned opioid receptors is consistent with their belonging to this receptor superfamily. G-proteins are heterotrimers, consisting of α, β, γ subunits, which bind guanine nucleotides to their α-subunit and catalyze the hydrolysis of GTP to GDP. G-protein mediate the interaction of opioid and other receptors with a variety of effector system, including adenylyl cyclase and ion channels.
The effector systems that have been implicated in the transduction mechanisms for opioid receptors, the best studies is opioid inhibition of adenyl cyclase. Thus binding of an agonist to opioid receptors inhibits the activity of adenylyl cyclase and decrease intracellular cAMP in a number of different tissues. Agonist activation of all three types of cloned opioid receptors to inhibit adenyl cyclase have been demonstrated. There is also some evidence that µ and k opioid receptors can stimulate adenylyl cyclase in certain tissues. There are conflicting receptors on whether δ opioid receptors stimulate or inhibit phosphatidylinsterol turnover in some tissues; δ and µ receptors however, do not appear to be coupled to phosphatidylinositol turnover in neuroblastoma cell lines [5-7].
Opioid receptors can also be coupled to ion channels through G-proteins. All three receptor types can decrease voltage-dependent Ca++ current. The coupling of opioid receptors to calcium channels involves a G-protein, and the actions of opioids on Ca++ current are blocked by pertussis toxin, indicating involvement of Gi or Go. Activation of µ and k receptors can also increase K++ conductance. Similar to results found for calcium channels, potassium channel coupling to opioid receptors appears to involve a G-protein and is sensitive to pertussis toxin.
Agonist binding to opioid receptors also appears to activate the the extracellular signal regulated kinase (ERK) cascade.
Characterization of opioid receptors
65 |
P a g e
pharmacokinetics, the choice of noxious stimulus, and theanimal species and strain used for assay. The results of in vitro assays are not influenced by many of these factors that complicate in vivo assays. The pharmacological activity of opioids in vitro can still be complex, however, because more than one opioid receptors type is present in many tissues. Opioid receptors are present in a variety of peripheral tissues, and isolated tissue preparations, particularly the guinea pig ileum (GPI) and mouse vas deferens (MVD), have been routinely used to assess opioid activity. Radioligand binding assays for each of the opioid receptor types have been instrumental in the identification of selective opioids. With the cloning of the opioid receptors, assays for both opioid receptors affinity and efficacy can now be routinely performed by use of these cells that express only a single receptor type, greatly simplifying the interpretation of the results of the assays [5-7].
The presynaptic action of opioids to inhibit neurotransmitter release is considered to their major effect in the nervous system. Opioid drugs act in both the central and peripheral nervous systems. The central nervous system opioids have effects in many areas including the spinal cord; peripheral nervous system actions of opioids in both the myenteric plexus and submucous plexus in the wall of the gut are responsible for the powerful constipating effects of opioids.
Transducer mechanism
All three type of opioid receptors that is mu (µ),
Kappa (Ƙ), delta (ɗ) have been cloned; all are GPCRs located mostly on prejunctional neurones. They generally exercise inhibitory modulation by decreasing release of the junctional transmitter. As such, various monoaminergic (NA, DA,5-HT), GABA, glutamate (NMDA/AMPA) pathways are intricately involved in opioid actions [1].
Opioid receptor activation reduces intracellular cAMP formation and open K+channels (mainly through µ and k receptor) or suppresses voltage gated N type Ca2+ channels (mainly µ receptor). These actions result in neuronal hyperpolarization and reduced availability of intracellular Ca2+- decreased neurotransmitter release by cerebral, spinal and myenteric neurone (e.g. glutamate from primary nociceptive afferents).
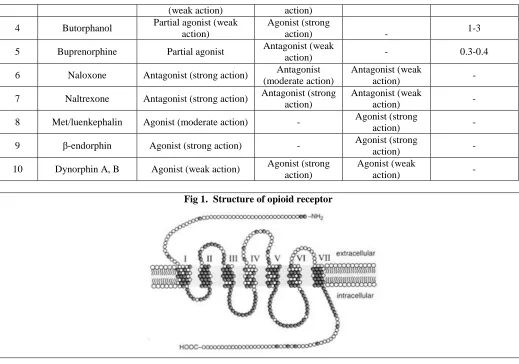
Structure of intracellular and extracellular mechanism of opioid receptors
Each transmembrane helix is labelled with a roman number.
The white empty circles represent non conserved amino acid among the MOP, KOP, DOP, and NOP receptors.
Violet circle with a letter represent further identity between the MOP-R, DOP-R and KOP-R.
Green circles highlight the highly conserved fingerprint residues.
Yellow circles depict the two conserved cystines in EL loops 1 and 2 likely forming a disulfide bridge.
IL- Intracellular loop and EL- Extracellular loop.4
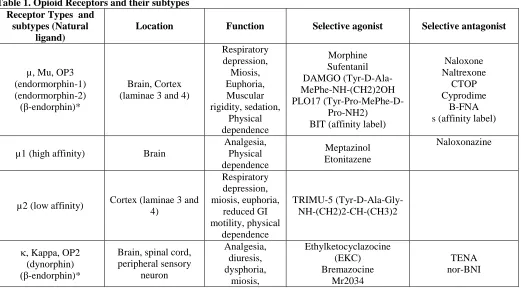
Table 1. Opioid Receptors and their subtypes Receptor Types and
subtypes (Natural ligand)
Location Function Selective agonist Selective antagonist
µ, Mu, OP3 (endormorphin-1) (endormorphin-2) (β-endorphin)*
Brain, Cortex (laminae 3 and 4)
Respiratory depression,
Miosis, Euphoria, Muscular rigidity, sedation,
Physical dependence
Morphine Sufentanil DAMGO (Tyr-D-Ala-MePhe-NH-(CH2)2OH PLO17
(Tyr-Pro-MePhe-D-Pro-NH2) BIT (affinity label)
Naloxone Naltrexone
CTOP Cyprodime
Β-FNA s (affinity label)
µ1 (high affinity) Brain
Analgesia, Physical dependence
Meptazinol Etonitazene
Naloxonazine
µ2 (low affinity) Cortex (laminae 3 and 4)
Respiratory depression, miosis, euphoria,
reduced GI motility, physical
dependence
TRIMU-5 (Tyr-D-Ala-Gly-NH-(CH2)2-CH-(CH3)2
, Kappa, OP2 (dynorphin) (β-endorphin)*
Brain, spinal cord, peripheral sensory
neuron
Analgesia, diuresis, dysphoria,
miosis,
Ethylketocyclazocine (EKC) Bremazocine
Mr2034
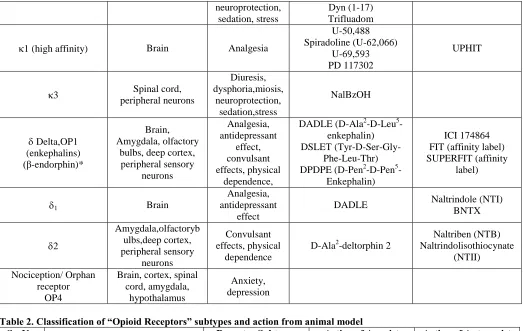
66 |
P a g e
neuroprotection,sedation, stress
Dyn (1-17) Trifluadom
1 (high affinity) Brain Analgesia
U-50,488 Spiradoline (U-62,066)
U-69,593 PD 117302
UPHIT
3 Spinal cord, peripheral neurons
Diuresis, dysphoria,miosis,
neuroprotection, sedation,stress
NalBzOH
Delta,OP1 (enkephalins) (β-endorphin)*
Brain, Amygdala, olfactory
bulbs, deep cortex, peripheral sensory
neurons
Analgesia, antidepressant
effect, convulsant effects, physical
dependence,
DADLE (D-Ala2-D-Leu5 -enkephalin) DSLET
(Tyr-D-Ser-Gly-Phe-Leu-Thr) DPDPE (D-Pen2-D-Pen5
-Enkephalin)
ICI 174864 FIT (affinity label) SUPERFIT (affinity
label)
1 Brain
Analgesia, antidepressant
effect
DADLE Naltrindole (NTI) BNTX
2
Amygdala,olfactoryb ulbs,deep cortex, peripheral sensory
neurons
Convulsant effects, physical
dependence
D-Ala2-deltorphin 2
Naltriben (NTB) Naltrindolisothiocynate
(NTII)
Nociception/ Orphan receptor
OP4
Brain, cortex, spinal cord, amygdala,
hypothalamus
Anxiety, depression
Table 2. Classification of “Opioid Receptors” subtypes and action from animal model
Sr. No. Receptor Subtypes Action of Agonist Action of Antagonist
1 Analgesia:-Supraspinal and Spinal
µ, ,
Analgesia No effect
2 Respiratory function µ Decrease No effect
3 Gastrointestinal tract µ, Decrease transit No effect
4 Psychotomimesis Increase No effect
5 Feeding µ, , Increase feeding Decrease feeding
6 Sedation µ, Increase No effect
7 Diuresis Increase
8 Hormone regulation:- Prolactin Growth hormone
µ µ and/ or
Increase release
Decrease release
9 Neurotransmitter release:- Acetylcholin Dopamine
µ
µ, Inhibit
10
Isolated organ bioassay:- Guinea pig ileum Mouse vas
deferens
µ
Decrease contraction No effect
Table 3. Nature of interaction of opioid ligand with the three major types of “Opioid receptors”, along with equivalent analgesic doses
Sr.
No. Ligand Mu (µ) Kappa () Delta ()
Analgesic* dose (mg)
1 Morphine Agonist (strong action) Agonist (weak action)
Agonist (weak
action) 10
2 Nalorphine Antagonist (strong action) Agonist (moderate
action) _ _
67 |
P a g e
(weak action) action)4 Butorphanol Partial agonist (weak action)
Agonist (strong
action) - 1-3
5 Buprenorphine Partial agonist Antagonist (weak
action) - 0.3-0.4
6 Naloxone Antagonist (strong action) Antagonist (moderate action)
Antagonist (weak
action) -
7 Naltrexone Antagonist (strong action) Antagonist (strong action)
Antagonist (weak
action) -
8 Met/luenkephalin Agonist (moderate action) - Agonist (strong
action) -
9 β-endorphin Agonist (strong action) - Agonist (strong
action) -
10 Dynorphin A, B Agonist (weak action) Agonist (strong action)
Agonist (weak
action) -
Fig 1. Structure of opioid receptor
ACKNOWLEDGEMENT Nil
CONFLICT OF INTEREST None
REFERENCES
1. Tripathi KD. Essential of pharmacology. 7th ed. Jaypee publication. New Delhi, 2013, 478 -480.
2. Wilson and Gisvold’s. Textbook of organic medicinal and pharmaceutical chemistry. 12th ed. Wolters Kluwer Pvt. Ltd. New Delhi, 2011, 778-782.
3. William O. Foye’s. Principles of medicinal and pharmaceutical chemistry. 3rd ed. Varghese publishing house. New York, 1986, 455-459.
4. Ashutosh kar. Medicinal Chemistry. 4th editions. New Age International publishers, 2007, 307, 377. 5. Donald J. Abraham. Burgers Medicinal Chemistry and Drug discovery, 6, 1998, 395, 400.
6. Graham L. Patrick. Introduction to Medicinal Chemistry. 5th ed, Oxford publication., 2013, 62, 115, 206, 635-636.
7. Goodman and Gilman’s. The Pharmacological basis of therapeutics.10th ed., Published by Joel G. Hardman and Lee. E. Limbird, 2001, 573-580.