The LIPPSMAck POP (Lung Infection Prevention Post Surgery Major Abdominal with Pre Operative Physiotherapy) trial: study protocol for a multi centre randomised controlled trial
Full text
Figure
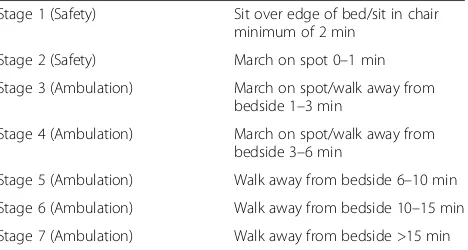
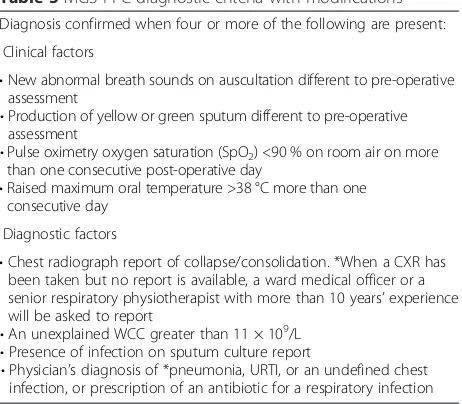
![Table 4 Discharge from physiotherapy scoring tool [62]](https://thumb-us.123doks.com/thumbv2/123dok_us/9035979.974703/8.595.55.286.96.425/table-discharge-from-physiotherapy-scoring-tool.webp)
Related documents
In the current study, we found oxidative damage to cells and molecular changes after injection with nanoparticles, which was asso- ciated with hepatic and renal tissue injury.
A new candidate of hybrid excitation flux switching motor (HE- FSM) at various rotor pole number such as 6S-4P, 6S-5P, 6S-7P, 6S-8P, 6S-14P, 4S- 4P, 4S-6P 4S-8P and 4S-10P
Oleh yang demikian, pengkaji akan menjalankan satu kajian bagi mengenalpasti tahap kompetensi guru yang mengajar pengajaran amali bagi mata pelajaran Reka Bentuk
Keywords: Active compliance, robotic hand, force control, impedance control, adaptive controller, passivity based
Abstract In this age, it is an accepted fact that architecture is not a phenomenon which comes into existence, only when it is constructed, but even the ideas which are at
To consider the behavior of young people – the majority, black favela residents – as suspicious is one of the common practices of these police officers, state employees who work
Annual fatality rates were calculated by dividing the number of deaths that resulted from severe cases of HFMD/herpan- gina for children who were younger than 15 years by the number
We have shown that the presence of the delayed feedback can change stability properties of the stationary localized structure leading to new complex instabilities which can
