Validation of Active Surveillance Testing for
Clostridium
difficile
Colonization Using the cobas Cdiff Test
Parul A. Patel,aDonna M. Schora,aKamaljit Singh,a,b,cLance R. Petersona,b,c
aDepartment of Laboratory Medicine and Pathology, NorthShore University HealthSystem, Evanston, Illinois, USA
bDepartment of Medicine, NorthShore University HealthSystem, Evanston, Illinois, USA cUniversity of Chicago Pritzker School of Medicine, Chicago, Illinois, USA
ABSTRACT Clostridium difficileinfection (CDI) is not declining in the United States. Nucleic acid amplification tests (NAAT) are used as part of active surveillance testing programs to prevent health care-associated infection. The objective of this study was to validate the cobas Cdiff Test on the cobas 4800 System (cobas) within a four-hospital system using prospectively collected perirectal swabs from asymptomatic patients at admission and during monthly intensive care unit (ICU) screening in an infection control CDI reduction program. Performance of the cobas was compared to that of toxigenic culture. Each positive cobas sample and the next following nega-tive patient swab were cultured. The study design gave 273 samples processed by both cobas (137 positive and 136 negative) and culture (one negative swab was not
cultured). Discrepant analysis was performed using a second NAAT, the XpertC.
diffi-cileEpi test (Xpert). This strategy was compared to a medical record review for
anti-biotic receipt that would inhibit growth of C. difficile in colonic stool. None of the
cobas-negative samples were culture positive. The cobas positive predictive value was 75.2% (95% confidence interval [CI], 66.9% to 82%) and positive percent agree-ment was 100% (95% CI, 96.0% to 100%). Overall agreeagree-ment between cobas and di-rect toxigenic culture was 87.6% (95% CI, 83.1% to 91%). For the cobas-positive/ culture-negative (discrepant) samples, 7 Xpert-positive samples were from patients receiving inhibitory antimicrobials; only 4 of 23 Xpert-negative samples received
these agents (P⫽ 0.00006). Our results support use of the cobas as a reliable assay
for an active surveillance testing program to detect asymptomatic carriers of
toxi-genicC. difficile.
KEYWORDS Clostridium difficile, colonization, asymptomatic, cobas 4800, active surveillance testing, real-time PCR
C
lostridium difficileis an important health care-associated pathogen known to causeC. difficileinfection (CDI), which is a spectrum of disease that ranges from moderate and severe diarrhea to pseudomembranous colitis, to toxic megacolon, and death. Frequency and severity of CDI have continued to increase in the United States and
worldwide (1, 2), and CDI has now surpassed methicillin-resistantStaphylococcus aureus
(MRSA) as the most common cause of health care-associated infection (2). Importantly,
uncontrolled CDI has significant morbidity and mortality, with the median risk ofⱖ1
recurrence being 22% (range, 12% to 64%). Other significant risks include having a complicated disease course (median, 15%; range, 7% to 48%), experiencing treatment failure (median, 21%; range, 5% to 50%), and death (median, 19%; range, 8% to 53%) according to a recent critical review (3).
One of the current, yet unproven, CDI prevention efforts suggests that admission
surveillance testing (AST) forC. difficilecolonization may be of value (4). There are no
Received28 September 2017Returned for modification24 November 2017 Accepted 17 January 2018
Accepted manuscript posted online24 January 2018
CitationPatel PA, Schora DM, Singh K, Peterson LR. 2018. Validation of active surveillance testing forClostridium difficile
colonization using the cobas Cdiff test. J Clin Microbiol 56:e01553-17.https://doi.org/10 .1128/JCM.01553-17.
EditorBetty A. Forbes, Virginia Commonwealth University Medical Center
Copyright© 2018 American Society for Microbiology.All Rights Reserved.
Address correspondence to Lance R. Peterson, [email protected].
crossm
on May 16, 2020 by guest
http://jcm.asm.org/
Food and Drug Administration (FDA)-approved commercial assays for this application although one report utilized an FDA-cleared real-time PCR test that demonstrated a
significant reduction in CDI when admission testing for toxigenic C. difficile was
deployed (5). The goal of our study was to validate the cobas Cdiff Test on the cobas 4800 System (cobas), an FDA-cleared diagnostic assay using real-time PCR technology
for detection of toxigenicC. difficile (toxin B gene) in stool samples (6), as a reliable
method for performing AST for toxigenicC. difficilecolonization. Our hypothesis was
that this test would be a useful assay for admission surveillance testing. A secondary goal was to evaluate the use of a second nucleic acid amplification test (NAAT) for discrepant analysis when there were discordant results between the assay under study
and direct (no broth enrichment) culture for toxigenic C. difficileby using a medical
record review to identify those patients receiving antimicrobials likely to interfere with
the growth ofC. difficile.
MATERIALS AND METHODS
Patient population and specimen collection.The NorthShore University HealthSystem includes four hospitals located in Evanston, Glenview, Highland Park, and Skokie, Illinois, with 908 inpatient beds and approximately 60,000 annual admissions. This study was conducted at Glenbrook Hospital and at the intensive care units (ICUs) at all four facilities during an infection control quality improvement interven-tion. Glenbrook Hospital was selected to perform a pilot of admission screening since it had the highest CDI rate at the time, and limited resources permitted the pilot program to be done at only one facility. Including the ICUs at all four hospitals provided samples from across our system. Patients were prospectively enrolled from July 2016 through August 2017. Perirectal (intra-anal) samples were collected from inpatients upon their admission using a premoistened, double-headed BBL culture swab with liquid Amies medium (Becton-Dickinson, Sparks, MD). All adult patients admitted to Glenbrook Hospital and to the intensive care units at all four facilities were eligible for inclusion. This study was done as an infection control quality improvement practice not subject to further Institutional Review Board (IRB) review, per IRB-approved policy.
Real-time PCR procedure.After receipt of the swab specimens, the cobas Cdiff Test was performed according to the manufacturer’s instructions. One swab was removed from the transport container and broken into cobas PCR medium, which was then briefly vortexed. The specimen was loaded directly on the automated cobas 4800 System for processing, PCR amplification, and detection (6). Positive and negative controls were included in each run as provided in the cobas kit.
Culture methods.The second swab was directly plated onto prereduced anaerobically sterilized (PRAS) selective medium composed of cycloserine-cefoxitin-fructose agar with horse blood and tauro-cholate (CCFA-HT; Anaerobe Systems, Morgan Hill, CA) forC. difficileculture whenever the cobas test was positive. Only direct plating was used due to resource limitations and the fact that we could compare these results to the FDA clearance trial results where direct plating was also utilized for a comparative measure. The first negative cobas sample from a new patient after each positive patient was also cultured in the same manner. Plates were incubated anaerobically for 5 days, and presumptiveC. difficilecolonies were confirmed by Gram stain, aerotolerance, and a Pro-disk (Hardy Diagnostics, Santa Maria, CA). To confirmC. difficilecolonies as toxigenic, strains were inoculated into anaerobic chopped-meat broth (Anaerobe Systems) that was incubated for 5 to 7 days at 35°C. Supernatant from the anaerobic chopped-meat broth was processed for detection ofC. difficiletoxin B using cell culture cytotoxicity testing according to the manufacturer’s instructions (C. difficileTox-B test; Techlab, Blacksburg, VA).
Discrepant analysis.Results that were discrepant between the cobas and the anaerobic culture were evaluated by testing of the remnant swab using the XpertC. difficile/Epi test (Xpert; Cepheid, Sunnyvale, CA). The samples that were also positive by the Xpert test were considered true-positive samples. We also reviewed the medical records of all patients with a positive cobas but negative culture results. The cobas result was considered a true positive if the patient was receiving oral vancomycin and/or oral metronidazole as therapy for confirmed CDI or intravenous piperacillin-tazobactam (7) and was Xpert positive. No other antimicrobial therapy (e.g., intravenous cefazolin, ceftriaxone, gentamicin, levofloxacin, metronidazole, vancomycin, and oral cephalexin or clindamycin) was considered to have a potential to interfere with a positive culture for toxigenicC. difficile. These data were compared to the results of the Xpert test in order to evaluate the use of this second NAAT as the discrepant reference method.
Statistical analysis.We selected a convenience set of samples to culture for toxigenicC. difficile, which consisted of all positive specimens plus the first negative swab from a new patient following each positive test, as opposed to culturing all negative samples, due to resource limitations. This restricted the data analysis for the cobas to the positive predictive value (PPV) and percent agreement of the tests. This selection of samples for inclusion on the basis of cobas results (a total of 273 positive and negative tests) influences the calculated sensitivity and specificity by artificially increasing the prevalence of positive results for that test in the population, and so a usual sensitivity and specificity analysis cannot be done in the strict sense. We had already documented the sensitivity and specificity of the cobas assay (6), which suggested that if the PPV and percent agreement are similar to earlier results, then the sensitivity and specificity are expected to be comparable. Since toxigenic culture is not a perfect reference standard, we also calculated the positive percent agreement (PPA), negative percent agreement (NPA), and overall
on May 16, 2020 by guest
http://jcm.asm.org/
agreement (OA) for these two testing approaches (8). For comparison of use of a medical record review to that of the Xpert test for discrepant analysis, a two-sided Fisher’s exact test was used.
RESULTS
The overall rate of cobas-positive tests in our investigation was 7.6%. A total of 273 samples had both real-time PCR (137 positive and 136 negative) and culture performed; one negative swab was not retained and could not be cultured. One real-time PCR
sample grew a nontoxigenic C. difficilestrain; all others were toxigenic. None of the
cobas-negative samples were culture positive. The overall performance of the cobas compared to that of culture is shown in Table 1. The performance of the test after discrepant analysis using the Xpert is shown in Table 2. As can be seen, in both analyses there were no swab samples that were cobas negative and culture positive, giving a positive percent agreement of 100%. There were a total of 27 false-positive tests out of 137 positive assays (19.7%). With a positive test rate of 7.6%, this translates to 1.5% of patients placed into isolation due to a false-positive assay, assuming all admissions are tested.
Table 3 provides data on the use of the Xpert test for the discrepancy analysis. The medical record review confirmed that this was a helpful assay to use for determination of true-positive tests from patients receiving antimicrobials expected to inhibit the
growth of C. difficilein anaerobic culture, with seven samples testing positive by
the Xpert. Only 4 of 23 Xpert-negative samples received these agents, indicating the reliability of this strategy as a tool for determination of true-positive results where an
initial NAAT is positive but culture for toxigenicC. difficileis negative (P⫽0.00006).
DISCUSSION
In this validation of the cobas for use in active surveillance testing on perirectal (intra-anal) swab specimens, we demonstrated that the test had performance similar to
that of the FDA-cleared test for detection of toxigenic C. difficileon unformed stool
samples. To our knowledge, this is the first report that analyzes the actual performance of a commercial NAAT for validation to use in an AST program, and the fact that it performed as expected is important. We also demonstrated that using a second NAAT from another manufacturer is a reasonable approach for discrepant analysis, based on medical record review for patients receiving antimicrobial therapy that would be
expected to inhibit the growth ofC. difficilein anaerobic culture. This finding is also
helpful for laboratories that plan to undertake a similar validation of a commercial
real-time PCR assay detecting C. difficile for use in an active surveillance testing
infection control program.
We expected that the cobas Cdiff Test would perform well since the published data
using this assay to detect toxigenicC. difficilefrom unformed stool demonstrated that
[image:3.585.42.371.83.116.2]it was robust (6). Also, the specimens collected for AST of patients potentially colonized
TABLE 1cobas CDiff Test compared to direct toxigenic culture
cobas test resulta Culture positive (no. of tests) Culture negative (no. of tests)
Positive 103 34
Negative 0 136
aPositive predictive value, 75.2% (95% CI, 66.9 – 82%); positive percent agreement, 100% (95% CI,
[image:3.585.41.372.679.711.2]96.0 –100%); negative percent agreement, 80% (95% CI, 73.4 – 85.3%); overall percent agreement, 87.6% (95% CI, 83.1–91.0%).
TABLE 2cobas Cdiff Test compared to direct toxigenic culture after discrepancy analysis using the XpertC. difficile/Epi test
cobas test resulta True positive (no. of tests) True negative (no. of tests)
Positive 110 27
Negative 0 136
aPositive predictive value, 80.3% (95% CI, 72.4 – 86.4%); positive percent agreement, 100% (95% CI,
95.8 –100%); negative percent agreement, 83.4% (95% CI, 77.0 – 88.4%); overall percent agreement⫽90.1% (95% CI, 86.0 –93.1%).
on May 16, 2020 by guest
http://jcm.asm.org/
with toxigenicC. difficileare very similar to those used in the FDA-cleared diagnostic test. Specifically, the cobas Cdiff Test uses a swab to transfer sample from the collection container to the test system rather than another device, such as an inoculating loop (9). Inserting a swab into the anus is, in a sense, similar to inserting it into a cup containing stool. The internal anal sphincter is involuntary while the external is voluntary (10). Thus, it is typical for some stool and/or mucus from the gastrointestinal tract to be retained in the anus, and sampling this material should provide results for AST of
patients colonized with toxigenicC. difficile similar to those of a diagnostic test that
incorporates a swab sampling of stool as part of the assay procedure. Finally, perirectal
and rectal swabs have been shown to have the same recovery rates ofC. difficilewhen
cultured on prereduced cycloserine-cefoxitin-brucella agar containing 0.1% taurocholic acid and lysozyme at 5 mg/ml (11), suggesting that sampling may not be critical as long as the swab enters the anus.
We performed a literature review using PubMed.gov (Medline) with the search terms
Clostridium difficilesurveillance, active surveillance testing, real-time PCR, and the names of
FDA-cleared molecular tests that detectC. difficileto search the medical literature from 2005
through August 2017. We also searched Google using these terms as well as the term anus. In the recent literature there have been two reports suggesting that admission
surveil-lance for toxigenicC. difficilemay be useful and that colonized persons are a significant
component of transmission within the hospital (12, 13). Mawer and colleagues found
that patients with stool harboring a toxigenicC. difficilestrain where the actual stool
toxin test was negative appeared responsible for 25% of transmission events to others when such transmission could be ascertained (12). Furthermore, they suggested that since no source for most symptomatic CDI was detected, isolation of asymptomatically colonized patients, who are severalfold more numerous than disease patients, may result in a larger reduction in transmission and presumably less disease (12). Caroff and coworkers also reported that most cases of hospital-onset CDI do not have a genetic
link to another patient strain and that clinical disease may be due to activation ofC.
difficilepresent on admission or to new transmissions from asymptomatic patients, thus leading to recommendations for new control measures, including admission screening (13). Admission surveillance testing is also suggested as a possible, but yet unproven, intervention for lowering the risk of hospital-onset CDI in the current UpToDate document on prevention and control of this disease (4).
Longtin and colleagues reported the impact ofC. difficileadmission testing, using a
commercial NAAT, on the rate of CDI in their facility (5). They found a disease reduction
of more than 50% when cases of CDI significantly decreased (P⬍0.001) from 0.69 per
1,000 patient days before the intervention to 0.3 cases per 1,000 patient days after screening was implemented (5). However, there was no information provided on the analytical performance of the real-time PCR assay they used when applied to rectal surveillance swabs. Terveer et al. also examined the suitability of PCR to detect asymptomatic colonization (14). In this study, swabs inserted into the stool were tested using a real-time PCR test as well as by an enzyme-linked fluorescent assay (ELFA) detecting glutamate dehydrogenase (14). As expected, the real-time PCR test outper-formed the ELFA, with the sensitivity and specificity of the real-time PCR being 96% and 93%, respectively, while the ELFA had a sensitivity and specificity of 87% and 91% (14).
[image:4.585.39.372.94.152.2]The only other study involving the use of perirectal swabs forC. difficilesurveillance was
TABLE 3Evaluation of the XpertC. difficile/Epi test as a tool for discrepant analysis compared to antibiotic receipt active againstC. difficilein stool
Treatment
Xpert result with cobas-positive test (no. of tests)a
Significance Positive Negative
Inhibitory antibiotics 7 4 P⫽0.00006 No inhibitory antibiotics 0 23
aTotal number of tests, 34.
on May 16, 2020 by guest
http://jcm.asm.org/
that by Curry and coworkers and involved preenrichment of swabs in selective broth, followed by testing using a modified commercial real-time PCR assay (15). The main limitation of this method was the need for preamplification in broth that reduces the rapidity of result reporting.
The cost-effectiveness of admission surveillance testing has also been evaluated. The investigators modeled the cost-effectiveness for admission screening of all patients and found a cost savings for every level of contact precaution compliance when the
prevalence of C. difficilecolonization exceeded 5% (16), with our testing rate being
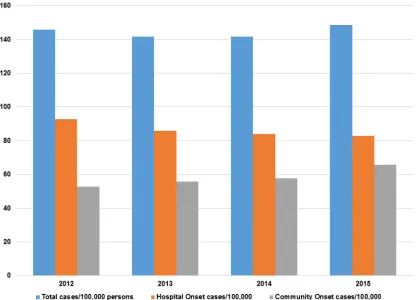
7.6%. They used a cost of surveillance testing up to $15.88 (15); but if one were able to perform targeted surveillance and have the same benefit for disease reduction, then the overall cost of testing could be lower, depending on the percentage of patients being screened. One important incentive to control the rate of CDI in U.S. hospitals is the Centers for Medicare and Medicaid Services (CMS) classification of CDI as a hospital-acquired condition (HAC), with potential for fines if rates are too high (17). Each year the HAC reduction program saves CMS $350 million by reducing payments to hospitals, thus incentivizing U.S. health care facilities to reduce these hospital-acquired infections (17). Combining the impact of this CMS program with surveillance data from the Centers for Disease Control and Prevention (CDC) demonstrating a rise in annual total CDI cases (Fig. 1) since 2013 (18), it is not surprising that hospitals are looking at novel interventions to lower CDI rates.
There are several limitations to our investigation. The primary one is that, because of limited financial resources, we did not culture all samples, which limited the culture
detection of toxigenicC. difficileto samples that were positive using the cobas as well
as the next following patient with a negative stool sample. This affected calculation of an actual sensitivity and specificity of the test based on the entire population tested. However, it is possible to estimate the sensitivity, specificity, and negative predictive value (NPV) from our data. Since the cobas Cdiff Test assay positive rate was 7.6%, this
FIG 1Annual incidence (cases per 100,000 persons) of CDI based on CDC surveillance data (18).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:5.585.42.458.72.372.2]indicates that the entire population was 1,803 patients. We also know that the total number of false-positive tests (before any discrepancy analysis) was 34. Since the test sensitivity in our sample was 100% (95% confidence interval [CI], 95.5 to 100%), then the greatest number of false-negative tests could be 5. Using these numbers, the estimate for sensitivity was 95.4 to 100% (95% CI, 89.0 to 100%), specificity was 98.0% (95% CI, 97.2 to 98.6%), and NPV was 99.7 to 100% (95% CI, 99.3 to 100%). These results are not different from those found for the cobas FDA-cleared test compared to direct culture (6), with a sensitivity of 97.3% (95% CI, 91.9 to 99.3%), specificity of 94.9% (95% CI, 92.7 to 96.5%), and NPV of 99.4% (95% CI, 98.3 to 99.9%). We were able to calculate the actual PPV and the positive percent agreement (PPA), which were comparable to the performance of this test on stool samples (6). The PPV on the FDA-cleared cobas Cdiff Test assay was 79.1% (95% CI, 71.3 to 85.4%) compared to our surveillance testing results of 75.2% (95% CI, 66.9% to 82%); and a comparison of the PPA values resulted in 97.3% (95% CI, 92.5% to 99.1%) versus 100% (95% CI, 96.0% to 100%). None of these
differences were statistically significant (P⬎0.1), and these are excellent results for a
surveillance test where detecting likely carriers of a potential pathogen is the goal. If
one develops a targeted admission surveillance program based on risk factors for C.
difficilecolonization, which we have done for our system-wide surveillance implemen-tation, one will likely test 1/3 of admissions (our practice), which leads to one unnec-essarily isolated patient per 200 admissions, which we consider a minimal number of false positives that is acceptable. Thus, we are confident that the test performed well on our surveillance swab samples. These results are consistent with the most recent CDI quality assessment review indicating that NAAT has the highest clinical diagnostic
sensitivity and provides the greatest confidence for absence of disease fromC. difficile
(19). We also did not perform any culture enrichment to detect samples with low numbers of colonies. In place of this, we tested discrepant samples using a second NAAT (Xpert), and when the results were compared to medical record review, there was an excellent correlation between a positive second NAAT and patients receiving
antimicrobial therapy that would be expected to inhibit the growth ofC. difficilein
anaerobic culture. The Xpert test would not be expected to detect low-colony-count positives that may be detected by enrichment culture that could increase direct culture-based sensitivity by at least 13% (20), but it was helpful in detecting patients
receiving antibiotics that inhibitC. difficilegrowth; and we believe that the majority of
true-positive tests were accurately identified.
Useful future research would be to validate additional NAAT assays that could be
deployed in AST for toxigenicC. difficile. Should AST become a recommended tool to
control the spread of CDI, it would be helpful for commercial vendors supplying these tests to perform needed studies that would permit an FDA claim for use of swab testing in facilities that do not have the capability to perform an in-house validation for this application.
In conclusion, we have demonstrated that the cobas is a reliable assay for detection
of toxigenicC. difficilein perirectal samples from asymptomatic patients undergoing
active surveillance testing as part of a hospital infection control program. We also
demonstrated that the Xpert assay confirmed (P⫽0.00006) the presence ofC. difficile
among patients who had received antibiotics that would have potentially interfered with organism viability in culture.
ACKNOWLEDGMENTS
We sincerely appreciate the contributions of the faculty and staff of NorthShore University Health System for diligently collecting samples to improve patient safety. We also thank Oliver Liesenfeld, Chief Medical Officer, Medical and Scientific Affairs, Roche Molecular Diagnostics, Pleasanton, CA, for his assistance with study concept and design, critical revision of the manuscript for important intellectual content, and material support.
This investigator-initiated work was supported by NorthShore University
on May 16, 2020 by guest
http://jcm.asm.org/
System, and partially by Roche Molecular Diagnostics, Pleasanton, CA, who provided the real-time PCR testing materials at no cost.
L.R.P. has received speaking honoraria from Becton Dickinson, Cepheid, Roche, and CareFusion. L.R.P. has received research funding from Becton Dickinson, Cepheid, Nanosphere, 3M, GeneWEAVE, and Roche. K.S. has received research funding from Becton Dickinson and Roche.
P.A.P., L.R.P., and K.S. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. L.R.P. and D.M.S. were responsible for the study concept and design. P.A.P., L.R.P., D.M.S., and K.S. were responsible for data acquisition, analysis, and interpretation. P.A.P. and L.R.P. drafted the manuscript. P.A.P., L.R.P., D.M.S., and K.S. were responsible for critical revision of the manuscript for important intellectual content. L.R.P. performed statistical analysis. L.R.P. and K.S. provided administrative, technical, or material support. L.R.P., P.A.P., D.M.S., and K.S supervised the study.
REFERENCES
1. Centers for Disease Control and Prevention. 2013. Annual report for the Emerging Infections Program forClostridium difficileinfection. Centers for Disease Control and Prevention, Atlanta, GA.https://www.cdc.gov/ hai/eip/pdf/cdiff/2013-annual-report.pdf.
2. Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC. 2015. Burden of
Clostridium difficileinfection in the United States. N Engl J Med 372: 825– 834.https://doi.org/10.1056/NEJMoa1408913.
3. Abou Chakra CN, Pepin J, Sirad S, Valiquette L. 2014. Risk factors for recurrence, complications and mortality inClostridium difficileinfection: a systematic review. PLoS One 9:e98400.https://doi.org/10.1371/journal .pone.0098400.
4. McDonald LC, Kutty PK. 2017.Clostridium difficileinfection: preven-tion and control. UpToDate topic 2687. Wolters Kluwer, Philadelphia, PA. https://www.uptodate.com/contents/clostridium-difficile-infection -prevention-and-control.
5. Longtin Y, Paquet-Bolduc B, Gilca R, Garenc C, Fortin E, Longtin J, Trottier S, Gervais P, Roussy JF, Lévesque S, Ben-David D, Cloutier I, Loo VG. 2016. Effect of detecting and IsolatingClostridium difficilecarriers at hospital admission on the incidence ofC. difficileinfections: a quasi-experimental controlled study. JAMA Intern Med 176:796 – 804.https://doi.org/10 .1001/jamainternmed.2016.0177.
6. Peterson LR, Young SA, Davis TE, Jr, Wang Z-X, Duncan J, Noutsios C, Liesenfeld O, Osiecki JC, Lewinski MA. 2017. Evaluation of the cobas Cdiff test for the detection of toxigenicClostridium difficilein stool samples. J Clin Microbiol 55:3426 –3436.https://doi.org/10.1128/JCM.01135-17. 7. Kundrapu S, Sunkesula VC, Jury LA, Cadnum JL, Nerandzic MM, Musuuza
JS, Sethi AK, Donskey CJ. 2016. Do piperacillin/tazobactam and other antibiotics with inhibitory activity againstClostridium difficilereduce the risk for acquisition forC. difficilecolonization? BMC Infect Dis 16:159. https://doi.org/10.1186/s12879-016-1514-2.
8. Obermeier P, Muehlhans S, Hoppe C, Karsch K, Tief F, Seeber L, Chen X, Conrad T, Boettcher S, Diedrich S, Rath B. 2016. Enabling precision medicine with digital case classification at the point-of-care. EBioMedi-cine 4:191–196.https://doi.org/10.1016/j.ebiom.2016.01.008.
9. U.S. Food and Drug Administration. 2014. 510(k) Substantial equivalence determination decision summary, K142422. U.S. Food and Drug Admin-istration, Silver Spring, MD.https://www.accessdata.fda.gov/cdrh_docs/ reviews/K142422.pdf.
10. Cleveland Clinic. 2013. The structure and function of the digestive system. Cleveland Clinic, Cleveland, OH.https://my.clevelandclinic.org/ health/articles/the-structure-and-function-of-the-digestive-system.
11. Rogers DS, Kundrapu S, Sunkesula VC, Donskey CJ. 2013. Comparison of perirectal versus rectal swabs for detection of asymptomatic carriers of toxigenicClostridium difficile. J Clin Microbiol 51:3421–3422.https://doi .org/10.1128/JCM.01418-13.
12. Mawer DPC, Eyre DW, Griffiths D, Fawley WN, Martin JSH, Quan TP, Peto TEA, Crook DW, Walker AS, Wilcox MH. 2017. Contribution toClostridium difficiletransmission of symptomatic patients with toxigenic strains who are fecal toxin negative. Clin Infect Dis 64:1163–1170.https://doi.org/10 .1093/cid/cix079.
13. Caroff DA, Yokoe DS, Klompas M. 17 May 2017. Evolving insights into the epidemiology and control ofClostridium difficilein hospitals. Clin Infect Dishttps://doi.org/10.1093/cid/cix456.
14. Terveer EM, Crobach MJ, Sanders IM, Vos MC, Verduin CM, Kuijper EJ. 2017. Detection ofClostridium difficilein feces of asymptomatic patients admitted to the hospital. J Clin Microbiol 55:403– 411.https://doi.org/ 10.1128/JCM.01858-16.
15. Curry SR, Schlackman JL, Hamilton TM, Henderson TK, Brown NT, Marsh JW, Shutt KA, Brooks MM, Pasculle AW, Muto CA, Harrison LH. 2011. Perirectal swab surveillance forClostridium difficileby use of selective broth preamplification and real-time PCR detection oftcdB. J Clin Mi-crobiol 49:3788 –3793.https://doi.org/10.1128/JCM.00679-11. 16. Bartsch SM, Curry SR, Harrison LH, Lee BY. 2012. The potential economic
value of screening hospital admissions forClostridium difficile. Eur J Clin Microbiol Infect Dis 31:3163–3171.https://doi.org/10.1007/s10096-012 -1681-z.
17. U.S. Centers for Medicare and Medicaid Services. 2015. Hospital-acquired conditions. U.S. Centers for Medicare and Medicaid Services, Baltimore, MD. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment -Instruments/Value-Based-Programs/HAC/Hospital-Acquired-Conditions .html.
18. Centers for Disease Control and Prevention. 2015.Clostridium difficile
infection (CDI) tracking. Centers for Disease Control and Prevention, Atlanta, GA.https://www.cdc.gov/hai/eip/clostridium-difficile.html. 19. Butler M, Olson A, Drekonja D, Shaukat A, Schwehr N, Shippee N, Wilt TJ.
2016. Early diagnosis, prevention, and treatment ofClostridium difficile: update. AHRQ publication no. 16-EHC012-EF. Agency for Healthcare Research and Quality. Rockville, MD.www.effectivehealthcare.ahrq.gov/ reports/final.cfm.
20. Peterson LR, Mehta MS, Patel PA, Hacek DM, Harazin M, Nagwekar PP, Thomson RB, Jr, Robicsek A. 2011. Laboratory testing forClostridium difficileinfection: light at the end of the tunnel. Am J Clin Pathol 136:372–380.https://doi.org/10.1309/AJCPTP5XKRSNXVIL.