Julia Kruk-Jeromin, Aleksandra Iljin
Polymorphism of Van der Woude Syndrome
and Its Symptom Intensification
in Subsequent Generations
Polimorfizm zespołu van der Woude i ekspansywność objawów
w kolejnych pokoleniach
Department of Plastic, Reconstructive and Aesthetic Surgery, Medical University of Lodz, Poland
Abstract
Background. Van der Woude syndrome is characterized by such developmental malformations as lower lip sinus-es/fistulas and cleft lip and/or palate. The etiology of the syndrome is probably linked to a mutation or deletion in chromosome 1q32-q41 or 1p34. Symptomatic treatment is based on surgical repair of the cleft lip and/or palate and excision of sinuses/fistulas of the lower lip.
Objectives. This is an analysis of 23 cases with van der Woude syndrome considering the pathomorphology, therapy, polymorphism, and the intensification of symptoms in successive generations.
Material and Methods. Twenty-three individuals (15 girls and 8 boys) with van der Woude syndrome treated at the Department of Plastic, Reconstructive and Aesthetic Surgery of the Medical University of Lodz between 1972–2007 were the subjects of the study. Etiopathogenesis, syndrome components, coexistence of other congenital malformations, and increasing symptoms in families with van der Woude syndrome were analyzed.
Results. Of 21 patients with the complete (sinuses and cleft) and 2 with the incomplete form (only sinuses) of van der Woude syndrome, 6 had other congenital malformations of the face, sexual organs, nervous system, bones, heart, feet, or abdominal integument. A hereditary background was confirmed in 10 cases. Lower lip sinuses were usually double and symmetrically distributed. Surgical repair was successful in 18 patients with lower lip sinuses and deformities and in 21 persons with cleft lip and/or palate.
Conclusions. Lower lip sinuses may accompany any form of cleft lip and/or palate. Van der Woude syndrome is more prevalent in females and carried mainly by mothers. Escalation of coexisting malformations can be expected in subsequent generations of families with van der Woude syndrome. Genotypic studies presented in the literature suggest the occurrence of genetic aberrations responsible for van der Woude syndrome inheritance confirmed by clinical observations (Adv Clin Exp Med 2010, 19, 1, 77–81).
Key words: van der Woude syndrome.
Streszczenie
Wprowadzenie. W skład zespołu van der Woude wchodzą anomalie rozwojowe w postaci zatok/przetok wargi dol-nej oraz rozszczep wargi i/lub podniebienia. Etiologia zespołu prawdopodobnie jest związana z mutacją lub delecją genu IRF6 znajdującego się na chromosomie 1q32-q41 lub 1p34. Leczenie objawów zespołu polega na chirurgicznej rekonstrukcji rozszczepionej wargi i/lub podniebienia oraz wycięciu zatok/przetok i plastyce wargi dolnej.
Cel pracy. Analiza 23 przypadków zespołu van der Woude pod względem patomorfologii i terapii oraz polimorfiz-mu zespołu i nasilenia jego objawów w kolejnych pokoleniach.
Materiał i metody. Badaniem objęto 23 osoby z zespołem van der Woude (15 dziewcząt, 8 chłopców) leczo-nych w Klinice Chirurgii Plastycznej, Rekonstrukcyjnej i Estetycznej UM w Łodzi w latach 1972–2007. W badanej grupie analizowano etiopatogenezę, składowe zespołu, współistnienie innych wad rozwojowych, a także narastanie zaburzeń w rodzinach z tym zespołem.
Wyniki. Wśród 21 osób z pełną (zatoki i rozszczep) i 2 osób z niepełną (tylko zatoki) postacią zespołu van der Woude 6 dzieci miało także inne wady wrodzone twarzy, narządów płciowych, układu nerwowego, kostnego, serca, stóp lub powłok brzucha. Czynniki dziedziczne odpowiadały za wystąpienie zespołu w 10 przypadkach. Zatoki wargi dolnej najczęściej były podwójne i symetrycznie rozmieszczone. Ostateczny wynik chirurgicznego leczenia
Adv Clin Exp Med 2010, 19, 1, 77–81 ISSN 1230-025X
ORIGINAL PAPERS
Van der Woude syndrome is characterized by such developmental malformations as cleft lip and/or palate and sinuses/fistulas of the lower lip (Fig. 1). Cleft lip and/or palate is one of the ten most frequent congenital malformations and affects 2 in 1000 living newborns [1]. It may be manifested either by cleft upper lip, cleft lip and alveolar process, isolated cleft of the hard and/ or soft palate or a complete lip, cleft alveolar pro-cess, and cleft palate. The malformation occurs uni- and bilaterally. A complete unilateral cleft lip and palate and an isolated cleft palate are the pre-dominant forms [2]. The etiopathogenesis of the defect has not been clearly explained. Apart from genetic agents (17–20%), environmental factors are believed to play an important role.
There are two different genetic patterns responsible for cleft lip and/or palate and isolat-ed palate cleft development [3]. Lower lip sinuses (also known as fistulas and pits) occur rarely as an isolated malformation. They are believed to be transmitted in an irregular dominant fashion [4]. Ann Van der Woude described the coexistence of a cleft with lower lip fistulas in 1954, suggest-ing autosomal dominant transmission. The first description of a family showing such coexisting malformations was provided by Demarquay in 1845 [5].
There are descriptions of hundreds of persons with this syndrome presented as case studies or analyses of larger patient groups in the literature [6–9]. The prevalence of VWS is estimated between 1:40,000 and 1:100,000, which probably results from the registration of children treated in dif-ferent centers rather than epidemiological studies [10]. The syndrome occurs more often in girls in its prevalent forms of unilateral lip and palate cleft as well as an isolated palate cleft [11–13]. Similar to the cleft defect, van der Woude syndrome may be accompanied by other congenital orofacial and extraoral malformations [8, 10, 14]. Analyses of families with a positive history of VWS indicate an autosomal dominant inheritance pattern with balanced gene penetration. New studies suggest gene aberrations located on locus 1q32-41 or 1p34 of chromosome 1 [15–17]. Surgical repair includes
reconstruction of the cleft lip and/or palate, sinus excision, and plasty of the lower lip [9, 13, 18].
Material and Methods
A group of 3150 children with different forms of cleft lip and/or palate, including 23 (0.73%) with van der Woude syndrome (15 girls and 8 boys), were registered at the Department of Plastic, Reconstructive, and Aesthetic Surgery of the Medical University of Lodz. Among the cleft defects were 9 cases of isolated palate clefts, 7 cases of unilateral lip and palate clefts, 4 cases of bilat-eral lip and palate clefts, and 1 case of bilatbilat-eral lip and maxillary alveolar process. According to the guidelines accepted in the clinic, cleft lip was repaired in the children at the age of 6 months and cleft palate at the age of 18 months. All chil-dren had lower lip sinuses. Twenty-one patients had two symmetric sinuses (91.3%); in 1 child the defect was singular and 1 patient had three sinus-es. The lower lip was deformed, the inlet of the sinuses was 3 mm in diameter and surrounded by heaped pachycheilia and the sinuses themselves were 2 cm in depth. In several cases, saliva was secreted out of the inlets, especially during eat-ing. Five children presented slight lip deforma-tion which did not require treatment. Eighteen patients aged 2–3 years underwent spindle-shaped excision of the sinuses with simultaneous correc-tive cheiloplasty. Six of them required remodeling of the lower lip. Histopathological examination of the excised sinuses revealed a framework of fibrous tissue covered with stratified squamous epitheli-um. The presence of salivary glands explained the saliva discharge to the sinuses’ lumen.
Results
Six of the children with van der Woude syn-drome developed other congenital malformations, such as asymmetric macrostomy, convergent squint of one eye, protruding auricles, hemangio-ma of the dorsal foot, syndactylia, contracture in zatok i zniekształceń wargi dolnej u 18 operowanych był dobry, podobnie jak u 21 osób operowanych z powodu rozszczepu wargi i/lub podniebienia.
Wnioski. Zatoki wargi dolnej mogą towarzyszyć każdej z postaci rozszczepu wargi i/lub podniebienia. Zespół van der Woude częściej pojawia się u dziewczynek i jest przenoszony głównie przez matki. W kolejnych poko-leniach rodzin z zespołem van der Woude można się spodziewać eskalacji postaci współistniejących wad. Przedstawione w piśmiennictwie badania genotypowe sugerują występowanie zaburzeń genetycznych odpowie-dzialnych za dziedziczenie zespołu van der Woude, co potwierdzają obserwacje kliniczne (Adv Clin Exp Med 2010, 19, 1, 77–81).
the knee joint, phimosis, vulva hypoplasia, umbili-cal hernia, and brain hygroma. Coexisting defects were not absolute indications for surgical repair.
The children with occlusion defects (buccal occlu-sion, disocclusion) related to the lip and/or palate cleft were guided to orthodontic treatment.
In the majority of cases, the family history was negative; however, 10 patients belonged to five families with positive histories of lower lip sinuses or cleft lip and/or palate. In one family the mother developed the complete syndrome, in three families the mothers had only lower lip sinuses, and in one family the mother of a non-affected woman developed an isolated cleft palate. One of fathers had syndactylia (IV/V) of both feet, which was also inherited by one of his daughters (with a complete syndrome) (Figs. 2, 3). Results of karyotyping performed in the patients were nor-mal. However, there was no possibility of doing genetic testing. Of the 23 patients with complete (a sinus and a cleft) or incomplete (sinus) van der Woude syndrome, 10 (43.4%) had genetically transmitted defects.
In the present material the defects were trans-mitted by the mothers, but also inherited by three
Fig. 1. Complete Van der Woude syndrome: bilateral cleft lip and palate and lower lip sinuses
Ryc. 1. Pełny zespół van der Woude: obustronny rozsz-czep wargi i podniebienia oraz zatoki wargi dolnej
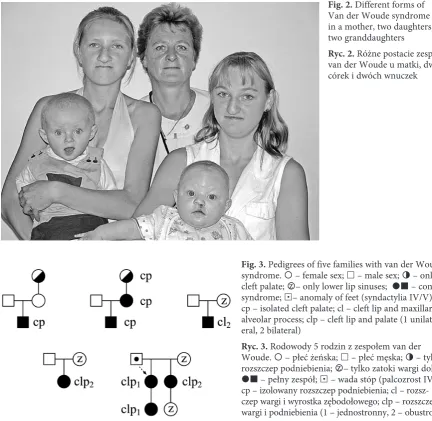
Fig. 2. Different forms of Van der Woude syndrome in a mother, two daughters, and two granddaughters
Ryc. 2. Różne postacie zespołu van der Woude u matki, dwóch córek i dwóch wnuczek
Fig. 3. Pedigrees of five families with van der Woude syndrome. – female sex; £ – male sex; » – only cleft palate; z – only lower lip sinuses; ¢ – complete syndrome; £ – anomaly of feet (syndactylia IV/V); cp – isolated cleft palate; cl – cleft lip and maxillary alveolar process; clp – cleft lip and palate (1 unilat-eral, 2 bilateral)
sons. Mothers with isolated cleft palate or only lower lip sinuses gave birth to children with com-plete van der Woude syndrome, which suggests symptom escalation.
In one case, a child of a mother with the com-plete syndrome, including the most severe form of the cleft defect (a complete bilateral lip and pal-ate cleft), whose grandmother had only lower lip sinuses, was born with an isolated lower lip defect (with no cleft). A sister (of the aforementioned mother ), also with the complete syndrome, gave birth to a daughter with identical malformations but without foot defects, which her mother had inherited from her father.
In families with isolated palate cleft, chil-dren with the same developmental malformations (+sinuses) were born. Lip and palate cleft (uni- or bilateral) appeared in the families with complete van der Woude syndrome or only lower lip sinuses.
Discussion and Conclusions
The polymorphism of clefts, i.e. the elements of the syndrome, observed in the study was also confirmed by other authors [12, 19, 20]. Lower lip sinuses, most frequently two symmetrically distributed deformities, can also occur as a sin-gular or multiple malformation with asymmet-ric localization on the vermillion [10, 21, 22]. Similarly to the present observations, there are cases of orofacial and extraoral defects coexist-ing with the syndrome described in the literature [23, 24]. According to the results of this study and other authors’ reports, the syndrome is predomi-nant in females [10]. Genetic determination of the syndrome is slightly higher than in the present observations (43.4%). Other authors also suggest symptom escalation in successive generations [4, 10, 13].
References
Antoszewski B, Kruk-Jeromin J:
[1] Epidemiology of cleft lip and palate in Lodz, Poland, in the years 1981–1995. Acta Chir Plast 1997, 39, 109–112.
Kruk-Jeromin J:
[2] The plan multidisciplinary treatment of cleft lip and palate. Ann Acad Med Lodz 1995, 36, 9–14.
Kot M, Kruk-Jeromin J:
[3] Analysis of family incidence of cleft lip and/or palate. Med Sci Monit 2007, 13, 231–234.
Kruk J:
[4] Zespół van der Woude’a. Czas Stomat 1985, 38, 105–110.
van der Woude A:
[5] Fistula labii inferioris congenita and its association with cleft lip and palate. Am J Hum Genet 1954, 6, 244–256.
Burdic AB, Bixler D, Puckett CL:
[6] Genetic analysis in families with van der Woude syndrome. J Craniofac Genet Dev Biol 1985, 5, 181–208.
Onofre MA, Brosco HB, Taga R:
[7] Relationship between lower-lip fistulae and cleft lip and/or palate in van der Woude syndrome. Cleft Palate Craniofac J 1997, 34, 261–265.
Wong F, Karsten A, Larson O, Huggare J, Hagberg C, Larsson C, Teh BT, Linder-Aronson S:
[8] Clinical and
genetic studies of van der Woude syndrome in Sweden. Acta Odontol Scand 1999, 57, 72–76.
Gawrych E, Jamroszczyk K:
[9] Familial occurrence of Van der Woude syndrome – a case report. Pediatr Pol 2004, 79, 327–329.
Rizos M, Spyropoulos MN:
[10] Van der Woude syndrome: a review. Cardinal signs, epidemiology, associated fea-tures, differential diagnosis, expressivity, genetic counseling and treatment. Eur J Orthod 2004, 26, 17–24.
Rintala A, Lahti A, Gylling US:
[11] Congenital sinuses of the lower lip in connection with cleft lip and palate. Cleft Palate J 1970, 7, 336–346.
Wójcicki P, Kobus K, Wójcicka K:
[12] Van der Woude Syndrome. Dent Med Probl 2007, 44, 18–21.
Kruk-Jeromin J, Żurawska-Klepacz M:
[13] Lower lip sinus with cleft lip and/or palate. Van der Woude syndrome. Czas Stomatol 2000, 53, 289–294.
Onofre M, Brosco H, Brosco J, Taga R:
[14] Congenital fistulae of the lower lip in van der Woude syndrome: a histo-morphological study. Cleft Palate Craniofac J 2002, 39, 219–225.
Kondo S, Schutte BC, Richardson RI, Bjork BC, Knight AS, Watanabe Y, Howard
[15] E, Ferreira de LimaRLL,
Daack-HirschS, Sander A, McDonald-McGinn DM, Zackai EH, LammerEJ, Aylsworth AS, Ardinger HH,
Lidral AC, Pober BR, Moreno L, Arcos-Burgos M, Valencia C, Houdayer C, Bahuau M, Moretti-Ferreira D, Richieri-Costa A, Dixon MJ, Murray JC: Mutations in IRF6 cause Van der Woude and popliteal pterygium syn-dromes. Nat Genet 2002, 2, 285–289.
Ghassibe M, Revencu N, Bayet BM, Gillerot Y, Vanwijck R, Verellen-Dumoulin C, Vikkula
[16] M: Six families with
van der Woude and/or popliteal pterygium syndrome: all with a mutation in the IRF6 gene. J Med Genet 2004, 41, e15.
Koillinen H
[17] , WongFK,Rautio J, Ollikainen V, Karsten A, Larson O, Teh BT, Huggare J, Lahermo P, Larsson C, Kere J: Mapping of the second locus for the van der Woude syndrome to chromosome 1p34. Eur J Hum Genet 2001, 9, 747–752.
Capon-Degardin N, Martinot-Duquennoy V, Auvray G, Pellerin P:
[18] Lower lip repair in van der Woude
syn-drome. Eur J Ped Surg 2003, 13, 92–96.
Gao N:
Ranta R, Rintala AE:
[20] Correlations between microforms of the van der Woude syndrome and cleft palate. Cleft Palate J 1983, 20, 158–162.
Plata-Nazar K, Kozielska E, Bogotko-Szarszewska M, Korzon M:
[21] Van der Woude syndrome: Case report. J Ped Neonatal 2005, 2, CR56–59.
Onofre M, Brosco H, Taga R:
[22] Relationship Between Lower-Lip Fistulae and Cleft Lip and/or Palate in Van der Woude Syndrome. Cleft Palate-Craniofac J 1997, 34, 261–265.
Nagore E, Sánchez-Motilla JM, Febrer MI, Serrano G, Bonillo J, Aliaga A:
[23] Congenital Lower Lip Pits (van der
Woude Syndrome): Presentation of 10 cases. Pediatr Dermatol 1998, 15, 443–445.
Guner U, Celik N, Ozek C, Cagdas A:
[24] Van der Woude syndrome. Scand J Plast Reconstr Surg Hand Surg 2002, 36, 103–105.
Address for correspondence:
Aleksandra Iljin
Department of Plastic, Reconstructive and Aesthetic Surgery Medical University of Lodz
Lutomierska 129 m. 70 91-037 Łódź
Poland
Tel.: +48 42 651 70 62 E-mail: [email protected]
Conflict of interest: None declared