ARTICLE
Optimal Intramuscular Needle-Penetration Depth
William C. Lippert, BAa, Eric J. Wall, MDb
aSchool of Public Health and Tropical Medicine, Tulane University, New Orleans, Louisiana;bDivision of Orthopaedic Surgery, Cincinnati Children’s Hospital Medical
Center, Cincinnati, Ohio
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
During vaccine administration, overpenetration of the intramuscular layer causing the needle to strike the bone often has been overlooked. Authors who have focused on overpenetration have deemed it better than underpenetration.
What This Study Adds
The CDC guidelines for vaccine needle lengths should be revised. We found a significant risk for overpenetration by using the guidelines. A universal needle length according to certain age, weight, or gender groups is unacceptable because of the tremendous vari-ability present.
ABSTRACT
OBJECTIVE.The US Centers for Disease Control and Prevention has needle-length rec-ommendations for intramuscular vaccinations in the thigh and shoulder on the basis of the age of the child. Underpenetration of the intramuscular layer with short needles has been documented; however, few studies have focused on the risk for overpenetration of the intramuscular level with needles that are too long. The purpose of this study was to determine the optimal needle length for intramuscular vaccination of children of various ages and sizes at the shoulder and thigh levels by using MRI and computed tomography scan measurements.
METHODS.A total of 250 MRI and computed tomography scans of shoulders and thighs of children who were 2 months to 18 years of age at a large children’s hospital were reviewed. The thicknesses of the subcutaneous fat tissue and muscle layers were measured. Measurements were correlated with age and weight, and regression analysis was performed.
RESULTS.Use of the Centers for Disease Control and Prevention’s recommended 1- and 11⁄4-in needles for intramuscular vaccination in the thigh of childrenⱖ1 year of age
would result in 11% (11 of 100) and 39% (34 of 88) overpenetration, respectively, with a minimal risk for underpenetration at 2% (2 of 100). Patients with vaccinations in the shoulder with the Centers for Disease Control and Prevention–recommended
5⁄8-,7⁄8-, and 1-in needles would experience 11% (16 of 150), 55% (83 of 150), and 61% (92 of 150) overpenetration,
respectively.
CONCLUSIONS.There is a substantial risk for overpenetration of the intramuscular layer when using current Centers for Disease Control and Prevention recommendations for vaccination needle lengths. We recommend a revision of the needle-length guidelines for thigh and shoulder injections to minimize the risk for needle overpenetration on the basis of the variability observed in the fat thickness.Pediatrics2008;122:e556–e563
I
NTRAMUSCULAR INJECTION IS recommended for most childhood vaccines. The thigh (vastus lateralis muscle) is the preferred intramuscular injection site for infants up to 12 to 18 months. Intramuscular injections are typically administered in the shoulder (deltoid muscle) for children beyond this age. Although there is some age overlap between the 2 sites, the deltoid muscle is often favored in children who are older than 1 year because it is associated with less pain in the affected extremity when ambulating and results in fewer and milder adverse reactions.1,2Intramuscular injectionhas several advantages over subdermal and intradermal delivery. Vaccines are preferably given at the intramuscular level to minimize local irritation, inflammation, granuloma formation, and tissue necrosis.1–13 Furthermore, intramuscular
vaccines, when properly delivered to the intramuscular level, increase immunogenicity and produce a better immune response than when they are delivered at the subcutaneous or intradermal level.1,2,4–8,10–14
Several research groups have studied the risk for short needles’ inadvertently underpenetrating the intramuscular level and delivering the vaccine in the subcutaneous fat tissue1,3–7,9,10,14,15; however, the potential for needle
over-penetration of the intramuscular level into the bone or periosteum has been given little examination because of its perception as being a minor problem. Overpenetration can cause pain and/or damage to the bone or periosteum in the patient who receives the vaccination. It can also cause the needle to detach from the syringe.
The February 2007 US Centers for Disease Control and Prevention (CDC) Pink Book recommended a 1-in needle for all thigh intramuscular immunizations in infants aged 1 to 12 months and; a 1-in to 11⁄4-in needle for all thigh
www.pediatrics.org/cgi/doi/10.1542/ peds.2008-0374
doi:10.1542/peds.2008-0374
Key Words
vaccine, intramuscular injection, anterolateral thigh, deltoid Abbreviations
CDC—US Centers for Disease Control and Prevention
CT— computed tomography Accepted for publication May 30, 2008
Address correspondence to Eric J. Wall, MD, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, MLC 2017, Cincinnati, OH 45229. E-mail: [email protected]
intramuscular immunizations in toddlers aged 12 to 24 months; and a5⁄8-in to 1-in needle for all deltoid
(shoul-der) intramuscular immunizations of children of all ages from 1 to 18 years.16,17 All recommendations from the
CDC are outlined in Table 1.
Previous vaccination studies examined muscle layer depth using ultrasound; however, pressure from the ul-trasound head may deform the tissue during measure-ment. Our study used MRI and computed tomography (CT) scans to measure injection depth. This is the first study conducted to determine the risk for overpenetra-tion and underpenetraoverpenetra-tion with MRI/CT measurements on a wide range of children within the United States. The purpose of this study was to determine accurately the depth of the muscle layer beneath the skin surface of the thigh and the shoulder in a large sample of chil-dren aged 0 to 18 years in the United States.
METHODS
After institutional review board approval was obtained, a total of 250 patients from a large children’s hospital were included in this study. We collected data on pa-tients who had an MRI or a CT scan of their normal thigh between the ages of 2 months and 6 years and patients who had an MRI or CT scan of their normal shoulder between the ages of 12 months and 18 years.
One-hundred patients between the ages of 2 months and 6 years had an MRI or a CT scan of their thigh. We measured the subcutaneous fat and muscle in the middle third of the vastus lateralis (anterolateral of the thigh) at a 90° angle to the skin, which is the recommended CDC site and technique for intramuscular injection (Figs 1 and 2).
A total of 150 patients between the ages of 12 months and 18 years had an MRI or a CT scan of their shoulder. We measured the soft tissue thickness 5 cm distally from the acromion in the deltoid muscle (roughly the middle third of the muscle) at a 90° angle to the skin, as rec-ommended by the CDC (Figs 3 and 4). Picture Archiving and Communications System software (GE Healthcare, Piscataway, NJ) was used to make these measurements to a scale of 1:1 to maximize the accuracy (Figs 1– 4). In addition, weight and age at the time of the MRI or CT scan were recorded from the patient’s medical chart.
The fat and muscle thickness measurements were cor-related to weight, age, and gender to determine the optimal needle length for a safe intramuscular injection. Regression analysis was performed to determine whether a linear re-lationship between age and skin-to-bone thickness, fat thickness, and muscle thickness separately was present. Also, SAS software (SAS Institute, Inc, Cary, NC) was used to analyze the data and Microsoft Excel 2004 (Microsoft Corp, Redmond, WA) was used to graph the data.
FIGURE 1
Fat and muscle thickness measurements in the thigh using MRI.
FIGURE 2
Fat and muscle thickness measurements in the thigh using a CT scan.
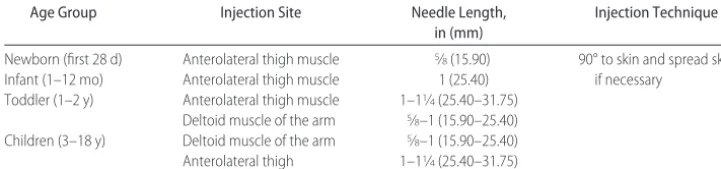
TABLE 1 Intramuscular Vaccination-Delivery Recommendations From the CDC Pink Book (Feb 2007)
Age Group Injection Site Needle Length, in (mm)
Injection Technique
Newborn (first 28 d) Anterolateral thigh muscle 5⁄8(15.90) 90° to skin and spread skin
if necessary Infant (1–12 mo) Anterolateral thigh muscle 1 (25.40)
Toddler (1–2 y) Anterolateral thigh muscle 1–11⁄4(25.40–31.75)
Deltoid muscle of the arm 5⁄8–1 (15.90–25.40)
Children (3–18 y) Deltoid muscle of the arm 5⁄8–1 (15.90–25.40)
RESULTS
Thigh
Thigh measurements were taken from MRI or CT scans of the thigh of 100 children aged 0 to 6 years; 12 were aged 0 to 1 year, and 88 were aged 1 year to 6 years. Using the CDC recommended needle lengths for the thigh muscle, overpenetration would occur in 11% (11 of 100) of patients who received an injection with a 1-in needle and 39% (34 of 88) of patients (age ⱖ1 year) who received an injection with a 11⁄4-in needle (Figs
5–7). Underpenetration would occur by using the 1-in needle for patients agedⱖ1 year only 2% (2 of 100) of the time. The7⁄8-in needle for intramuscular injection in
the thigh (not recommended by the CDC) would result in a 4% (4 of 100) overpenetration rate and a 2% (2 of 100) underpenetration rate.
Shoulder
Shoulder measurements were taken from MRI or CT scans of the deltoid of 150 children aged 1 to 18 years; 12 were aged 1 to 2 years, and 138 were aged 3 to 18 years. The risk for overpenetration by using CDC needle-length guidelines was much higher in the shoulder deltoid muscle. The CDC recommended5⁄8-in,7⁄8-in, or 1-in needles for
intramuscu-lar injections in the deltoid in children aged 1 to 18 years would cause 11% (16 of 150), 55% (83 of 150), and 61% (92 of 150) of patients to experience overpenetration (Figs 8 and 9). Also, underpenetration would occur in 8% (12 of 150), 2% (3 of 150), and 1.3% (2 of 150) of patients receiving a5⁄8-in, 7⁄8-in, or 1-in needle for intramuscular
injection in the deltoid. A1⁄2-inch needle for intramuscular
injection in the deltoid would yield a 1.3% (2 of 150) overpenetration rate, but will underpenetrate 15% (23 of 150) of the time.
We observed differences in fat and muscle thickness in the thigh and deltoid muscles on the basis of gender. On average, girls had greater fat and muscle thickness in
the thigh in comparison with boys of a similar age. Also, girls had a thicker fat thickness in the deltoid but a thinner muscle thickness in comparison with boys of a similar age; however, results of 2-samplettests between the fat and muscle thicknesses between girls and boys were statistically significant only for the fat thickness of the deltoid muscle in the 1- to 2-year age group. Also, the muscle and fat thickness of the deltoid muscle in the 3- to 18-year age group was found to be statistically significant (Table 2).
Regression analysis for fat and skin-to-bone thickness of the thigh against age in the 1 to 2 years and 3 to 6 years, respectively, was statistically significant at the .01 level. Analysis for muscle thickness of the thigh against age in the 3 to 6 years was statistically significant at the .05 level. Analysis for skin-to-bone thickness and muscle thickness of the deltoid against age in the 3 to 18 years was statistically significant at the .001 level (Table 3).
DISCUSSION
Our results reveal a striking risk for needle intramuscu-lar overpenetration into the bone, especially at the shoulder site. The CDC recommended a5⁄8-in,7⁄8-in, or
1-in needles for intramuscular injections in the deltoid in children aged 1 to 18 years would cause 11% (16 of 150), 55% (83 of 150), and 61% (92 of 150) of patients to experience overpenetration (Figs 8 and 9). These skin-to-bone thickness results in the shoulder are con-sistent with the ultrasound-measured results of Gros-wasser et al4and Lo et al.10Calculating from the
mea-surements in these other studies, overpenetration would be seen in 100% of patients on the basis of the needle length recommendations offered by the CDC in the shoulder, but the authors mostly focused on underpen-etration, which would occur less commonly at 0% of the time.
Conversely, the results were not as significant for the thigh muscle. Our results showed that overpenetration of the thigh muscle would occur in 11% (11 of 100) of patients who were administered an injection with a 1-in needle and 39% (34 of 88) of patients (age ⱖ1 year)
FIGURE 3
Fat and muscle thickness measurements in the deltoid using MRI.
FIGURE 4
who were administered and injection with a 11⁄4-in
nee-dle (Figs 5–7). Hicks and colleagues2,6,11,16,17 found
sub-cutaneous fat thickness measurements in the thigh sim-ilar to ours and agreed with the CDC recommendation that a 1-in needle should be used when vaccinating at a 90° angle a child, aged 1 to 12 months, in the thigh. Consequentially, we recommend a7⁄8-in or longer
nee-dle for all children up to age 6 years to ensure proper intramuscular injections in the thigh muscle (Table 4). With these recommendations, 90% of all children who receive a vaccination in the thigh will be vaccinated into the intramuscular level, in comparison with the 64% intramuscular delivery rate if using the current CDC recommendations (Figs 5–7).
The recommendations for the male and female del-toid are more complex. On the basis of our data, we advise that a 1⁄2-in needle be used for any girl who
weighsⱕ70 kg and any boy who weighsⱕ75 kg. A5⁄8-in
needle is recommended for any girl who weighs be-tween 70 and 115 kg and any boy who weighs bebe-tween 75 and 140 kg. A7⁄8-in or longer needle should be used
for any girl who weighs ⬎115 kg and any boy who weighs ⬎140 kg (Table 4). With these recommenda-tions, 90% of both female and male patients would be vaccinated safely at the intramuscular level. Also, these recommendations ensure a 0% overpenetration rate for all patients (Figs 8 and 9).
A standard needle size for a particular weight, age, or gender will not guarantee successful intramuscular in-jection in all patients as the CDC and other institutions advise because of the significant anatomic variability, especially in the deltoid muscle layer. This is confirmed through the regression analysis, because a linear trend between skin-to-bone thickness, fat thickness, and mus-cle thicknesses with age in the 1- to 2-year age group was not observed. Also, a linear trend was not seen between fat thicknesses with age in the 3- to 18-year age group. Similar results occurred in the thigh muscle for the 3- to 6-year age group (Table 3). The sample sizes for the 3- to 18-year age group in the deltoid and 3- to 6-year age group in the thigh are substantial enough to suggest that the subcutaneous fat tissue at these
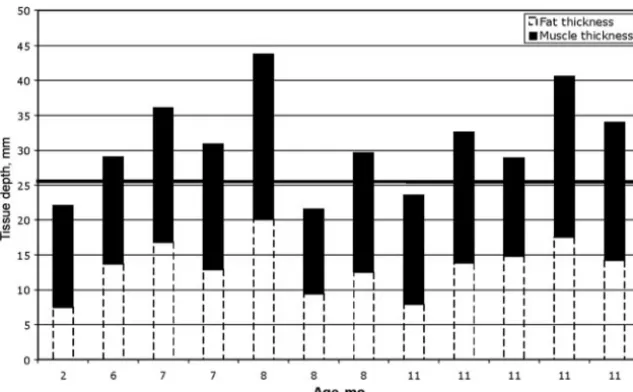
injec-FIGURE 5
Depth from skin to bone in patients from 2 to 12 months of age who would receive an intramuscular vaccination in the thigh on the basis of recommendations from the CDC. The age is in months, and the tissue (skin-to-bone) depth is in millimeters. The skin/subcutaneous fat thickness is represented by the white area inside the dotted lines; the muscle thickness is represented by the shaded region; and the bone is represented by the white area above the shaded region.
FIGURE 6
tion sites is the possible cause for the variability seen in the overall results. If the other age groups for the thigh and deltoid muscles had larger sample sizes, then the same trend may be witnessed. In addition, the results of the 2-sample ttests show that the boys and girls mea-sured at the deltoid muscle site show significant varia-tions in fat and muscle thicknesses for the 3- to 18-year age group. A significant variation in the 1- to 2-year age group of the deltoid muscle between boys and girls was seen only in the fat thickness. Along with the variability between fat thickness and age, the variability between genders may have contributed to the strong variability in the deltoid muscle. Consequentially, we recommend that clinical judgment be used and an assortment of different needle lengths be readily available for vaccine injection. The Groswasser et al4and Zuckerman5studies
made similar recommendations, as well as promoted
the use of clinical judgment in selecting appropriate needle length during vaccine administration to optimize the success of intramuscular delivery. An ultrasound may be used to determine the skin-to-bone thickness before administering the vaccine, but this adds a level of complexity to the process. The variability in our data does not represent the entire variability seen in the general population. Thus, the CDC may want to alter their recommendations to include using clinical judg-ment, because a standard needle size for a certain age group or weight class will never guarantee proper intra-muscular administration in all patients. The pinch tech-nique, in which the vaccinator pinches a fold of thigh or arm tissue, may decrease the risk for overpenetration, but this technique may increase the risk for underpen-etration. The accuracy of the pinch technique has not been validated. Typically, the pinch technique is used
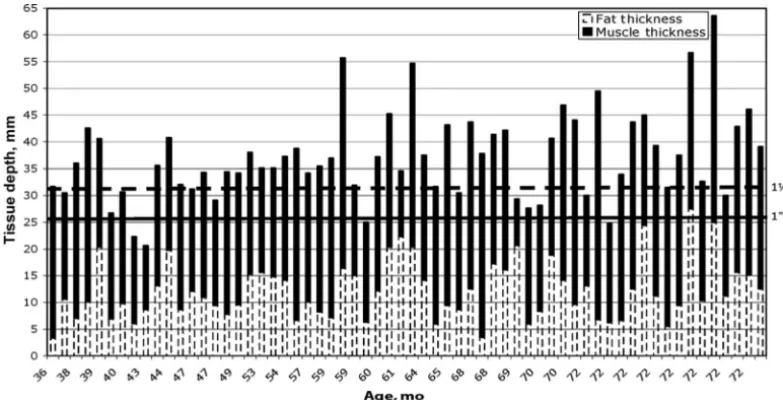
FIGURE 7
Depth from skin to bone in patients 3 to 6 years of age who would receive an intramuscular vaccination in the thigh on the basis of recommendations from the CDC. The age is in months, and the tissue (skin-to-bone) depth is in millimeters. The skin/subcutaneous fat thickness is represented by the white area inside the dotted lines; the muscle thickness is represented by the shaded region; and the bone is represented by the white area above the shaded region.
FIGURE 8
when administering subcutaneous vaccines to avoid the possibility of injecting the vaccine at the intramuscular level.17The spreading technique is executed to ensure an
intramuscular injection, because it reduces the thickness of the subcutaneous layer.17 We suggest that a future
study be conducted to assess the pinch technique on a wider range of US children by using ultrasound. The pinch technique may increase vaccine safety with the current CDC needle-length recommendations. Given that this study has yet to be conducted, skinfold thick-ness measurement with calipers may be a simple way to improve the success of intramuscular vaccine delivery.
Our study has several limitations because of its retro-spective nature. Although this is one of the largest stud-ies to report on vaccination anthropometric data, the weight and age of the patients are not evenly distributed throughout the large range. Our sample from a large Midwestern city may not accurately represent the gen-eral population of the United States. Because of wide geographic variation in infant and child weight, it is difficult to make universal needle-length recommenda-tions. Obesity in children and adolescents has increased tremendously in many Western countries, especially in the United States, and can depend on ethnic, socioeco-nomic, and religious status.18–20There are a high number
of undernourished children who are younger than 5 years in India and China,21,22 which likely skew the
results of the Lo et al and Chugh et al studies. The tremendous variability in fat and muscle thickness found in our study makes universal intramuscular vaccine nee-dle-length recommendations difficult. The discrepancy in the results attained from our study in comparison with the Chugh et al,9Cook and Murtagh,13Groswasser
et al,4Hick et al,6and Lo et al10studies could be because
we used MRIs and CT scans, which are deemed more accurate in measuring and showing the distinction be-tween muscle and fat layers because they do not use a probe that touches or compresses the skin.23
We used the healthy shoulder and thigh on MRIs and CT scans that were obtained for other reasons, and this population may not exactly represent the vaccination population at large. We used the normal side of a bilat-eral shoulder or thigh MRI or CT scan from which to make measurements. Most of the MRI or CT scans for the young shoulders were performed for brachial plexus palsy on the opposite side, and these children are known to have higher birth weights than a typical newborn.24
This would tend to underestimate the risk for overpen-etration. The measurement accuracy in Picture Archiv-ing Communications System for MRI and CT scans was another possible limitation. The measurement error was
⫾1 pixel when the image was scaled to its absolute size or original resolution (1:1).25,26Furthermore, the spacing
of the pixels was not a standard size for all patients, and
FIGURE 9
Depth from skin to bone in patients from 3 to 18 years of age who would receive an intramuscular vaccination in the deltoid on the basis of recommendations from the CDC. The age is in months, and the tissue (skin-to-bone) depth is in millimeters. The skin/subcutaneous fat thick-ness is represented by the white area inside the dotted lines; the muscle thickness is represented by the shaded region; and the bone is represented by the white area above the shaded region.
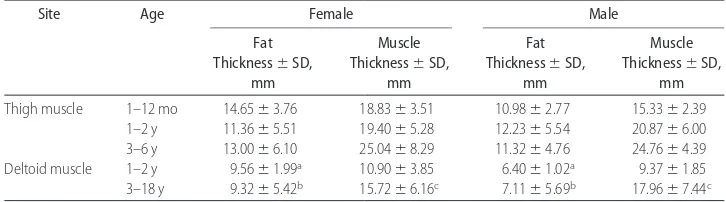
TABLE 2 Fat (Subcutaneous) and Muscle Layer Thickness Measurements for Thigh and Deltoid Muscles in Both Female and Male Patients Arranged by Age According to CDC Recommendations
Site Age Female Male
Fat Thickness⫾SD,
mm
Muscle Thickness⫾SD,
mm
Fat Thickness⫾SD,
mm
Muscle Thickness⫾SD,
mm
Thigh muscle 1–12 mo 14.65⫾3.76 18.83⫾3.51 10.98⫾2.77 15.33⫾2.39 1–2 y 11.36⫾5.51 19.40⫾5.28 12.23⫾5.54 20.87⫾6.00 3–6 y 13.00⫾6.10 25.04⫾8.29 11.32⫾4.76 24.76⫾4.39 Deltoid muscle 1–2 y 9.56⫾1.99a 10.90⫾3.85 6.40⫾1.02a 9.37⫾1.85
3–18 y 9.32⫾5.42b 15.72⫾6.16c 7.11⫾5.69b 17.96⫾7.44c
the average measurement of each pixel in all the patients was⫾0.63 mm.
In addition, the results of our study assume that the needle is fully inserted so that the hub touches the patient’s skin. Typically, overpenetration has not been perceived as a major problem in comparison with un-derpenetration because vaccinators are advised simply to pull back before depositing the vaccine if they sense that the needle has hit the bone12; however, striking the bone
with the needle is liable to cause pain, damage to the bone or periosteum, and/or breakage of the needle.
CONCLUSIONS
Our study supports the conclusion that a 7⁄8- or 1-in
needle is excellent for thigh intramuscular injections in both genders of infants and children up to age 6 years, which is similar to the CDC recommendations; however, our data suggest that the CDC recommendations for needle length for intramuscular injection in the shoulder will overpenetrate the muscle layer and strike bone or periosteum in 11%, 55%, and 61% of patients who receive a5⁄8-,7⁄8-, or 1-in needle. This could cause severe
pain and also impair delivery to the intramuscular level. This has prompted the following recommendations for vaccination in the shoulder: a 1⁄2-in needle for any girl
who weighsⱕ70 kg and any boy who weighsⱕ75 kg; a
5⁄8-in needle for any girl who weighs between 70 and
115 kg and any boy who weighs between 75 and 140 kg; and a7⁄8- to 1-in needle for any girl who weighsⱖ115 kg
and any boy who ⱖweighs 140 kg to ensure proper intramuscular injection (Table 4).
ACKNOWLEDGMENTS
We thank Sara Stark, Carrie Schmitt, and the Orthopae-dic Clinic Staff at the Cincinnati Children’s Hospital Medical Center for assistance. We also thank Dr Janet Rice (Department of Biostatistics, Tulane University School of Public Health and Tropical Medicine) for as-sistance with data analysis.
REFERENCES
1. Ipp MM, Gold R, Goldbach M, et al. Adverse reactions to diphtheria, tetanus, pertussis-polio vaccination at 18 months of age: effect of injection site and needle length.Pediatrics.1989; 83(5):679 – 682
2. Pickering LK, ed. Red Book: 2006 Report of the Committee on Infectious Diseases. 27th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006
3. Bergeson PS, Singer SA, Kaplan AM. Intramuscular injections in children.Pediatrics.1982;70(6):944 –948
4. Groswasser J, Kahn A, Bouche B, Hanquinet S, Perlmuter N, Hessel L. Needle length and injection technique for efficient in-tramuscular vaccine delivery in infants and children evaluated through an ultrasonographic determination of subcutaneous and muscle layer thickness.Pediatrics.1997;100(3 pt 1):400 – 403 5. Zuckerman JN. The importance of injecting vaccines into
muscle: different patients need different needle sizes. BMJ.
2000;321(7271):1237–1238
6. Hick JF, Charboneau JW, Brakke DM, Goergen B. Optimum needle length for diphtheria-tetanus-pertussis inoculation of infants.Pediatrics.1989;84(1):136 –137
7. Poland GA, Borrud A, Jacobson RM, et al. Determination of deltoid fat pad thickness: implications for needle length in adult immunization.JAMA.1997;277(21):1709 –1711
8. Cook IF, Murtagh J. Paediatric vaccination practice in a divi-sion of general practice. Aust Fam Physician. 2001;30(12): 1185–1189
9. Chugh K, Chawla D, Aggarwal BB. Optimum needle length for DPT inoculation of Indian infants.Indian J Pediatr.1993;60(3): 435– 40
10. Lo YS, Lu CC, Chen LY, Huang LY, Jong YJ. Quantitative measurement of muscle and subcutaneous fat thickness in newborn by real-time ultrasonography: a useful method for site and depth evaluation in vaccination.Gaoxiong Yi Xue Ke Xue Za Zhi.1992;8(2):75– 81
11. Pickering LK, ed. Red Book: 2003 Report of the Committee on Infectious Diseases. 26th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2003
12. Bentley C.Immunization Techniques: Safe, Effective, Caring[DVD]. Sacramento, CA: California Department of Health Services Im-munization Branch; 2001
13. Cook IF, Murtagh J. Needle length required for intramuscular vaccination of infants and toddlers: an ultrasonographic study.
Aust Fam Physician.2002;31(3):295–297
14. Diggle L, Deeks J. Effect of needle length on incidence of local reactions to routine immunisation in infants aged 4 months: randomised controlled trial.BMJ.2000;321(7266):931–933
TABLE 3 Regression Analysis Results for Thigh and Deltoid Muscles Versus Age According to CDC Recommendations
Site Age Demographic tTest Statistic Value
P
Thigh muscle 1–12 mo Skin-to-bone thickness 1.038 .324
Fat thickness 1.013 .335
Muscle thickness 0.937 .371 1–2 y Skin-to-bone thickness ⫺1.438 .163 Fat thickness ⫺2.972 .007a
Muscle thickness 0.720 .479 3–6 y Skin-to-bone thickness 2.782 .007b
Fat thickness 1.557 .125
Muscle thickness 2.093 .041c
Deltoid muscle 1–2 y Skin-to-bone thickness 1.188 .262
Fat thickness 1.248 .240
Muscle thickness 0.673 .516 3–18 y Skin-to-bone thickness 3.280 .001d
Fat thickness ⫺0.519 .605 Muscle thickness 5.547 ⬍.001e
aStatistically significant at␣⫽.01 level. bStatistically significant at␣⫽.01 level. cStatistically significant at␣⫽.05 level. dStatistically significant at␣⫽.001 level. eStatistically significant at␣⫽.001 level.
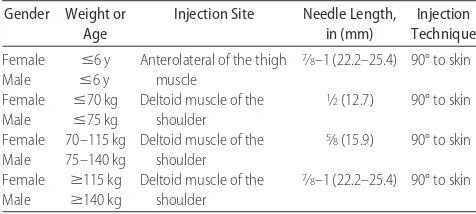
TABLE 4 Our Recommendations for Intramuscular Injection on the Basis of Data From This Study
Gender Weight or Age
Injection Site Needle Length, in (mm)
Injection Technique
Female Male
ⱕ6 y ⱕ6 y
Anterolateral of the thigh muscle
7⁄8–1 (22.2–25.4) 90° to skin
Female Male
ⱕ70 kg ⱕ75 kg
Deltoid muscle of the shoulder
1⁄2(12.7) 90° to skin
Female Male
70–115 kg 75–140 kg
Deltoid muscle of the shoulder
5⁄8(15.9) 90° to skin
Female Male
ⱖ115 kg ⱖ140 kg
Deltoid muscle of the shoulder
15. Thow JC, Coulthard A, Home PD. Insulin injection site tissue depths and localization of a simulated insulin bolus using a novel air contrast ultrasonographic technique in insulin treated diabetic subjects.Diabet Med.1992;9(10):915–920
16. General recommendations on immunization. Recommenda-tions of the Advisory Committee on Immunization Practices (ACIP).MMWR Recomm Rep.1994;43(RR-1):1–38
17. Centers for Disease Control and Prevention.Epidemiology and Prevention of Vaccine-Preventable Diseases: The Pink Book—Course Textbook.10th ed. Washington, DC: Public Health Foundation; 2007
18. Kuczmarski RJ, Flegal KM, Campbell SM, Johnson CL. Increas-ing prevalence of overweight among US adults: the National Health and Nutrition Examination Surveys, 1960 to 1991.
JAMA.1994;272(3):205–211
19. Pi-Sunyer FX. The fattening of America.JAMA.1994;272(3): 238 –239
20. Troiano RP, Flegal KM, Kuczmarski RJ, Campbell SM, Johnson CL. Overweight prevalence and trends for children and
adolescents: the National Health and Nutrition Examination Surveys, 1963 to 1991.Arch Pediatr Adolesc Med.1995;149(10): 1085–1091
21. Sen A. Gender equity and the population problem.Int J Health Serv.2001;31(3):469 – 474
22. Haen HD.Hunger and Mortality: The State of Food Insecurity in the World (SOFI). Rome, Italy: Food and Agriculture Organization of the United Nations. 2002
23. Rankin S. CT and MRI.Surgery (Oxford). 2005;23(5):162–165 24. van Ouwerkerk WJ, van der Sluijs JA, Nollet F, Barkhof F,
Slooff AC. Management of obstetric brachial plexus lesions: state of the art and future developments. Childs Nerv Syst.
2000;16(10 –11):638 – 644
25. Poglitsch A. PACS instrument design description and system performance. Available at: http://pacs.ster.kuleuven.ac.be. Ac-cessed June 28, 2007
DOI: 10.1542/peds.2008-0374 originally published online August 11, 2008;
2008;122;e556
Pediatrics
William C. Lippert and Eric J. Wall
Optimal Intramuscular Needle-Penetration Depth
Services
Updated Information &
http://pediatrics.aappublications.org/content/122/3/e556 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/122/3/e556#BIBL This article cites 19 articles, 6 of which you can access for free at:
Subspecialty Collections
_sub
http://www.aappublications.org/cgi/collection/vaccine:immunization
Vaccine/Immunization
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2008-0374 originally published online August 11, 2008;
2008;122;e556
Pediatrics
William C. Lippert and Eric J. Wall
Optimal Intramuscular Needle-Penetration Depth
http://pediatrics.aappublications.org/content/122/3/e556
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.