Available Online at www.ijpret.com 10
INTERNATIONAL JOURNAL OF PURE AND
APPLIED RESEARCH IN ENGINEERING AND
TECHNOLOGY
A PATH FOR HORIZING YOUR INNOVATIVE WORK
WEAR STUDY ON ARTIFICIAL JOINT REPLACEMENT, TOTAL DISC
REPLACEMENT- A STATE OF ART REVIEW
SUBHANKAR BISWAS1, ADITYA S. GORE1, VAIBHAV P. MEHTA2 1. M. Tech CAD/CAM VIT University Chennai Campus.
2. M. Tech, Structural Engineering Division, VIT University Chennai Campus.
Accepted Date: 27/01/2016; Published Date: 01/03/2016
\
Abstract: -This paper reviews the results of an investigation on artificial joint replacements specially total disc replacement under dry and wet sliding conditions for different conditions of loading, lubrication ,different composition of materials, various pH concentration and various others condition. In this paper various experiment done relevant to wear for titanium alloy (Ti—6Al—4V, Ti—6Al—7Nb and Ti—13Nb—13Zr) cobalt chromium alloy (Co– 29Cr–8Mo, Co–29Cr–6Mo, Co–Cr–Mo) and various Stainless Steel and are reviewed. It has been found that wear of implant depends not only a single parameter the environmental or working condition of the implant but also other factors like varying the material composition of the materials.
Keywords:Wear, Biomaterial, Implants, Artificial joint replacement, Failure of implants
Corresponding Author: MR. SUBHANKAR BISWAS
Access Online On:
www.ijpret.com
How to Cite This Article:
Available Online at www.ijpret.com 11
1. INTRODUCTION
Directly or indirectly in the case of knee and hip joint prosthesis Wear is the main cause of failure of implants. Minimization of wear is the most important aspect to be taken care for making the joint more efficient. A survey report of USA says that 90% of population over the age of 40 suffers from these kinds joint problem, the aged people population has increased tremendously in recent past and it is estimated there will be a seven times increase (from 4.9 million which was in 2002 to 39.7 million by 2010). [56] Noteworthy is the fact that knee replacement surgery (TKR)is performed on more than 2.5 million people in USA alone annually, followed by total hip joint replacement (TJR) of more than 3.5 million and around 7 million spinal fusions [83]There are two different aspect of Wear failure. Firstly, softer material part (most of the cases, Ultra High Molecular Weight Polyethylene) of the joint prosthesis will go totally worn off for reciprocating motion. Secondly, entrapped wear debris between implant and bone cement which is mainly responsible for prosthesis loosening. To avoid those types of failure, different scientist has been performed different type of wear tests, with different type of frequently used biocompatible materials. Most of the cases, two types of wear testing machine (pin & disk and reciprocating), are used for experiments. In this area, numerous experiments were performed. In the current context, we consider both the two type of machine for experiment. Before going to the main context let us discuss about some commonly referred type of wear to wear mechanisms (or processes):
They are Adhesive wear, Abrasive wear, Surface fatigue, Fretting wear, Erosive wear, Corrosion, and oxidation wear
A. Adhesive wear
Adhesive wear is generally found between surfaces during frictional contact . This type of wear refers to unwanted displacement and attachment of wear debris and material compounds from one surface to another.[57]
Two sliding bodies over each other or pressing into each other causes adhesive wear and it promote material transfer.[56] Adhesive wear is a common fault factor in industrial applications such as sheet metal forming [57]
B. Abrasive wear
Available Online at www.ijpret.com 12 are forced against and move along a solid surface. It is commonly classified according to the type of contact and the contact environment.
C. Surface fatigue
In surface fatigue process, the surface of a material is weakened by cyclic loading, and it is one type of general material fatigue.[58].Fatigue wear is produced when the wear particles are detached by cyclic crack growth of micro-cracks on the surface.[58]
D. Fretting wear
Repeated cyclical rubbing between two surfaces causes fretting wear over a period of time, which is known as fretting, will remove material from one or both surfaces in contact [59]. It occurs in bearings, although most bearings have their surfaces hardened to resist the problem [59].
E. Erosive wear
Extremely short sliding motion executed within a short time interval causes Erosive wear. [60] Erosive wear is caused by the impact of particles of solid or liquid against the surface of an object [61].
F. Corrosion and oxidation wear
Corrosion and oxidation wear occurs in a variety of situations both in lubricated and un-lubricated contacts. The main cause of these wear is chemical reaction between the worn material and the corroding medium.
WEAR AT DRY STATE CONDITION
Test may be conducted in dry state or in wet state or in lubricating case. there is very few information regarding dry wear test on pin on disk experiment. (wang a. et.al (2000)) showed that wear or loss of volume is measured in the function of loss mass of particle the formula for that is
Available Online at www.ijpret.com 13 or by specifying this we can say FOR PARTICULAR case and for disc volume loss may be calculated from the generalised formula as
or for specific case we can say for
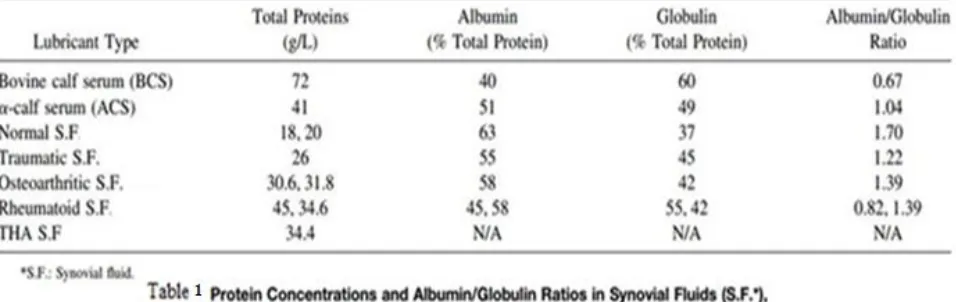
Wear at wet state condition in the presence of lubrication
Available Online at www.ijpret.com 14 Now let us look various Protein Concentrations and Albumin/Globulin Ratios in Synovial Fluids (S.F.*), Bovine Calf Serum (BCS) and -Calf Serum (ACS) in tabulated format which is shown in Table 3 .
Available Online at www.ijpret.com 15 represented both the passive and active regions of the materials and these curves were used to compare the resistance to pitting corrosion of each material. The sliding-wear of these materials was studied in both non-corrosive and corrosive environments. During wear calculation of implants we should also consider the direction of application of force along with other parametric conditions. Philip J. Hyde et.(2015) observed that Changing the phasing of the flexions to create a low (but finite) amount of crossing path motion at the bearing surfaces resulted in a significant fall in wear volume.
Results of different wear test on titanium material through pin on disc experiment
Available Online at www.ijpret.com 16 it was found that corrosion reduced the hardness of the surface oxides of all the alloys. In PBS the reduction was smallest for Ti—6Al—4V and largest for Ti—13Nb—13Zr and that corrosion in protein solutions further reduced the hardness of the surface oxides. This effect was greater for Ti—6Al—4V and Ti—6Al—7Nb than for Ti—13Nb—13Zr. In conclusion, proteins in the environment appear to interact with the repassivation process at the surface of these alloys and influence the resulting surface properties. A simple pin-on-disc type wear apparatus was designed and built to simulate the co-joint action of corrosion and sliding-wear. Using this apparatus, it was also possible to evaluate the effect of wear-accelerated corrosion, which was also evaluated by wearing the surface of the specimens prior to corrosion. It was evident that the mixed phase alphabeta alloys (Ti-6AI-4V and Ti-6AI-7Nb) possessed the best combination of both corrosion and wear resistance, although commercially pure titanium and the near-beta (Ti-13Nb-13Zr) and beta (Ti-15Mo) alloys displayed the best corrosion resistant properties. In the test of Philip J. Hyde et.al (2015) they have shown that the rate of wear was larger than under zero cross shear conditions. Reducing the load did not result in a significant change in wear rate. Moving the centre of rotation of the disc inferiorly did significantly increase wear rate. A phenomenon of debris re-attachment on the UHMWPE surface was observed and hypothesised to be due to a relatively harsh tribological operating regime in which lubricant replenishment and particle migration out of the bearing contact zone were limited.
Available Online at www.ijpret.com 17 parameter, with great influence during the initial rubbing, was the surface roughness of the polymer, which would be more rough in the initial stages and gradually polished during the later stages. This can be well observed as initials peak point in the individual and as well as comparative graphs. It is observed that after this peak point, wear was gradually decreased and attained a lowest point, which continued upto several number of cycles.
They have taken three material (as shown in figure 1 and 2) as sample and observed The slopes of three curves are different as shown in the figure 1 and figure 2.
In an another experiment they have shown that Initially, for Co-Cr-Mo alloy plate, Ra value was 1.8 micron. After 77,000 cycles Ra value became 98 micron. Then after 2,50,000 cycles, it was reduced to 78 micron. It was observed that rate of change of Ra value was initially high then it was low. In case of ceramics, we observed similar trend of change of Ra value. Initially the Ra value was 1.03 micron and after 77,000 cycles, we measured it as 88 micron. After 2,50,000 cycles, it was reduced to 84 micron. So it was concluded for the ceramics, the rate of change of Ra value was slower than Co-Cr-Mo alloy, but the trend of change of Ra value was quite same with Co-Cr-Mo plate, as well as titanium alloy plate. It is obvious that to minimize the wear, we require better surface finish. On the other hand, badly finished prosthesis may generate large size of wear debris in vivo.
Available Online at www.ijpret.com 18
Figure 4: Charite SEM images (left to right (clock wise): increase in magnification) of roughened area around the UHMWPE pole region showing appearance of built up surface
Available Online at www.ijpret.com 19
Biocompatibility of medical devices and the need for surface modification
Depending on the intended implant location, like desired application of the biomedical device, there are different factors to be considered. As an example, if the biomedical device is intended to be a blood-contacting device (catheter, graft and stent), blood compatibility (haemocompatibility) of the biomaterials is crucial, but for bone applications osseointegration is the key parameter. For both types of applications, the host response and its severity are strictly related to the surface properties of the biomaterial.[1]
Biomedical devices for use in contact with blood must not activate the intrinsic blood coagulation system, nor attract or alter platelets or leucocytes. From this point of view, biocompatibility is more difficult to achieve as it covers aspects such as thrombogenicity, complement activation, leukocyte activation and changes in plasma proteins [2].
Achieving osseointegration, particularly by establishing a strong and long-lasting connection between the implant surface and peri-implant bone, leading to a stable mechanical attachment of the implant at the site of the implantation is the clinical goal and most critical factor in the success of bone implants (orthopaedics and dentistry) [6]. In bone, titanium is integrated in close opposition to the mineralized tissues under the proper conditions. However, titanium and bone are generally separated by a thin soft-tissue layer as a result of a weak foreign body reaction that prevents titanium from being in direct contact with the bone [7]. When the implantation procedure occurs, several biological reactions take place in a specific order. Firstly, there will be wetting of the implant surface and rapid adsorption of biologically active molecules (such as proteins), followed by enlisting of the osteoprogenitor cells that would regenerate the tissue [8]. From the observation, it is shown that the two factors affecting osseointegration are the mechanical properties of the implant and the biological interactions with the metal surface, of which the latter is more relevant.
Available Online at www.ijpret.com 20 improvement is by modification of the implant’s surface properties, either morphologically and/or by biochemical coatings.
It is evident that the response of a biomaterial depends entirely on its biocompatibility and surface properties. Therefore, in order to improve the performance of biomaterials in biological systems, there is an urgent need for their surface modification [10]
CONCLUSION:
Knee joints that operate as dynamically loaded bearing are subjected to 108 cycles of loading in 70-year lifetime. The average coefficient of friction of the load bearing synovial joints such as hip and knee is about 0.02 and the wear factor is about 106 mm3/N. On the other hand, the
Available Online at www.ijpret.com 21 high metal concentrations were found in tissue taken from the region around Ti alloy prostheses, while, the metals debris level were low in the tissues surrounding the CoCr and SS that were articulating against polyethylene [84]. Metal on metal prostheses is found to produce 20–100 times lower wear volumes compared to metal on polyethylene bearing [85]. The biological reaction to metal particles in vivo has been shown to be markedly different to that produced by UHMWPE wear debris and lower inflammatory reactions are found to be caused by metal [86] However, it has also been observed that metal on metal prosthesis exhibits high frictional torques than the metal on polymer [88]. Though
Available Online at www.ijpret.com 22 properties and have high resistance to crack propagation. Today more than 6, 00, 000 zirconia head implants have been fixed and it is more frequently used in USA and Europe than any other countries. Metal on metal pair exhibited high friction coefficient when tested with CMC and lowest wear rate when tested in bovine serum [86]. Wapner reviewed the toxic effects of metals viz., Ni, Co and Cr released from prosthetic implants [95]. Skin related diseases such as dermatitis due to Ni toxicity have been reported and numerous animal studies have shown arcinogenicity due to the presence of Co [96]. In addition, both 316L SS and Cr–Co alloys possess much higher modulus than bone, leading to insufficient stress transfer to bone leading to bone resorption and loosening of implant after some years of implantation. The high cycle fatigue failure of hip implants is also reported as the implants are subjected to cycles of loading and unloading over many years [97]. Amongst the materials available for implant applications, the natural selection of titanium-based materials for implantation, is due to the combination of its outstanding characteristics such as high strength, low density (high specific strength), high immunity to corrosion, complete inertness to body environment, enhanced biocompatibility, low modulus and high capacity to join with bone and other tissues [98] Coming to Ti alloys. Their youngs modulus varying from 110 to 55 GPa compared to 316 L stainless steel (210 GPa) and chromium cobalt alloys (240 GPa), which have been used for the past several years is a very positive factor.
The modulus of elasticity of various biomedical alloys is compared with bone and shown in Fig. 6. Commercially pure Ti and Ti–6Al–4V ELI (Ti64, Extra Low interstitial) are most commonly used titanium materials for implant applications. The strength of the titanium alloys is very close to that of 316 L SS, and its density is 55% less than steel, hence, when compared by specific strength (strength per density), the titanium alloys outperform any other implant material. In addition, vanadium is also toxic both in the elemental state and oxides V2O5, which are present
Available Online at www.ijpret.com 23 surface in order to attain increased functional longevity of the implant in the human body. In short if we list out all the conclusions and decisions we can come in the conclusion that Knee joints that operate as dynamically loaded bearing are subjected to 108 cycles of loading in 70-year lifetime. The average coefficient of friction of the load bearing synovial joints such as hip and knee is about 0.02. On the other hand, the coefficient of friction for implant materials varies from 0.16 to 0.05 depending upon the materials that are in contact and the kind of lubricant used for testing From the implant retrieval studies of femoral head of cobalt–chrome– molybdenum (Co–Cr–Mo), 316L stainless steel (SS) and titanium –aluminium – vanadium (Ti– 6Al–4V) alloy that were loosened by aseptic loosening, it was noted that
Titanium alloy femoral heads consistently had the maximum wear averaging 74.3% against high molecular weight polyethylene acetabular component.[84]
Co–Cr alloy was found to wear the least and wear of SS was in between Co–Cr and Ti alloy.[86]
Further, high metal concentrations were found in tissue taken from the region around Ti alloy prostheses, while, the metals debris level were low in the tissues surrounding the CoCr and SS that were articulating against polyethylene [89]
.Metal on metal prostheses is found to produce 20–100 times lower wear volumes compared to metal on polyethylene bearing. [91]
The biological reaction to metal particles in vivo has been shown to be markedly different to that produced by UHMWPE wear debris and lower inflammatory reactions are found to be caused by metal. However, it has also been observed that
Metal on metal prosthesis exhibits high frictional torques than the metal on polymer .[46]
Though the metal on metal prosthesis produces low wear volume, there is concern for the effect of the metal particles released after long duration.[64]
Both the in vivo and in vitro studies have shown that CoCr particles have toxic effects on different cells and tissues. [58]
Available Online at www.ijpret.com 24 When the toxicity of CoCr wear particles of nanometre size was tested for its
cytocompatibility, it showed high toxicity when compared to the ceramic wear particles that were obtained from the implant made of alumina. The other ceramic material used for implant applications is zirconia, which was considered to be a better alternative for alumina as alumina is highly brittle. [32]
Zirconia exhibits best mechanical properties and have high resistance to crack propagation. Today more than 6,00,000 zirconia head implants have been fixed and it is more frequently used in USA and Europe than any other countries. [69]
Metal on metal pair exhibited high friction coefficient when tested with CMC and lowest wear rate when tested in bovine serum[41].
Wapner reviewed the toxic effects of metals viz., Ni, Co and Cr released from prosthetic implants. Skin related diseases such as dermatitis due to Ni toxicity have been reported and numerous animal studies have shown arcinogenicity due to the presence of Co. In addition, [52]
Both 316L SS and Cr–Co alloys possess much higher modulus than bone, leading to insufficient stress transfer to bone leading to bone resorption and loosening of implant after some years of implantation. [46]
The high cycle fatigue failure of hip implants is also reported as the implants are subjected to cycles of loading and unloading over many years. Their youngs modulus varying from 110 to 55 GPa compared to 316 L stainless steel (210 GPa) and chromium cobalt alloys (240 GPa),. [61]
The strength of the titanium alloys is very close to that of 316 L SS, and its density is 55% less than steel, hence, when compared by specific strength (strength per density), the titanium alloys outperform any other implant material. In addition, [94]
Vanadium is also toxic both in the elemental state and oxides , which are present at the surface. Further, titanium has poor shear strength, making it less desirable for bone screws, plates and similar applications. [59]
Available Online at www.ijpret.com 25 modulus and high capacity to join with bone and other tissues. which have been used for the past several years is a very positive factor. Commercially pure Ti and Ti–6Al–4V ELI (Ti64, Extra Low interstitial) are most commonly used titanium materials for implant applications
Future work
Extensive research is presently being carried out to improve the wear parameter of biomaterials.
o Though due to the lack of appropriate protocol for measurements of wear property of metallic biomedical materials at present, only
o Comparative studies are carried out at different conditions of loading and environment.
o More research on development of an appropriate protocol for measuring the wear property should be performed for development of an alloy with better wear resistance.
o The performance of titanium and its alloys can be enhanced profoundly by developing an appropriate surface treatment procedure that will lead to increased wear resistance and Osseo integration.
o It can be suggested that in future, greater focus should be made on the areas of development of very hard nano surface of appropriate hardness on frictional parts and the formation of biomimetic surface in order to attain increased functional longevity of the implant in the human body.
REFERENCES
1. Kulkarni Mukta , Mazar Anca et. Al; Biomaterial surface modification oftitanium and titanium alloys for medicalapplications; anomedicine;2010
2. Bakir M. Haemocompatibility of titanium and its alloys. J. Biomater. Appl. 2012; 27: 3–15. 3. Blombäck B, Hessel B, Hogg D, Therkildsen L. A two-step fibrinogen–fibrin transition in blood coagulation. Nature 1978; 275: 501–505.
4. Roy S, Paulose M, Grimes C. The effect of TiO2 nanotubes in the enhancement of blood clotting for the control of hemorrhage. Biomaterials. 2007; 28(31): 4667–72.
Available Online at www.ijpret.com 26 6. Branemark P, Hansson B, Adell R, Breine U, Lindstrom J, Hallen O, Ohman A. Osseointegrated implants in the treatment of edentulous jaw. Scand. J. Plast. Reconstr. Surg. Suppl. 1977; 16: 1– 132.
7. Xiao S-J, Kenausis G, Textor M. Titanium in Medicine: Material Science, Surface Science, Engineering, Biological Responses and Medical Applications (eds. eds. Brunette D M, TengvallP, Textor M, Thompson P), Springer-Verlag, Berlin and Heidelberg 2001; 417–455.
8. Mas-Moruna C, Espanol M, Montufar E, Mestres G, Aparicio C, Javier F, Ginebra M. Biomaterials Surface Science (eds. Taubert A, Mano J F, Rodríguez-Cabello J C), Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim 2013; 337–374.
9. Anderson J M, Cristina A G, Hanson S R, Harker L A, Johnson R J, Merritt K, Naylor P T, Schoen F J. Biomaterials Science: An Introduction to Materials in Medicine (eds. Ratner B D, Hoffman A S, Schoen F J, Lemons J E) Academic Press 1997; 165–214.
10. Vasilev K, Poh Z, Kant K, Chan J, Michelmore A, Losic D. Tailoring the surface functionalities of titania nanotube arrays. Biomaterials 2010; 31: 532–540.
11. Cochran D , Schenk R, Lussi A, Higginbottom F, Buser D. Bone response to unloaded and loaded titanium implants with a sandblasted and acid-etched surface: A histometric study in the canine mandible. J. Biomed. Mater. Res. 1998; 40: 1-11.
12. Ivanoff c , Hallgren C, Widmark G, Sennerby L, Wennerberg A. Histologic evaluation of the bone integration of TiO 2 blasted and turned titanium microimplants in humans. Clin. Oral Implants Res. 2001; 12: 128-134.
13. Gongadze E, Kabaso D, Bauer S, Slivnik T, Schmuki P, van Rienen U, Iglič A. Adhesion of osteoblasts to a nanorough titanium implant surface. Int. J. Nanomed. 2011; 6: 1801–1816. 14. Gongadze E, Kabaso D, Bauer S, Park J, Schmuki P, Iglič A. Adhesion of osteoblasts to a vertically aligned TiO2 nanotube surface. Mini Rev. Med. Chem. 2012; 13: 94–200.
15. Ueno T, Yamada M, Suzuki T, Minamikawa H, Sato N, Hori N, Takeuchi K, Hattori M, Ogawa T. Enhancement of bone–titanium integration profile with UV-photofunctionalized titanium in a gap healing model. Biomaterials 2010; 31: 1546-1557.
16. Schwarz F, Herten M, Sager M, Wieland M, Dard M, Becker J. Bone regeneration in dehiscence-type defects at chemically modified (SLActive) and conventional SLA titanium implants: a pilot study in dogs. J. Clin. Periodontol. 2007; 34(1): 78-86.
17. Zhao G, Schwartz Z, Wieland M, Rupp F, Geis-Gerstorfer J, Cochran D L, Boyan B D. High surface energy enhances cell response to titanium substrate microstructure. J. Biomed. Mater. Re.s A. 2005; 74(1): 49-58.
Available Online at www.ijpret.com 27 Brunette D M, Tengvall P, Textor M, Thompson P), Springer-Verlag, Berlin and Heidelberg 2001; 231–266.
19. Liu X, Chu P, Ding C. Surface modification of titanium, titanium alloys, and related materials for biomedical applications. Mater. Sci. Eng. R 2004; 47: 49–121
20. Bagno A, Bello C. Surface treatments and roughness properties of Ti-based biomaterials. J. Mater. Sci. Mater. Med. 2004; 15: 935-949.
21. Kim K H, Ramaswani N. Electrochemical surface modification of titanium in dentistry. Dent. Mater. J. 22 2009; 28(1): 20–36.
22. Diebold U. The surface science of titanium dioxide. 2003; 48: 53–229.
23. Puckett S D, Taylor E, Raimondo T, Webster T J. The relationship between the nanostructure of titanium surfaces and bacterial attachment. Biomaterials 2010; 31: 706–713. 24. Dale G R, Hamilton J W, Dunlop P S, Lemoine P, Byrne J A. Electrochemical growth of titanium oxide nanotubes: the effect of surface roughness and applied potential. J Nanosci. Nanotechnol. 2009; 9(7): 4215–4219.
25. Xiao S J, Textor M, Spencer N D, Sigrist H, Langmuir 1998; 14: 5507–5516.
26. Li P, Ohtsuki C, Kokubo T, Nakanishi K, Soga N. J. Am. Ceram. Soc. 1992; 75(8): 2094–2097. 27. Sul Y, Johansson C B, Jeong Y, Albrektsson T. Med. Eng. Phys. 2001; 23: 329–346.
28. Brinker C, Scherer G. Sol–Gel Science: The Physics and Chemistry of Sol–Gel Processing. American Press, San Diego; 1990.
29. Li P, Kangasniemi I, de Groot K, Kokubo T. Bonelike Hydroxyapatite Induction by a Gel-Derived Titania on a Titanium Substrate. J. Am. Ceram. Soc. 1994; 77: 1307–1312.
30. Ohring M. Materials Sciences of Thin Film: Deposition and Structure, Academic Press Ltd., Boston, 1992; 277.
31. Hampden-Smith M J, Kodas T T. Chemical Vapor Deposition of Metals: Part 2. Overview of Selective CVD of Metals. Chem. Vap. Deposition 1995; 1: 39-48.
32. Advincula M, Fan X, Lemons J, Advincula R. Surface modification of surface sol-gel derived titanium oxide films by self-assembled monolayers (SAMs) and non-specific protein adsorption studies. Colloids Surf. B Biointerfaces 2005; 42(1): 29–43
33. Yoshida K, Kamada K, Sato K, Hatada R, Baba K, Atsuta M. J. Biomed. Mater. Res. 1999; 48: 778–785.
34. Krzakala A, Kazek-Kesik A, Simka W. Application of plasma electrolytic oxidation to bioactive surface formation on titanium and its alloys. RCS Adv. 2013; 3: 19725-19743.
35. Morra M. Biochemical modification of titanium surfaces: peptides and ECM proteins. Eur. Cell Mater. 2006; 12: 1–15.
Available Online at www.ijpret.com 28 37. Bauer S, Schmuki P, von der Mark K, Park J. Engineering biocompatible implant surface: Part I:Materials and surfaces, Prog. Mater. Sci. 2013; 58: 261-326.
38. Schliephake H, Scharnweber D, Dard M, Sewing A, Aref A, Roessler S. Functionalization of dental implant surfaces using adhesion molecules. J. Biomed. Mater. Res. B 2005; 73(1): 88– 96. 39. Ruoslahti E. RGD and other recognition sequences for integrins. Annu. Rev. Cell Dev. Biol. 1996; 12: 697–715
40. D’Souza S E, Ginsberg M H, Plow E F. Arginyl-glycyl-aspartic acid (RGD): a cell adhesion motif. Trends Biochem. Sci. 1991; 16: 246–250
41. Li H, Khor K A, Cheang P. Titanium dioxide reinforced hydroxyapatitate coatings deposited by high velocity oxy-fuel (HVOF) spray. Biomaterials 2002; 23: 58–91.
42. de Groot K, Geesink R, Klein C P A T, Serekian P. Plasma-sprayed coatings of hydroylapatite J. Biomed. Mater. Res. 1987; 21: 1375–1391.
43. Gardon M, Guilemany J M. Milestones in Functional Titanium Dioxide Thermal Spray Coatings: A Review, JTTEES 2014; 23: 577–595.
44. Hussain T. Cold Spraying of Titanium: A Review of Bonding Mechanisms, Microstructure and Properties, Key Eng. Mater. 2012; 533: 53–90.
45. Chen Y M, Yu G P, Huang J H. Role of process parameters in the texture evolution of TiN films deposited by hollow cathode discharge ion plating. Surf. Coat. Technol. 2001; 141:156– 163.
46. Mediaswanti K, Wen C, Ivanova E, Berndt C, Wang J. Titanium Alloys – Advances in Properties Control (eds. Sieniawski J, Ziaja W), Intech, 2013; Available
from:http://www.intechopen.com/books/titanium-alloys-advances-in- propertiescontrol/sputtered-hydroxyapatite-nanocoatings-on-novel-titanium-alloys-for-biomedicalapplications
47. Applications 79. Rautray T R, Narayanan R, Kim K-H. Ion implantation of titanium based biomaterials. Prog. Mater. Sci. 2011; 56: 1137–1177.
48. Yamamoto H, Shibata Y, Miyazaki T. Anode glow discharge plasma treatment of titanium plates facilitates adsorption of extracellular matrix proteins to the plates. J.Dent. Res. 2005; 84: 668–671.
49. http://www.datamonitor.com.
50. Standard Terminology Relating to Wear and Erosion, Annual Book of Standards, Vol 03.02, ASTM, 1987, p 243-250
51. https://en.wikipedia.org/wiki/Wear
Available Online at www.ijpret.com 29 53. Stachowiak, G. W., and A. W. Batchelor (2005). Engineering Tribology. Burlington, Elsevier Butterworth-Heinemann
54. .( Sinmazcelik, T. and I. Taskiran (2007). "Erosive wear behaviour of polyphenylenesulphide (PPS) composites." Materials in engineering 28(9): 2471-2477
55. Clarke IC. Wear of polymeric prostheses—clinical reality, retrieved implants and laboratory predictions. Natl Bur Stand Spec Pub 1981;601:471–499.
56. Bigsby RJA, Hardaker CS, Fisher J. Wear of ultra-high molecular weight polyethylene acetabular cups in a physiological hip joint simulator in the anatomical position using bovine serum as a lubricant. Proc Inst Mech Eng Pt H 1997;211:265–269.
57. Clarke IC, Dai QC, Brahm A, Gustafson A. Effects of serum and water lubrication on PTFE/CoCr implants. Trans. Combined ORS Mtg., San Diego. Rosemont, IL: Orthop. Res. Society; 1995. p 204.
58. Derbyshire B, Fisher J, Dowson D, Hardaker C, Brummitt K. A comparative study of the wear of UHMWPE with zirconia ceramic and stainless steel femoral heads in artificial hip joints.Med Eng Phys 1994;16:229–36.
59. Wang A, Essner A, Stark C, Dumbleton JH. Comparison of the size and morphology of UHMWPE wear debris produced by a hip joint simulator under serum and water lubricated conditions. Biomaterials 1995;17:865–871.
60. Atkinson JR, Dowson D, Isaac GH, Wroblewski BM. Laboratory wear tests. II: A microscopical study of the surfaces of Charnley polyethylene acetabular sockets. Wear 1985;104:217–224.
61. Campbell P, Ma S, Yeom B, McKellop HA, Schmalzried T, Amstutz HC. Isolation of predominantly submicron-sized UHMWPE wear particles from periprosthetic tissues. J Biomed Mater Res 1995;29:127–131.
62. Campbell P, Doorn P, Dorey F, Amstutz HC. Wear and morphology of ultra-high molecular weight polyethylene wear particles from total hip replacements. Proc Inst. Mech Eng1996; 210:167–175.
63. Duff-Barclay I, Spillman DT. Total human hip joint prostheses—A laboratory study of friction and wear. Symp. In: Lubrication & Wear in Living & Artificial Human Joints. London: Institution of Mechanical Engineers; 1966.
64. Good V, Clarke IC Anissian L. Water and bovine serum lubrication compared in simulator PTFE/CoCr wear model. J Biomed Mater Res 1996;33:275–283.
Available Online at www.ijpret.com 30 66. Shanbhag AS, Jacobs JJ, Glant T, Gilbert JL, Black J, Galante JO. Composition and morphology of wear debris in failed uncemented total hip replacement. J Bone Joint Surg 1994;76- B:60–67.
67. Stachwaik, Gwidon W.; Batchelor, Andrew W. (2005). Engineering tribology (3rd ed.).
Elsevier Inc
68. Charnley J, Kamangar A, Longfield MD. The optimum size of prosthetic heads in relation to the wear of plastic sockets in total replacement of the hip. Med Biol Eng 1969;7:31–39.
69. Clarke IC, Good V, Anissian L, Gustafson A. Charnley wear model for validation of hip simulators—ball diameter versus polytetrafluoroethylene and polyethylene wear. Proc Inst Mech Eng 1997;211(H):25–36.
70. Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg 1990;72A:518–528.
71. Phipatanakul W, Johnson S, Good V, Clarke IC. The fallacy of evaluating biomaterial wear-rates with water as lubricant: A hip simulator study of alumina-PTFE and CoCr-PTFE combinations. J Biomed Mater Res 1998;39:229–233.
72. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. J Bone Joint Surg Am 2007;89:780–5.
73. Polineni VK, Wang A, Essner A, Stark C, Dumbleton JH. Effect of lubricant protein concentration on the wear of UHMWPE acetabular cups against cobalt-chrome and alumina femoral heads. Trans 23rd Annual Meeting of the Society for Biomaterials, New Orleans, LA; 1997. p 154.
74. Wang A, Polineni VK, Essner A, Stark C, Dumbleton JH. The impact of lubricant protein concentration on the outcome of hip joint simulator testing. In: 45th ORS, Anaheim, CA; 1999. p 52.
75. Wang A, Polineni VK, Essner A, Stark C, Dumbleton JH. Role of proteins and hyaluronic acid in the lubrication and wear of UHMWPE acetabular cups. Trans 24th Annual Meeting Society for Biomaterials; 1998. p 218.
76. Scholes SC, Unswrth A, Goldsmith AAJ. Phys Med Biol 2000;45:3721–35.
77. Margaret A, McGee Donald W, Howie, Costi Kerry, Haynes David R, Corinna I, et al. Wear 2000;241:158–65.
78. McCalden RW, Howie DW, Ward L, Subramanian C, Nawana NS, Pearcy MJ. In: Trans. 41st Ann. Meet. Orthop. Res. Soc., vol.20; 1995. p. 242.
79. Tipper JL, Firkins PJ, Ingham E, Fischer J, Stone MH, Farrar R. J Mater Sci: Mater Med 1999;10:353–62.
Available Online at www.ijpret.com 31 81. Akahori T, Niinomi M, Fukui H, Suzuki A, Hattori Y, Niwa S, et al. Titanium 2003 science and technology. Weinhem, Germany: Wiley VCH Verlag, GMBH and Co. KGaA; 2003.
82. ones DA. Principles and prevention of corrosion, 2nd ed., vol. 5. New Jersey: Prentice Hall; 1996. p. 75–115.
83. Clerc CO, Jedwab DW, Mayer PJ, Thompson, Stinson JS. J Biomed Mater Res 1997;38:229– 34.
84. Mueller HJ, Greener EH. J Biomed Mater Res 1970;4:29–41. 85. Blackwood DJ. Corros Rev 2003;21:97–124.
86. Probster L, Dent M, Lin WL, Huttenmann H. Int J Oral Max Impl 1992;7:390–4. 87. Yu J, Zhao ZJ, Li LX. Corros Sci 1993;35:587–97.
88. Wapner KL. Clin Orthop Relat Res 1991;271:12–20.
89. McGregor DB, Baan RA, Partensky C, Rice JM, Wibourn. Eur J Cancer 2000:307–13. 90. Teoh SH. Int J fatigue 2000;22(10):825–37.
91. Niinomi M. Met Mater Trans 2001;32A:477–86.
92. Eisenbarth E, Velten D, Muller M, Thull R, Breme J. Biomaterials 2004;25:5705–13.
93. Zinger O, Anselme K, Denzer A, Habersetzer P, Wieland M, Jeanfils J, et al. Biomaterials 2004;25:2695–711.
94. Jayaraman Mythili, Meyer Ulrich, Buhner Martin, Joos Ulrich, Wiesmann Hans-peter. Biomaterials 2004;25:625–31.
95. Brunette DM, Ratkay J, Chehroudi B. The bone–biomaterial interface. Toronto: University of Toronto Press; 1991. p. 49–61.
96. Pilliar RM. Implant Dent 1998;7:305–14.
97. Wennerberg A, Hallgren C, Johansson C, Daneli S. Clin Oral Implant Res 1998;9:11–9. 98. Martin JY, Schwartz Z, Hummert TW, et al. Clin Oral Implant Res 1995;29:389–93.
99. Buser D, Schenk RK, Stienemann S, Fiorelini JP, Fox CH, Stich H. J Biomed Mater Res 1991;25:889–902.
100. Mac Donald DE, Rapuano BE, Deo N, Stranick M, Somasundaram P, Boskey AL, et al. Biomaterials 2004;25:3135–46.
101.Prevey PS, Loftus EF, Hornbach DJ. J ASTM Int 2006:3.
102.Sauer BW, Weinstein AM, Klawitter JJ, Hulbert SF, Leonard RB, Bagwell JG. J Biomed Mater Res 1974;8:145–53
103.Li J, Liao H, Fartash B, Hermansson L, Johnsson. Biomaterials 1997;18:691–6.
104.Gotz HE, Muller M, Emmel A, Holzwarth U, Erben RG, Stangl R. Biomaterials 2005;25:4057– 64
Available Online at www.ijpret.com 32 106.Li SJ, Yang R, Ninomi M, Hao YL, Cui YY. Biomaterials 2004;25:2525–32
107.Kim HM, Miyaji F, Kokubo T, Nakamura T. J Biomed Mater Res 1996;32:409–17.
108.A. Wang, et.al, The Effects of Lubricant Composition on in Vitro Wear Testing of Polymeric Acetabular Components; 2003 Wiley Periodicals, Inc. J Biomed Mater Res Part B: Appl Biomater 68B: 45–52, 2004; accepted 29 May 2003
109.Shanbhag AS, Jacobs JJ; Standard Test Method for Wear Testing with a Pin-on-Disk Apparatus; Designation: G 99 – 95a (Reapproved 2000)
110.Roychowdhury Amit et.al; WEAR STUDIES OF FREQUENTLY USED IMPLANT MATERIALS; Trends Biomater. Artif. Organs. Vol.17(2) pp 135-140 (2004)
111.Philip J. Hyde et.al.; Wear characteristics of an unconstrained lumbar total disc