SPECIAL ARTICLE
Part-Time Training in Pediatric Residency Programs:
Principles and Practices
Mary Beth Gordon, MDa,b, Gail A. McGuinness, MDc, Bonita F. Stanton, MDb,d, Susan Brooks, BAa, Vincent W. Chiang, MDa, Robert Vinci, MDa,
Theodore C. Sectish, MDa,b
aBoston Combined Residency Program in Pediatrics (Department of Pediatrics, Boston University School of Medicine and Boston Medical Center, and Department of
Medicine, Harvard Medical School and Children’s Hospital Boston), Boston, Massachusetts;bFederation of Pediatric Organizations Task Force on Women in Pediatrics,
Chapel Hill, North Carolina;cAmerican Board of Pediatrics, Chapel Hill, North Carolina;dDepartment of Pediatrics, Children’s Hospital of Michigan and Wayne State
University School of Medicine, Detroit, Michigan
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
Despite growing interest in part-time work, few pediatricians are pursuing part-time residency training. There is currently little guidance for programs or residents who wish to design an alternative path through residency. In this article we review the need for part-time residencies and address obstacles to be overcome in their initia-tion. Strategies are offered for residents and program directors planning part-time training pathways, with recommendations for implementation amid a changing environment for graduate medical education. The needs of trainees, residency pro-grams, hospitals, and credentialing organizations are considered.Pediatrics2008;122: e938–e944
P
ART-TIME RESIDENCIES HAVE been implemented in a variety of specialties since the 1970s. Changing demographics, including more women in medicine and new generations concerned with lifestyle management, suggest that interest in this training option will grow.1 With its high percentage of women physicians andprofessional focus on family health, pediatrics is likely to be at the leading edge of any movement to part-time training.2 Nevertheless, at present few pediatric programs
and even fewer residents are publicly using reduced-hours schedules, and there is little guidance for how to do so effectively.3,4
It is our goal to review the growing need for part-time solutions and to address the potential pitfalls. Because each program is structured differently, individual programs will need to create solutions that work in their own environment. We hope to encourage this practice by sharing examples of successful models of part-time train-ing, including reduced-hours, shared positions, and prolonged or variable periods of absence.
WHAT IS THE DEMAND FOR PART-TIME TRAINING?
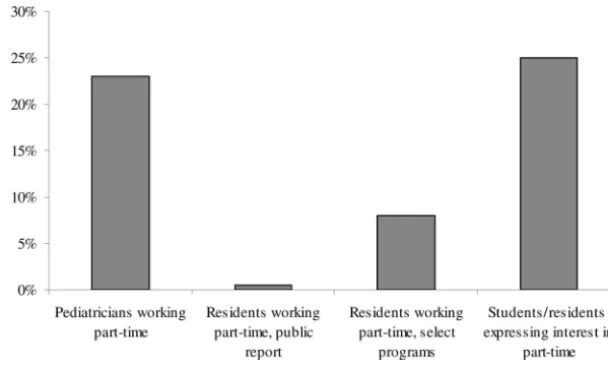
Evidence suggests that there is unmet demand for part-time work during residency. Medical students report strong interest in part-time training and are increasingly choosing specialties with controllable lifestyle.5,6Beyond residency,
23% of board-certified pediatricians are working part-time (up from 11% in 1993).7–9Nevertheless, currently only
12% of pediatric programs report offering part-time schedules, and fewer than 1% of pediatric residents report working part-time.3,4Fig 1 summarizes these data.
Demographic and cultural trends indicate that this demand may increase. Female gender is a strong predictor of seeking part-time employment, and in the last 15 years the proportion of female pediatrics residents has grown from 58% to 72%.9,10Although to a lesser extent than women, young male physicians also increasingly seek part-time
work, possibly reflecting changing cultural norms in the era of the dual-career family.5,9,11
In 2 large pediatric programs (our own Boston Combined Residency Program and the University of California San Francisco [UCSF]) that have offered a “blocks on/blocks off” training schedule after internship, 8% to 9% of residents elected this option. In the UCSF report of their 10-year experience, an additional 7.4% of residents using the regular schedule regretted not taking advantage of the option.12
Looking to other fields, it is interesting to examine general surgery. The implementation of the 80-hour workweek in 2003 represented a 20% decrease in general surgery residents’ hours, but applications to general surgery residencies have remained stable.13,14 Whether additional lifestyle enhancements during training would affect
applications to this or any specialty is unclear. Still, in a national survey of surgical trainees conducted after 2003, 25% of female and 13% of male residents expressed interest in a part-time option (40 – 80 hours weekly, with a proportionate increase in length of residency).5The same authors found that 24% to 36% of medical students (male
www.pediatrics.org/cgi/doi/10.1542/ peds.2008-0719
doi:10.1542/peds.2008-0719
Key Words
part-time, medical residency, graduate medical education, pediatric workforce
Abbreviations
UCSF—University of California, San Francisco
Match—National Resident Matching Program
ABP—American Board of Pediatrics ACGME—Accreditation Council for Graduate Medical Education RRC—Residency Review Committee FTE—full-time equivalent GME—Graduate Medical Education Accepted for publication Jun 6, 2007
Address correspondence to Mary Beth Gordon, MD, Children’s Hospital Boston, Department of Medicine, 300 Longwood Ave, Boston, MA 02115. E-mail: marybeth.gordon@ childrens.harvard.edu.
and female, respectively) agreed to increased interest in surgical careers if part-time training 40 to 80 hours per week were an option.5Smaller studies corroborate that
students believe work-hour limitations enhance the life-style of surgeons and make the field more attractive.15,16
On the basis of these data, we estimate that expand-ing and publicly offerexpand-ing part-time options may yield
⬃10% to 15% of residents arranging part-time training.
WHY PART-TIME TRAINING?
Taking a “big picture” view, one could argue that by incorporating part-time training pathways pediatrics as a field will attract and retain the best talent. For individual institutions, the sense of loyalty created by investment in balanced lifestyles during the period of training may create a long-term mutually beneficial and productive relationship.17 This may be particularly important for
encouraging women to pursue academic careers. As pediatricians we are also committed to the devel-opment of healthy families. We would be better able to role-model healthy family behaviors for our patients if we could provide employment structures for all of our physicians, including trainees, to satisfactorily attend to their home life. Indeed, the primary reason pediatricians seek part-time employment both during training and postresidency is to balance work and family responsibil-ities.3,7,9
Biologically this issue is most acute for women. Pro-longed absences from home and odd hours during train-ing necessitate special arrangements for child care and lactation. Classic reports raise concerns about the effect of prolonged work hours on the health of a pregnan-cy.18,19Similarly provocative work shows negative effects
of prolonged periods of nonmaternal care on some as-pects of infant social development.20–22
For all of these reasons the Federation of Pediatric Organizations Task Force on Women in Pediatrics and the Women Chairs Group of Association of Medical School Pediatric Department Chairs have both recently published consensus opinions endorsing the need to cre-ate part-time work options for pediatricians in training and beyond.17,23
OBSTACLES TO CREATING PART-TIME RESIDENCIES
Despite the apparent need, creating part-time solutions poses many challenges. Real and perceived obstacles likely contribute to current low utilization rates.
Knowledge and Access
From the perspective of residents, the first obstacle is awareness that a part-time option may exist. Although a program may formally report a part-time option, the failure to advertise it actively and/or the lack of partici-pating residents may create the impression that part-time employment is impossible. Medical student appli-cants may be educated about the availability of part-time options through the Fellowship and Residency Elec-tronic Information Database, via a program Web site, or via advisors at their school. It is therefore important for program directors to ensure that these information sources are updated.
Access to part-time internships or shared residencies is particularly problematic. Residency positions are ac-quired through a national matching system (National Resident Matching Program, “the Match”), which con-nects graduating medical students with residency pro-grams. Although there is a formal process for entering the Match as a pair applying to 1 full-time slot in a participating program, very few residency programs par-ticipate. There is also no national coordination effort to aid applicants in finding an appropriate counterpart. The partnering is critical because the overall potential for the dyad to match is generally based on the weaker appli-cant, and if the pair is matched to a full-time position, both individuals are bound by the terms of the Match to accept it.24,25If offering shared internships through the
Match, program directors must carefully evaluate each member of the dyad on individual merits. For this prac-tice to be disseminated, it will require additional educa-tion of program directors, such as occurs through efforts of the Association of Pediatric Program Directors.
Impact on the Resident
Even when in possession of the necessary knowledge and access to pursue part-time work, residents must
FIGURE 1
consider practicalities. Financially, residents may not be able to afford to work part-time, particularly if benefits are tied to a full salary.7The affordability of the part-time
option is a real problem to incoming residents, 85% of whom carry medical school debt, with a median of $140 000.26This problem is compounded by rising
inter-est rates and the elimination of deferment programs. Although some salary deficits can be bridged through moonlighting opportunities, this is not generally true for fringe benefits. The need for benefits to accompany sal-ary is especially important for health care coverage if the request for part-time work is related to the care of young children, who require significant routine health care. As a corollary, some may not wish to extend the period of training, either because of salary needs or future plans.5
Similarly, for residents studying in the United States from other countries, there are significant visa implica-tions for part-time pathways both as a function of ex-ceeding the duration of the visa and mandates for full-time employment. This is especially true for those with J1 visas, which do not allow part-time training.
Other concerns include completing residency “off-cycle,” which may affect fellowship applications or social relationships between residents. Residents may also fear that they would be perceived as overburdening full-time resident colleagues. In addition, physicians wishing to pursue research careers may believe that choosing or even investigating a part-time pathway may negatively impact their advancement.27–30
It should be noted that the presence of a part-time option, although engendering some feelings of resent-ment among colleagues, overall has been supported by full-time residents within the same program, who found the presence of the part-time option provided a sense of support that enabled them to cope with the stresses of residency.12
Program Considerations
Program directors, who need to balance training require-ments with hospital service needs, may not fully em-brace part-time training because of the complex admin-istrative challenges that customization imposes. These challenges encompass planning, scheduling, documen-tation, and expense. When an individual resident re-quests a modified work schedule, the impact on day and night staffing, documentation of competency, and fi-nances of paying the resident and any necessary replace-ment all must be considered. The customization process must be planned far enough in advance to consider workforce needs and allow for midtraining hires, in-creasing match numbers, advertising shared positions, or finding alternatives to house officers (eg, “physician ex-tenders”). Ideally, a program could hire enough resi-dents in advance to account for potential fluctuations in workforce, eg, because of parental leaves or midyear schedule reductions. This “buffer” may not be financially feasible for all programs.
Once a mutually satisfactory reduction in hours has been agreed on, an accommodating schedule and salary structure must be designed. The increased scheduling complexity on both a long-term planning and a daily
basis requires active management by appropriately trained staff. This is especially true if the part-time status varies over time for a single resident or if more than 1 resident is part-time and the same schedule is not used. During the implementation phase, monitoring progress toward the goals of physician competency must con-tinue. The growing availability of computerized sched-uling tools and competency-based assessments should ultimately aid in these at times cumbersome tasks. Fi-nally, maintaining strong communication about day-to-day residency issues and long-term planning issues is critical. Fortunately, the ubiquity of e-mail can facilitate such interactions when a part-time resident is off-cam-pus for a prolonged period: either direct explanations, invitations to “town meetings,” or minutes of meetings can keep everyone current.
Certification Considerations
The American Board of Pediatrics (ABP) is responsible for the certification of individuals and the assurance to the public and the profession that individuals have suc-cessfully completed an accredited educational program and have the knowledge, skills, attitudes, and behaviors to provide high-quality care. In 1992, the ABP began a robust tracking and evaluation program that requires program directors to provide yearly evaluations of the clinical competence and professional behavior of all res-idents and to indicate the number of months of training credit to be applied to the requirements for certification (33 months, with possible 2 months waived for family leave). The tracking program assures the appropriate monitoring is in place to permit deviations from the usual training pathways, such as part-time training. This system has enabled flexibility without compromising ed-ucational quality. Options currently include transferring from one program to another, taking a leave of absence, and engaging in part-time or shared training.
The Credentials Committee of the ABP will review plans for part-time or shared training opportunities on request. Although preapproval is not required, the ABP will advise on whether the proposed program ade-quately meets the goals of training. Program directors tend to contact the ABP when they are devising an unusual or complicated training structure (eg, night-call only without daytime responsibilities, or prolonged ab-sences). The program director should articulate a clear rationale for the training plan, address any potential concerns regarding diluted training or lack of immersion in the discipline, and must assure the ABP that the schedule will provide a full training experience, albeit on an extended time table. The program director must doc-ument annual progress reports and at the completion of training verify that the resident is competent to enter practice without direct supervision.
the traditional resident and engage in the same supervi-sory experiences and in a continuity clinic that is longi-tudinal in nature.
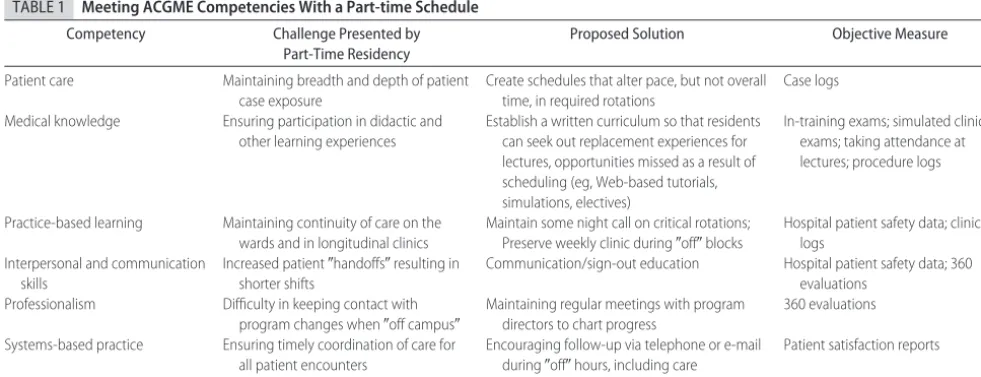
The ACGME has defined 6 competencies that must be achieved by the end of residency training: patient care, medical knowledge, practice-based learning and im-provement, interpersonal and communication skills, professionalism, and systems-based practice. The ABP and RRC further delineate specific pediatric training goals for each competency. A program must specifically document progress toward these goals. For each compe-tency, there are several principles underlying the RRC pediatric program requirements that must be carefully considered when customizing a part-time schedule. Meeting the competencies with a part-time schedule is potentially complex. Illustrative challenges posed by part-time training and examples of possible solutions are provided for each competency in Table 1.
It should be noted that part-time residents might best meet some competencies. Indeed, in a study of internal medicine residents, part-time trainees were rated higher than their counterparts in interpersonal skills and hu-manism.31This may represent a self-selection bias, closer
relationships with the advisors performing the evalua-tions, or perhaps decreased burnout among residents working part-time.
PART-TIME TRAINING IN PRACTICE
Although experience with part-time residencies is not broad, there are multiple existing models. We will dis-cuss here the job sharing model and its variations, as well as the impact of each model on the resident and program.
The job-sharing option may be conceived “in series” or “in parallel.” An “in series” model involves mixing blocks of time of full-time training with blocks of time off, in the model of “1-month on, 1-month off” or larger groups of blocks on and off. That is, for each month-long rotation, either 1 resident or the other is on duty. In a smaller program, this model may necessitate specific
pairing of 2 part-time residents so that rotation sched-ules remain intact. In 1 small program, a husband-wife team recently job-shared in this fashion so that 1 would always be home with their infant. In larger programs there may be sufficient interest in fractional positions that several residents can combine to create the appro-priate workforce. For example, 5 residents each working 0.8 full-time equivalents (FTEs) combine to work as 4 resident FTEs. This model preserves continuity within each rotation; however, it requires attention to main-taining a presence in longitudinal clinics during “off” months. With more residents to fill a stable number of full-time equivalents, a program may benefit from in-creased staffing flexibility. Some additional effort may be required to keep the residents connected to the program educationally and socially during the off months. This was the model chosen by UCSF, and of note, their board passage rates between “flexible option” and “regular schedule” residents did not differ significantly.12
The “in parallel” model has each resident sharing a role within a rotation schedule. In our program, we use this model to accommodate rotating family practice res-idents on our wards because this group must participate in more outpatient clinics during the week. In this ar-rangement, 2 residents are assigned the same schedule, and they work together to cover the same patient load. The night call is alternated between the 2, so that on an every fourth night rotation each individual takes call every eighth night. The daytime responsibilities are ei-ther shared during the day, or covered by 1 resident when the other must be off the ward. For pediatrics residents seeking more flexible time to attend to outside responsibilities or interests, this model reduces the fre-quency of evening call and provides more flexible time during the day (eg, if 1 resident needs to be home 1 afternoon, the other is available to cover patients). This system may also forge a bond between the sharing res-idents that may satisfactorily replace any loss of connect-edness to a class. This model works well for preserving continuity clinics, but requires more inpatient handoffs
TABLE 1 Meeting ACGME Competencies With a Part-time Schedule
Competency Challenge Presented by Part-Time Residency
Proposed Solution Objective Measure
Patient care Maintaining breadth and depth of patient case exposure
Create schedules that alter pace, but not overall time, in required rotations
Case logs
Medical knowledge Ensuring participation in didactic and other learning experiences
Establish a written curriculum so that residents can seek out replacement experiences for lectures, opportunities missed as a result of scheduling (eg, Web-based tutorials, simulations, electives)
In-training exams; simulated clinical exams; taking attendance at lectures; procedure logs
Practice-based learning Maintaining continuity of care on the wards and in longitudinal clinics
Maintain some night call on critical rotations; Preserve weekly clinic during⬙off⬙blocks
Hospital patient safety data; clinic logs
Interpersonal and communication skills
Increased patient⬙handoffs⬙resulting in shorter shifts
Communication/sign-out education Hospital patient safety data; 360 evaluations
Professionalism Difficulty in keeping contact with program changes when⬙off campus⬙
Maintaining regular meetings with program directors to chart progress
360 evaluations
Systems-based practice Ensuring timely coordination of care for all patient encounters
Encouraging follow-up via telephone or e-mail during⬙off⬙hours, including care coordination in sign-outs
that could potentially disrupt continuity of care to the detriment of the patient and/or to the resident’s educa-tion. It also may be more difficult for faculty to evaluate individuals with such an enmeshed patient load and with reduced overall contact.
Some programs have divorced day and night cover-age, allowing for an easier “shift work” approach to scheduling a part-time option. For example, on a sub-specialty rotation that has night and weekend call on the wards on an every fourth night basis, roughly one half of the time is spent on the daytime weekday rotation and the other half is spent on night and weekend call cov-erage. Therefore, splitting weekday daytime responsibil-ities on the subspecialty rotation from the night and weekend call can create 2 part-time positions each at 0.5 FTEs. Program directors must decide which rotations are amenable to such a split: some would argue that inpa-tient ward rotations are not amenable to a split because of the impact on continuity of care. Similar approaches to splitting full-time rotations into part-time rotations can be done on a rotation-by-rotation basis and the pro rata share apportioned to the split roles. The “split roles” model allows for a good degree of predictability in the schedule and minimal extended shifts, especially bene-ficial for those with child care responsibilities.
Pediatricians or physician extenders could be hired to supplement some or all of the uncovered service re-quirements of part-time residents. This approach was commonly employed in response to New York State work-hours restrictions initiated in 1989 (the “Libby Zion” law) and in response to the ACGME duty-hours restrictions in 2003, with approximately one third of pediatrics residency programs using this option32–34
Fol-low-up studies of residents and program directors in pediatrics and other fields employing nonphysicians in-dicate positive impact on resident education, quality of life, and career preparation.32,35To date, this option has
not been widely used specifically to allow for part-time training. This may be because of the relative infrequency of part-time residencies or to expense.
All of these options allow for varying the percentage of FTEs for an individual during part or all of residency. In aggregate, these options have delayed graduation by an average of 15 months.3
At the departmental level, these scheduling efforts need to be supported by appropriate assignment of ben-efits to make the option financially feasible both for the department and for the resident. Of note, the use of part-time pediatric residents should not impact a hospi-tal’s Graduate Medical Education (GME) funding, whether a stand-alone children’s hospital or a depart-ment within a general hospital. The funding is based on total full-time equivalents and is not specifically attached to individuals.
Establishing a time line within a department is critical for managing the complex logistics and smooth imple-mentation of part-time residencies. A program should plan to know as much as possible their staffing expecta-tions 9 months in advance of the upcoming academic year. This allows time for adjustment of numbers to match into an intern class, to recruit into an upper level
class, and/or to arrange job-share opportunities. The particulars of the part-time schedule should be sketched out at this time, including percentage of full-time and concomitant salary benefits, as well as the basic struc-ture, with actual day-to-day responsibilities filled in as the academic year approaches.
Although perfect knowledge 9 months in advance is impossible, our program uses some effective strategies that enhance our ability to anticipate future absence. These include a formal letter from the program directors sent in October requesting a commitment for the follow-ing academic year and a consideration of the likely num-ber of pregnancies. The “likely pregnancies” is a rela-tively stable number in our program year-to-year, representing 10% to 15% of female senior residents and 5% of female junior residents; annual estimates are bol-stered by a culture of confidence in our residency coor-dinator, who is often informed of an intention to become pregnant so that this information may be considered confidentially when arranging scheduling.
In current practice, the majority of part-time work is established after the intern year. This practice may exist because of lack of infrastructure for hiring part-time interns through the Match, or because the need for a part-time option does not become apparent and work-able until after one has already lived residency. In our experience, flexible schedules often arise as crisis inter-ventions. That is, a discussion about reduced workload too often occursaftera resident struggles with the stan-dard schedule. When proactive discussions of training trajectory are initiated, as part of a regular review, “part-time” is dissociated from failure, and becomes a positive intervention. Such proactive discussion may thus pre-vent considerable stress and frank morbidity among res-idents who desire increased flexibility, whereas at the same time allowing the program to better predict staffing needs and avoid overwhelming other residents who would otherwise need to cover in a pinch.
In addition to schedule planning, educational plan-ning is also critical. Changes in how we deliver educa-tion and monitor progress will contribute to improved feasibility of part-time residencies. Acquisition of factual medical knowledge during a nontraditional schedule may occur through a variety of offsite modalities both interactive (video-conferencing, video calls) and nonin-teractive (reading assignments, Web-casting lectures). Simulated training experiences (eg, with electronic pa-tients) are in increasing use to supplement training. This modality is useful for improving instruction and assess-ment in all of the competencies, and can be scheduled flexibly.36 As we move to competency-based assessment,
reliance on time-in-training to determine board eligibility may decline, thereby enhancing the feasibility of reduced-hours schedules for some residents. Competency-based as-sessment may even allow for academic credit for parental leave, during which many basic pediatric lessons are ab-sorbed.23 The trend toward creation of written curricula,
Such monitoring, at both the local and national levels, will be critical for the success of part-time programs.
SUMMARY AND RECOMMENDATIONS
There is a growing need for part-time training solutions in pediatrics. Although the current experience is limited, it provides some guidance with respect to successful implementation and potential pitfalls. Changes in the way education is delivered and assessed may enhance our ability to provide part-time training. We suggest the following for training programs:
Open Communication
Recognize the growing demand for alternative training schedules and maintain open communication about this option to maximize awareness. Indicate in your Web site and other materials available to resident applicants that you are willing to consider part-time residencies to en-able potentially interested residents/applicants to open the conversation. Proactively identify residents who may benefit from part-time training to optimize planning and implementation and to minimize resident stress.
Experimentation
Experiment with different schedules to benefit individ-ual residents and define best practice, being mindful of guiding principles of GME and patient care. Define spe-cific curriculum requirements and competencies. Em-brace technology allowing for flexible attainment of these goals and institute objective measures for moni-toring progress toward them.
Advocate
Advocate within the department and hospital for im-proved funding to cover additional costs that may arise when making part-time training financially feasible for residents (eg, benefits for part-time residents and/or ex-tended paid family leaves). GME committees may be of assistance when presenting these issues at a national level.
Although complex in initial implementation, part-time residencies will meet a growing demand for alter-native training options among medical school graduates and early-career pediatricians. Our ability as a profession to provide this option will allow us to meet our goals of attracting and maintaining a talented workforce, and promoting the health of all families.
REFERENCES
1. Jagsi R, Tarbell NJ, Weinstein DF. Becoming a doctor, starting a family: leaves of absence from graduate medical education. N Engl J Med.2007;357(19):1889 –1891
2. Sectish TC, Zalneraitis EL, Carraccio C, Behrman RE. The state of pediatrics residency training: a period of transformation of graduate medical education.Pediatrics.2004;114(3):832– 841 3. Holmes AV, Cull WL, Socolar RR. Part-time residency in
pediatrics: description of current practices. Pediatrics. 2005; 116(1):32–37
4. McPhillips HA, Burke AE, Sheppard K, Pallant A, Stapleton FB, Stanton B. Toward creating family-friendly work environ-ments in pediatrics: baseline data from pediatric department
chairs and pediatric program directors.Pediatrics.2007;119(3). Available at: www.pediatrics.org/cgi/content/full/119/3/e596 5. Saalwachter AL, Frieschlag JA, Sawyer RG, Sanfey HA.
Part-time training in general surgery: results of a Web-based survey. Arch Surg.2006;141(10):977–982
6. Dorsey ER, Jarjoura D, Rutecki GW. Influence of controllable lifestyle on recent trends in specialty choice by US medical students.JAMA.2003;290(9):1173–1178
7. Cull WL, Mulvey HJ, O’Connor KG, Sowell DR, Berkowitz CD, Britton CV. Pediatricians working part-time: past, present, and future.Pediatrics.2002;109(6):1015–1020
8. O’Connor KG, Cull WL, Sanford S. Trends in part-time em-ployment among pediatricians. Presented at: the 2007 Pediatric Academic Societies annual meeting. Available at: www.aap. org/research/abstracts/07abstract10.htm. Accessed May 27, 2008
9. Cull WL, Caspary GL, Olson LM. Many pediatric residents seek and obtain part-time positions.Pediatrics.2008;121(2):276 –281 10. American Board of Pediatrics. General pediatrics resident tracking. In:Workforce Data, 2007–2008.Chapel Hill, NC: Amer-ican Board of Pediatrics; 2008:31–32
11. Sanfey, HA, Saalwachter-Schulman AR, Nyhof-Young JM, Ei-delson B, Mann BD. Influences on medical student career choice: gender or generation? Arch Surg. 2006;141(11): 1086 –1094
12. Kamei RK, Chen C, Loeser H. Residency is not a race: our ten year experience with a flexible schedule residency training option.Acad Med.2004;79(5):447– 452
13. Whang EE, Perez A, Ito H, Mello MM, Ashley SW, Zinner MJ. Work hours reform: perceptions and desires of contemporary surgical residentsJ Am Coll Surg.2003;197(4):624 – 630 14. National Resident Matching Program. Applicants matched to
PGY-1 positions by specialty, 1999 –2007. Available at: www. nrmp.org/data/resultsanddata2007.pdf. Accessed May 2, 2008 15. Arnold MW, Patterson AF, Tang AS. Has implementation of the 80-hour work week made a career in surgery more appeal-ing to medical students?Am J Surg.2005;189(2):129 –133 16. Miller G, Bamboat ZM, Allen F, et al. Impact of mandatory
resident work hour limitations on medical students’ interest in surgery.J Am Coll Surg.2004;199(4):615– 619
17. Women Chairs of the Association of Medical School Pediatric Department Chairs. Women in pediatrics: recommendations for the future.Pediatrics.2007;119(5):1000 –1005
18. Klebanoff MA, Shiono PH, Rhoads GG. Outcomes of preg-nancy in a national sample of resident physicians.N Engl J Med. 1990;323(15):1040 –1045
19. Klebanoff MA, Shiono PH, Rhoads GG. Spontaneous and in-duced abortion among resident physicians. JAMA. 1991; 265(21):2821–2825
20. Brooks-Gunn J, Han WJ, Waldfogel J. Maternal employment and child cognitive outcomes in the first three years of life: the NICHD Study of Early Child Care. Child Dev. 2002;73(4): 1052–1072
21. Han WJ. Maternal non-standard work schedules and child cognitive outcomes.Child Dev.2005;76(1):137–154
22. Goldberg WA, Prause J, Lucas-Thompson R, Himsel A. Mater-nal employment and children’s achievement in context: a meta-analysis of four decades of research.Psychol Bull.2008; 134(1):77–108
23. Task Force on Women in Pediatrics. Report of the Task Force on Women in Pediatrics. Federation of Pediatric Organizations Newsletter. 2005, Number 6. Available at: www.ambpeds.org/ Site/education/education_FPO_newsletter.htm. Accessed Feb-ruary 18, 2008
25. National Resident Matching Program. Match participation agreements. Available at: www.nrmp.org/res㛭match/policies/ index.html. Accessed February 6, 2008
26. American Association of Medical Colleges. Medical school tu-ition and young physician indebtedness: an update to the 2004 report. Available at: https://services.aamc.org/Publications. Accessed May 22, 2008
27. Committee on Maximizing the Potential of Women in Aca-demic Science and Engineering.Beyond Bias and Barriers: Ful-filling the Potential of Women in Academic Science and Engineering. Washington, DC: National Academies Press; 2006
28. Socolar RR, Kelman LS, Lannon CM, Lohr JA. Institutional policies of U.S. medical schools regarding tenure, promotion, and benefits for part-time faculty. Acad Med. 2000;75(8): 846 – 849
29. Socolar RR, Kelman RS. Part-time faculty in academic pediat-rics, medicine, family medicine, and surgery: the views of the chairs.Ambul Pediatr.2002;2(5):406 – 413
30. Kaplan SH, Sullivan LM, Dukes KA, Phillips CF, Kelch RP, Schaller JG. Sex differences in academic advancement: results of a national study of pediatricians. N Engl J Med. 1996; 335(17):1282–1289
31. Carling PC, Hayward K, Coakley EH, Wolf AM. Part-time res-idency training in internal medicine: analysis of a ten-year experience.Acad Med.1999;74(3):282–284
32. Samuels RC, Chi GW, Rauch DA, Palfrey JS, Shelov SP. Les-sons from pediatrics residency program directors’ experiences with work hour limitations in New York State. Acad Med. 2005;80(5):467– 472
33. Cull WL, Mulvey HJ, Jewett EA, Zalneraitis EL, Allen CE, Pan RJ. Pediatric residency duty hours before and after limitations. Pediatrics. 2006;118(6). Available at: www.pediatrics.org/cgi/ content/full/118/6/e1805
34. Mathur M, Rampersad A, Howard K, Goldman G. Physician assistants as physician extenders in the pediatric intensive care unit setting: a 5-year experience.Pediatr Crit Care Med.2005; 6(1):14 –19
35. Buch KE, Genovese MY, Conigliaro JL, et al. Non-physician practitioners’ overall enhancement to a surgical resident’s ex-perience.J Surg Educ.2008;65(1):50 –53
DOI: 10.1542/peds.2008-0719 originally published online September 22, 2008;
2008;122;e938
Pediatrics
W. Chiang, Robert Vinci and Theodore C. Sectish
Mary Beth Gordon, Gail A. McGuinness, Bonita F. Stanton, Susan Brooks, Vincent
Part-Time Training in Pediatric Residency Programs: Principles and Practices
Services
Updated Information &
http://pediatrics.aappublications.org/content/122/4/e938
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/122/4/e938#BIBL
This article cites 26 articles, 5 of which you can access for free at:
Subspecialty Collections
dev_sub
http://www.aappublications.org/cgi/collection/teaching_curriculum_
Teaching/Curriculum Development
b
http://www.aappublications.org/cgi/collection/medical_education_su
Medical Education following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2008-0719 originally published online September 22, 2008;
2008;122;e938
Pediatrics
W. Chiang, Robert Vinci and Theodore C. Sectish
Mary Beth Gordon, Gail A. McGuinness, Bonita F. Stanton, Susan Brooks, Vincent
Part-Time Training in Pediatric Residency Programs: Principles and Practices
http://pediatrics.aappublications.org/content/122/4/e938
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.