Posttraumatic Migraine Characteristics Predict Extended Recovery Following Sport-Related Concussion in High School Athletes
by
Avanish Madhavaram
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for graduation with Honors in the Department of Exercise and
Sport Science 2020
Approved by:
________________________ Advisor: Jason P. Mihalik
________________________ Reader: Kevin A. Carneiro
ii ©2020
Avanish Madhavaram
iii ABSTRACT
AVANISH MADHAVARAM: Posttraumatic Migraine Characteristics Predict Extended Recovery Following Sport-Related Concussion in High School Athletes
(Under the direction of Jason P. Mihalik)
In previous studies, posttraumatic migraine (PTM) characteristics have been associated with neurocognitive deficits and higher overall symptom severity scores at a single timepoint post injury. In this study, we sought to further confirm the effect of PTM characteristics on symptom duration time and total time loss from sport in youth athletes. 324 athletes (266 males, 58 females) were grouped into posttraumatic migraine (PTM), posttraumatic headache (PTH), and no headache cohorts. We observed a significant relationship between headache group and prolonged symptom duration (F2,304 = 34.96, P< 0.0001) and total time loss from sport (F2,319 =
iv
Thank you to the entire team at the Matthew Gfeller Sport-Related Traumatic Brain Injury Research Center for their guidance and steadfast support. Thank you to Drs. Lisa Carey and Matt
v
TABLE OF CONTENTS
CHAPTER I: INTRODUCTION ...1
Aims ...3
Clinical Significance ...3
CHAPTER II: LITERATURE REVIEW ...4
Introduction ...4
Natural Recovery Trajectory of Concussion ...5
Definition of Posttraumatic Migraine ...6
Inflammation and Pain Modulation Associated with Migraine ...7
Further Pathophysiology of Posttraumatic Migraine ...8
Posttraumatic Migraine and TBI Recovery ...9
Posttraumatic Migraine as an Indicator of Cognitive Impairments ...9
Purpose and Relevance ...10
CHAPTER III: METHODOLOGY ...12
Data Analysis ...13
CHAPTER IV: RESULTS ...14
CHAPTER V: DISCUSSION ...16
Summary of Results ...16
Limitations and Further Study ...16
vi
Conclusions ...19
vii
LIST OF TABLES
viii
LIST OF FIGURES
1
CHAPTER I
INTRODUCTION
According to the Centers for Disease Control and Prevention, traumatic brain injury (TBI) is a public health problem in the United States that contributes to a number of deaths and disability.1 Concussions are the most common form of TBI experienced. Specifically in sport, an
estimated 1.6 to 3.8 million concussions occur each year, including cases where athletes sought no medical care.2 The National Collegiate Athletic Association reports 10,500 documented cases
of concussion in college athletes between the years of 2009-2014.3 TBI is among the most
expensive conditions to treat in adolescents.4 Despite the prevalence of TBI in the athlete
population, symptom treatment is still inconsistent between clinicians.5 Current return to
participation (RTP) guidelines following concussion are not considered true evidence-based standards for clinical care.6 However, encouragingly, providers are beginning to pay closer
attention to standard parameters that require athletes to be asymptomatic prior to sport participation.
There is a risk that any severity of TBI can cause long-term neurological deficits in patients.7 Therefore, it is important to consider certain features of concussion that may signal for
heightened and extended symptoms during recovery. Headache is the most commonly reported symptom following concussion.8 Headache after TBI is often grouped into either cluster-like
headaches, tension-type headaches, or posttraumatic migraine (PTM).9 PTM is of particular
2
Migraine is a condition diagnosed by acute attacks of pain alongside nausea, photophobia, or phonophobia.13 The International Headache Society labels migraine as an
episodic condition that result in impairment and disability.13 There is little known of a metabolic
mechanism that may link TBI to migraine symptoms. However, the literature does note that a depression of activity that follows concussion may reduce the activity of serotinergic (5-HT) neurons, which are responsible for weakening pain transmission.14 5-HT dysregulation has been
commonly noted in migraine patients to induce migraine-typical symptoms.15 This preliminary
mechanism may provide further efficacy to the use of PTM as a prognostic indicator. In previous studies, PTM characteristics were consistent with athletes experiencing greater deficits in neurocognitive testing when compared to controls at a single timepoint post-injury.10 Athletes experiencing PTM are also noted to report higher overall symptom severity
scores compared to controls at 7 days post injury.11 Posttraumatic migraine subjects have been
found to experience extended cognitive deficits during recovery, as well. At 14 days, PTM characteristics have been linked to visual memory and reaction time deficits.12 At 4 weeks post
injury, reaction time deficits persisted for athletes with PTM compared to controls.16 Most
interestingly, one study measuring cognitive deficits noted that athletes with PTM have a 7 times greater likelihood of requiring 21 days or longer for complete symptom recovery compared to no headache controls.12 Athletes with PTM were also twice as likely to continue having symptoms
at 3 weeks when compared to athletes with posttraumatic headache (PTH).12
3
Aims
We evaluated symptom duration time and time until fully cleared for participation (defined as total time lost post-injury). We assessed the effects of headache status (PTM, PTH, and none) on both variables.
We characterized prolonged symptom and RTP duration as ≥ 2 weeks. We determined whether there was an association between headache group and 1) prolonged symptom duration and 2) RTP duration.
We determined if headache group is a predictor for experiencing ≥ 2 weeks of prolonged total time loss from sport
Clinical Significance
4
CHAPTER II
LITERATURE REVIEW
Introduction
An estimated 1.6 to 3.8 million sports related concussions occur each year, including cases where athletes sought no medical care.2 The National Collegiate Athletic Association
(NCAA) reports that 10,500 documented concussions occurred in college athletics from 2009-2014.3 Health care providers must be trained in not only recognizing and providing prompt, acute
care to athletes following injury, but also play an active role in managing symptoms until
complete recovery. There is no universal consensus regarding the definition and classification of concussion.7 There are also some issues with the use of concussion as a diagnostic label for the
variety of symptoms experienced after a traumatic brain injury (TBI), especially as all
concussive symptoms are expected to resolve completely.7 It is clear that any severity of TBI can
have long-term neurological effects in patients.7 These long-term effects are often characterized
as post-concussion syndrome (PCS) if they persist longer than six weeks.17 PCS can include
symptoms ranging from fatigue and irritability to headache and nausea.17
In order to best inform clinical practices, researchers should explore prognostic indicators that may require adjusted or novel treatment pathways. Headache and dizziness are the two most common post-concussion symptoms reported.8 Prior findings have suggested posttraumatic
5
However, not all PTHs that follow concussion temporally are alike. Cluster-like headaches, tension type headaches, and migraine are all common variants of PTH.9
Posttraumatic migraine (PTM) is of particular importance to clinical study because it is often inadequately diagnosed in clinical settings and has been linked to specific recovery changes in some populations.10–12 Also, the metabolic mechanisms linking brain injury to a pattern of
symptom presentation seen in PTM patients are poorly understood.12
By establishing the risk of protracted recovery associated with PTM, clinicians can make guarded return to play decisions when athletes present with the symptoms and advise for more comprehensive migraine evaluations following traumatic injury.
Natural Recovery Trajectory of Concussion
There appears to be a natural recovery course that proceeds over the first few days in most athletes following injury.20 Athletes often display a range of task impairments including
cognitive deficits and balance problems following concussion.21 The typical recovery of such
symptoms occurs over the course of 5-7 and 3-5 days, respectively.21 Neuropsychological and
postural stability testing performed over multiple timepoints decreases reinjury risk in athletes by catching lingering symptoms prior to return to play.21 However, patients experiencing an
unexpected recovery trajectory often present unique clinical challenges.
Often, these challenges stem from clinicians using improper clinical indicators to measure concussion severity.22 Research has increasingly shown that the presence of many
indicators such as loss of consciousness, posttraumatic amnesia, confusion, or visual problems at the time of injury were poor predictors of protracted recovery.22 Often, the most consistent
indicators of protracted recovery are athlete pre-injury ratings of common concussion
6
the athlete prior to injury.25 PTM has the potential to become another tool clinicians can use to
better predict TBI recovery patterns for their patients.
Definition of Posttraumatic Migraine
Migraine is a condition diagnosed by acute attacks of pain alongside nausea, photophobia, or phonophobia.13 The International Headache Society labels migraine as an
episodic condition that result in impairment and disability.13 Interestingly, the lack of a simple
measurable tool for migraine results in its diagnosis only by exclusion. Clinicians often report a condition as migraine only when other, more recognizable, pathologies of headache are ruled out.26
PTM presents an additional diagnostic challenge for clinicians. Migraine and concussion are closely related, and similarities in evaluation of both are common. There is considerable overlap in post-concussive symptoms typical of TBI and the symptoms commonly noted in traditional migraine. It is proposed that concussion may trigger migraine; however, migraine may be misdiagnosed as concussion, or both may co-occur through a similar biological mechanism or by chance.27 Future research utilizing PTM would benefit from a health professional diagnosis of
the condition.
Additionally, certain individuals may be more susceptible to chronic headache, and the first occurrence of TBI may act as a trigger for a migraine attack. PTM may be more likely to appear in people with previous chronic headache experiences, where TBI exacerbates historical conditions.28 Therefore, headache history may be a risk factor for increased symptom severity
7
Psychosocial factors may also affect PTM and PTH symptom severity. Depression and post-traumatic stress disorder may increase the perceived intensity of PTH, especially in patients that present with prolonged mTBI symptoms. 14 In contrast, improved psychological resistance
has been measured to reduce the likelihood of extended symptoms following TBI, including PTH and PTM.14
Inflammation and Pain Modulation Associated with Migraine
Pain during migraine may be related to changes in cerebrovascular blood flow. Stimulation of the cranial vessels develops a strong pain response.29 One animal model study
showed a 25% reduction in cerebrovascular blood flow during migraine that occurs in parallel to extracerebral vasodilation.29 Globally altered cerebral blood flow is a prominent feature of pain
processing seen in migraine patients.30
Migraine links neuroinflammation with the sensitivity of neurovascular structures. While neuroinflammation may play a role in TBI recovery, prolonged neuroinflammation may lead to neuronal hyperexcitability and migraine development.14 Neuroinflammation commonly presents
as tension-like headache at first, which transforms to migraine as hyperexcitability advances.14
TBI-induced neuroinflammation also dysregulates pain modulation and enhances neuronal death.14
Migraine causes widespread activity changes in pain modulatory centers of the brain. These areas are commonly located in the periphery of the cortex, including the dorsal midbrain and the posterior hypothalamic grey.29 Attention to pain during headache is based on trigeminal
innervation of several target nuclei in these centers.30 Additionally, trigeminal nociceptive
8
back of the head in migraine patients.29 These neural pathways are most important for top-down
or subject-driven pain modulation.31
Pathophysiology of Posttraumatic Migraine
Widespread potassium, sodium, and calcium flux characteristic of the neurometabolic cascade of mTBI has been described to create a depression of activity in the cerebral cortex.32
That phenomenon, called cortical spreading depression, is a transient state of neuronal and glial cell depolarization and is a widely recognized trigger of migraine aura and headache pain.33
Following spreading depression, a migrainous brain does not habituate to signals in a normal manner.34
Following TBI, cortical spreading depression also reduces the activity of serotinergic (5-HT) neurons, which play a prominent role in diminishing pain transmission.14 A low 5-HT state
also triggers the trigeminovascular nociceptive pathway. Importantly, in controls that did not have prior history of migraine, short-term reduction of brain 5- HT levels induced nausea, dizziness and motion sickness.15 5- HT dysregulation may provide the most encouraging
evidence for a common mechanism between TBI and PTM symptoms, and demonstrate how PTM could exacerbate a post-injury symptom profile.
Under MRI study, PTH without migraine and PTM each have distinct underlying structural differences. When observing regional volumes, cortical thickness, surface area and brain curvature, individuals experiencing PTH and PTM differed in three areas: lateral
orbitofrontal lobe, superior and middle frontal lobe, and precuneus and supramarginal gyrus.35
These regions are associated with a wide area of functions, including sensory association, vision, higher order cognitive processing, and emotion.36,37 There were also differences in cortical
9
convincing evidence for a varied underlying pathophysiology specific to different types of headache. Yet still, more research is required to better delineate those particular functional changes.35
Posttraumatic Migraine and TBI Recovery
PTM has been documented as a potential prospective indicator of recovery. A
preliminary study tested athletes with and without PTM for 7 days and then at follow up on day 90.11 Patients with PTM had higher symptom severity scores in comparison to baseline at 7 days
post-injury. However, when considering recovery through the Balance Error Scoring System (BESS) and Standard Assessment of Concussion (SAC) scores, no group differences were noted.11 However, without studying recovery on timepoints past one week, a proper prognosis
may have been misidentified.
In this study, athletes with PTM report higher symptom burden on days 1, 3, 5, and 7.11
Athletes were not given a definitive asymptomatic assessment, and full recovery time is not noted for the cohorts. However, the presence of significant symptom severity differences in the PTM group compared to controls at 7 days demonstrate that protracted recovery is likely. A larger overall symptom burden for individuals reporting PTH without migraine quickly resolved to baseline within 5 days of injury—indicating that PTH alone likely did not demonstrate
protracted recovery over time.
Posttraumatic Migraine as an Indicator of Cognitive Impairments
10
Initially, such differences were only measured at one timepoint directly following the injury event.
Follow-up studies shows that PTM cognitive impairments model a 7 times higher likelihood of requiring 21 days or longer for complete symptom recovery compared to no headache controls12. Athletes with PTM were also twice as likely to continue having symptoms
at 3 weeks when compared to PTH cohorts.12
In PTM subjects, visual memory and reaction time showed consistent deficits across the first two weeks of recovery.12 At 14 days, the PTM cohort still showed significant deviance from
PTH and no headache controls for these two measures.12 At 4 weeks post-injury, in the PTM
cohort, reaction time deficits persisted.16 These results provide further evidence of sustained
cognitive impairments that may last several weeks in athletes presenting with PTM.
Posttraumatic migraine is likely linked to protracted recovery as sustained neurocognitive deficits have been consistently associated with the condition. However, in order to confirm recovery deficits, researchers must observe athlete cohorts over a wide spectrum of behavioral, balance and cognitive tasks. Therefore, further research related to psychosocial and vestibular changes following injury are necessary.
Purpose and Relevance
11
evidence for or against PTM’s prognostic capacity, as using many indicators in the same athletes will tend to better supplement conclusions.
12
CHAPTER III
METHODOLOGY
In this investigation, we collected data from a study completed between the years 1998-2001 on concussion recovery in 375 high school aged athletes. We did not discriminate by sex when selecting subjects. All athletes in the study were high school sport participants.
Consistent with prior study in the area,11 athletes were grouped into posttraumatic
migraine (PTM), posttraumatic headache (PTH), and no headache cohorts. A post-concussive symptom survey was conducted at several clinical timepoints following initial injury until an athlete was asymptomatic and again fully participating in sport. Posttraumatic migraine athletes were defined as reporting headache along with either 1) nausea or vomiting, or 2) photophobia and phonophobia. PTH athletes reported any degree of headache but without the other migraine-like symptoms (nausea or vomiting, or sensitivity to light and noise). The no headache cohort did not report any degree of headache. Group determinations were made based on the participant’s symptom presentation on Day 1. Valid symptom data on Day 1 were available for only 324 athletes (266 males, 58 females). Therefore, these 324 participants were retained for our analyses. Our patients were injured while participating in the following sports: football
(63.73%), hockey (1.33%), lacrosse (11.20%), and soccer (23.73%). Demographic information for our patients including age, height, weight, sex and sport participation are provided in Table 1.
We operationalized prolonged symptom duration and prolonged total time loss using a 2-week timepoint (≥14 days), consistent with prior PTM studies.38 Athlete recovery that is shorter
13
We determined if any cohort is more likely to remain away from sport participation at 2 weeks post injury.
Data Analysis
We completed the following statistical analyses in accordance with this study’s aims. We completed chi-square analyses on both prolonged symptom duration and prolonged total time loss in order to determine if headache group was associated with either variable. We then
14
CHAPTER IV
RESULTS
A total of 375 athletes were tracked for recovery following concussion in this study. Of these participants, only 324 had sufficient symptom reporting data to categorize them into the appropriate post-injury group. We classified injured athletes into PTM (n=107, 33%), PTH (n=143, 44%), or no headache (n=74, 22.8%) groups.
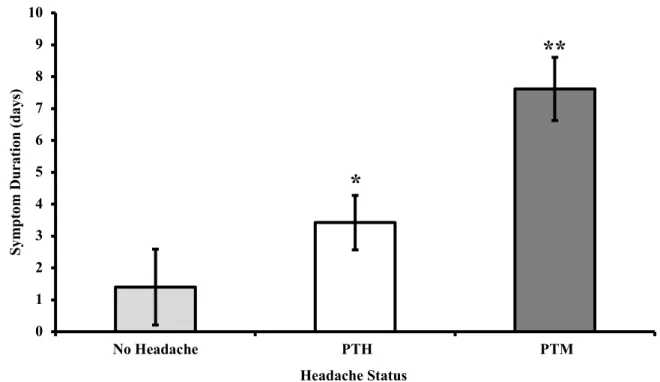
A one-way between-subjects ANOVA was conducted to compare the effect of headache group on symptom duration and total time loss for no headache, PTH, and PTM conditions. We observed a significant effect of headache group on symptom duration (F2,304 = 34.96, P< 0.0001).
Post hoc analyses demonstrate that symptom duration time for the PTM group was significantly greater than the PTH cohort by 4.19 days (95% CI: 2.62, 5.77) and no headache group by 6.22 days (95% CI: 4.36, 8.08). The PTH group also had a mean symptom duration time significantly exceeding the no headache cohort by 2.02 days (95% CI: 0.26, 3.78). A graph of mean symptom duration as a function of headache status is shown in Figure 1, and all data related to this analysis are provided in Table 2.
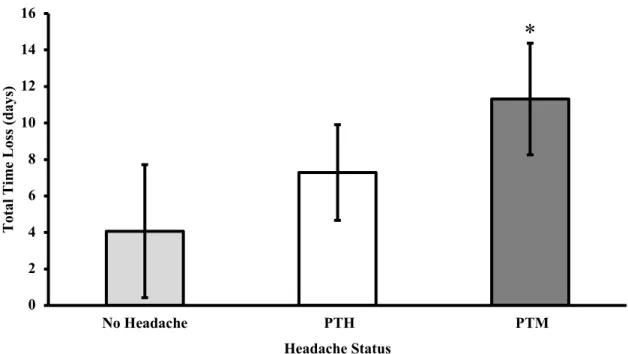
There was also a significant effect of headache group on total time loss from sport (F2,319 = 4.62, p = 0.011). Post hoc analyses demonstrate that total time loss for the PTM group
15
We observed a significant association between headache group and prolonged symptom duration (χ2(2) = 32.55, P < 0.0001). There was also an association between headache group and
total time loss (χ2(2) = 7.73, P = 0.021). In both instances, athletes with PTM characteristics
demonstrated a relative frequency increase for experiencing symptoms or total time loss exceeding 2 weeks than athletes with PTH or no headache.
Lastly, we also observed that headache group was a significant predictor of experiencing ≥2 weeks of prolonged total time loss from sport (χ2(2) = 7.28, P = 0.026). The PTM group had
3.57 times (95% CI: 1.29, 9.92) greater odds of experiencing prolonged total time loss from sport compared to the no headache group. This observation was not observed in our comparison
16
CHAPTER V
DISCUSSION
Summary of Results
The purpose of this study was to determine if characteristics of PTM immediately following injury predicted sustained symptoms and an extended recovery timeline. Overall, the results indicate that the presence of PTM characteristics following injury significantly
lengthened symptom resolution times compared to PTH and no headache controls. Posttraumatic migraine characteristics also extended RTP times compared to no headache controls.
The study found a significant relationship between headache status and prolonged symptom and RTP duration. The PTM group had 3.57 times greater odds of athletes of
experiencing >2 weeks of total time loss from sport. The PTM group had an average symptom duration longer than both PTH and no headache controls by 4.19 and 6.22 days, respectively. Athletes with characteristics of PTM also took an average of 7.245 days longer to RTP compared to no headache controls.
The PTH cohort did experience a longer average symptom duration of 2.02 days
compared to no headache controls. However, the PTH group did not show significant differences in RTP duration compared to no headache controls. The PTH group also did not display evidence for being more likely to require 2 weeks prior to RTP compared to no headache controls.
Limitations and Future Study
17
may have had an overall larger symptom burden than a no headache participant, which could have played a contributing role in prolonging RTP duration and symptom recovery trajectory. We also did not have available data among participants to report a prior history or family background of migraine. We were also unable to make any reliable predictions about the likelihood of continued symptom or RTP status beyond 2 weeks post injury due to the nature of the data.
Perhaps the biggest weakness in this study is the date of data collection. Epidemiologists have consistently reported that sport-related concussion was underreported in athletes for many years.39 In a high school concussion study, researchers found a 4-fold increase in concussions per
athlete exposure between the years 1997 and 2007.40 The data collected for this project was
originally obtained between the years 1998-2001. During this time, high school athletes may have been more likely to RTP quicker following injury regardless of symptom status and
commonly underreport symptom severity. Concussion evaluation and removal from participation has drastically advanced in the past 20 years. Therefore, it is difficult to claim that the trends we notice here apply to modern youth athletes and current standards of care.
Future research shows the opportunity to study symptom data from college-aged athletes, a population that has not been investigated for the effects of PTM characteristics on recovery. Additionally, it is more appropriate to use current athlete data obtained from updated concussion evaluation standards to best support any future clinical judgements. There is also a novel
18
Significance
The literature shows considerable evidence for the effect of PTM on recovery trajectory and symptom severity through a host of different measures. The results of this study show that symptom duration and return to play time are often increased in athletes with PTM
characteristics. That observation is correlated with studies that have used serial computerized neurocognitive testing to understand the effects of PTM. Studies have shown that significant neurocognitive deficits are correlated with PTM characteristics at a single timepoint post-injury.10 Reaction time deficits and visual memory deficits remain at 2 weeks post injury for
athletes with PTM characteristics.12 At 4 weeks post injury, reaction time deficits have been
demonstrated to persist in athletes with PTM characteristics compared to both PTH and no headache groups.12
Studies have also demonstrated that symptom severity has been more pronounced in athletes with PTM throughout the first 2 weeks of recovery. Posttraumatic migraine has correlated with a higher overall symptom severity score on days 1, 3, 5, and 7 of recovery.11
Cognitive, somatic, emotional, and sleep symptoms have all been reported as more severe in PTM groups at 2 weeks post injury.12 Therefore, the literature does indicate that posttraumatic
migraine is associated with heightened concussive effects. These studies again agree with results presented in this project as we found that PTM is correlated with a more severe and extended recovery timeline.
Finally, one study observed athletes’ medical records and predicted that PTM characteristics were associated with 7.3 times greater odds of requiring 21 days to recover
compared to no headache controls.12 The PTM group also had 2.6 times greater odds of requiring
19
While the literature shows more sizable differences between groups than what was found in this study, we still observed that PTM was associated with 3.57 times greater odds of experiencing over 2 weeks total time loss from sport compared to those athletes not endorsing post-injury headache. Our conclusions again match those predicted from prior study.
Further support is still necessary in additional populations and through matching experimental design prior to using PTM to make any clinical judgements. However, current evidence indicates that PTM is a promising indicator of predicting more severe and extended concussive symptoms. There are also studies that begun to investigate a metabolic mechanism between TBI and PTM characteristics. These include observing 5-HT serotonergic neuron dysfunction triggering a nociceptive pathway as a result of cortical spreading depression
following concussion.15 There has also been MRI testing that has revealed differences in regional
volumes, cortical thickness, surface area and brain curvature in 3 brain areas, the lateral orbitofrontal lobe, superior and middle frontal lobe, and precuneus and supramarginal gyrus, when comparing patients with a diagnosed PTH and PTM.35 Results from this analysis reveal the
necessity for a more definitive understanding of how migraine symptoms present following concussion physiologically. This requires additional investigation into a conclusive
neurometabolic pathway that assesses how the effects of TBI cause migraine-like symptoms to present and persist.
Conclusions
This study presents significant results that demonstrate that athletes with characteristics of PTM following concussion are likely to experience a longer symptom duration and a
20
21
TABLES AND FIGURES
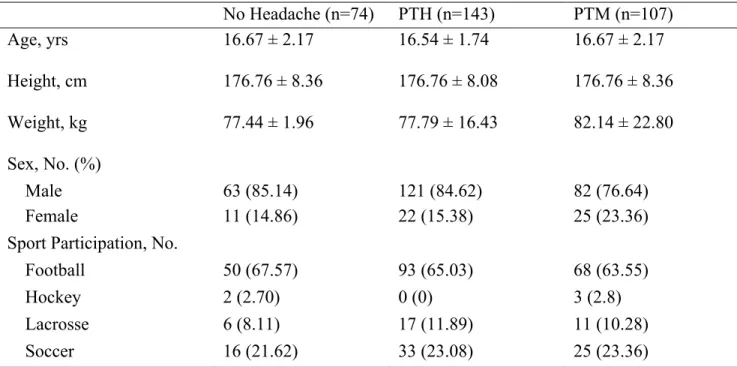
Table 1. Demographic information (mean ± SD unless otherwise noted) for our study sample by group
No Headache (n=74) PTH (n=143) PTM (n=107) Age, yrs 16.67 ± 2.17 16.54 ± 1.74 16.67 ± 2.17 Height, cm 176.76 ± 8.36 176.76 ± 8.08 176.76 ± 8.36 Weight, kg 77.44 ± 1.96 77.79 ± 16.43 82.14 ± 22.80 Sex, No. (%)
Male 63 (85.14) 121 (84.62) 82 (76.64)
Female 11 (14.86) 22 (15.38) 25 (23.36)
Sport Participation, No. (%)
Football 50 (67.57) 93 (65.03) 68 (63.55)
Hockey 2 (2.70) 0 (0) 3 (2.8)
Lacrosse 6 (8.11) 17 (11.89) 11 (10.28)
22
Table 2. Average symptom duration in days for each headache group
Headache Group N* Mean Std Dev
No headache 70 1.40 1.80
PTH 136 3.42 2.73
PTM 101 7.61 8.13
23
Table 3. Total time loss from sport in days for each headache group.
Headache Group N* Mean Std Dev
No headache 74 4.07 9.13
PTH 143 7.29 15.77
PTM 105 11.32 19.67
* Group-level sample sizes for this analysis may be reduced due to availability of total time loss from sport data among study participants.
24 0 1 2 3 4 5 6 7 8 9 10
No Headache PTH PTM
Sym pt om D ur at ion (days ) Headache Status
Figure 1. Mean symptom duration with 95% confidence intervals distributed between headache groups. The vertical axis displays symptom duration in days, while the horizonal axis represents the three headache conditions. Error bars signify 95% confidence intervals. One asterisk (*) denotes a significant difference in symptom duration when compared to no headache controls. Two asterisks (**) denotes a significant difference in symptom duration compared to both no headache and PTH conditions.
*
25 0 2 4 6 8 10 12 14 16
No Headache PTH PTM
To ta l Ti m e Lo ss ( da ys ) Headache Status
Figure 2. Mean total time loss with 95% confidence intervals distributed between headache groups. The vertical axis displays total time loss in days, while the horizonal axis represents the three headache conditions. Error bars signify 95% confidence intervals. One asterisk (*) denotes a significant difference in symptom duration when compared to no headache controls.
26
REFERENCES
1. Basic Information about Traumatic Brain Injury | Concussion | Traumatic Brain Injury | CDC Injury Center. https://www.cdc.gov/traumaticbraininjury/basics.html. Published March 6, 2019. Accessed November 19, 2019.
2. Langlois JA, Rutland-Brown W, Wald MM. The Epidemiology and Impact of Traumatic Brain Injury: A Brief Overview. J Head Trauma Rehabil. 2006;21(5):375.
3. Martin TG, Wallace J, Suh YI, Harriell K, Tatman J. Sport-Related-Concussions Pilot Study: Athletic Training Students’ Media Use and Perceptions of Media Coverage. Int J Sport Commun. 2018;11(1):75-94. doi:10.1123/ijsc.2017-0086
4. Schneier AJ, Shields BJ, Hostetler SG, Xiang H, Smith GA. Incidence of pediatric traumatic brain injury and associated hospital resource utilization in the United States.
Pediatrics. 2006;118(2):483-492. doi:10.1542/peds.2005-2588
5. Polinder S, Cnossen MC, Real RGL, et al. A Multidimensional Approach to Post-concussion Symptoms in Mild Traumatic Brain Injury. Front Neurol. 2018;9. doi:10.3389/fneur.2018.01113
6. Echemendia RJ, Giza CC, Kutcher JS. Developing guidelines for return to play: consensus and evidence-based approaches. Brain Inj. 2015;29(2):185-194.
doi:10.3109/02699052.2014.965212
7. Sharp DJ, Jenkins PO. Concussion is confusing us all. Pract Neurol. 2015;15(3):172-186. doi:10.1136/practneurol-2015-001087
8. Mullally WJ. Concussion. Am J Med. 2017;130(8):885-892. doi:10.1016/j.amjmed.2017.04.016
9. Lucas S. Headache management in concussion and mild traumatic brain injury. PM R. 2011;3(10 Suppl 2):S406-412. doi:10.1016/j.pmrj.2011.07.016
10. Mihalik JP, Stump JE, Collins MW, Lovell MR, Field M, Maroon JC. Posttraumatic migraine characteristics in athletes following sports-related concussion. J Neurosurg. 2005;102(5):850-855. doi:10.3171/jns.2005.102.5.0850
11. Mihalik JP, Register-Mihalik J, Kerr ZY, Marshall SW, McCrea MC, Guskiewicz KM. Recovery of Posttraumatic Migraine Characteristics in Patients After Mild Traumatic Brain Injury. Am J Sports Med. 2013;41(7):1490-1496. doi:10.1177/0363546513487982
27
13. Consensus statement on improving migraine management. - PubMed - NCBI. https://www.ncbi.nlm.nih.gov/pubmed/11279900. Accessed October 2, 2019. 14. Ruff RL, Blake K. Pathophysiological links between traumatic brain injury and
post-traumatic headaches. F1000Research. 2016;5. doi:10.12688/f1000research.9017.1
15. Serotonin and Migraine: Biology and Clinical Implications - E Hamel, Headache Currents, 2007.
https://journals.sagepub.com/doi/full/10.1111/j.1468-2982.2007.01476.x?casa_token=GNNSsUPnGhQAAAAA%3ArjS5ZVvWiLnoiqLff7DwP _htk4BwaCFUXGgQf634U_NlA9F4jqNui-iyF4kJ0EsGQ_kYvN3PgC7j. Accessed November 7, 2019.
16. Kontos AP, Reches A, Elbin RJ, et al. Preliminary evidence of reduced brain network activation in patients with post-traumatic migraine following concussion. Brain Imaging Behav. 2016;10(2):594-603. doi:10.1007/s11682-015-9412-6
17. Leddy JJ, Sandhu H, Sodhi V, Baker JG, Willer B. Rehabilitation of Concussion and Post-concussion Syndrome. Sports Health. 2012;4(2):147-154. doi:10.1177/1941738111433673 18. Collins MW, Field M, Lovell MR, et al. Relationship between Postconcussion Headache
and Neuropsychological Test Performance in High School Athletes. Am J Sports Med. 2003;31(2):168-173. doi:10.1177/03635465030310020301
19. Evans RW. Persistent Post-Traumatic Headache, Postconcussion Syndrome, and Whiplash Injuries: The Evidence for a Non-Traumatic Basis With an Historical Review. Headache J Head Face Pain. 2010;50(4):716-724. doi:10.1111/j.1526-4610.2010.01645.x
20. Guskiewicz KM, Weaver NL, Padua DA, Garrett WE. Epidemiology of Concussion in Collegiate and High School Football Players. Am J Sports Med. 2000;28(5):643-650. doi:10.1177/03635465000280050401
21. McCrea M, Guskiewicz KM, Marshall SW, et al. Acute Effects and Recovery Time Following Concussion in Collegiate Football Players: The NCAA Concussion Study.
JAMA. 2003;290(19):2556-2563. doi:10.1001/jama.290.19.2556
22. Lau BC, Kontos AP, Collins MW, Mucha A, Lovell MR. Which On-field Signs/Symptoms Predict Protracted Recovery From Sport-Related Concussion Among High School Football Players? Am J Sports Med. 2011;39(11):2311-2318. doi:10.1177/0363546511410655 23. Injury versus noninjury factors as predictors of postconcussive symptoms following mild
traumatic brain injury in children. - PubMed - NCBI.
https://www.ncbi.nlm.nih.gov/pubmed/23356592. Accessed October 2, 2019. 24. Early symptom burden predicts recovery after sport-related concussion | Ovid.
28
25. Machulda MM, Bergquist TF, Ito V, Chew S. Relationship Between Stress, Coping, and Postconcussion Symptoms in a Healthy Adult Population. Arch Clin Neuropsychol. 1998;13(5):415-424. doi:10.1093/arclin/13.5.415
26. Margulies S. The postconcussion syndrome after mild head trauma part II: is migraine underdiagnosed? J Clin Neurosci Off J Neurosurg Soc Australas. 2000;7(6):495-499. doi:10.1054/jocn.1999.0773
27. Gordon KE, Dooley JM, Wood EP. Is migraine a risk factor for the development of concussion? Br J Sports Med. 2006;40(2):184-185. doi:10.1136/bjsm.2005.022251 28. Solomon S. Posttraumatic Migraine. Headache J Head Face Pain. 1998;38(10):772-778.
doi:10.1046/j.1526-4610.1998.3810772.x
29. Goadsby PJ. Pathophysiology of migraine. Ann Indian Acad Neurol. 2012;15(Suppl 1):S15-S22. doi:10.4103/0972-2327.99993
30. AHMAD AH, ABDUL AZIZ CB. The Brain in Pain. Malays J Med Sci MJMS. 2014;21(Spec Issue):46-54.
31. Donaldson LF, Lumb BM. Top‐down control of pain. J Physiol. 2017;595(13):4139-4140. doi:10.1113/JP273361
32. Giza CC, Hovda DA. The New Neurometabolic Cascade of Concussion. Neurosurgery. 2014;75(0 4):S24-S33. doi:10.1227/NEU.0000000000000505
33. Eikermann-Haerter K, Ayata C. Cortical Spreading Depression and Migraine. Curr Neurol Neurosci Rep. 2010;10(3):167-173. doi:10.1007/s11910-010-0099-1
34. Ambrosini A, Schoenen J. Electrophysiological response patterns of primary sensory
cortices in migraine. J Headache Pain. 2006;7(6):377-388. doi:10.1007/s10194-006-0343-x 35. Schwedt TJ, Chong CD, Peplinski J, Ross K, Berisha V. Persistent post-traumatic headache
vs. migraine: an MRI study demonstrating differences in brain structure. J Headache Pain. 2017;18(1):87. doi:10.1186/s10194-017-0796-0
36. Functions of the left superior frontal gyrus in humans: a lesion study | Brain | Oxford Academic. https://academic.oup.com/brain/article/129/12/3315/266905. Accessed November 18, 2019.
37. Penniello M-J, Lambert J, Eustache F, et al. A PET study of the functional neuroanatomy of writing impairment in Alzheimer’s disease The role of the left supramarginal and left angular gyri. Brain. 1995;118(3):697-706. doi:10.1093/brain/118.3.697
29
39. Tucker AM. Update on Sports Concussion. Curr Rev Musculoskelet Med. 2014;7(4):366-372. doi:10.1007/s12178-014-9243-x
40. Trends in Concussion Incidence in High School Sports: A Prospective 11-Year Study - Andrew E. Lincoln, Shane V. Caswell, Jon L. Almquist, Reginald E. Dunn, Joseph B. Norris, Richard Y. Hinton, 2011.