121904-4848-IJBAS-IJENS © August 2012 IJENS I J E N S
Abstract-- Chromium is one of the essential nutrients whose
metabolism changes in diabetes. It has been shown that there is a relationship between serum chromium and both kinds of diabetes [non-dependent diabetes mellitus (NIDDM) and insulin-dependent diabetes mellitus (IDDM)]. The aim of the present study is to investigate the serum chromium (Cr) status (In Type-1 DM patients, Type-2 patients, and insulin resistance. The study was conducted on 50 type-1 DM subjects, 50 type-2 DM subjects, 50 patients with Insulin resistance and 50 control subjects. Glucose, HbA1c and Cr were analyzed in fasting serum of all subjects. Serum chromium (Cr) levels were decreased in all three patients groups, respectively Type-1 DM, Type-2 DM and insulin resistance group (p<0.05, p=0,001, p<0,001). There were strong negative correlation between serum Cr and HbA1C levels respectively ( Type-1 DM patients, Type-2 DM patients, insulin resistance) (r =-0 .67, p <0.05) (r= -0.75, p<0,05) (r= -0.64, p<0,05).
Index Term-- Serum Chromium, Type-1 and 2 DM, Insulin resistance.
INTRODUCTION
Chromium is an essential micronutrient which is required for normal insulin effect and regulation of blood sugar level. Serum chromium status of patients with type-2 diabetes is compared with control non-diabetic subjects [1]. The trace
Hamid Ghaffoori Hasan
Department of Chemistry /Ibn Al‐Haitham College, Baghdad
University, Baghdad‐IRAQ.
Parween A. Ismael
Department of Chemistry /College of Education Science,
University of Salahaddin, Erbil‐IRAQ.
Nazk Mohammed Aziz
Department of Chemistry, School of Science, Faculty of
Science and Science Education, University of Sulaimani, Sulaimani‐Iraq.
element, chromium increases insulin binding to cells by increasing insulin receptor numbers. It may lead to increased insulin sensitivity, glucose utilization and beta-cell sensitivity. Chromium as part of a compound known ‘glucose tolerance factor’ (GTF) is needed for appropriate metabolism, and insulin receptor glucose use, Lipid sensitivity [2]. Micronutrients have been investigated as potential preventive and therapeutic agents for type-2 diabetes and for common complications of diabetes. In particular, diabetes has been shown to be associated with abnormalities in the metabolism of zinc, chromium, copper, magnesium and manganese. Diabetes mellitus is a very common metabolic disorder with the potential to cause devastating chronic complications. Type-2 DM shows identical pathophysiological features with Type-1 DM but differs in etiology [3]. Though, the nature of both disease complications are generally the same, duration and appearance time are different from each other. Chromium possibly influences glucose metabolism by helping in the binding of insulin to its receptors and potentiating its action. Insulin resistance, which is central to the pathogenesis of type-2 diabetes mellitus [4], may be a consequence of chromium deficiency. Attempts have been made to identify chromium deficiency in diabetes and to supplement dietary chromium to ameliorate symptoms in diabetics [5]. The search for Cr-containing biologically active substances, since 1950, has identified several products which have all been termed GTF, composed of chromic ion, nicotinic acid and amino acids glycine, glutamic acid and cysteine [6]. This agent, which potentiates the action of insulin, had been isolated initially from brewer’s yeast and kidney powder. It is an organic, low molecular weight complex containing trivalent chromium a naturally occurring oligopeptide, low molecular-weight Cr-binding substance, LMW Cr [7,8], which is widely distributed in liver, kidney, spleen, intestines, testicles and brain and binds four equivalents of Cr in a multicentric assembly, has been proposed. It comprises amino acids glycine, cysteine, glutamic acid and aspartic acid. The chromic centers are bridged by anionic ligands and are supported by carboxylate group from aspartate and glutamate residues [9,10]. This LMW Cr has been postulated to be a part of an insulin signal amplification mechanism [11] in which its apo-form, present in cells, is
Evaluation of Serum Chromium Levels in
Patients with Type1 and 2 Diabetes Mellitus and
insulin resistance
121904-4848-IJBAS-IJENS © August 2012 IJENS I J E N S activated by binding Cr ions and mobilizing them into the
cells. This binding results in stabilization of the active conformation of insulin receptor tyrosine kinase. Reduced
insulin efficiency or insulin resistance may precede the development of diabetes by many years and is the time frame where nutritional intervention to prevent the onset of type-2 DM is likely to have the most significant effects. The first detectable sign of insulin resistance is a rise in circulating insulin concentrations. As insulin resistance increases, the body compensates for this inefficiency of insulin function by progressive increases in insulin production and release by the pancreas. This is followed by rises in blood glucose [12]. There have been more than seventeen studies involving Cr supplementation of subjects with diabetes. The overwhelming majority of these reports involved subjects with type-2 DM but there are a bit less studies involving Cr and type-1 DM. Chromium absorption of people with insulin dependent or type-1DM is approximately double that of control or subjects with type-2 DM. Urinary Cr excretion of subjects with type-1 DM is also more than twice that of control subjects. People with type-1 diabetes also have lower hair and tissue Cr. It appears that the metabolic control mechanisms of people with type-1 DM they are in need for additional Cr, which is reflected by increased absorption, but this absorbed Cr does not appear to be utilized and is excreted in the urine [13, 14].
MATERIALS AND METHODS
Selection of Subjects:
Study groups evaluated as group1 Type 1 DM patients (50 samples), group 2 Type 2 DM (50 samples), group 3 Insulin resistance patients (50 samples), and group 4 healthy persons (50 samples).
Collection of Blood Samples
Ten ml blood samples were collected. In order to obtain plasma and to avoid clotting, 2 cc of blood samples were put in a tube containing EDTA 5% (0.3 ml). The blood was centrifuged at 1500 g for 10 minutes, and plasma was separated, then red blood cells were washed with normal saline three times to take hemolization to measure HbA1c.. We put the rest blood samples (8 cc) in another tube without anticoagulant. Firstly, the tube was placed in laboratory temperature for 0.5 h and then was centrifuged at 1500 g for 10 minutes to separate serum.
Assay Methods
Serum glucose was measured by using enzymatic method (Zistshimi kit. Tehran, Iran). Colorimetric assay was used (M. Parker method) to determine HbA1c. For chromium determination serum samples was diluted at ratio 1 to 4 in 0.1 % (v/v) triton-x 100 + 0.01 mol/l nitric acid and was prepared for atomic absorption spectrometric analysis. All chemical reagents were of analytical grade purchased from Merck and Sigma agents, in Iran. The chromium stock solution (1000 mg/l Cr) was prepared from titrisol concentrates. Chromium
standard solutions for preparing the calibration curve (2, 5, 10, 15 mg/l Cr) were freshly prepared by serial dilution of the stock solution with 0.01 mol/l nitric acid. A graphite furnace atomizer (Shimadzu GFA-AA) was set on an atomic absorption spectrometer (Shimadzu 670G). Samples were introduced by auto sampler (Shimadzu model ASC 60G). The light source was a 5mA Chromium hollow cathode lamp, wavelength of 357.9nm and 0.5nm spectral slit width was used to check the samples .After obtaining calibration curve, 10μl aliquots of diluted serum sample (or aqueous Cr standards) were injected into graphite tube, the absorbance was recorded and the chromium concentration was determined.
RESULTS
Table (1), documents the results of mean serum levels of glucose, HbA1c , and Cr in diabetics(In Type 1 DM patients ,Type 2 patients ,Insulin resistance )and controls. In diabetics, significantly elevated (P<0.001) serum levels of glucose and HbA1c, were noticed as compared to healthy age matched controls.
TABLE I
Mean Serum Levels of Glucose, % HbA1C and Cr in Diabetics and Control Subjects.
Group 4 Insuli
n resista
nce (n=50
) Group3 Type II DM (n=50) Group2
Type I DM (n=50) Group1
Healthy Subjects (n=50) Parameters
0.037 8±0.0 24 0.0378±
0.024 0.0578±0.01
1 0.50±0.1
Cr (Mg/L)
188 189
176 88
Glucose|(m g/DL)
8.61± 0.24 9.59±0.
11 7.23±0.12
4.99±0.16 % HbA1C
p<0,0 01 p=0,001 p <0.001
<0.05 P-value
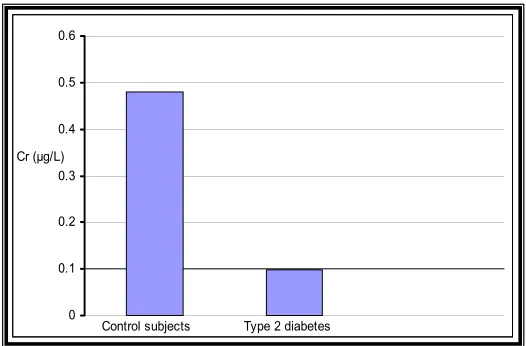
Diabetic subjects had significantly (p<0.001) lower serum concentrations of Cr as compared
With the control. Same decreases were found in Cr concentration in insulin resistance serum patirnt compared with control. The decreases were found to be significant (p=0,001). Figures (1, 2, 3)
121904-4848-IJBAS-IJENS © August 2012 IJENS I J E N S
0 0.1 0.2 0.3 0.4 0.5 0.6
Control subjects Type 1 diabetes
Cr (μg/L)
0 0.1 0.2 0.3 0.4 0.5 0.6
Control subjects Type 2 diabetes
Cr (μg/L)
0 0.1 0.2 0.3 0.4 0.5 0.6
Control subjects Insulin resistance Cr (μg/L)
y = -28.404x + 8.6431
0 2 4 6 8 10 12
0 0.02 0.04 0.06 0.08 0.1
r=-0.671
Cr (μg/L)
HbA1c
y = -14.441x + 8.6659
0 2 4 6 8 10 12
0 0.05 0.1 0.15 0.2
r=-0.75
HbA1c Cr (μg/L)
y = -12.634x + 8.5099
0 2 4 6 8 10 12
0 0.05 0.1 0.15 0.2 0.25
r=0-64
HbA1c Cr (μg/L)
Fig. 1. Serum chromium level in control and Type I DM groups.
Fig. 2. Cr concentrations in sera of control and Type-2 DM.
Fig. 3. Serum chromium level in control and Insulin resistance groups.
Type 1 DM, Type 2 DM and Insulin resistance patients
(r = -0.670, r=-0.75 ,r=-0.644) respectively. Correlation
curves of chromium with HbA1c are shown in (Figures 4,5,6).
Serum chromium concentration correlated inversely with HbA
1c
, and a significant negative correlation (p<0.05) was observed in between serum chromium III and HbA1cFig -4: correlation between serum chromium levels and HbA1c in Type I DM patients
Fig. 5. Correlation between serum chromium levels and HbA1c in Type II
IDM patients.
Fig. 6. Correlation between serum chromium levels and HbA1c in Insulin resistance patients
DISCUSSIONS
121904-4848-IJBAS-IJENS © August 2012 IJENS I J E N S the progression of diabetes. Chromium is a cofactor in the
action of insulin and it potentiates the action of insulin. As such it may improve blood glucose levels in individuals with a tendency towards blood glucose fluctuations associated with diabetes (hyperglycaemia). Thus, it may not be surprising to find an inverse relationship between serum chromium levels and blood glucose control.(15,16). In the present study, lower serum levels of chromium were observed in the diabetics compared to the non-diabetic population of the study. This agrees with the works of Ekmecioglu and Anderson (2007)(17) who also demonstrated lower levels of these elements only in the lymphocytes of diabetics and no differences in their levels in other blood components of both groups. However, significantly lower levels Cr were reported in serum and hair of diabetics by Nouramonammadi and Underwood (2007) (18). Hyperglycaemia and high levels of insulin increase chromium excretion (Watts, 1999), so low serum levels of chromium seen in the diabetics has been attributed to insulin resistance, hyperglycaemia and osmotic diuresis resulting from glycosuria, which increase urine chromium excretion. Hyperinsulinemia and insulin resistance may be correlated with a decrease in insulin receptors, reduced insulin binding, or post-insulin- receptor signaling defects. Insulin resistance is thought to be the initial cause in people with type 2 diabetes. Patients with type 2 diabetes and insulin resistance demonstrate a diminished sensitivity of target tissue (primarily the liver and skeletal muscle) to the action of insulin and a relative deficiency of endogenous insulin secretion. Impaired insulin secretion and increased glucagons contribute to continued hepatic glucose output resulting in elevated fasting glucose levels [19]. Some patients may have elevated blood glucose because of excessive glucagon or abnormal and excessive hepatic glucose production. Others may have a defect in somatostatin, an excess of growth hormone, cortisol, epinephrine, or other hormone that affects blood glucose regulation. Cushing’s syndrome, pheochromocytoma, aldosteronism, hyperthyroidism, pancreatitis, cirrhosis, pregnancy, emotional stress, and myocardial infarctions are other factors that may cause an increased in blood glucose. It appears that the etiology is probably multifactorial. It has been shown that trace elements may regulate hormone secretion and its function[20]. Among trace elements, chromium deficiency was first identified as a cause of impaired glucose tolerance in 1959. Chromium as part of a compound known ‘glucose tolerance factor’ (GTF) is needed for appropriate glucose use, Lipid metabolism, and insulin receptor sensitivity [21]. One study has been reported that administration of 500mg chromium two times per day for 2 months resulted in a significant improvement of glycosylated hemoglobin (HbAlc) values, and indication of how well glucose is metabolized.This study investigated the possible relationships between serum chromium concentration and blood sugar (glucose and HbA1c) in in Type 1 DM, Type 2 DM and Insulin resistance patients. Several studies have shown that there is a negative relationship between serum chromium concentration and serum glucose
levels. In these studies chromium deficiency elevated glucose concentration and chromium supplement decreased it. Chromium plays an important role in insulin synthesis and function, insulin connection to the cells, and glucose entrance to the cells. Also, chromium is a main cofactor in some glucose metabolism enzymes and as a result, its deficiency can disrupt carbohydrates metabolism (21, 22). Chromium deficiency can complicate glucose transportation into the cells, by disrupting lipid metabolism and membrane flexibility (23). Some studies have demonstrated that Zn supplement reduces lipid peroxidation and oxidative stress in diabetic patients, although it does not significantly change glucose levels, Cr is powerful antioxidants and its deficiency increases oxidative damages to various organs; nevertheless, hyperglycemia may elevate lipid peroxidation and oxidative stress in diabetic patients that could lead to cardiovascular complications in these patients (24, 25). Therefore, Cr has a possible role in improving diabetic patients through reducing glucose levels and oxidative stress.
CONCLUSIONS
Chromium is an essential micronutrient which is required for normal insulin effect and regulation of blood sugar level. Chromium is a cofactor in the action of insulin and it potentiates the action of insulin. Thus, it may not be surprising to find an inverse relationship between serum chromium levels and blood glucose control
REFERENCES
[1]Sun Y, Ramirez J, Woski SA & Vincent JB (2000) The binding of trivalent chromium to low-molecular-weight chromium-binding substance (LMWCr) and the transfer of chromium from transferring and chromium picolinate to LMWCr. Journal of Biological Inorganic Chemistry 5, 129–136.
[2]Tuman RW & Doisy RJ (2007) Metabolic effects of the glucose tolerance factor (GTF) in normal and genetically diabetic mice. Diabetes 26, 820– 826.
[3]Vincent JB (2000) The biochemistry of chromium. Journal of Nutrition 130, 715–718
[4]Mooradian AD, Failla M, Hoogwerf B, Marynuik M, Wylie-Rosett J. (2009) Selected vitamins and minerals in diabetes. Diabetes Care; 17: 464–79.
[5]Retnam VJ, Bhandarkar SD. (2008) Trace elements in diabetes mellitus. J Postgrad Med; 27: 129–32.
[6]Walter RM, Uriu-Hare JY, Olin KL, et al. (2005) Chromiumr, zinc, manganese and magnesium status and complication of diabetes mellitus. Diabetes Care; 14: 1050–6.
[7]El-Yazigi A, Hannan N, Raines DA. (2008) Urinary excretion of chro-mium, copper and manganese in diabetes mellitus and associated disorders. Diabetes Res; 18: 129–34.
[8]Zargar AH, Shah NA, Massodi SR. (2007) Chromiumr ,Copper, zinc, and magnesium levels in non-insulin-dependent diabetes mellitus. Postgrad Med J; 74: 665–
[9] Anderson RA (2008). Chromium, glucose intolerance and diabetes. J Am Coll Nutr; 17: 548-555.
[10] Chausmer AB. Zinc, insulin, and diabetes. J Am Coll Nutr (2008); 17: 109–15.
[11] Mosaad A, Abou-Seif G., Abd-Allah Y. (2004).Evaluation of some biochemical changes, in diabetic patients.
[12] Clinica Chimica Acta; 346: 161–70. 12- Anderson RA, Cheng N,
121904-4848-IJBAS-IJENS © August 2012 IJENS I J E N S improve glucose and insulin variables with type 2 diabetes. Diabetes;
46: 1786–91.
[13] Nsonwu AC, UsoroCAO, Etukudo MH, Usoro IN. (2006). Glycemic control and serum and urine levels of chromium and magnesium in diabetics in Calabar, Nigeria. Pakistan J Nutrit; 5: 75–8.
[14] Chalmers KH (2005). Medical nutrition therapy. In Joslin’s Diabetes mellitus, 14th edition. Eds Kahn CR et al. Philadelphia: Lippincott Williams and Wilkins: pp 611–29.
[15] Muula A. (2000).Preventing diabetes associated morbidity and mortality in resource poor communities. Diabetes Int; 10: 47–8. [16] Kimura K. (2009).Role of essential trace elements in the disturbance
of carbohydrate metabolism. Nippon Rinsho; 54: 79–84.
[17] Ekmecioglu G.and Anderson RA. (2007). Chromium. Status in
diabetes mellitus. Nutritional factors influencing the glucose/insulin system: Chromium. J Am Coll Nutr; 16: 404–10.
[18] Nouramonammadi and Underwood EJ. (2007)Trace Elements in in diabetes Human and Animal Nutrition, 4th edition. New York: Academic press; pp 258–70.
[19] Mertz W. (2007). Clinical and public health significance of chromium. In Clinical, Biochemical, and Nurtritional Aspects of Trace Elements. Ed Prasad AS. New York: Alan R Liss, Inc. : pp 315–23.
[20] Retnam VJ, Bhandarkar SD (2008).Trace elements in diabetes mellitus. J Postgrad Med; 27: 129–32
[21] Eisenbarth, G.S (2009). Type I diabetes mellitus: A Chronic auto immune disease. New England J. Medicine, 314, 1368.
[22] Jeejeebttoy, K.N., et al.(2008). Chromium deficiency, glucose intolerance, and neuropathy reversed by chromium supplementation, in a patients receiving long-term total parental nutrition, Am. J. Clin. Nut., 30, 531
[23] Balk E. M., Tatsioni A., Lichtenstein A. H., Lau J., Pittas A. G.(2009). Effect of Chromium Supplementation on Glucose Metabolism and Lipids: A systematic review
[24] of randomized controlled trials. Diabetes Care, 30, 2154. Hellerstein MK (2009). Is chromium supplementation effective in managing type II diabetes? Nut. Rev., 56, 302.