Perceptions
of Vulnerability
31/2
Years
After
Problems
of Feeding
and Crying
Behavior
in
Early
Infancy
Brian
W.C.
Forsyth,
MF, ChB,
FRCP(C),*
and
Priscilla
F. Canny,
PhDf
From the *Depa,.ment of Pediatrics and epartment of Epidemiology and Public Health,
Yale University School of Medicine, New Haven, Connecticut
ABSTRACT. The long-term consequences for infants with problems of feeding and crying behavior remain unknown. The purpose of this research was to determine whether such children are later perceived by their parents as vulnerable and more often have behavior problems and have different personalities than children without problems in infancy. The implications of managing such problems by changing milk formulas is explored. Mothers of 379 infants were enrolled in the postpartum period.
Information about problems of feeding and crying
behav-ior was obtained at 4 months. Thirty-six percent of the infants had problems and the formula had been changed
for 17%. At 3#{189}years, 320 (84%) mothers completed a
questionnaire. Children who had had problems were more often perceived as vulnerable (relative risk ERR] 1.86;
95% confidence interval [CI] 1.09, 3.19) and more often had behavior problems (RR 1.78; 95% CI 1.03, 3.07). There were no differences in personality. Children whose problems had been managed by changing milk formulas were more often perceived as vulnerable (RR 2.18; 95% CI 1.05, 4.53). Although allergies were reported signifi-cantly more often for those children who had had prob-lems, there were no differences in the prevalence of asthma or eczema. Problems of feeding and crying
behav-ior in early infancy and the way they are managed may have long-term implications for the child. Pediatrics
1991;88:757-763; infancy, feeding, crying, behavior,
vul-nerability, parental perceptions.
ABBREVIATIONS. RR, relative risk; CI, confidence interval; OR,
odds ratio.
Received for publication Jan 18, 1990; accepted Sep 18, 1990.
Reprint requests to (B.W.C.F.) Dept of Pediatrics, Yale
Univer-sity School ofMedicine, 333 Cedar St. P0 Box 3333, New Haven,
CT 06510-8064.
PEDIATRICS (ISSN 0031 4005). Copyright © 1991 by the
American Academy of Pediatrics.
Problems of feeding and crying behavior such as excessive fussiness and spitting occur commonly in early infancy.’ Although often regarded as of little consequence to the immediate health and well-being of the child, these problems often are of great concern to parents. A number of authors have sug-gested that these types of problems and the way in which they are managed might have long-term im-plications for the child. Solnit and Provence,2 citing complaints such as irritability, colic, spitting, and food intolerance, suggested that the way the parents and physicians respond to the problem can deter-mine whether it becomes a mild or severe burden on the child’s psychological development. Taitz3 has expressed the opinion that in such cases the overdiagnosis of cow’s milk hypersensitivity is a more serious threat than its underdiagnosis in that it may have potential “long term effects on the child’s rearing.” Warner and Hathaway4 have sug-gested that concern about milk allergy may result in an “allergic child syndrome” in which the original problem is short-lived but other nonrelated symp-toms later in life may reawaken concerns about allergy.
The first few months after the birth of a child is a formative period for both the parents and their child. During this period, parents develop feelings about their child’s personality, behavior, and strengths and weaknesses. This period, therefore, is logically a time in which any untoward events
In this research we consider whether problems of feeding and crying behavior in early infancy and the approach taken to managing these problems can affect the parents’ perceptions of their child’s vulnerability. As has been described in the vulner-able child syndrome, parents who view their child as vulnerable may develop an overprotective rela-tionship that has adverse effects on the child’s psychological development.5
This report focuses on the long-term outcomes for children previously described in a study of in-fants observed prospectively over the first 4 months of infancy.”6 Thirty-five percent ofthe infants were reported by their mothers to have problems of feeding or crying behavior that were considered to be of at least moderate severity. In that study it was found that mothers of first-born infants and mothers with less education more frequently re-ported problems.
A substantial proportion of the infants had their milk formulas changed to non-cow’s milk-contain-ing formulas. Compared with those with problems but no change of formula, the infants who received a change of formula were more often viewed by their mothers as having something intrinsically wrong (eg, milk allergy).
STUDY
HYPOTHESES
The hypotheses of this study are the following: first, that children with problems of feeding and crying behavior in infancy are later more likely to be perceived as vulnerable and are more likely to have behavior problems and different personalities than those who did not have problems in infancy; second, when the problem in infancy is managed by changing the milk formula, children are even more likely to be perceived as vulnerable; and third, children with problems of feeding and crying be-havior in infancy continue to be considered allergic years later.
METHODS
This study includes children observed prospec-tively from birth to the age of 3#{189}years. Eligible study subjects included singleton children born at Yale-New Haven Hospital (CT) between July and October 1980. Subjects were recruited from the well-baby nursery and were enrolled in the study after informed consent was obtained from their mothers. Only children who were to be followed up by pediatricians in private practice were included; children who were admitted to the newborn special care unit were excluded. We enrolled all formula-fed neonates, but only those breast-fed neonates who were born on the first 3 days of each week.
This strategy allowed us to enroll approximately equal numbers of formula-fed and breast-fed neo-nates from a population in which breast-feeding predominated. Pediatricians were aware that chil-then were being enrolled in a study investigating “feeding problems” but neither they, nor the moth-ers, were aware of the exact purpose of the study.
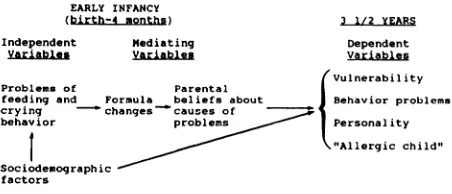
An overview of the study design and the variables measured are shown in Fig 1. Sociodemographic data were collected in a baseline questionnaire com-pleted by study mothers in the postpartum period prior to discharge from the hospital. When the infants were 4 months old, a structured telephone interview was conducted by one of the researchers (B.W.C.F.) to obtain information on the presence and severity of problems of feeding and crying behavior, the mothers’ beliefs about the causes of the problems, and information about all changes of formula. For the purpose of analyses, only problems considered by mothers to be “real” problems and either “moderate” or “severe” were categorized as problems. Formula changes were only those where there was a change from a cow’s milk formula to a soy protein or casein hydrolysate formula.
A mother’s belief about the cause of the problem was categorized as intrinsic when she believed that her infant had a biological abnormality such as milk allergy. In other instances, mothers believed that problems were behavioral or they identified extrinsic factors, such as an infection or something to do with the feeding process.
When subjects were aged 3#{189}years, a question-naire was mailed to all mothers. This questionnaire obtained information about the child’s behavior and personality and maternal perceptions of the child’s vulnerability. Additional information about the child’s health status and use of health care was obtained and changes in the mother’s marital status and number of children were noted.
Measures
of Vulnerability,
Behavior,
and
Personality
The Child Vulnerability Scale was designed spe-cifically for this research to measure parents’ per-ceptions of their children’s vulnerability. It is a
10-EARLY INFANCY
(birth-4 onthst 3 112 YEARS
Independent Mediating Dependent
Variables Variables Variables
(Vulnerability
Problems of Parental I
feeding and Formula beliefs about I Behavior problems crying changescauses of
behavior problems
I
PersonalityI
‘%,“Allergic child”Sociodemographic
factors
item questionnaire that measures general concerns about health as well as specific concerns that have been noted in the vulnerable child syndrome (Table
1). For each of the 10 items the mother is asked to check one of three statements that best describes her child. Each item is scored as 0, 1, or 2, resulting in a total score between 0 and 20. Vulnerability is considered a dichotomous, rather than a continu-ous, variable because of the underlying theoretical concept that a child is either perceived by the parent as abnormally susceptible to illness (and possibly death) or is considered average and nor-mal. In this study, a child with a score greater than one standard deviation above the mean was cate-gorized as a vulnerable child. (For more information about an updated version and scoring of the Child Vulnerability Scale, contact the first author.)
The child’s behavior was measured using the Richman Behavior Checklist, an instrument adapted from the Behavior Screening Question-naire for use by parents. The checklist measures 12 different behaviors and provides a score between 0 and 24, with a score of 10 or above indicating a significant behavior problem.7 The validity and re-liability of both the questionnaire and checklist have been demonstrated in earlier studies.7#{176}
The Cohen Child Personality Scale is a 20-item questionnaire that provides a score for five different areas of personality: the ability to pay attention, modulation of behavior, sociability, zestfulness, and verbal expressiveness. Reports on the reliability and validity of this instrument have been published
by the authors of the scale.”2
Statistical
Methods
We first conducted bivariate analyses to deter-mine associations between dependent and inde-pendent variables and then conducted multivariate analyses to determine the relative effect of possible confounding sociodemographic factors. The relative risk (RR) and 95% confidence intervals (CIs) were calculated as described by Rothman.’3 We used
x2
and t test analyses for bivariate comparisons. De-pending on the nature of the dependent variable,TABLE 1. Items in the Child Vulnerability Scale
Gets sick more easily than other children. Parent often thinks about calling the doctor. Child often kept indoors because of health reasons. Has more accidents than other children.
Parent often checks on child at night. Doesn’t eat enough.
Doesn’t look well. Circles under the eyes.
Has less energy than other children.
Parent concerned about child’s stomach pains.
multiple regression or logistic regression analyses were used to assess the relative effects of independ-ent variables. Odds ratios (OR) calculated from logistic regression j3 coefficients were considered approximations of the RR.
RESULTS
Of 487 mothers invited to participate in the study, 379 (78%) completed the baseline question-naire and were enrolled. Three hundred twenty mothers (84% of those enrolled) completed the follow-up questionnaire when the children were 3#{189} years old. Of those mothers who completed the study, 95% were white, 57% had more than a high school education, 49% had family incomes greater
than $20 000, and 89% were married. Forty-five percent of the children were first-born children. The mean maternal age at follow-up was 31.7 years. Thirty-six percent of the children were considered by their mothers to have problems of feeding and crying behavior by 4 months of age. Fifty-five (17% of all infants) had had their formulas changed from a cow’s milk formula to a soy protein or casein hydrolysate formula; 43 of these changes were for problems of feeding and crying behavior. Children who were lost to follow-up at 3#{189}years had had similar rates of problems and changes of formula in early infancy as those completing follow-up.
At 3#{189}years of age, 45 (14%) of the 320 children were classified as vulnerable on the Child Vulner-ability Scale. Because this scale is a new instru-ment, the data were examined for evidence to sup-port its validity in identifying children perceived to be vulnerable. Compared with children categorized as nonvulnerable, vulnerable children were re-ported to have had more health care visits in the preceding year (4.04 vs 2.11, P < .0001), and the parents had phoned the pediatrician more fre-quently (4.18 vs 2.26, P < .0001). Twenty-seven percent of mothers of children categorized as vu!-nerable had at some time feared that their child might die, compared with only 8% of those mothers of children categorized as not vulnerable (P <
.0005).
Of the 320 children, 44 (14%) had a score of greater than 10 on the Richman Behavior Checklist and were categorized as having a behavior problem. Although there was a significant relationship be-tween vulnerability and behavior problems (P =
rio ii10100.iM
I1 ‘2051
l PROBLEM
110 formula
change lN”721
iFloilI.F.M
Cli.’xn(io of
fornu 1a
I N=4 11
Association Between Problems of Early Infancy and Outcomes at 31/2
Years
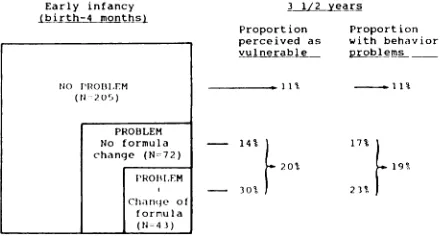
As shown in Fig 2, 20% of children who had had problems of feeding and crying behavior in early infancy were reported as vulnerable at 3#{189}years compared with only 1 1 % of those who had no problems in early infancy (RR 1.86; 95% CI L09, 3.19). Similarly, children who had had problems in early infancy more often had behavior problems at the time of follow-up (19% vs 11%, RR 1.78; 95% CI 1.03, 3.07).
To explore the possibility that sociodemographic characteristics might account for these associa-tions, we first determined whether mothers who perceived their children as vulnerable might have significantly different sociodemographic character-istics from mothers who did not report their chil-dren as vulnerable. In fact, mothers who viewed their children as vulnerable tended to be younger (P < .005), single (P < .01), and their family in-comes were lower (P < .05). Perceptions of vulner-ability were not significantly related to the level of maternal education or to the child’s gender or birth order. Because the study group was 95% white, the effects of race could not be fully evaluated. Similar analyses were performed to determine the associa-tion between sociodemographic characteristics and behavior problems. Behavior problems were re-ported more frequently by single mothers (P < .05), but there were no significant associations with other sociodemographic variables. However, when the effects of sociodemographic characteristics were controlled using logistic regression analyses, there continued to be significant independent associa-tions between problems of feeding and crying be-havior in early infancy and perceptions of vulner-ability (OR 2.24; 95% CI 1.12, 4.47) and behavior problems (OR 2.04; 95% CI 1.03, 403) at 3#{189}years.
To assess the association between problems of feeding and crying behavior in early infancy and the five personality characteristics at 3#{189}years, the personality scores of those children with and
with-Early infancy
(birtto-4 months)
3 1/2 years
Proportion Proportion perceived as with behavior
vulnerable ppfems
.
uT -.01%- 14%
F
- 30% 1
17%
F
09%20%
J
Fig 2. Outcomes at 3#{189}years after problems of feeding
and crying behavior and formula changes in early infancy.
out problems in early infancy were compared. Chil-dren with problems in early infancy appeared to
have significant increases in behavior modulation (P < .05) and a decrease in their ability to pay attention (P < .05), but when the effects of con-founding sociodemographic factors were explored using multiple regression analyses, these
associa-tions were no longer statistically significant.
Associations Between Formula Changes in Infancy and Outcomes at 31/2 Years
Of the 115 children reported to have problems of feeding and crying behavior in early infancy, 43 (37%) had had their formula changed to a
soy-based or casein hydrolysate formula by 4 months of age. At 3#{189}years of age, 13 (30%) of the 43 children who had had their formula changed were perceived as vulnerable compared with only 10 (14%) of the 72 children who had had problems in
infancy but had not had their formula changed (RR 2.18; 95% CI 1.05, 4.53) (Fig 2). Mothers who had believed that the cause of the problem in early infancy was an intrinsic abnormality were nearly twice as likely to view their child as vulnerable at the age of 3#{189}years (30% vs 16%), although this increased risk was not statistically significant (RR 1.94; 95% CI 0.93, 4.05). Although perceptions of vulnerability were increased for those children who in early infancy had had formula changes or had
been viewed as having an intrinsic abnormality, there was no significant increase in reports of be-havior problems for these children.
Reports
of Allergies
at
31/2 YearsAt the 3#{189}-year follow-up, mothers whose
chil-dren had had problems in early infancy more fre-quently reported their children to be allergic to milk and to have other allergies although these
children had no significant increase in asthma or eczema (Table 2). Allergies, asthma, and eczema were not reported any more frequently for those
infants who had had their formula changed.
DISCUSSION
In 1964, Green and Solnit5 published their land-mark article describing the vulnerable child
syn-drome in which children who had recovered from a near death experience in early childhood were later falsely perceived by their parents to be at increased risk of illness or accident. This abnormal perception of the child causes the parents to relate to the child in an overprotective manner and results in
TABLE 2. Association Between Problems of Feeding
and Crying Behavior in Early Infancy and Reports of
Allergies at 3#{189}Years
Allergic % With Allergies P
Manifestation
at3’/2y
at 3#{189}y
Children With Children Problems in Without Infancy Problems (n
=
115) in Infancy(n
=
205)Milk allergy 8.70 0.49 <.0005
Other allergy 18.26 9.27 <.05
Asthma 1.74 4.39 NS*
Eczema 8.70 5.37 NS*
* Not significant.
A number of other authors have described in-stances in which a less severe event than the threat-ened death of a child have had similar, although perhaps less severe, consequences on the parents’ perceptions of their child’s vulnerability and on the behavior of their child.34”9 These have included descriptions of the long-term psychological effects of false-positive screening tests for phenylketonu-na, severe gastroenteritis, and the birth of a child prematurely.14’6
In another type of study, Levy20 evaluated per-ceptions of vulnerability of parents who brought their children for medical care. She reported that 27% of parents viewed their child as uniquely threatened by an episode of illness, although for 40% of this group of children who were considered vulnerable, there was no clinical basis for their concerns. In Levy’s study, the classification of vu!-nerability depended on the parents’ responses to a single question: “Do you have special worries about the child’s health or feel the need for extra cautious-ness?” Assessing vulnerability by using a response to this single question neither allows for variations in the degree of concern nor does it take into account that parents may worry about their chil-dren without viewing them as abnormally suscep-tible to illness.
The Child Vulnerability Scale was developed to measure the degree to which parents share the same specific concerns about their children as reported in descriptions of the vulnerable child syndrome. The scale, however, is intended only to provide a measure of perception of vulnerability and not to categorize a child as having the “vulnerable child syndrome,” which, by definition, includes behav-ioral abnormalities. Interestingly, only one third of those children categorized as vulnerable also had behavior problems at 3#{189}years.
Although the scale has not been fully validated, some construct validity is provided by the fact that those children who were categorized as vulnerable
were taken to the doctor significantly more often and 27% of their mothers reported that they at some time had feared that their child might die. This earlier fear of death of the child is one of the hallmarks of the vulnerable child syndrome. It is a
limitation of the study, however, that, because all data were obtained from mothers’ reports, we are unable to differentiate between those children who are truly ill and vulnerable from well children for whom the problem is purely the parents’ perception.
Our finding that perceptions ofvulnerability were increased among younger mothers, mothers who were single, and mothers with less income is not surprising, given that these characteristics indicate a more stressful environment. Levy20 found that vulnerability was more often reported for children receiving Medicaid than for those with third-party insurance. The subjects in the present study rep-resent a predominantly white population attending pediatricians in private practice. It is unknown whether the same results would be found in other population groups.
As hypothesized, we found that children who had problems of feeding and crying behavior in infancy were significantly more likely at 3#{189}years to be viewed as vulnerable, but interestingly, it was those who had had a change of formula who contributed most to this difference. It is important to note, in
fact, that those who had problems but no formula change had no significantly increased risk of vu!-nerability when compared with those with no
prob-lems (14% vs 11%). Thus, the formula change ap-pears to be a more potent factor than the problem in affecting later perceptions of vulnerability. It should be recognized, however, that the change of formula is not an isolated factor but is more likely a marker for the overall way in which the physician managed the problem and explained it to the par-ents. Certainly, when the formula is changed, there is at least the implication that the infant is allergic to or in some way intolerant of the formula. Also, in some instances parents may have preset beliefs that there is something intrinsically wrong with
their infant and request a change of formula. The change of formula may not necessarily cause par-ents to later view their child as vulnerable, but the results of this research suggest that it is at least a reinforcing factor.
The prevalence of behavior problems in this pop-ulation (14%) was similar to that found in other
the fact that perceptions of vulnerability and be-havior problems are not always interrelated.
The fact that children with problems in infancy did not have significantly different personalities at 3#{189}years also is important. This speaks to the fact that children with this type of problem in early infancy are not constitutionally different, at least not in any way that is long lasting.
As was expected, children with problems in in-fancy were, at 3#{189}years, more often considered to have allergies. It should be noted, however, that the manifestations of allergy that can be diagnosed with
greater certainty, such as asthma and eczema, were not found significantly more often among these children. However, in contradiction to Warner and Hathaway’s4 suggestion that a focus on dietary approaches to management might have long-lasting effects on beliefs about allergies, the parents of those who had their formulas changed to a
non-cow’s milk formula were not more likely to consider their child allergic.
IMPLICATIONS
Although problems of feeding and crying behav-ior in early infancy are self-limited and often con-sidered by clinicians to be of little consequence, they may have more serious long-term implications
for the child and parents and the approach taken by the clinicians to the management of the problem may modify these long-term effects. Studies have shown that supportive approaches used in the man-agement of more serious problems of early infancy such as premature birth have fairly dramatic effects on decreasing both psychological sequelae and sub-sequent excessive use of health care.2’ It would seem logical that for problems of feeding and crying
behavior, an approach could be taken that would decrease perceptions of vulnerability. Such an ap-proach might include recognizing and addressing the concerns of the parents while identifying the problem as self-limited-without the suggestion that the child is allergic or has other intrinsic abnormalties.
It has been shown that for some infants with colic, changing to a non-cow’s milk formula leads to a decrease in crying.22’23 However, even for these infants, the pattern of response is not one of a!-lergy.23 Thus, even with infants who do respond to such a change, returning to the original cow’s milk formula at a later date and an explanation that the problem is self-limited with no long-lasting medical implications might have an important effect on
decreasing perceptions of vulnerability.
In this study we have not addressed the issue of how to help those children who are already
per-ceived as vulnerable. It is hoped, however, that this
focus on parental perceptions of vulnerability and the precedents that affect these might lead clini-cians to recognize children who are regarded as vulnerable and focus their management appropri-ately. Further development and use of the Child Vulnerability Scale in research should provide a
greater knowledge of factors that affect parental perception of vulnerability and the ways in which they can be modified.
ACKNOWLEDGMENTS
We are grateful to Donna Torcia for her assistance in conducting this research and her extensive efforts in tracing subjects. We thank Drs John Leventhal, Eugene Shapiro, and Sarah Horwitz for providing critical review of the manuscript.
REFERENCES
1. Forsyth BWC, Leventhal JM, McCarthy PL. Mothers’ per-ceptions ofproblems of feeding and crying behaviors. AJDC.
1985;139:269-272
2. Solnit AJ, Provence S. Vulnerability and risk in early
child-hood. In: Osafsky JD, ed. Handbook of Infant Development.
Philadelphia, PA: John Wiley & Sons; 1979:799-808
3. Taitz LS. Soy feeding in infancy. Arch Dis Child.
1982;57:814-815
4. Warner JO, Hathaway MJ. Allergic form of Meadow’s
syn-drome (Munchausen by proxy). Arch Dis Child.
1984;59:151-156
5. Green M, Solnit AJ. Reactions to the threatened loss of a child: a vulnerable child syndrome. Pediatrics. 1964;34:58-66
6. Forsyth WBC, McCarthy PL, Leventhal JM. Problems of early infancy, formula changes and mothers’ beliefs about
their infants.J Pediatr. 1985;106:1012-1017
7. Richman N. Is a behavior checklist for pre-school children
useful? In: Graham PJ, ed. Epidemiological Approaches in
Child Psychiatry. New York, NY: Academic Press Inc;
1977:125-137
8. Richman N, Graham PJ. A behavioral screening question-naire for use with three-year-old children: preliminary find-ings. J Child Psychol Psychiatry. 1971;12:5-33
9. Richman N, Stevenson JE, Graham PJ. Prevalence of
be-havior problems in 3-year-old children: an epidemiological study in a London borough. J Child Psychol Psychiatry.
1975;16:277-287
10. Earls F. The prevalence of behavior problems in 3-year-old children: comparison of the reports of fathers and mothers.
JAm Acad Child Psychiatry. 1980;19:439-452
11. Dibble E, Cohen DJ. Companion instruments for measuring children’s competence and parental style. Arch Gen Psy-chiatry. 1974;30:805-815
12. Cohen DJ, Dibble E, Grawe JM. Fathers’ and mothers’
perceptions of children’s personality. Arch Gen Psychiatry.
1977;34:480-487
13. Rothman KJ. Modern Epidemiology. Boston, MA: Little,
Brown & Co; 1986:170-175
14. Rothenberg MB, Sills EM. latrogenesis: the PKU anxiety syndrome. J Am Acad Child Psychiatry. 1968;7:689-692 15. Sigal J, Gagnon P. Effects of parents’ and pediatricians’
worry concerning severe gastroenteritis in early childhood
on later disturbances in the child’s behavior. J Pediatr.
1975;87:809-814
17. Sigal JJ, Chagoya L, Villeneuve C, Mayerovitch J. Later
psychological sequelae of early childhood illness (severe
croup). Am J Psychiatry. 1973;130:786-789
18. Hampton ML, Anderson J, Lauizzo BS, Bergman AB, Sickle
cell “nondisease.” AJDC. 1974;128:58-61
19. Carey WB. Psychologic sequelae of early infancy health
crisis. In: Swartz JL, Swartz LH, eds. Vulnerable Infants: A
Psychosocial Dilemma. New York, NY: McGraw-Hill Book
Co; 1977:195-202
20. Levy JC. Vulnerable children: parents’ perspectives and the
use of medical care. Pediatrics. 1980;65:956-963
21. Perrault C, Coates AL, Collinge J, Pless IB, Outerbridge E.
Family support system in newborn medicine: does it work?
Follow-up study of infants at risk. J Pediatr. 1986;108:1025-1030
22. Lothe L, Lindberg T. Cow’s milk whey protein elicits
symp-toms of infantile colic in colicky formula-fed infants: a
double-blind crossover study. Pediatrics. 1989;83:262-266
23. Forsyth BWC. Colic and the effect of changing milk
for-mulas: a double-blind, multiple-crossover study. J Pediatr.
1989;115:521-526
N.Y.
BANS
DWARF
TOSSING
IN BARS
ALBANY, N.Y.-Gov. Mario Cuomo signed legislation Tuesday banning dwarf tossing and dwarf bowling in New York bars, calling the activities a “strange diversion.”
“Any activity which dehumanizes and humiliates these people is degrading to us all,” Cuomo said. “This bill recognizes that and, in effect, declares these bizarre games to be debased.”
Dwarf tossing is a competition in which people pick up dwarfs, who are wearing harnesses, and heave them as far as possible at a padded target. It produced an offshoot, dwarf bowling, in which a helmeted dwarf is strapped to a skateboard and rolled into bowling pins. Both have been held as competitions for cash prizes, Cuomo said.
N.Y. bans dwarf tossing in bars. The Burlington Free Press. July 24, 1990.
1991;88;757
Pediatrics
Brian W.C. Forsyth and Priscilla F. Canny
Behavior in Early Infancy
Perceptions of Vulnerability 3½ Years After Problems of Feeding and Crying
Services
Updated Information &
http://pediatrics.aappublications.org/content/88/4/757
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
1991;88;757
Pediatrics
Brian W.C. Forsyth and Priscilla F. Canny
Behavior in Early Infancy
Perceptions of Vulnerability 3½ Years After Problems of Feeding and Crying
http://pediatrics.aappublications.org/content/88/4/757
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.