suspected. Only one infant who had an intra
cranial
hemorrhage
at autopsy
(case
1, Table
I)
did not have a difference
in the percentages
of
fetal hemoglobin
in spinal
fluid and circulating
blood,
a
false-negative
test.
However,
the
patient's
clinical
course
suggested
the intraven
tricular
hemorrhage
occurred
after
his
initial
transfusion
and
that
the
lumbar
puncture
was
performed
prior to any subsequent
transfusions.
Mixing of hemorrhagic
spinal fluid and systemic
blood during lumbar
puncture
might also reduce
the difference
in the percentages
of fetal hemo
globin in blood and spinal fluid, also yielding
a
false-negative
test.
Changes in the percentage
of fetal hemoglobin
following several transfusions
were determined
in
one patient
(Fig. 2). By 18 hours of age, only 40%
of the circulating
hemoglobin
was fetal.
Since
96% of the spinal
fluid hemoglobin
obtained
at
this time was fetal, we concluded that the intra
ventricular hemorrhage occurred prior to 18
hours
of age. By collecting
samples
of blood
prior
to each transfusion
in a group of infants
at high
risk
of
having
intracranial
hemorrhage,
we
believe
this
technique,
together
with
clinical
signs,
might
establish
the
time
of
bleeding.
However,
the use of the
test
in this way
has
certain limitations.
Repeated
episodes of bleeding
into the spinal
fluid or mixing
of hemorrhagic
spinal
fluid and systemic
blood
at the time
of
lumbar
puncture
might
suggest
that
the
initial
bleeding
episode took place at a later age than it
actually
had occurred.
Despite
possible
limitations
of the
test
for
estimating the tinie intracranial hemorrhages
occur,
the
comparison
of the
percentages
in
samples
of blood
and
hemorrhagic
spinal
fluid
appears
to be a useful
way
to differentiate
a
subarachnoid
hemorrhage
from
a
traumatic
lumbar
puncture
in infants
who have
been
trans
fused.
EDWARD R. CHAPLIN, M.D.
MUREEN A. SCHLUETER, B.S.
RODERIC H. PHLBBS, M.D.
JOSEPH
A. KITTERMAN,
M.D.
WILLIAM H. TOOLEY, M.D.
Cardiovascular
Research
Institute
and the Depart
ments of Pediatrics
and
Neurology,
University
of California
San Francisco, California
Supported b@ NHL1 Pulmonary SCOR grant HL 14201
and Child Health and Human Development grant HD
00397. Dr. Chaplin is the recipient of a National Institutes of
Health Special Postdoctoral Fellowship Award (1 Fli
NS
02745) and Dr. Phibbs is the recipient of a National Institutes of Health Career Development Award (HD 18275).
ADDRESS FOR REPRINTS: (E.R.C.) Department of
Neurology, University of California, San Francisco, Cali fornia 94143.
REFERENCES
1. Gröntoft 0: Intracerebral and meningeal haemorrhages in perinatally deceased infants: I. Intracerebral
haeniorrhages. Acta Obstet Gynecol Scand 32:303,
1953.
2. Larroche JC: Hémorragies cérébralesintraventricu laires chez le premature. I. Anatonlie et physiopa thologie. Biol Neonate 7:26, 1964.
3. Amid C: Héniorragies cérébralesintraventriculaire chez Ic premature: II. Les elements du diagnostic
clinique. Biol Neonate 7:57, 1964.
4. Ross JJ, Dirnmette RM: Subependymal cerebral hemor
rhage in infancy. Am J Dis Child 110:531, 1965.
5. Towbin A: Cerebral intraventricular hemorrhage and
slll)ependvmal infarction in the fetus and prema
tore newborn. Am J Pathol 52:121, 1968. 6. Valdes-Dapena MA, Arey JB: The causes of neonatal
mortality: An analysis of 501 autopsies on newborn
infants. J Pediatr 77:366, 1970.
7. Fredrick J, Butler WR: Causes of neonatal death: II. Intraventricular haemorrhage. Biol Neonate
15:257, 1970.
8. Larroche JC: Post-haemorrhagic hydrocephalus in infancy: Anatomical study. Biol Neonate 20:287,
1972.
9. Oski FA, Naiman JL: Hematological Problems in the Newborn. Philadelphia, WB Saunders Co. 1972, p 135.
10. Chaplin ER, Schlueter MA, Phibbs RH, et al: The use of CSF fetal hemoglobin to differentiate pathological
subarachnoid bleeding from traumatic lumbar
punctures. Clin Res 23:158A, 1975.
11. Jonxis JHP, Huisman TH: The detection and estimation of fetal hemoglobin by means of the alkali denatu ration test. Blood 11:1006, 1956.
12. Lorber J, Bahat US: Post-hemorrhagic hydrocephalus. Arch Dis Child 49:751, 1975.
Intussusception
in Twins
The risk of intussusception
occurring
in the
siblings
of
patients
with
intussusception
is
thought
to be low, and there
is no previous
report
of the condition
occurring
in twins.
In our case the second twin was affected within
36 hours
of the onset
in the first. Adenovirus
was
cultured
from
the
one
twin
who
was
investi
gated.
754
PEDIATRICS
Vol. 58 No. 5 November1976
at Viet Nam:AAP Sponsored on September 8, 2020
www.aappublications.org/news
FIG. 1. Barium enema outlining intussusception in twin A.
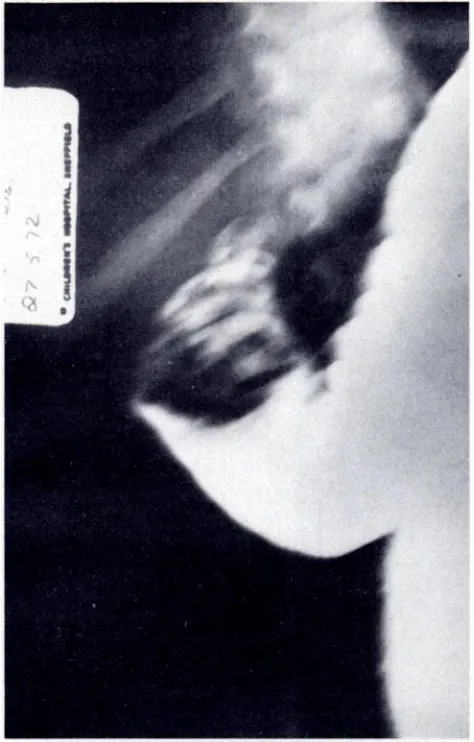
FIG. 2. Barium enema outlining intussusception near hepatic flexure in twin B.
CASEREPORT
The twins were identical boys of West Indian descent, 25 months of age, born and bred in England. They were perfectly well until the early hours of May 26, 1972, when
twin A began to scream with acute abdominal pain. He was
admitted to hospital within 18 hours and by that time he had
vomited four times and had passed six loose stools, the last
two containing blood.
Examination revealed an ill-looking boy, with a tempera
ture of 39.6 C and a pulse rate of 100 beats per minute. There was a nontender ITLISSlying across the epigastriiim and on rectal examination blood was present. Hemoglobin was 10 gm/100 flll and the WBC was 5,500/cu mm with 58%
polymorphonuclear leukocytes, 1% eosinophils, 1% baso
phils, 34% lymphocytes, and 6% monocytes.
Shortly after admission a barium enema confirmed an
intussusception with the apex in the transverse colon (Fig. 1). The intussusception was partly reduced by the barium enema, but a filling defect was still present in the cecum, and at operation the intussusception was confirmed and reduced
easily, having started in the terminal ileum. It was noted that
there were masses of enlarged nodes in the mesentery. Twin B presented at 2 @sion May 27th within 36 hours of the onset of the condition in twin A. There was a five-hour
history of episodes of crying and drawing up his knees. He
had vomited twice and passed two stools consisting of mucus and blood only. Examination revealed a healthy-looking boy, with a temperature of 37.5 C, and a pulse rate of 100 beats
per minute.
He was tender on the right side of the abdomen with a
suspicion of a mass in the right hypochondrium. Rectal
examination revealed the presence of blood. Hemoglobin was 9.0 gm/100 ml and WBC 5,500/cu mm with 41% lynl phocytes and 12% monocytes.
A barium enema revealed a picture similar to that of the other twin, with the apex of the intussusception reaching the
transverse colon (Fig. 2). The intussusception was partly
reduced by the barium enema but still left a filling defect in the cecum and final reduction had to be undertaken by
operation, when it was found that the intussusception had
started in the terminal ileum.
The Peyer's patches were very enlarged, and one Peyer's
patch at the apex of the intusSu.sception felt almost like a foreign body. The mesenteric lymph nodes were also grossly enlarged. The appendix and one mesenteric node were re moved for virology studies.
Both twins made an uneventful recovery before discharge
EXPERIENCE AND REASON
755
at Viet Nam:AAP Sponsored on September 8, 2020
www.aappublications.org/news
together on June 5, 1972. A heavy growth of adenovirus was
obtained from the appendix and also from the mesenteric
lymph nodes. The antibody titers for twin B were less than 1:20 in all viruses tested (adenovirus, mumps virus V, mumps virus 5, herpes simplex virus, measles, varicella-zoster and
cox.sackie). It had been intended to undertake a study of
antibody titers in both twins: unfortunately the laboratory
staff thought a mistake had been made in sending a second
specimen with the same surname and discarded it, not realizing that this was from twin A, and there was a similar failure to undertake studies of convalescent serum.
DISCUSS1ON
Intussusception
occurring
in siblings has been
described.
MacMahon'
described
eight families in
which the siblings were affected
in a series of 296
confirmed cases of intussusception. Clos& found
five cases in siblings in 363 cases (a very low ratio)
and
Hogg
and
DonovanI
described
three
cases
arising
in
relatives
of
123
patients.
Ravitch4
concluded
that “¿there
is no evidence
that there is
any increased likelihood of intussusception in a
sibling
once a child in a family
has been
affected,―
but MacMahon
estimated
the risk to siblings as 1
in 40, about
15 to 20 times the incidence
in the
general
population.
No reference
has been
found
relating
to intus
susception
in twins.
The lymph
nodes
and
Peyer's
patches
were
very
enlarged
ih
both
twins,
and
the
Peyer's
patches
seemed
to be the leading
points
in the
intussusception.
The
enlargement
of
this
lym
phoid tissue is likely to be associated
with a recent
infection
and many observers
have drawn
atten
tion
to the
role of viruses
in the
etiology
of
intussusception.3'
Indeed, Potter and Zachary'
were able to demonstrate
an adenovirus
in the
feces, throat
swabs, or mesenteric
nodes in more
than 50% of cases of intussusception,
compared
with 3% in children
admitted
to the hospital
with
various
other
conditions,
including
respiratory
infections.
It seems remarkable,
therefore,
that
Dennison
and Shaker― were
unable
to find virus
infection
in children
with
intussusception
more
frequently
than
in a series
of controls.
The presence
of enlarged
lymphoid
tissue and
the positive culture
of virus from both these cases
is in itself suggestive that the infection was an
important
etiological
factor.
The
onset
of the
disease in the second twin within 36 hours of the
onset
in the first twin
strengthens
this view.
GARETH G. THOMAS, F.R.C.S.
R. B. ZACHARY, F.R.C.S.
Sub-Department
of Pediatric
Surgery,
University
of Sheffield,
and the Children's
Hospital
Sheffield, England
ADDRESS FOR REPRINTS: (R.B.Z.) The Children's Hospital, Western Bank, Sheffield 10, England.
REFERENCES
1. MacMahon B: Data on the etiology of acute intussuscep tion in childhood. Am J Hum Genet 7:430, 1955. 2. Close HG: Acute intussusception in children. Guy's
Hosp Rep 81:436, 1931.
3. Hogg BM, Donovan EJ: Acute intussusception in infants and children. Ann Surg 124:262, 1946.
4. Ravitch MM: Intussusceptiori in Infants and Children. Springfield, Illinois, Charles C Thomas, 1959. 5. Clarke EJ, Phillips IA, Alexander ER: Adenovirus infec
tion in intussusception in children in Taiwan.
JAMA 208:1671,1969.
6. Strang R: Intussusception in infancy and childhood. Br J Surg 46:484, 1959.
7. Bell TM, Steyn JH: Viruses in lymph nodes of children with mesenteric adenitis and intussusception. Br
Med J 2:700, 1962.
8. Gardiner PS, Knox EG, Court SDM, Green CA: Virus
infection and intussusception in childhood. Br Med
J 2:697, 1962.
9. PotterCW, Zachary RB: The etiology of intussuscep
tion: With particular attention to the adenovirus infectiolls. Surg Clin North Am 44:1509, 1964.
10. Dennison WM, Shaker M: Intussusception in infancy and childhood. Br J Surg 57:679, 1970.
756
INTUSSUSCEPTION IN TWINS
at Viet Nam:AAP Sponsored on September 8, 2020
www.aappublications.org/news
1976;58;754
Pediatrics
Gareth G. Thomas and R. B. Zachary
Intussusception in Twins
Services
Updated Information &
http://pediatrics.aappublications.org/content/58/5/754
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on September 8, 2020
www.aappublications.org/news
1976;58;754
Pediatrics
Gareth G. Thomas and R. B. Zachary
Intussusception in Twins
http://pediatrics.aappublications.org/content/58/5/754
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 1976 by the
been published continuously since 1948. Pediatrics is owned, published, and trademarked by the
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
at Viet Nam:AAP Sponsored on September 8, 2020
www.aappublications.org/news