Enterocolitis in Preterm Infants
WHAT’S KNOWN ON THIS SUBJECT: Necrotizing enterocolitis (NEC) can present within thefirst week of life in term infants. In preterm infants, NEC usually appears after commencement of feeds and can occur between 2 and 3 weeks of life.
WHAT THIS STUDY ADDS: Among infants,33 weeks’gestation, NEC appears to occur at mean age of 7 days in more mature infants, whereas onset of NEC is delayed to 32 days of age in smaller, lower gestational age infants.
abstract
OBJECTIVES:To examine the variation in the incidence and to identify the timing of the presentation of necrotizing enterocolitis (NEC) in a cohort of preterm infants within the Canadian Neonatal Network (CNN).
METHODS:This was a population-based cohort of 16 669 infants with gestational age (GA),33 weeks, admitted to 25 NICUs participating in the CNN between January 1, 2003, and December 31,2008. Variations in NEC incidence among the participating NICUs for the study period were examined. We categorized early-onset NEC as occurring at,14 days of age and late-onset NEC occurring at$14 days. Multivariate logistic regression analysis was performed to identify risk factors for early-onset NEC.
RESULTS:The overall incidence of NEC was 5.1%, with significant var-iation in the risk adjusted incidence among the participating NICUs in the CNN. Early-onset NEC occurred at a mean of 7 days compared with 32 days for late-onset NEC. Early-onset NEC infants had lower incidence of respiratory distress syndrome, patent ductus treated with indomethacin, less use of postnatal steroids, and shorter duration of ventilation days. Multivariate logistic regression analysis identified that greater GA and vaginal delivery were associated with increased risk of early-onset NEC.
CONCLUSIONS:Among infants,33 weeks’gestation, NEC appears to present at mean age of 7 days in more mature infants, whereas onset of NEC is delayed to 32 days of age in smaller, lower GA infants. Further studies are required to understand the etiology of this dis-ease process.Pediatrics2012;129:e298–e304
AUTHORS:Wendy H. Yee, MD, FRCPC, MSc,aAmuchou Singh
Soraisham, MD, DM, FRCPC, MSc,aVibhuti S. Shah, MD,
MRCP, FRCPC,bKhalid Aziz, MBBS, FRCPC,cWoojin Yoon,
MSc,bShoo K. Lee, MBBS, FRCPC, PhD,band the Canadian
Neonatal Network
aDepartment of Pediatrics, Alberta Children’s Hospital Research Institute for Child and Maternal Health, University of Calgary, Alberta, Canada;bDepartment of Pediatrics, Maternal-Infant Care Center, Mount Sinai Hospital, University of Toronto, Toronto, Canada; andcDepartment of Pediatrics, University of Alberta, Alberta, Canada
KEY WORDS
necrotizing enterocolitis, preterm infant, incidence
ABBREVIATIONS BW—birth weight
CNN—Canadian Neonatal Network GA—gestational age
IVH—intraventricular hemorrhage NEC—necrotizing enterocolitis PDA—patent ductus arteriosus RDS—respiratory distress syndrome SGA—small for gestational age SIP—spontaneous intestinal perforation
SNAP-II—Score for Neonatal Acute Physiology, version II VLBW—very low birth weight
Drs Yee and Soraisham were involved in the study conception, design, interpretation of data, and drafting the article; Drs Shah and Aziz contributed to the study conception, design, interpretation of data, and critical review of the article; and Drs Yoon and Lee were involved in acquisition of data, data analysis, interpretation of data, and critical review of the article.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-2022
doi:10.1542/peds.2011-2022
Accepted for publication Oct 11, 2011
Address correspondence to Wendy H. Yee, MD, FRCPC, MSc, Rockyview General Hospital, 63-7007 14 St SW, Calgary, AB, Canada T2V 1P9. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
Necrotizing enterocolitis (NEC) is one of the leading causes of morbidity and mortality in preterm infants.1–3 The
incidence of NEC has remained rela-tively stable over recent epochs in the very low birth weight (VLBW) infant po-pulations. The Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network reported gestational age (GA) specific mean incidence of NEC of 3% to 11% between 1997 and 20004and 5% to
15% between 2003 and 2007.5 Other
single centers and neonatal networks have reported similar incidence of NEC.6 –8One group9from Australia has
repor-ted a decrease in the incidence in NEC from 12% between 1992 and 1993 com-pared with 6% between 1998 and 1999 for infants 24 to 28 weeks’gestation.9
Traditionally, NEC in the preterm infant is described in enterally fed infants occurring at several days, if not weeks of age.2,10Lin and Stoll,1in their review,
state that“the disease [NEC] is espe-cially poignant because it mainly affects premature infants who have survived the early neonatal period and subsequently face a disease with high morbidity and mortality.”The mortality for NEC can be as high as 50% and surgical treatment is necessary in almost 20% to 40%. The inverse re-lationship between GA and age of onset of NEC has been well documented,11,12
with term infants presenting with NEC in thefirst week of life. Based on recent clinical experience, we raise the ques-tion of whether there is an earlier on-set of NEC emerging in the VLBW infant population as some infants appear to be presenting with NEC in thefirst week of life.
Sankaran et al13 reported that there
was no significant variation in the risk adjusted incidence of NEC among Ca-nadian NICUs. Since that publication, the number of participating NICUs in the Canadian Neonatal Network (CNN) has increased from 17 to 25. By using
this expanded network cohort we un-dertook this study (1) to examine the variation in the incidence and (2) to identify the timing of the presentation of NEC in a national population-based co-hort of infants,33 weeks’GA admitted to participating NICUs of the CNN.
METHODS Study Population
This population-based cohort included 16 669 infants with GA,33 weeks ad-mitted to 25 NICUs participating in the CNN between January 1, 2003, and De-cember 31, 2008.
Data Collection
The CNN maintains an established na-tional database for the purposes of outcomes evaluation, benchmarking, and quality improvement. Data for CNN are collected from patient charts by trained data abstractors at each of the participating NICUs in accordance to the manual of standardized operational definitions for variables and outcomes defined by the CNN. Details of data collection and data management have been published elsewhere.14 Ethical
approval was obtained from the in-stitutional review board of all partici-pating institutions.
Definitions
Indices of neonatal outcome were
de-fined according to the CNN Data Ab-stractor Manual.14 GA was calculated
from the best obstetric estimate based on early prenatal ultrasound exami-nation, obstetric examiexami-nation, and ob-stetric history, if the postnatal pediatric estimate of gestation differed from the obstetric estimate by more than 2 weeks, the pediatric estimate was used. NEC was defined according to modified Bell’s criteria ($ stage 2),15
and patent ductus arteriosus (PDA) was defined as clinical diagnosis plus treatment with indomethacin, surgical
ligation, or both. Bronchopulmonary dysplasia was defined as requirement for oxygen at 36 weeks’corrected GA16
or at discharge from the participating unit. Retinopathy of prematurity was di-agnosed according to the international classification of retinopathy of pre-maturity.17 Diagnosis and severity of
intraventricular hemorrhage (IVH) was based on the criteria of Papile.18
Se-verity of illness was measured by the Score for Neonatal Acute Physiology, version II (SNAP-II) as described by Richardson et al.19Small for GA (SGA)
was defined as birth weight (BW)
,10th percentile for the given GA, and outborn status was defined if the infant was born at a hospital different from the one in which the participating NICU was located. Congenital anomalies were identified from a defined list within the CNN database.
Data Analysis
We performed 2 separate analyses to identify: (1) risk factors for NEC, and (2) risk factors for early-onset NEC.
In thefirst analysis, univariate analyses were performed to describe the char-acteristics of the study population and to explore associations between pop-ulation characteristics and NEC. Multi-variate logistic regression model was used to identify risk factors for NEC. The variables shown to be significantly different (P,.05) between the infants diagnosed with NEC and those without NEC in the univariate analyses were selected as possible risk factors for NEC and entered in the model.
Variations in NEC incidence among the participating NICUs for the study period were examined by looking at crude and risk adjusted odds ratios for the NEC incidence, where the site with median incidence rate was chosen as the ref-erence site. Variables included in the adjusted model were GA, Apgar score at 5 minutes, SNAP-II, girl, cesarean de-livery, outborn infant, and SGA.
fi
8 days of age and the second peak around at 19 days of age. The least overlap between the 2 distributions was noted to be at day 14. Based on this cutoff, we categorized early-onset NEC as oc-curring at ,14 days of age and late-onset NEC occurring at $14 days. A second analysis was restricted to the subset of infants with NEC. In this second analysis, univariate analyses were per-formed to explore the characteristics of infants with early- and late-onset NEC. Multivariate logistic regression analysis was performed to identify risk factors for early-onset NEC. Significant variables (P,.05) identified on univariate anal-yses were entered into the regression model. Statistical significance was con-sidered to be present at the levelP,
.05. Statistical analysis was performed by using SAS version 9.2 (SAS Institute, Inc, Cary, NC) software package.
RESULTS
NEC in the Cohort
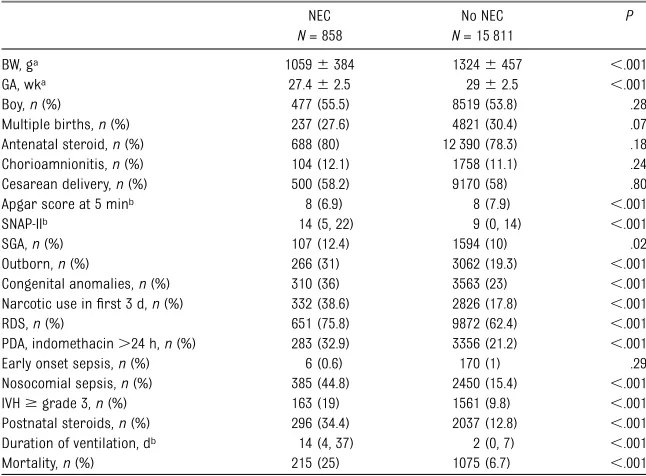
Of the 16 669 preterm infants ,33 weeks admitted during the study pe-riod, 858 (5.1%) infants had NEC $ stage 2. Baseline characteristics and clinical outcomes of infants with and without NEC are presented in Table 1. The neonatal factors significantly cor-related with NEC were lower BW, GA, and 5-minute Apgar score, higher ad-mission SNAP-II, SGA infant, outborn infant, use of narcotic in thefirst 3 days of life, and postnatal steroid use. Clinical morbidities significantly associated with NEC were respiratory distress syndrome (RDS), PDA treated with in-domethacin after 24 hours of age, nosocomial infection, IVH $ grade 3, and more ventilation days. Mortality was significantly higher in infants with NEC compared with those without NEC. On multivariate logistic regression anal-ysis, risk factors for NEC were lower GA,
SGA infant, outborn infant, narcotic use during thefirst 3 days of life, postnatal steroid use, and presence of congenital anomalies (Table 2).
Variations in the Incidence of NEC The overall incidence of NEC was 858 of 16 669 (5.1%) with crude incidence varying from 1.3% to 12.9% (median 4.6%). Figure 1 shows that there was significant variation in the risk ad-justed incidences of NEC among the participating NICUs. Six NICUs had sig-nificantly increased incidence of NEC compared with the reference site with the median incidence rate, whereas 2 sites had lower incidence of NEC.
Early- Versus Late-Onset NEC The time of diagnosis of NEC (in days) was documented in 841 of 858 (98%) of infants. Of the 841 infants, 336 (40%) infants had early-onset NEC, whereas 505 infants had late-onset NEC. The mean (SD) age of diagnosis in the early-onset NEC group was 7.6 (3.1) days as compared with 32 (17.2) days among the late-onset NEC group. The incidence of surgical NEC was significantly higher in early-onset NEC group (40%) com-pared with late-onset NEC group (28%;
P, .001). Figure 2 shows the distri-bution of cases according to GA at birth and the postmenstrual age at the time of NEC diagnosis. The peak onset of NEC
BW, ga 10596384 13246457 ,.001
GA, wka 27.462.5 2962.5 ,.001
Boy,n(%) 477 (55.5) 8519 (53.8) .28
Multiple births,n(%) 237 (27.6) 4821 (30.4) .07
Antenatal steroid,n(%) 688 (80) 12 390 (78.3) .18
Chorioamnionitis,n(%) 104 (12.1) 1758 (11.1) .24
Cesarean delivery,n(%) 500 (58.2) 9170 (58) .80
Apgar score at 5 minb 8 (6.9) 8 (7.9) ,.001
SNAP-IIb 14 (5, 22) 9 (0, 14) ,.001
SGA,n(%) 107 (12.4) 1594 (10) .02
Outborn,n(%) 266 (31) 3062 (19.3) ,.001
Congenital anomalies,n(%) 310 (36) 3563 (23) ,.001
Narcotic use infirst 3 d,n(%) 332 (38.6) 2826 (17.8) ,.001
RDS,n(%) 651 (75.8) 9872 (62.4) ,.001
PDA, indomethacin.24 h,n(%) 283 (32.9) 3356 (21.2) ,.001
Early onset sepsis,n(%) 6 (0.6) 170 (1) .29
Nosocomial sepsis,n(%) 385 (44.8) 2450 (15.4) ,.001
IVH$grade 3,n(%) 163 (19) 1561 (9.8) ,.001
Postnatal steroids,n(%) 296 (34.4) 2037 (12.8) ,.001
Duration of ventilation, db 14 (4, 37) 2 (0, 7) ,.001
Mortality,n(%) 215 (25) 1075 (6.7) ,.001
aMean6SD.
bMedian (interquartile range).
TABLE 2 Risk Factors for NEC From Multivariate Logistic Regression Analysis
Adjusted Odds Ratio (95% Confidence Interval) P
GA 0.84 (0.81–0.87) ,.001
SGA 1.35 (1.08–1.69) .007
Narcotics infirst 3 d 1.97 (1.67–2.32) ,.001
Outborn 1.55 (1.31–1.83) ,.001
Postnatal steroids 1.71 (1.43–2.06) ,.001
PDA treated with indomethacin 0.98 (0.82–1.16) .84
Apgar at 5 min 1.03 (0.98–1.07) .16
SNAP-II 0.99 (0.99–1.003) .36
RDS 1.12 (0.93–1.36) .22
in this cohort was ∼32 weeks’ post-menstrual age.
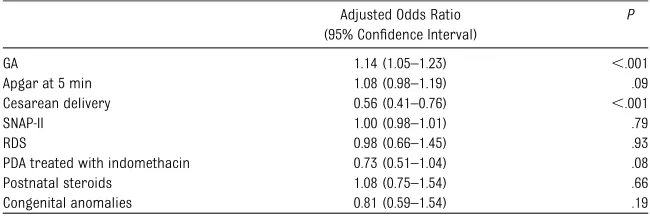
As shown in Table 3, early-onset NEC infants were of greater BW and GA, had higher 5-minute Apgar score, were more likely to be delivered vaginally, had lower SNAP-II, and had a lower rate of congenital anomalies on univariate analysis. Compared with late-onset NEC infants, the early-onset NEC infants had lower incidence of RDS, PDA treated with indomethacin after 24 hours of age, less use of postnatal steroids, and shorter duration of ventilation days (Table 4). Multivariate logistic regression analysis identified that greater GA and vaginal delivery were associated with increased risk of early-onset NEC. Post-natal steroid use was not associated
with early-onset NEC. There was a trend toward reduction in risk of early-onset NEC in infants with PDA treated with in-domethacin (Table 5).
DISCUSSION
The overall incidence of NEC was 5.1% in this national population cohort of infants,33 weeks’GA, which is within the range reported by other large network databases and single cen-ters.4,5,7,8There was a significant
vari-ation in the risk adjusted incidence of NEC among the 25 NICUs within the CNN. Our findings are consistent with the Eunice Kennedy Shriver Na-tional Institute of Child Health and Human Development neonatal network
who report persistent variation across sites in the incidence of NEC in VLBW infants.4,5
The authors of previous epidemiologic studies11,12,20have described early- and
late-onset NEC with early-onset NEC presenting in thefirst week of life in term infants. Studies of lower GA and lower BW infants reveal mean or me-dian age of occurrence of NEC ranging from 13 to 23 days.11,12,20–22In his
re-view, Neu2describes“classic”NEC
oc-curring in preterm infants after 8 to 10 days of age. The peak onset of NEC at postmenstrual age of 32 weeks is similar to that reported previously.11
Our data suggest that a different profile and presentation of NEC has emerged in this population of preterm infants,33 weeks’gestation. There remains an in-verse relationship between GA/BW and onset of NEC, but the timeline has shifted such that the preterm infants with BW
.1000 g present with NEC at a mean of 7 days (early onset) and NEC is delayed until a mean of 32 days (late onset) in lower GA infants with BW ,1000 g. Grosfeld et al23reported on a 25-year
cohort of infants with surgical NEC and identified average age at diagnosis of 13 days for infants with BW.1000 g and 21 days for infants with BW,1000 g.
In the late 1980s and early 1990s, reports of focal intestinal perforation began emerging.24–27 The authors of
sub-sequent studies began to make the as-sociation between this entity and use of indomethacin and postnatal steroids.28,29
The term spontaneous intestinal perfo-ration (SIP) has also been used to de-scribe this lesion, which occurs in preterm infants, receiving minimal teral feeds or before receiving any en-teral feeds and occurring in the first week of life. The incidence of SIP has been difficult to ascertain because it can only be confirmed histologically with laparot-omy.30Surgical management of intestinal
perforation with intraperitoneal drain cannot reliably confirm the diagnosis.
FIGURE 1
Risk adjusted incidence of NEC by hospital for neonates,33 weeks’GA. (Adjusted for GA, Apgar score at 5 minutes, SNAP-II, girl, cesarean delivery, and SGA.) Hospital sites are on the x-axis, and the odds ratio (95% confidence interval) is on the y-axis.
FIGURE 2
Distribution of cases of NEC according to GA and postmenstrual age (PMA) in the study cohort.
Because most neonatal networks and single centers,4–8including CNN, have
not reported an overall increase in NEC $stage 2 and 1 group reported a de-crease,9this suggests that if SIP is
misclassified and disproportionately contributing to the incidence of stage 3 surgical NEC, the incidence of stage 2 nonsurgical NEC must be decreasing globally. Alternatively, if SIP contributes marginally to the overall incidence of NEC, we should consider the possibility
of existence of an early-onset NEC that occurs in VLBW preterm infants pre-senting in the first 2 weeks of life at a mean of 7 days postnatal.
In our study, early-onset NEC occurred in 40% of the cohort. From multivariate analysis, the independent risk factors for early-onset NEC were greater GA and vaginal delivery. There was a trend to lower risk of NEC in infants with PDA treated with indomethacin. This as-sociation of decreased NEC with PDA
independently associated with onset NEC. Therefore, even if early-onset NEC represented misclassified SIP, the described risk factors of in-domethacin and postnatal steroids treatment were not significantly asso-ciated with early-onset NEC in our co-hort. Our data do not permit us to distinguish between early postnatal steroid use for treatment of hypoten-sion compared with later treatment of bronchopulmonary dysplasia and this may explain the lack of association between postnatal steroids and early-onset NEC.
We do not know why vaginal delivery is a risk factor for early onset NEC. We speculate that the early-onset NEC group were more mature, larger BW infants and probably more likely to be delivered vaginally. The“apparent paradox” of these vaginally delivered infants developing early-onset NEC may be related to feeding practices. Enteral feeding has been associated with NEC as most infants developing NEC have been fed. We speculate that more ma-ture and potentially more stable infants could have been given enteral feeds earlier with more aggressive volume advancement. There is
con-flicting evidence as to whether these are risk factors associated with NEC. Recent meta-analyses32,33 do not con-firm that early trophic feeds or rate of feeding advancements are associated with NEC. Exclusive breast milk feeds have been identified as protective for development of NEC compared with mixed feeds or formula feeds.34,35More
aggressive advancement of feeds with suboptimal breast milk volumes may have resulted in supplementation with formula feeds.36In a recent study, only
30% of mothers were able to provide sufficient breast milk to their extremely premature infants.37
BW, ga 11606435 9926328 ,.001
GA, wka 2862.7 2762.3 ,.001
Boy,n(%) 197 (58.6) 272 (53.8) .18
SGA,n(%) 36 (10.7) 70 (13.8) .17
Multiple gestations,n(%) 99 (29.4) 130 (25.7) .24
Cesarean delivery,n(%) 179 (53.2) 316 (62.5) .005
Antenatal steroid,n(%) 270 (80.3) 407 (80.5) .81
Chorioamnionitis,n(%) 34 (10.1) 69 (13.6) .12
Apgar score at 5 minb 8 (7, 9) 7 (6, 8) ,.001
SNAP-IIb 10 (0, 21) 14 (7, 24) .01
Outborn,n(%) 109 (32.4) 151 (29.9) .40
Congenital anomalies,n(%) 106 (31.5) 200 (39.6) .01
aMean6SD.
bMedian (interquartile range).
TABLE 4 Comparison of Clinical Outcomes Between Early and Late NEC Group Early-Onset NEC
N= 336
Late-Onset NEC
N= 505
P
RDS,n(%) 235 (69.9) 400 (79.2) .004
PDA, indomethacin.24 h,n(%) 89 (26.4) 186 (36.8) .001
Early onset sepsis,n(%) 1 (0.3) 5 (1) .41
Nosocomial sepsis,n(%) 145 (43) 233 (46) .39
Narcotic use infirst 3 d,n(%) 133 (39.5) 194 (38.4) .73
IVH$grade 3,n(%) 62 (18.4) 98 (19.4) .78
Postnatal steroids,n(%) 100 (29.7) 193 (38.2) .01
Duration of ventilation, da 9 (3, 27) 20 (5, 42) ,.001
Mortality,n(%) 92 (27.3) 121 (23.9) .26
aMedian (interquartile range).
TABLE 5 Risk Factors for Early NEC From Multivariable Logistic Regression Analysis Adjusted Odds Ratio
(95% Confidence Interval)
P
GA 1.14 (1.05–1.23) ,.001
Apgar at 5 min 1.08 (0.98–1.19) .09
Cesarean delivery 0.56 (0.41–0.76) ,.001
SNAP-II 1.00 (0.98–1.01) .79
RDS 0.98 (0.66–1.45) .93
PDA treated with indomethacin 0.73 (0.51–1.04) .08
Postnatal steroids 1.08 (0.75–1.54) .66
The authors of recent reviews1–3,10
dis-cuss the multifactorial pathogenesis of NEC and suggest the complex interplay between immature gastrointestinal tract with associated immature muco-sal barrier, immune defense, circulatory regulation, altered microbiota, infl am-matory response, and genetics along with the more traditional putative fac-tors of hypoxic-ischemic injury and en-teral feeding in the host preterm infant. This raises the possibility that NEC is a developmental phenomenon with GA interacting with perinatal events, such as bacterial colonization and use of perinatal antibiotics that may influence the microbiota of the immature gut.
It is possible that NEC represents 2 or more different conditions, in differing patient populations, with differing eti-ologies. Gordon et al30has suggested
that NEC represents a disease entity within a spectrum of conditions affecting the neonatal gut, which they have termed “acquired neonatal intestinal disease.” SIP may be part of this spectrum of con-ditions. The association between surgical NEC and poorer neurodevelopmental outcome as compared with no NEC has been reported.38 Others have reported
poorer neurodevelopmental outcome in patients with surgical NEC as compared with SIP.39The expression of NEC and the
long-term outcomes may depend on the underlying etiology in the population af-fected.
Strengths of this study include the large size cohort, the standardization of definitions of neonatal morbidities, and the quality of the CNN database in a regionalized healthcare system.
The definition of early- versus late-onset NEC derived from dichotomizing the cohort at 14 days is not based on any physiologic principle but on an
inspection of our data. The distinction between stage 3 surgical NEC with in-testinal perforation and SIP requiring surgical intervention cannot be de-lineated in our network population co-hort. Data are not available to describe the relationship between type, timing, and rate of advancement of feeds and development of NEC. These are signifi -cant limitations of this study. Our study data do not allow for reporting of long-term neurodevelopmental outcomes in infants with NEC. Network databases, including the CNN, may have to consider stratification of these disease entities to better identify risk factors and predict long-term outcomes.
CONCLUSIONS
The overall incidence of NEC within the CNN is similar to other centers and networks. Within a cohort of preterm infants,33 weeks’GA, NEC appears to present at a mean of 7 days (early on-set) in more mature preterm infants and is delayed to 32 days (late onset) in lower BW, lower GA preterm infants. This early-onset NEC represents a shift in the timing of traditional preterm NEC. Fur-ther studies are required to understand the etiology of this disease process.
ACKNOWLEDGMENTS
The Maternal-Infant Care Research Cen-ter is supported by the Ministry of Health and Long-term Care, Ontario, Canada.
Site Investigators of the Canadian Neo-natal Network were as follows: Shoo K. Lee (Director, Canadian Neonatal Net-work); Prakesh S. Shah (Associate Di-rector, Canadian Neonatal Network); Wayne Andrews (Janeway Children’s Health and Rehabilitation Centre, St John’s, NF, Canada); Francine Lefebvre
(Sainte Justine Hospital, Montreal, QC, Canada); Nalini Singhal (Foothills Medi-cal Centre, Calgary, AB, Canada); Barbara Bullied (Everett Chalmers Hospital, Fredericton, NB, Canada); Rody Canning (Moncton Hospital, Moncton, NB, Canada); Gerarda Cronin (St Boniface General Hospital, Winnipeg, MB, Canada); Kim-berly Dow (Kingston General Hospital, Kingston, ON, Canada); Michael Dunn (Sunnybrook Health Sciences Centre, Toronto, ON, Canada); Adele Harrison (Victoria General Hospital, Victoria, BC, Canada); Andrew James (Hospital for Sick Children, Toronto, ON, Canada); Zarin Kalapesi (Regina General Hospi-tal, Regina, SK, Canada); Lajos Kovacs (Jewish General Hospital, Montreal, QC, Canada); David Lee (St Joseph’s Health Centre, London, ON, Canada); Douglas D. McMillan (Izaak Walton Killam Health Centre, Halifax, NS, Canada); Prakesh Shah (Mount Sinai Hospital, Toronto, ON, Canada); Cecil Ojah (St John Re-gional Hospital, St John, NB, Canada); Khalid Aziz (Royal Alexandra Hospital, Edmonton, AB, Canada); Bruno Pied-boeuf (Centre Hospitalier Universitaire de Québec, Sainte Foy, QC, Canada); Pat-ricia Riley (Montreal Children’s Hospital, Montreal, QC, Canada); Daniel Faucher (Royal Victoria Hospital, Montreal, QC, Canada); Nicole Rouvinez-Bouali (Child-ren’s Hospital of Eastern Ontario, Ottawa, ON, Canada); Koravangattu Sankaran (Royal University Hospital, Saskatoon, SK, Canada); Mary Seshia (Health Sci-ences Centre, Winnipeg, MB, Canada); Sandesh Shivananda (Hamilton Health Sciences Centre, Hamilton, ON, Canada); Todd Sorokan (Royal Columbian Hospi-tal, New Westminster, BC, Canada); and Anne Synnes (Children’s and Women’s Health Centre of British Columbia, Van-couver, BC, Canada).
REFERENCES
1. Lin PW, Stoll BJ. Necrotising enterocolitis.
Lancet. 2006;368(9543):1271–1283
2. Neu J, Walker WA. Necrotizing enterocolitis.
N Engl J Med. 2011;364(3):255–264
3. Schnabl KL, Van Aerde JE, Thomson AB,
4. Fanaroff AA, Stoll BJ, Wright LL, et al; NICHD Neonatal Research Network. Trends in neonatal morbidity and mortality for very low birthweight infants.Am J Obstet Gynecol. 2007;196(2):147–148, e1–e8
5. Stoll BJ, Hansen NI, Bell EF, et al; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Neonatal outcomes of extremely preterm infants from the NICHD Neonatal Research Network. Pediatrics. 2010;126(3):443–456
6. Guthrie SO, Gordon PV, Thomas V, Thorp JA, Peabody J, Clark RH. Necrotizing enteroco-litis among neonates in the United States. J Perinatol. 2003;23(4):278–285
7. Horbar JD, Badger GJ, Carpenter JH, et al; Members of the Vermont Oxford Network. Trends in mortality and morbidity for very low birth weight infants, 1991-1999. Pedi-atrics. 2002;110(1 pt 1):143–151
8. Wilson-Costello D, Friedman H, Minich N, et al. Improved neurodevelopmental out-comes for extremely low birth weight infants in 2000-2002. Pediatrics. 2007;119 (1):37–45
9. Luig M, Lui K; NSW & ACT NICUS Group. Epidemiology of necrotizing enterocolitis— part I: changing regional trends in extre-mely preterm infants over 14 years. J Paediatr Child Health. 2005;41(4):169–173
10. Thompson AM, Bizzarro MJ. Necrotizing enterocolitis in newborns: pathogenesis, prevention and management.Drugs. 2008; 68(9):1227–1238
11. Llanos AR, Moss ME, Pinzòn MC, Dye T, Sinkin RA, Kendig JW. Epidemiology of neonatal necrotising enterocolitis: a pop-ulation-based study. Paediatr Perinat Epi-demiol. 2002;16(4):342–349
12. Stoll BJ, Kanto WP, Jr;Glass RI, Nahmias AJ, Brann AW Jr;. Epidemiology of necrotizing enterocolitis: a case control study.J Pediatr. 1980;96(3 pt 1):447–451
13. Sankaran K, Puckett B, Lee DS, et al; Canadian Neonatal Network. Variations in incidence of necrotizing enterocolitis in Canadian neonatal intensive care units. J Pediatr Gastroenterol Nutr. 2004;39(4):366–372
14. Lee SK, McMillan DD, Ohlsson A, et al. Var-iations in practice and outcomes in the Canadian NICU network: 1996-1997. Pediat-rics. 2000;106(5):1070–1079
15. Walsh MC, Kliegman RM. Necrotizing en-terocolitis: treatment based on staging criteria.Pediatr Clin North Am. 1986;33(1): 179–201
from oxygen requirement in the neonatal period.Pediatrics. 1988;82(4):527–532
17. International Committee for the Classifi ca-tion of Retinopathy of Prematurity. The In-ternational Classification of Retinopathy of Prematurity revisited. Arch Ophthalmol. 2005;123(7):991–999
18. Papile LA, Munsick-Bruno G, Schaefer A. Relationship of cerebral intraventricular hemorrhage and early childhood neuro-logic handicaps.J Pediatr. 1983;103(2):273– 277
19. Richardson DK, Corcoran JD, Escobar GJ, Lee SK. SNAP-II and SNAPPE-II: simplified newborn illness severity and mortality risk scores.J Pediatr. 2001;138(1):92–100
20. Teasdale F, Le Guennec JC, Bard H, Per-reault G, Doray B. Neonatal necrotizing en-terocolitis: the relation of age at the time of onset to prognosis.Can Med Assoc J. 1980; 123(5):387–390
21. Snyder CL, Gittes GK, Murphy JP, Sharp RJ, Ashcraft KW, Amoury RA. Survival after necrotizing enterocolitis in infants weigh-ing less than 1,000 g: 25 years’experience at a single institution.J Pediatr Surg. 1997; 32(3):434–437
22. Uauy RD, Fanaroff AA, Korones SB, Phillips EA, Phillips JB, Wright LL; National Institute of Child Health and Human Development Neonatal Research Network. Necrotizing enterocolitis in very low birth weight infants: biodemographic and clinical cor-relates.J Pediatr. 1991;119(4):630–638
23. Grosfeld JL, Cheu H, Schlatter M, West KW, Rescorla FJ. Changing trends in necrotizing enterocolitis. Experience with 302 cases in two decades. Ann Surg. 1991;214(3):300– 306, discussion 306–307
24. Aschner JL, Deluga KS, Metlay LA, Emmens RW, Hendricks-Munoz KD. Spontaneous fo-cal gastrointestinal perforation in very low birth weight infants.J Pediatr. 1988;113(2): 364–367
25. Buchheit JQ, Stewart DL. Clinical compari-son of localized intestinal perforation and necrotizing enterocolitis in neonates. Pedi-atrics. 1994;93(1):32–36
26. Mintz AC, Applebaum H. Focal gastrointes-tinal perforations not associated with necrotizing enterocolitis in very low birth weight neonates. J Pediatr Surg. 1993;28 (6):857–860
27. Novack CM, Waffarn F, Sills JH, Pousti TJ, Warden MJ, Cunningham MD. Focal intestinal perforation in the extremely-low-birth-weight infant.J Perinatol. 1994;14(6):450–453
in extremely low birth weight infants. J Perinatol. 2001;21(3):156–160
29. Shorter NA, Liu JY, Mooney DP, Harmon BJ. Indomethacin-associated bowel perfora-tions: a study of possible risk factors. J Pediatr Surg. 1999;34(3):442–444
30. Gordon PV, Swanson JR, Attridge JT, Clark R. Emerging trends in acquired neonatal intestinal disease: is it time to abandon Bell’s criteria?J Perinatol. 2007;27(11):661– 671
31. Sharma R, Hudak ML, Tepas JJ III, et al. Prenatal or postnatal indomethacin expo-sure and neonatal gut injury associated with isolated intestinal perforation and necrotizing enterocolitis.J Perinatol. 2010; 30(12):786–793
32. Bombell S, McGuire W. Early trophic feeding for very low birth weight infants.Cochrane Database Syst Rev. 2009;(3):CD000504
33. McGuire W, Bombell S. Slow advancement of enteral feed volumes to prevent necrot-ising enterocolitis in very low birth weight infants.Cochrane Database Syst Rev. 2008; (2):CD001241
34. Lucas A, Cole TJ. Breast milk and neonatal necrotising enterocolitis. Lancet. 1990;336 (8730):1519–1523
35. Sullivan S, Schanler RJ, Kim JH, et al. An exclusively human milk-based diet is asso-ciated with a lower rate of necrotizing en-terocolitis than a diet of human milk and bovine milk-based products. J Pediatr. 2010;156(4):562–567, e1
36. Stout G, Lambert DK, Baer VL, et al. Nec-rotizing enterocolitis during thefirst week of life: a multicentered case-control and cohort comparison study.J Perinatol. 2008; 28(8):556–560
37. Schanler RJ, Lau C, Hurst NM, Smith EO. Randomized trial of donor human milk versus preterm formula as substitutes for mothers’own milk in the feeding of ex-tremely premature infants. Pediatrics. 2005;116(2):400–406
38. Hintz SR, Kendrick DE, Stoll BJ, et al; NICHD Neonatal Research Network. Neurodevel-opmental and growth outcomes of ex-tremely low birth weight infants after necrotizing enterocolitis. Pediatrics. 2005; 115(3):696–703
DOI: 10.1542/peds.2011-2022 originally published online January 23, 2012;
2012;129;e298
Pediatrics
Yoon, Shoo K. Lee and the Canadian Neonatal Network
Wendy H. Yee, Amuchou Singh Soraisham, Vibhuti S. Shah, Khalid Aziz, Woojin
Infants
Incidence and Timing of Presentation of Necrotizing Enterocolitis in Preterm
Services
Updated Information &
http://pediatrics.aappublications.org/content/129/2/e298 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/129/2/e298#BIBL This article cites 39 articles, 9 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2011-2022 originally published online January 23, 2012;
2012;129;e298
Pediatrics
Yoon, Shoo K. Lee and the Canadian Neonatal Network
http://pediatrics.aappublications.org/content/129/2/e298
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.