Policy Proposal for the Use of Fluoride Varnish
in Early Head Start Programs
by
Kristine M. Enright, D.D.S.
10 April 2006
A Master's paper submitted to the faculty of the University of North Carolina at Chapel
Hill in partial fulfillment of the requirements for the degree of Master of Public Health in
the School of Public Health, Public Health Leadership Program.
Fluoride V amish
Abstract
Dental caries is the most common unmet health care need of children and has
been termed a "silent epidemic" by the Surgeon General. Children living at :::._200% of
the Federal Poverty Level statistically experience a disproportionate amount of the
nation's reported caries. Disparities in oral health status as well as in access to care
provide the impetus for aggressive, proactive involvement in the reduction of caries in
indigent children.
Early Head Start provides an ideal venue for targeting a high caries risk
population of children. Due to its existent infrastructure that supports health initiatives for
children living near the poverty level, the Head Start program not only offers access to a
population base composed of indigent children but also has program planning that
involves health improvement interventions. Fluoride varnish is a caries preventive topical
fluoride that is applied in a thin layer to teeth.
It
is a safe, easy to apply, cost effective,
and efficacious modality for reducing caries, especially in young children. The use of
fluoride varnish in Early Head Start programs provides a logical yet simple approach to
reducing caries in indigent children.
A policy of administering an annual application of fluoride varnish to children,
ages 0-3 years of age who are participants in a Early Head Start program will decrease
the negative impact not only of Early Childhood Caries but caries in general for this high
Policy Paper on the Use of Fluoride Varnish
in Federally Funded Childcare Agencies
Fluoride Varnish 3
Oral health is a multi-factorial state of health and requires a holistic view of one's
physical, social, demographic, and economic condition. The traditional
medical/surgical model was applied to dentistry in the 1840's and dentists
became known as Doctors of Dental Surgery. The concept of alleviation of
discomfort via symptom treatment was the norm until the mid 1900's, despite
insightful commentaries found in works such as Chirurgia Magna written in 1386
by Guy de Chaulia advocating a preventive nutritional and oral hygiene approach
to oral care.1 In the 1940s, the establishment of fluoride as an oral health
preventive agent and its inaugural use in public water supplies as a deterrent to
tooth decay launched a new era of proactive oral health medicine. 2 This era has
been accentuated in the 21'1 century by the practice of evidence-based dentistry as well as the use of sophisticated technology and advanced information
services. However, despite the shift in focus in dentistry towards prevention and a
plethora of technologic improvements, oral health disparities are glaring in
populations defined by low income, lack of insurance, minority ethnicity, and
geographic isolationism. In a review of the oral health status of children who fall
into one of these categories, the disparity is even more pronounced.
Dental caries (tooth decay) results from the demineralization of tooth
structure from acid produced by oral flora. The effects of dental caries on young
children can be devastating. This paper proposes the establishment of a policy
Fluoride Varnish 4
days, of fluoride varnish to high caries risk children, from first tooth eruption to
age three, who are participants in Early Head Start programs. The policy will
assist in: decreasing the risk of caries, improving the potential for a caries free
oral health history, increasing the parent or caregiver's oral health literacy, and
addressing the oral health disparity issue of initial access to the oral health care
system. The effects of such a policy for use in these programs will isolate a key
marker for high caries risk children: poverty. Low socioeconomic status of the
household is a constant variable for increased risk for caries in children,
according to groups such as the American Academy of Pediatric Dentistry and
the Center for Disease Control [CDC] (Division of Oral Health).3 According to the
CDC Key Findings Report of NHANES (National Health and Nutrition
Examination Survey) 1999-2002 (2005), the risk of caries for indigent children is
twice that of children not living near the poverty level. The resultant oral health
disparity is corroborated by the fact that over 34% of indigent children, aged 2-11
years old, have untreated dental caries as compared with 13% of children living
in households with incomes> 200% of Federal Poverty Levels (FPL)4 Not only
are poor children more likely to have caries, but they are also more likely to have
untreated caries. Seale and Casamassimo (2003) conducted a survey of general
dentists reviewing their office protocol for appointing children for dental treatment.
Even though 91% of the 4,970 dentists surveyed treated children, very few
dentists offered care to children who were younger than four years of age, had
Medicaid insurance, or had rampant caries.5
The use of fluoride varnish is an avenue of hope in reducing this access to
Fluoride V amish 5
proactive care that is easy to place and has a low biologic risk factor. Since
fluoride varnish is a sticky formulation that sets rapidly on the teeth, smaller
amounts of fluoride can be used due to the increased contact time with tooth
structure. The increased contact time not only allows for less fluoride to be used,
but also facilitates increased uptake of fluoride by the tooth-" There is less
swallowing ofthe fluoride varnish than other topical fluoride applications due to
its rapid set and the small amount that is applied. The fluoride varnish is easily
removed by tooth. brushing at home the next day. This simple yet efficacious
preventive technique has been shown to reduce caries on both primary and
permanent dentition.
In February 2006, in the Journal of Dental Research, Dr. Jane Weintraub
released the results of a study by a team of dental researchers from the San
Francisco School of Dentistry. The two-year randomized,
dental-examiner-masked clinical trial substantiates the efficacy of fluoride varnish, in reducing
decay in young children with no adverse effects. Her findings conclude that
indigent children who did not receive an annual fluoride varnish were twice as
likely to have decay as children who did receive the fluoride varnish treatment7
Fluoride varnish's effectiveness coupled with a low risk factor, even in infants,
has spawned public health, the Center for Disease Control (CDC), and groups
such as the Children's Dental Health Project in Washington, D.C. to advocate the
use of fluoride varnishes on high caries risk children from initial tooth eruption to
Fluoride Varnish 6
this age group and the use of fluoride varnish is gaining momentum as a
reimbursable service for medical providers.12
Rationale for an oral health policy geared towards ages 0-3 years of age:
In 1996, in an effort to assist state oral health programs assess need and efficacy
of action, the CDC and the National Institute of Dental and Craniofacial Research
(NIDCR) developed the NHANES tool for the assessment and monitoring of oral
health parameters. The national surveillance data collected includes the oral
health status of minority and underserved populations with a key focus being to
provide such data for analysis of achieving Healthy People 2000 and 2010
objectives.13 A product of that partnership was presented in a CDC report,
Summary Surveillance for Dental Caries, Dental Sealants, Tooth Retention,
Edentulism, and Enamel Fluorosis (2005). The summary offered an analysis of
the NHANES for years 1988-1994 and 1999-2002. Despite the overall decrease
in caries and severity of caries in the permanent dentition, no such trend was
seen in primary dentition. Forty one percent of children ages 2-11 years had a
decayed, missing, or filled primary tooth and 21% of this same population had
untreated caries present. These percentages escalated when children living
below the Federal Poverty Level (FPL) were carved out. The percentage of
children living below the FPL who have decayed teeth was almost doubled when
compared to the percentage of children with decayed teeth who live at> 200% of
the FPL.14 The same escalation factor applies to the untreated caries found in
children living at< 100% of the FPL: the percentage of untreated caries is 33.5%
Fluoride Varnish 7
FPL.15 The summary additionally noted that more than 91% of the adults with
remaining dentition had experienced caries.16 This is a significant finding
attributed to the communicable nature of caries. If the primary caregiver has
caries, the cariogenic oral flora may be transmitted to the child. Mutans
streptococci, the primary cariogenic bacteria found in the mouth, can be
transmitted from caregiver to child by commonplace actions, such as licking a
child's pacifier prior to placing it in the child's mouth or tasting the child's food
prior to feeding the child.17 It is noteworthy to consider that once a child has
active caries, he is more likely to have future caries experiences.18 Other
significant economic and epidemiologic risk factors of caries are identified in the
American Academy of Pediatric Dentistry's Caries Risk Assessment Tool. (Table
1)
Caries, resulting from the demineralization of tooth enamel, is affected by
various individual factors such as amount of cariogenic flora present in the
mouth, the length of time the teeth are exposed to carbohydrates, frequency of
exposure, type of carbohydrates ingested (refined vs. complex), consistency and
rate of salivary flow (which may be altered by medications that dry out the
mouth), natural buffering capacity of saliva, enamel structure (especially if
defective or thin), and the presence of active decay. It is also essential to
consider any inability to perform daily oral hygiene functions as a result of
physical, mental, or environmental barriers (such as a lack of clean water).
The caries paradigm is also influenced by factors beyond the individual's
Fluoride V amish 8
noted in the caregiver's and/or siblings' oral history also potentiates the
individual's risk of caries."·20•21
The American Dental Association (ADA) defines Early Childhood Caries
(ECC) as "the presence of one or more decayed (non-cavitated or cavitated
lesions), missing (due to caries) or filled tooth surfaces in any primary tooth in a
preschool-age child between birth and 71 months of age". 22 The State of
Nevada's Oral Health Program reported that in 2004, 25% of their Head Start
preschoolers had Early Childhood Caries23
Another critical factor in caries prevention and treatment is access to care.
Weintraub's recent findings underscore the efficacy of preventive treatments in
decreasing caries activity. 24 The dilemma for indigent children is getting access
to these treatments. According to Oral Health in America: A Report of the
Surgeon General, only 30% of the children living near the poverty level are likely
to see a dentist within a year25 Access to care is affected by numerous barriers,
including: language barriers, transportation barriers, lack of providers who accept
public insurance or a sliding fee arrangement, lack of the caregiver's
understanding of the importance of early preventive dental care (low oral health
literacy), and fear (caregiver fear of the dentist, fear of navigating the Medicaid
and public insurance system to arrange an appointment, and fear of
chastisement or denigration when presenting the child for treatment).
In the Maternal and Child Oral Health Issues fact sheet (2004), one reason
for lack of access was underscored by the statistic that even though 90% of
general dentists will treat children, very few dentists will see children less than
Fluoride Varnish 9
of access is borne out for Medicaid children with the finding that less than 20% of
Medicaid children were the recipient of at least one preventive dental service
annually27 In addition, an August 2005 fact sheet from CDC noted a differential
in the number of lost days from school due to dental pain or emergencies when
comparing different income groups (indigent children have 12 times the rate of
absences when contrasted with families living at >200% of FPL). Chronic dental
pain also contributed to dysfunctions in eating, speaking, and learning28
The devastation to oral health from the actual decayed dentition, the
decrease in general systemic health due to the inability to properly chew food and
maintain a high level of nutritional intake, and the psychological as well as
physical effects of pain and decreased self esteem are strong indicators of the
need of a policy to address the prevention of tooth decay early in life.
Fluoride Modalities and Efficacy:
In the late 1930s, puzzled by the brown mottled appearance.of his patients' teeth
in Colorado, Frederick McKay began a research project that resulted in one of the
ten greatest public health achievements of the 201" Century, the fluoridation of water. 29 With the advent of fluoridated water in the 1940s, after World War II the
decay rate in the United States decreased by 50-60%.30
Once the role of fluoride was confirmed in reducing tooth decay, new
topical and systemic fluoride products appeared on the market. The first fluoride
toothpastes were introduced in the 1950s.31 Today, some fluoride containing
products are available over-the-counter, such as toothpastes and mouth rinses
Fluoride Varnish I 0
prescription or received at a medical or dental office. For areas where the water
supply does not contain optimal levels of natural fluoride there are fluoride
supplements, such as prescription drops or tablets, which provide a systemic
source of fluoride. This source is beneficial for children during the development of
their permanent dentition. Professional topical fluoride products include
prescription strength fluoride pastes for brushing, professionally applied gels and
foams, and fluoride varnishes. Fluoride is even found in some sealant and
restorative products, such as glass ionomers.
Fluoride Varnish
The first fluoride varnish was developed in Germany in 1964 by Schmidt. It was a
5% NaF product in a neutral colophonium base, marketed under the name
Duraphat (Woelm pharma Co., Eschwege, FRG). Approximately 10 years later,
another fluoride varnish product, Fluro Protector, was introduced by Arends and
Schuthof. Due to its polyurethane base, the new varnish dried in contact with air
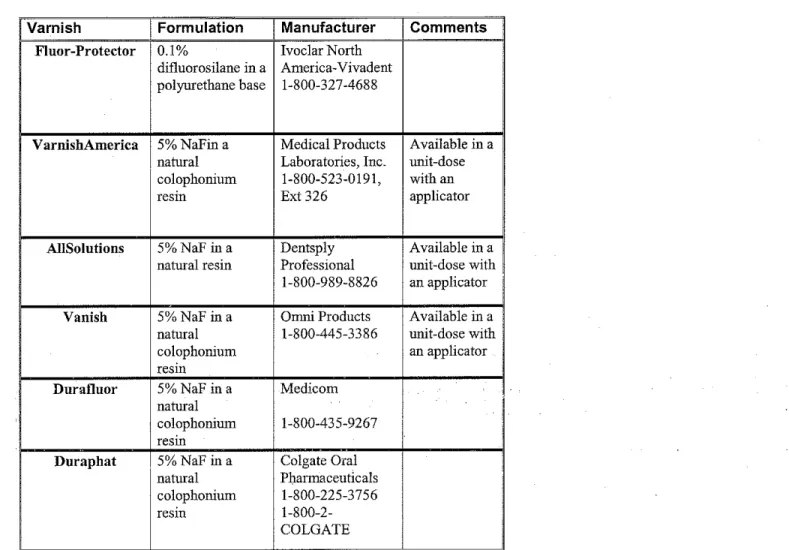
to a thin, transparent film.32 Today, all six available varnishes are still in the
natural colophonium base or in the polyurethane base. The trade names,
manufacturers, and description of the products are listed in Table 2.
Even though fluoride varnish has been used in Europe for more than 30
years as a topical fluoride agent, only in the last 20 years has it gained entry into
the American dentists' armamentarium. In 1994, the U.S. Food and Drug
Administration (FDA) first authorized use of Duraphat as a cavity liner and
desensitizing agent. 33 Despite the fact that fluoride varnish has not yet been
Fluoride Varnish 11
topical fluoride, it currently has widespread use by the dental community as an
"off-label" topical fluoride product. This legal and common practice often occurs
when a product has been proven safe within the realm of a reasonable and safe
standard of care but the anticipated usage is not yet approved by the FDA.34 In
November of 2004, the American Dental Association released the announcement
of Resolution 37H, which states "the ADA supports the use of fluoride varnishes
as safe and efficacious within a caries prevention program that includes caries
diagnosis, risk assessment, and regular dental care."35
Fluoride varnish is an ideal topical fluoride delivery model for children due
to its effective fluoride release, ease of use, relative inexpensive cost per
application (the cost per uni-dose application is approximately 93 cents, only
slightly higher than the average fluoride gel application), prolonged contact with
the tooth, and lack of systemic ingestion resulting in adverse reactions or
eventual fluorosis. 36 The tooth surface does not have to be totally dry or
professionally cleaned prior to placement of the fluoride varnish. Using a small
brush applicator, a thin layer of fluoride varnish (0.3 to 0.5 milliliters) is applied
directly to the teeth. Fluoride has been shown to be more effective with prolonged
contact with the tooth structure.37 In 1985, Hellwig, Klimek, Schmidt, and Egerer
also confirmed an increased fluoride uptake by enamel with increased contact
time.38•39 This precept shaped the development of fluoride varnish for dental use40 Due to the prolonged contact time with the tooth, more fluoride uptake by
the enamel occurs in a dental varnish than in other fluoride application methods.
Fluoride varnish has been shown to be a safe mode for topical fluoride
Fluoride Varnish 12
gels (gels are approximately 9-12,000 ppm fluoride while varnishes are
1,000-22,600 ppm fluoride), due to the small amount of fluoride varnish needed for a
varnish application, the net exposure to fluoride is decreased41•42 Less
swallowing of the product by the young patient due to the adhesiveness of the
fluoride varnish coupled with the net decrease in bioavailable fluoride has
reduced the potential for fluoride varnish to contribute to fluorosis, enamel defects
resulting from excess systemic fluoride intake during tooth development43 One
way to measure the fluorosis potential of a topical fluoride delivery system is to
determine the plasma level of fluoride after application of the fluoride. According
to the results of a study by Dr. Jaana Autio (University of Florida College of
Dentistry) released in 2000, the blood levels of fluoride after a fluoride varnish
treatment were less than other fluoride delivery systems. This was one oLthe first
research studies focused on the primary dentition and was presented to the
International Association for Dental Research Conference in Washlngtor D.C. in
April 200044 The substantiation of decreased fluoride ingestion and risk of
fluorosis when fluoride varnish was applied to teeth as compared to othertopical
fluorides was also confirmed by Ekstrand (1987) in Pharmokinetic Aspects of
Topical Fluorides.45 The current studies on safety of fluoride varnish and its
significant benefit to high caries risk children prompted the Scottish
Intercollegiate Guidelines Network (2005) to note in their guideline
recommendations that "for high risk children where reliance on the home based
use of fluoride toothpaste and tablets is deemed to be insufficient, professional
Fluoride V amish !3
Rationale for Use of Fluoride Varnish:
In 1994, Ogard, Seppa, and Rolla reviewed the cariostatic properties and
remineralization process resulting from topical fluoride application that earmarks
fluoride as an effective anti-caries agent.47 As acid contacts the enamel surface,
minerals are dissolved, including calcium, phosphate, and carbonate. These
minerals are trapped by dental plaque, the "sticky organic matrix of bacteria, food
debris, dead mucosal cells, and salivary components that adheres to tooth
enamel" .48 Just as the dissolved minerals are trapped by dental plaque, the
introduction of fluoride via a topical application as well as its presence in saliva
also causes fluoride to be trapped in plaque. The cycle of demineralization and
remineralization is an ongoing event throughout the time a tooth is present in the
mouth. However, when fluoride is in prolonged contact with the tooth surface, the
fluoride can bind to the enamel by means of remineralization. In remineralization,
the fluoride replaces the carbonaie in the enamel's mineral content,
res~lting
in afluoro-apatite crystalline structure which replaces the hydroxy-apatite crystals.
The fluoride in varnish may actually alter the porosity of a carious lesion and
encourage the uptake of fluoride into the enamel matrix49 Interestingly, studies
have also shown that a slightly demineralized enamel surface will facilitate
uptake of fluoride more than sound enamel.50'51 This finding underscores the efficacy of professionally applied topical fluorides for high caries risk children,
who are highly likely to have areas of demineralization as is evidenced by their
increased caries rate.
In the physical act of remineralization, the altered enamel mineral content
Fluoride Varnish 14
surface that is more resistant to acid demineralization. The cariostatic action of
fluoride has been shown on a limited basis in animal models where, in the
presence of fluoride acid producing bacteria are limited in their ability to produce
acid. 52
In the CDC report, Recommendations for Using Fluoride to Prevent and
Control Dental Caries in the United States (2001), a review of Canadian and
European studies support the findings of fluoride varnish being an effective
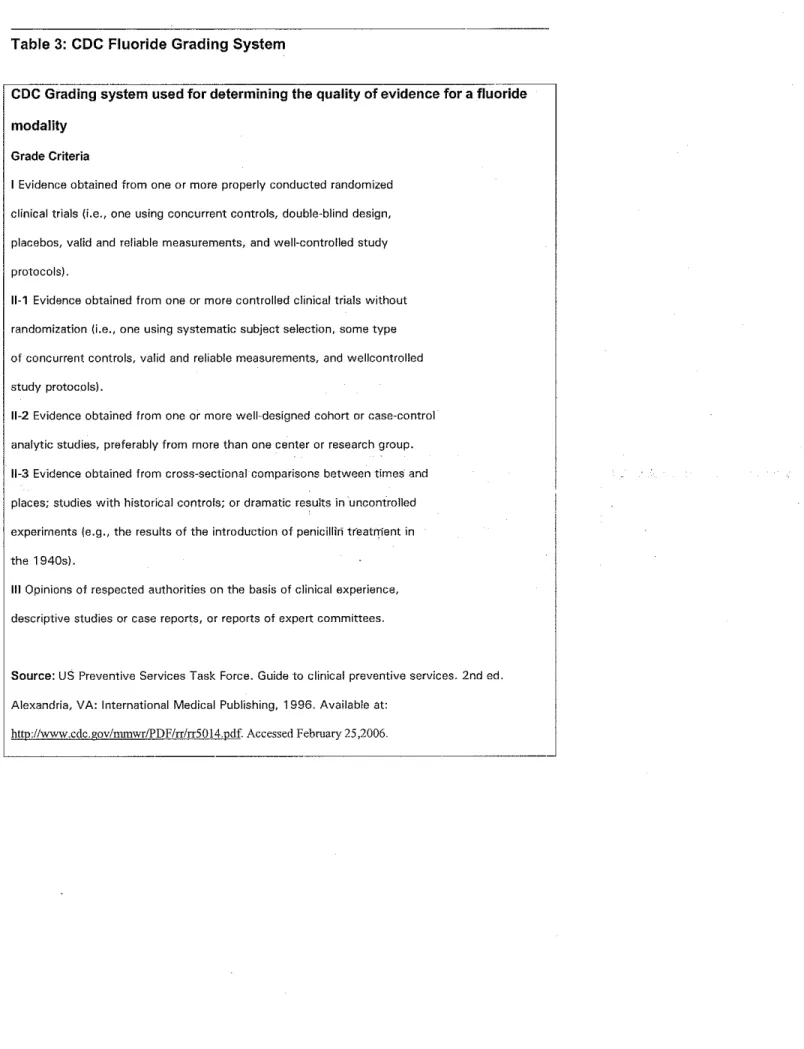
anti-caries agent. 53 The evidence used by CDC fell in a Grade 1 category, where
"evidence [was] obtained from one or more properly conducted randomized
clinical trials (i.e., one using concurrent controls, double-blind design, placebos,
valid and reliable measurements, and well-controlled study protocols)."54 (Table
3) The CDC weighs their recommendations for various fluoride modalities based
on a target audience's risk of dental caries, current availability and standards of
practice for other fluoride sources, and the biologic risk of_ enam~i fluorosis
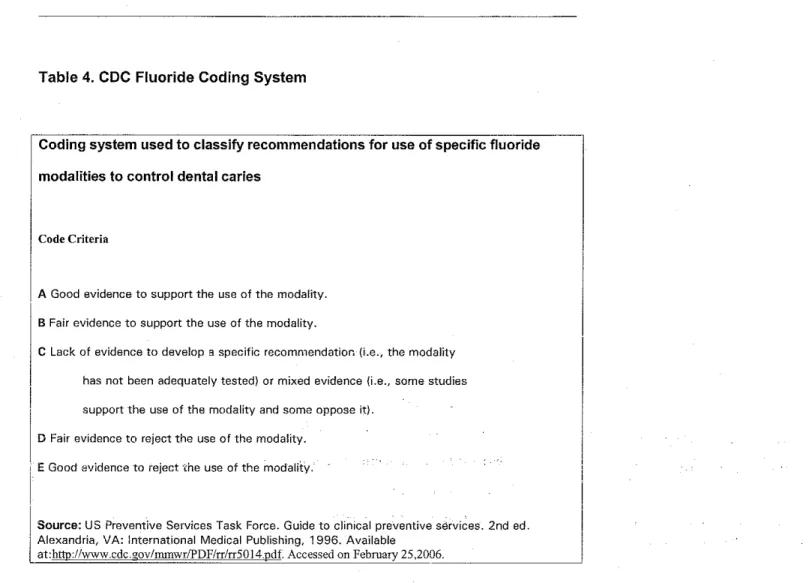
Based on current studies including data published in 2001, CDC supported the
use of fluoride varnish for caries management in high risk children, noting that
there was substantial and proven clinical evidence proving fluoride varnish's
safety and efficacy-"5 (Table 4)
In a systematic review of literature by Strohmenger and Brambilla (2001 ),
a meta-analysis of various studies is presented. Their analyses confirm the
efficacy of fluoride varnish as an anti-caries agent, especially when directed
toward the needs of indigent children as a high risk population. Fluoride varnish
has been shown to reduce the demineralization of enamel by 53-75%, though the
Fluoride V amish 15
studies were devoted to caries prevention in the primary dentition as well as
inhibiting the progression of existing caries. Fluoride varnish performed
significantly well in both instances. Early Childhood Caries is a major caries event
and occurs more frequently in indigent children. The review commented that one
main advantage of a fluoride varnish is its ability to adhere to tooth surface and
consequently deposit more significant amounts of fluoride to demineralized areas
of enamel. 56
In a literature review for the Agency for Healthcare Research and Quality,
Bader, Rozier, Harris, and Lohr (2002) acknowledge that though the risk of
fluorosis precludes recommending fluoride supplementation for low risk children,
that there is benefit for high risk children. It was also noted that the American
Academy of Pediatrics has adopted the CDC protocol for fluoride use-"7 As noted
earlier in this paper, the CDC has endorsed the use of fluoride varnish as a
topical fluoride agent for high risk children. In 1994, an. expert committee· from the
World Health Organization (WHO) concurs that fluoride varnish, particularly in
high caries risk patients, has been shown to be an effectiveanti'caries agent. 58
Rationale for Use of Early Head Start Programs:
Established in 1964 as a program to aid disadvantaged preschoolers, Head Start
has developed into a comprehensive child development program according to the
Department of Health and Human Services. Administered by the Head Start
Bureau, Head Start and Early Head Start have an umbrella goal of school
preparedness for indigent children. Programs oriented toward developing healthy
Fluoride Varnish 16
early childhood development; medical, dental, and mental health; nutrition; and
parent involvement...[which are] responsive and appropriate to each child's and
family's developmental, ethnic, cultural, and linguistic heritage and experience".59
In 1995, the Head Start Bureau broadened their scope of service from
aiding disadvantaged preschool children to including birth to age 5 years60
With the provision of adherence to a Program Performance Standard, Head Start
programs have defined goals and objectives, which must be met in order for a
program to be called successful. Serving more than 62,000 children under the
age of five years in Fiscal Year 2004, Head Start and Early Head Start would be
an appropriate backdrop for timely intervention in breaking the high caries risk
activity pattern seen in indigent children81
Lewis, Lynch, and Richardson (2005) investigated the parameters of a
successful outreach program for fluoride varnish in high caries risk populations of
children. In some practices, the fluoride varnish placement by a pediatric~ an was
the only oral health preventive service available to the children. However, the
best program outcomes resulted from practices that had a community coalition of
dental and other health care services. Based on Roger's Diffusion Theory, Lewis
and her team identified key constructs for the successful implementation of a
fluoride varnish program in the medical/dental interface. 62 The researchers
summarized the positive potential for such a model: "Fluoride varnish can be
adopted successfully into medical practice given PCP [Primary Care Provider]
and staff commitment and openness, training that leaves participants motivated,
appropriate systems, and resources for professional dental care referral. In
Fluoride Varnish 17
preventive oral health with families. Specific recommendations to encourage
fluoride varnish diffusion in other settings are offered for program planners and
PCP offices"-"3 Head Start programs already have in place the kind of network
and infrastructure suggested in this study.
According to the Scottish Intercollegiate Guidelines Network's {SIGN)
Reference Guide on Targeted prevention of dental caries in the permanent teeth
of 6-16 year olds presenting for dental care (2002), primary prevention efforts
should be focused on home and office care by means of behavior modification,
such as age appropriate oral hygiene instructions, and tooth protection.
Secondary prevention is achieved by decreasing the effects of decay in early
childhood and tertiary prevention is evidenced by treatments aimed toward
remineralization of tooth enamel.64 It is also emphasized in the reference guide to
confirm the consistency of oral health messages distributed by all partners. Head
Start programs are focused on a multi-layererJ apprqach ,to. child and fall)ily
education, utilizing networked community members to reinforce the ,steps_
necessary to achieve health and well-being. The formatting is similar to that
presented by SIGN for improved oral health.
The National Institute of Health released a Conference report in 2001
noting that "effective dentistry requires early identification of children at high risk
for extensive caries so that they may receive early and intense preventive
intervention."65 This basic premise is the foundational theme for model programs. Head Start programs have links with local medical and dental practitioners who
Fluoride Varnish 18
programs are readily accessible in the community with established community
networks necessary for the preventive oral health treatment of a high risk child.
Rationale for Annual Application:
In a 2001 CDC report on Recommendations for Using Fluoride to Prevent and
Control Dental Caries in the United States, the topic of effective frequency of
application in caries reduction is addressed. The article continues with a
discussion of appropriate time intervals between applications, noting that a
semi-annual fluoride varnish application offers equivalent fluoride benefits as
professionally applied fluoride gels. There is also mention of an alternative
application protocol of three applications within a one-week time frame. This
annual routine may even prove to be more advantageous in caries management
and remineralization than a tradition semi-annual application.66 A literature review
by Strohmenger and Brambilla (2001) of studies.pursued in the 1990's
substantiated the greater efficacy of an annual, three times in seven days,
application of fluoride varnish as opposed to the traditional semi-annual
application67
Beltran-Aguilar, Goldstein, and Lockwood reviewed variances in
application interval and its effect on caries prevention and remineralization. In
their assessment of the annual three times/week in a seven day period
application protocol, the results indicated a caries reduction of 46 to 67 % in
proximal surfaces of teeth68 A confluent finding by Castillo and Milgram (2004)
noted the more concentrated uptake of fluoride and slower release of fluoride in
Fluoride Varnish 19
annual interval as compared to a single annual application. Their commentary on
the clinical ramification was insightful. They noted the positive implication for a
caries risk management program for children who are members of a transient
household or not likely to return for recall.69
Seppa, Tuuti, and Luoma (1984) offered a different perspective on
intervals in their study of children with a high caries rate despite living in a
fluoridated water supply community. Even after receiving semi-annual fluoride
varnish applications for a total of three years, when re-evaluated after receiving
no fluoride varnish treatments for the following two years, the "the absolute
reduction in caries found during the treatment was retained, but the cariostatic
effect did not continue after treatment...[ suggesting] that fluoride varnish
applications should not be discontinued after three years."70 This finding supports
the positioning of policy for continuity of care and the integration of community
health partners for collaborative preventive ora! health efforts beyond the child's
first three years of life.
The research substantiates the need for the ongoing application of a
fluoride varnish, at least on an annual basis, with increased frequency of
application yielding even greater benefit. An annual application with a three
times/week within a seven day period would be beneficial to an indigent child
population . .This population would benefit from the remineralization effects of the
increased frequency of application. The other advantage would be the increased
likelihood of treating children who are in a mobile family. These children may not
be enrolled in the Head Start program when it is time for a follow up semi-annual
Fluoride V amish 20
and auditing evaluations already in place, the frequency and interval of
applications can be readily tracked and recorded in a child's record.
Conclusion and Recommendations:
This paper is written for the intent of proposing policy for the application of
fluoride varnish on high caries risk children, ages 0-3 years old, who are
participants in Early Head Start. The U.S. Surgeon General, Richard H.
Carmona, M.D., has labeled dental caries
'a
silent epidemic" among indigentchildren71
Despite the knowledge that access to care and oral health disparities tied
to socioeconomic status and minority ethnicities are common factors for indigent
young children's higher caries rate, in 2004 only 18 states had submitted an oral
health plan to CDC to address these issues72 The CDC encourages the
development of state plans and offers toolkits and other resources to aid in the
formulation and implementation of state plans. The CDC commentary on state
plans recognizes the plans as "a roadmap ... that has as its goal reducing the
prevalence of oral diseases [including] specific objectives related to oral health
promotion, disease prevention and control, and specified risk factors." 73 The
framework of an oral health plan assists state public health teams and other key
oral health stakeholders in effective resource management and meaningful
evaluation of outcomes. According to Turnock (2004), policy development not
only informs and empowers people but also weaves community assessment into
an effective community health initiative74 With a policy in place to encourage
Fluoride V amish 21
young indigent children, state dental public health offices are provided with a
stronger platform for development of oral health plans. When effective, the
resultant decreased prevalence of oral disease will benefit the general health of
the overall population, but most especially those at greatest risk, such as indigent
children.
Since the caries rate in the indigent child population is not decreasing,
innovative preventive modalities must be developed and implemented. The
development of a product such as fluoride varnish, supported by research stating
its efficacy and safety in treating caries in high risk populations, gives policy
makers the opportunity to implement policy that will have far reaching positive
health outcomes.
The policy suggested by this paper would include:
1. Program development for the placement of an annual topical fluoride
varnish application, with 3 applications placed within· a 7 day period, on the
primary dentition of all children in Early Head Start, ages 0-3 years of age,
pending parental consent. The fluoride varnish will be placed by a dentist,
physician, or legally eligible expanded duty medical/dental personnel.
2. Program data on caries rates and frequency of fluoride varnish application
will be made available to state and federal reporting agencies.
The hope of health is a powerful tool for increasing the quality of life.
James Joyce, at age 25, noted in a letter to his brother "my mouth is full of
Fluoride V anrish 22
our current understanding of the intricacies and interrelationships of good oral
health, self esteem, improved school performance, and general good health. As
our children begin to function free from the stigma of decayed teeth, swollen
jaws, and painful distractions, their self-perception takes on a more global
consciousness. This new vantage point affords them an opportunity to see the
Acknowledgements:
Joseph Doherty, DDS, MPH
Frank Farrington, DDS
Susan Pharr, RDH, MPH
Maternal and Early Child Oral Health Coordinator Division of Dental Health
Virginia Department of Health
Fluoride Varnish 24
Bibliography
1 Wilderding,T. History of Dentistry. Available athttp:I/WW\N.idakerala.org/dentistryhome.asp. Accessed on February 04,2006.
2 History of Dentistry. American Dental Association web site. Available at:
http://www .ada.org/public/resources/history/timeline _20cent.asp. Accessed on February 0 1 ,2006.
3 American Academy of Pediatric Dentistry. Policy Statement on the Use of a Caries-Risk Assessment Tool. Adopted
2002. Avallable at from: http:I/W-NW.aapd.org/pdf/policycariesriskassessmenttool.pdf. Accessed on February 4, 2006. 4 Center for Disease Control. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, EdentuHsm and Enamel Fluorosis-United States, 1988-1994 and 1999-2002, Prevalence of Decay (Children Aged 2-11).2005. Available at:
http://www.cdc.gov/oralhealth!factsheets/nhanes_findings.htm. Accessed February 4,2006.
5 Seale, N, Casamassimo,P. Access to dental care for children in the United States: a suNey of general practitioners. J Am Dent Assoc. 2003 Dec;134(12):1630-40.
Availableat:http:/lwww.ncbi.nlm.nih.gov/entrez/query.fcgi?CMD=Display&DB=pubmed. Accessed on March 26,2006. 6 Strohmenger, L., Brambilla, E. The Use of Fluoride Varnishes in the Prevention of Dental Caries: a Short Review. Oral Diseases. Volume 7 Issue 2 Page 71 - March 2001.doi:1 0.1034/j.1601-0825.2001.70202.x Available at:
http:/lwww.systram.org/systematicreviews.Accessed on February 11,2006.
7 Weintraub, J.A., Ramos-Gomez, F., Jue, B., Shain, S., Hoover, C.l., Featherstone, J.D.B., Gansky, S.A. Fluoride Varnish Efficacy in Preventing Early Childhood Caries.J Dent Res2006 85: 172-176. Available at:
http:!/jdr.iadljournals.org/cgi/content/short/85/2/172 .Accessed on March 4,2006.
S Virginia Department of Health, Division of Dental Health. Bright Smiles for Babies. Available
at:http://www.vahealth.org/teeth/brightsmi!es.asp. Accessed on February 4,2006. 9 North Carolina Academy of Family Physicians, Inc. Into the Mouth of Babes.Available at:
http://www.ncafp.com/site3/web/imb/tools.htmi.Accessed on: February 4,2006.
10 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States.August 2001 Available at: http:/lwww.cdc.gov/mmwr/preview/mmwrhtrnllrr5014a1.htm. Accessed on: February 11,2006.
11 Children's Dental Health Project. Available at :http:l/cdhp.org. Accessed on February 4,2006.
12 Lewis, C., Lynch, H., Richardson, L.Fiuoride Varnish Use in Primary Care; What Do Providers Think? Pediatrics
2005 115: e69-76 (doi:10.1542/peds.2004-1330). Available at:
http://pediatrics.aappublications.org/cgi/contentlfull/115/1/e69. Accessed on March 4, 2006.
13 Center for Disease Control. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism and Enamel Fluorosis-United States, 1988-1994 and 1999-2002, Prevalence of Decay (Children Aged 2-11).2005. Available at:
http://www.cdc.gov/oralhealthffactsheets/nhanes_findings.htm. Accessed onFebruary 4,2006.
14 Centerfor Disease Control. SurVeillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism and Enamel Fluorosis- United States, 1988-1994 and 1999-2002, Prevalence of Decay (Children Aged 2-11 ).2005. Available at:
http://www.cdc.gov/oralhealthffactsheetsfnhanes_findlngs.htm. Accessed on February 4,2006.
15 Centerfor Disease Control. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism and Enamel Fluorosis- United States, 1988-1994 and 1999-2002, Prevalence of Decay (Children Aged 2-11 ).2005. Available at:
http://www.cdc.gov/oralhealthlfactsheets/nhanes_findings.htm. Accessed on February 4,2006.
16 Center for Disease Control. Surveillance for Dental Caries, Dental Sealants, Tooth Retention, Edentulism and Enamel Fluorosis- United States, 1988-1994 and 1999-2002, Prevalence of Decay (Children Aged 2-11 ).2005. Available at:
Fluoride Varnish 25
17 Featherstone, J., et al. Caries Management by Risk Assessment: Consensus Statement, April 2002. Journal of the
California Dental Association. 2002. Available at: http://www.cda.org/cda _ member/pu bs/journal/jour0303/consensus. htm. Accessed on March 26, 2006.
18 National Institute of Health. Diagnosis and Management of Dental Caries Throughout Life, National Institutes of
Health Consensus Development Conference Statement. March 26-28, 2001.Available at: http://consensus.nih.gov/2001/2001Denta!Caries115html.htm. Accessed on: March 4,2006.
19 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States.August 2001. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtmllrr5014a1.htm. Accessed on: February
11,2006.
20 Sox man, J. Preventive guidelines for the preschool patient. Academy of General Dentistry.Accepted October 19, 2004 Available at: http:/Jwww.agd.org/library/2005!feb/Soxman_153.pdf. Accessed on: February 11,2006.
21 Featherstone, J., eta!. Caries Management by Risk Assessment: Consensus Statement, April2002. Joumal of the
California Dental Association. 2002 Available at: httpJ/www .cda.org/cda _ member/pubs/journal/jour0303/consensus.htm. Accessed on March 26, 2006.
22 American Dental Association. Statement on Early Childhood Caries. Available at
http:/fwww.ada.org/prof/resources/positions/statements/caries.asp. Accessed on March 26, 2006. 23 Nevada State Oral Health Program 2004. The Burden of Oral Disease in Nevada-2004. Available at: http:/lwww.ada.org/prof/resources/positions/statements/caries.asp. Accessed March 26, 2006.
24 Weintraub, J.A., Ramos-Gomez, F., Jue, B., Shain, s., Hoover, C.l., Featherstone, J.D.B., Gansky, S.A. Fluoride Varnish Efficacy in Preventing Early Childhood Caries.J Dent Res 2006 85: 172-176. Available at:
http://jdr.iadrjournals.org/cgi/contentlshorU85/2/172 .Accessed on March 4,2006.
25 US DHHS. Oral Health in America: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institute of Health, 2000.Available at http://silk.nih.gov/pub!ic/[email protected]!rpt.pdf. Accessed on M.arcti 26, 2006.
26 National Maternal and Child Oral Health Resource Center. Child and adolescent oral hea-lth issu~s. 2064. Available at http://www.mchOralhealth.org/PDFs/lssues.pdf. Aci::essecr' on MarCh 4, 2006.
27 Center for Disease Control. Preventing Dental Caries with Community Programs.August 2005. Available at: http://www.cdc.gov/oralhealth/factsheets/dental_caries.htm.Accessed on: February 11,2006. 28 Center for Disease Control. Preventing Dental Caries with Community Programs.August 2005.
Available at: http:/fwww.cdc.gov/oralhealth/factsheets/dentaJ_caries.htm.Accessed on: February 11,2006. 29 CDC Media Relations. Ten Great Publi~ Health Achievements of the 20th Century. Available at: http://www.cdc.gov/od/oc/media/tengpha.htm. Accessed on March 26, 2006.
30 American Dental Hygienists' Association. Professional Issues:. CDC Releases Guidellnes on Fluoride Use to Prevent Tooth Decay. Available at: http://www.adha.org/profissues/cdc_fluoride_guide!ines.htm. Accessed on March 26, 2006.
31 American Dental Association. History of Dentistry. Available at
http://www.ada.org/public/resources/historyltlme!ine_20cent.asp. Accessed on March 26, 2006.
32 Petersson, L.(1993). Fluoride Mouth rinses and Fluoride Varnishes. Caries Research' 27, suppl1:35-42. Available at: http://www.db.od.mah.se/car/data/fluoride.html. Accessed on February 4,2006.
33 Beltran-Aguilar, E. D., Goldstein, J. W., Lockwood, S. A.,F!uoride Varnishes: A Review of Their Clinical Use, Cariostatic Mechan!sm, Efficacy and Safety.J Am Dent Assoc 2000 131: 589-596. Available at
http://www. medscape.com/medline/pu blicationbrowser/6259/131_ 5/dt_ 050 12000/limit_ 5. Accessed on February 4, 2006. 34 Domoto, P. Off-label Use of Fluoride Varnishes. Available at
Fluoride Varnish 26
35 American Dental Association web site. ADA House OKs fluoride varnishes. November 2004. Available at: http://www.ada.org/prof/resources/pubs/adanews/adanewsarticle.asp?articleid=1157. Accessed on March 5, 2006.
36 Sullivan Schein Dental Products. (Preventive Products}Avai!able at:
http:l/www.henryschein.com/srchResultasp?SearchType=2&Keyword=2111. Accessed on March 4, 2006. 37 Relief, D., Sorvas, P .. , Bradley, E .. , Taylor, R., Walker, A. R.ln vitro fluoride uptake, distribution and retention by human enamel after 1 • and 24-hour application of various topical fluoride agents J Dent Res 1980 59: 573-582 . Available at: http:/Jjdr.iadrjournals.org/cgi/reprint/59/3/573. Accessed on February 18,2006.
38 Hellwig, E., Klimek, J., Schmidt, H. F., Egerer, R.Fiuoride uptake in plaque-covered enamel after treatment with the fluoride lacquer Duraphat.J Dent Res 1985 64: 1080-1083. Available at:
tp://jdr Jad~ournals.orgJcgi/content/abstract/64/8/1 080.Accessed on February 11 ,2005.
39 Strohmenger, L., Brambil!a, E. The Use of Fluoride Varnishes in the Prevention of Dental Caries: a Short Review.Oral Diseases. Volume 7 Issue 2 Page 71 -March 2001.doi:10.1034/j.1601-0825.2001.70202.x Avallable at:
http://www.systram.org/systematicreviews.Accessed on February 11,2006
40 Ogard, B., Seppa, L, Rolla, G.Professiona! topical fluoride applications-clinical efficacy and mechanism of action.Adv Dent Res. 1994 8: 190-201. Avallable at: http:l/adr.iadrjournals.org/cgi/reprint/8/2/190. Accessed on: March 4,2006.
41 Center for Disease ControL Other Fluoride Products. Available at:
http://www.cdc.gov/oralhealth/watertluoridatlon/other.htm. Accessed on March 26, 2006.
42 Donly,K. Fluoride Varnishes. Jouma/ of the California Dental Association. March 2003. Available at:
http://www.cdc.gov/oralhealth/wat'?rfluoridation/other.htm. Accessed on March 26, 2006.
43 Center for Disease Control. Recornmendatlons for Using Fluoride to Prevent and Control Dental Caries in the United States.August 2001. Available at: http:/!www.cdc.gov/rnmwr/preview/mmwrhtrnl/rr5014a1.htrn. Accessed on: February 11,2006.
44 Daughtry, C. Painting Teeth With Fluoride Varnish Is Effective Against Tooth Decay In Chlldren.University of F!oridia
News. April2000. Available at http://www.napa.ufl.edu/2000news/varnish.htm. Access.ed :m: February 18,2006. 45 Ekstrand, J.Pharmacokinetic aspects of topical fluorides.J Dent Res 1987 66: 1061-1065 .Available at:
http:/ljdr.iadrjournals.org/cgi/reprint/66/5/1 061. Accessed on M?Jrch 4, 2006.
46 SIGN. Scottish Intercollegiate Guidelines Network's Reference Guide on Targeted p~ev;ention o~ dental caries in the
permanent teeth of 6-16 year olds presenting for dental care (2002).Available at http://www .sign.ac. uklg uideli nes/fulltext/4 7 /section3.html.Accessed on February. 18,20,06.
47 Ogard, 8., Seppa, L, Rolla, G.Professional topical fluoride applications-clinic~! efficacy and mechanism of action.Adv
Dent Res.1994 8: 19G-201.Available at: http:!/adr.iadrjournals.orglcgi/reprint/8/2/190. Accessed on January 21, 2006.
48 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States. August 2001/ VoL 50 I No. RR-14.Available athttp://www.cdc.gov/mmwr/PDF/rr/rr5014.pdf.Accessed on February 3, 2006.
49 Beltran-Agullar, Eugenio D., Goldstein, Jonathan W., Lockwood, Stuart A.Fluoride Varnishes: A Review of Their Clinical Use, Cariostatlc Mechanism, Efficacy and Safety .JAm Dent Assoc 2000 131: 589-596. Available at:
http://www.medscape.com/medline/publicationbrowser/6259/131_5/dt_050120001lirnit_5. Accessed on March 4, 2006. 50 Beltran-Aguilar, Eugenio D., Goldstein, Jonathan W., Lockwood, Stuart A.Fluoride Varnishes: A Review of Their Clinical Use, Cariostatic Mechanism, Efficacy and Safety.J Am DentAssoc2000 131: 589-596. Available at:
http://www.rnedscape.com/medline/publicationbrowser/6259/131_5/dt_05012000/limit_5. Accessed on March 4, 2006. 51 Hellwig, E., Klimek, J., Schmidt, H. F., Egerer, R.Fiuoride uptake in plaque-covered enamel after treatment with the fluoride lacquer Duraphat.J Dent Res 1985 64: 1080-1083. Available
at:htlp://jdr.iadrjournals.org/cgi/content/abstract/64/8/1 080.Accessed on February 11,2005.
52 Center for Disease ControL Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United
Fluoride Varnish 27
53 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States.-August 200'i I Vol. 50 I No. RR-14.p.18.Available athttp:/fwwv..o.cdc.gov/mmwr/PDF/rr/rr5014.pdfAccessed on February 3, 2006.
54 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental caries in the United States. August 2001 I Vol. 50 I No. RR-14.p. 19,21.Avaf!able athttp:/lwww.cdc.gov/mmwr/PDF/rrlrr5014.pdf.Accessed on February 3,2006.
55 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United States. August 2001/ Vol. 50 I No. RR-14. p. 24-25. Available at:http:/lwww.cdc.gov/mmwr/PDF/rr/rr5014.pdf.Accessed
on February 3, 2006.
56 Strohmenger, l., Brambilla, E. The Use of Fluoride Varnishes in the Prevention of Dental Caries: a Short Review.Oral Diseases. Volume 7 Issue 2 Page 71 - March 2001.doi:1 0.1 034/j.1601-0825.2001. 70202.x Available at:
http:/Jwww.systram.org/systematicreviews.Accessed on February 11,2006.
57 Bader,J, Rozier, G, Haris, R, Lohr, K .. Dental Caries Prevention: The Physician's Role in Child Oral HealthSystematic Evidence Review (2002).Agency for Healthcare Research and Quality.Contract #290-97-0011, Task Order No. 3.Technica! Support for the U.S. Preventive Services Task Force.Available at:
http://www.ahrq.gov/downloads/pub/prevent/pdfser/dentser.pdf. Accessed on March 1, 2006.
58 World Health Organization. Fluorides and oral health; WHO Expert Committee on Oral Health Status and Fluoride Use,
WHO Technical Report Series, 846, 1994. Available at: http://www.db.od.mah.se/car/datatfluoride.htmi.Accessed on February 4, 2006.
59 Head Start Bureau. (General Information). Available at http://lrWIIw2.acf.dhhs.gov/programs/hsb/about/index.htm.
Accessed on March 4,2006.
60 Early Head Start National Resource Center. Available at: http://ehsnrc.org/AboutUs!Jndex.htm. Accessed on: March 26,
2006.
61 Head Start Bureau. (General Information). Available at: http:l/lrWIIw2.acf.dhhs.gov/programs/hsb/about/index.htm.
Accessed on March 4,2006.
62 Lewis, C, Lynch, H, Richardson, L. Fluoride Varnish Use io Primary Care: What Do Providers Think? Pediatrics2005
115: e69-76 (doi:10.1542/peds.2004-1330).Available at:
http://pediatrics.aappublications.org/cgi!content/abstract/115/1/e69. Accessed ·an: February 21, 2006.
63 Lewis, C, Lynch, H, Richardson, L. Fluoride Varnish Use in-Rrimary Care. What Do. Providers Think? Pediatdcs2005
11-5: e69-76 (doi:10.1542/peds.2004-1330).Available at:
http://pediatrics.aappublications.org/cgi/content/abstract!115/1/e69. Accessed on: February 21, 2006.
64 SIGN. Scottish Intercollegiate Guidelines Network's Reference Guide on Targeted prevention of dental caries in the permanent teeth of 6-16 year olds presenting for dental care (2002). Available at http://www.sign.ac.ukfpdf/qrg47.pdf. Accessed on February 4, 2006.
65 National Institute of Health. Diagnosis and Management of Dental Caries Throughout Life, National Institutes of Health Consensus Development Conference Statement. March 26-28, 2001.Available at:
http:f/consensus.nih.gov/2001/2001Denta1Caries115html.htm. Accessed on: March 4,2006.
66 Center for Disease Control. Recommendations for Using Fluoride to Prevent and Control Dental Caries in the United
States. August 2001/ Vol. 50 I No. RR-14.p. 18.Available at:http://www.cdc.gov/mmwr/PDF/rr/rr5014.pdf.Accessed on
February 3, 2006.
67 Strohmenger, L, Brambilla, E. The Use of Fluoride Varnishes in the Prevention of Dental Caries: a Short Review. Oral Diseases. Volume 71ssue 2 Page 71 ~March 2001.doi:10.1034/j.1601-0825.2001.70202.x Available at
http://www.systram.org/systematicreviews.Accessed on February 11,2006.
68 Beltran-Aguilar, Eugenio D., Goldstein, Jonathan W., Lockwood, Stuart A.Fiuoride Varnishes: A Review of Their
Clinical Use, Cariostatic Mechanism, Efficacy and Safety.JAm Dent Assoc2000 131: 589-596. Available at
Fluoride Varnish 28
69 Castillo, J, Milgram, P.Fiuoride release from varnishes in two in vitro protocols.J Am Dent Assoc2004 135:
1696-1699.Avai!able at: hnp:/lcrobm.iad~ournals.org/cgi/contenVabstracV4/3/357. Accessed on February 4, 2006.
70 Seppa, L., Tuutti, H., Luoma, H. Post-treatment effect of fluoride varnishes in children with a high prevalence of dental
caries in a community with fluoridated water.J Dent Res 1984 63: 1221-1222. Available at:
http:/~dr.iadrjournals.org/cgi/reprint/6311 0/1221. Accessed on January 15, 2006.
71 National Maternal and Child Oral Health Resource Center. Child and adolescent oral health issues. 2004. Available at: http://www.mchoralhealth.org/PDFsllssues.pdf. Accessed on March 4, 2006.
72 Center for Disease ControL State Oral Health Plans. February 2006. Available
athttp://www.cdc.gov/oralhealth/state_reports/OH_planslindex.htm. Accessed on March 4, 2006. 73 Center for Disease Control. Infrastructure Development Tools, Activity 3:State Oral Health Plan Available at: http://www.cdc.gov/oralhealth!library/activity3.htm. Accessed on February 18,2006.
74 Turnock,B. Public Health: What It Is And How It Works, 2nd ed. Sudbury, Mass:Jones and Bartlett Publishers; 2001,
p.177.
Fluoride Varnish 29
Tables
Table 1. Caries Risk Assessment Tool
f\.10 nrlw~ teeth in
jtMt 24 ttl<:fUhs
r-.w HMmd dmbirwn!iz.ltkm
{erumri cJii>!$ "'vihitt-->{Xltimklrn}
Erwin:mt:tWJIIA! thm~«lHhdn
* Or,t!nr;,l r;shHnk Jnd
tq:;kal nu(}rklt m:pmm•t§
~ C.:.n$1lrnpt-k>n <>f simp.le ;ups
or f=ds nrongty ;mod;;k'<'l
with c,1rW5 inltk'!tkm
prirrwrily ~r nwaltin\>.'sl! High -C$<1ginrr mciote.c'rnromlc ~tilttr.1f
~ Rf.gqbr u·w of •.kntal caro
ln m r~ublh!wcl drnull'>>llW
(:.,rk:>u~ tN>Ih Jn t~
J)J<t 24 nmn!hs
l :~ua of tlumd -(;k,mio~mJiwtion
(crhlmcl qfi(f~ ~whitiNpot lni;::ll'ls")
• C:.rbt~S t&&lh i!1 dw
I)Ml 12: lt\tifldU
~ i'l>fm'i! d!.ln 1 :lNl of ermrwl
deminer.:lliz::.l:ion (m:mwl
c.::.ries ~whit<:-${Xit !ts!on() • Vbibk-p.Ji!que on ;10l<irk>r
(front) !>!Cih
· Radli-'itf-iW!ik'd:l.Jmd a1rfe~ Hi&h i:lNro o(
w"·'"""
~wvtocc=iI
\li<?¥ing<:kmw.1 m il'fthot.k>ntk;lpp!brue~!
En.:untl hy~•opLill.J·t
~ S..th<:;pthtl:lhpt~nd<: fiuodde .;,XJX11ll<"' • Sutw:optirm!l topk,~t
wl1h optiti11ll u:.pkal eXj:litiUI"l'§ lkwrkle t:~;poslln'1§ ~ Ckal\ionul {1<\ J~Zi iM:IVCI':!H'IWJ!
;;,xp.'JSlJWS w 5impk }tl:lJTS or f;;;.:dt $t!Vngi'j ~S>PC!JWd Wilh PrW~
• t\4\dk.vJ GW\'gi>tcr
wdfN(UIWfllic M;~h%
\k, di;;jb!"" for <~:hocl
lunth progntn or SCHif')
Ir~lilf w:.-d -:knt;:~J Si'rvk,_;s
Fn•qt"'nt (W, 3 ormonl) bctV;U'OINY,:,:tJ CXj:O$UfM
lo simple sug.Jx:Sor roods
s!-rongl;• ;w~<:o:i.1tt:cl with <:Jfi~
• l,(')w·!<"<vl <Amghtr KXk·KCilt>JUjC \Wll!!> (k. d\-1.,\lbk for lvkdit,)iJ)
• (h!ldrun wi!h 5J)tdJI htJtth
{"<ln'~(k#
• Conditions ifilp.:iir!t~i;s.:!U•;;~
wmpt&ition/floN••
Source: American Academy of Pediatric Dentistry. Policy on Use of a Caries-risk Assessment Tool (CAT) for Infants, Children, and Adolescents. 2002.Available at:
Fluoride Varnish 30
Table 2. Fluoride Varnishes
Varnish Formulation Manufacturer Comments
Fluor-Protector 0.1% Ivoclar North
difluorosilane in a America-Vivadent
polyurethane base 1-800-327-4688
V arnishAmerica 5% NaFin a Medical Products Available in a
natural Laboratories, Inc. unit-dose
colophonium 1-800-523-0191, with an
resin Ext326 applicator
AI1Solutions 5% NaF in a Dentsply Available in a
natural resin Professional unit-dose with
1-800-989-8826 an applicator
Vanish 5% NaF in a Omni Products Available in a
natural 1-800-445-3386 unit-dose with
colophonium an applicator
resin
Durafluor 5% NaF in a Medicom natural
colophonium 1-800-435-9267
resin
Duraphat 5% NaF in a Colgate Oral
natural Pl)armaceuticals
colophoniurn 1-800-225-3756
resm
1-800-2-COLGATE
Sources:
Fluoride Varnish Manual. February2005.Nevada State Health Division( Oral Health Program).Available at: http:/lh.ealth2k.state.nv.usloraVFVManual.pdf. Accessed February II ,2006.
Bittke,D. Fluoride varnishes: A new kind of disappearing act. RDH. February 2006.Available at: http :1/rdh.pennnet.com/ Articles/ Article_ Display.cfm? ARTICLE_ ID=247527 &p=56.
Accessed on March !4, 2006.
' '
Fluoride Varnish 31
Table 3: CDC Fluoride Grading System
CDC Grading system used for determining the quality of evidence for a fluoride
modality
Grade Criteria
I Evidence obtained from one or more properly conducted randomized
clinical trials (i.e., one using concurrent controls, double-blind design,
placebos, valid and reliable measurements, and well-controlled study
protocols).
11-1 Evidence obtained from one or more controlled clinical trials without
randomization (i.e., one using systematic subject selection, some type
of concurrent controls, valid and reliable measurements, and wellcontrol!ed
study protocols).
11-2 Evidence obtained from one or more well-designed cohort or case-control
analytic studies, preferably from more than one center or research group.
11-3 Evidence obtained from cross-sectional comparisons between timeS and
places; studies with historical controls; or dramatic results in uncontrolled
experiments (e.g., the results of the introduction of penicillin treatrTient in
the 1940s).
Ill Opinions of respected authorities on the basis of clinical experience,
descriptive studies or case reports, or reports of expert committees.
Source: US Preventive Services Task Force. Guide to clinical preventive services. 2nd ed.
Alexandria, VA: International Medical Publishing, 1996. Available at:
Fluoride Varnish 32
Table 4. CDC Fluoride Coding System
Coding system used to classify recommendations for use of specific fluoride
modalities to control dental caries
Code Criteria
A Good evidence to support the use of the modality.
B Fair evidence to support the use of the modality.
C Lack of evidence to develop a specific recommendation (i.e., the modality
has not been adequately tested) or mixed evidence {i.e., some studies
support the use of the modality and some oppose it).
0 Fair evidence to reject the use of the modality.
E Good evidence to reject ·J:he use of the modality.
I